
Imaging in Hip Arthroplasty Management Part 2: Postoperative Diagnostic Imaging Strategy

 , , , and
, , , and
Abstract
:1. Introduction
2. Types of HA
2.1. Type of Prosthesis and Implants
2.2. Type of Fixation
2.3. Bearing Surfaces
3. Imaging Follow-Up of HA
3.1. Initial Imaging Assessment
3.2. Technical Aspects
3.2.1. Computed Tomography
3.2.2. Magnetic Resonance Imaging
3.3. Implants Positioning and Their Implications
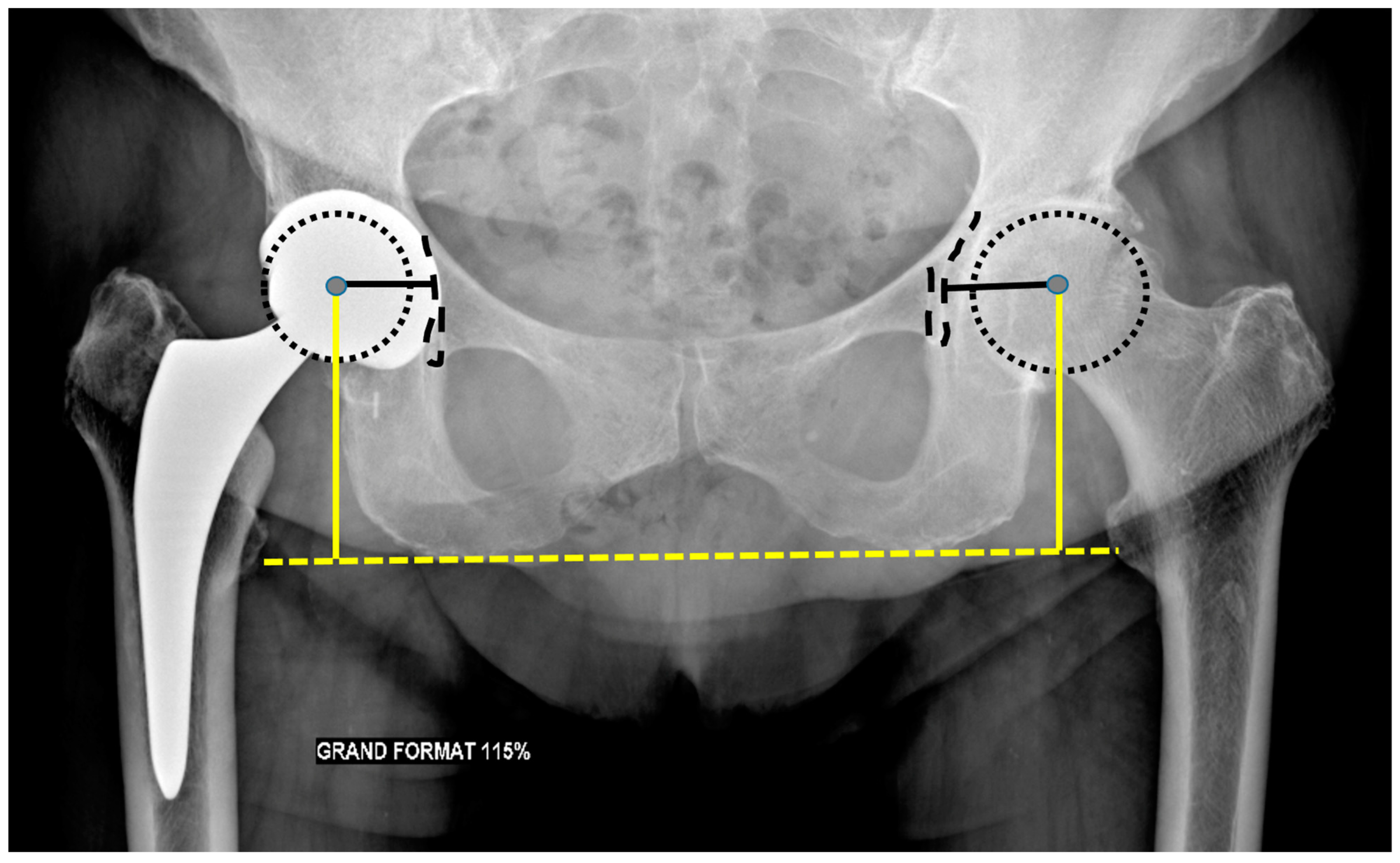
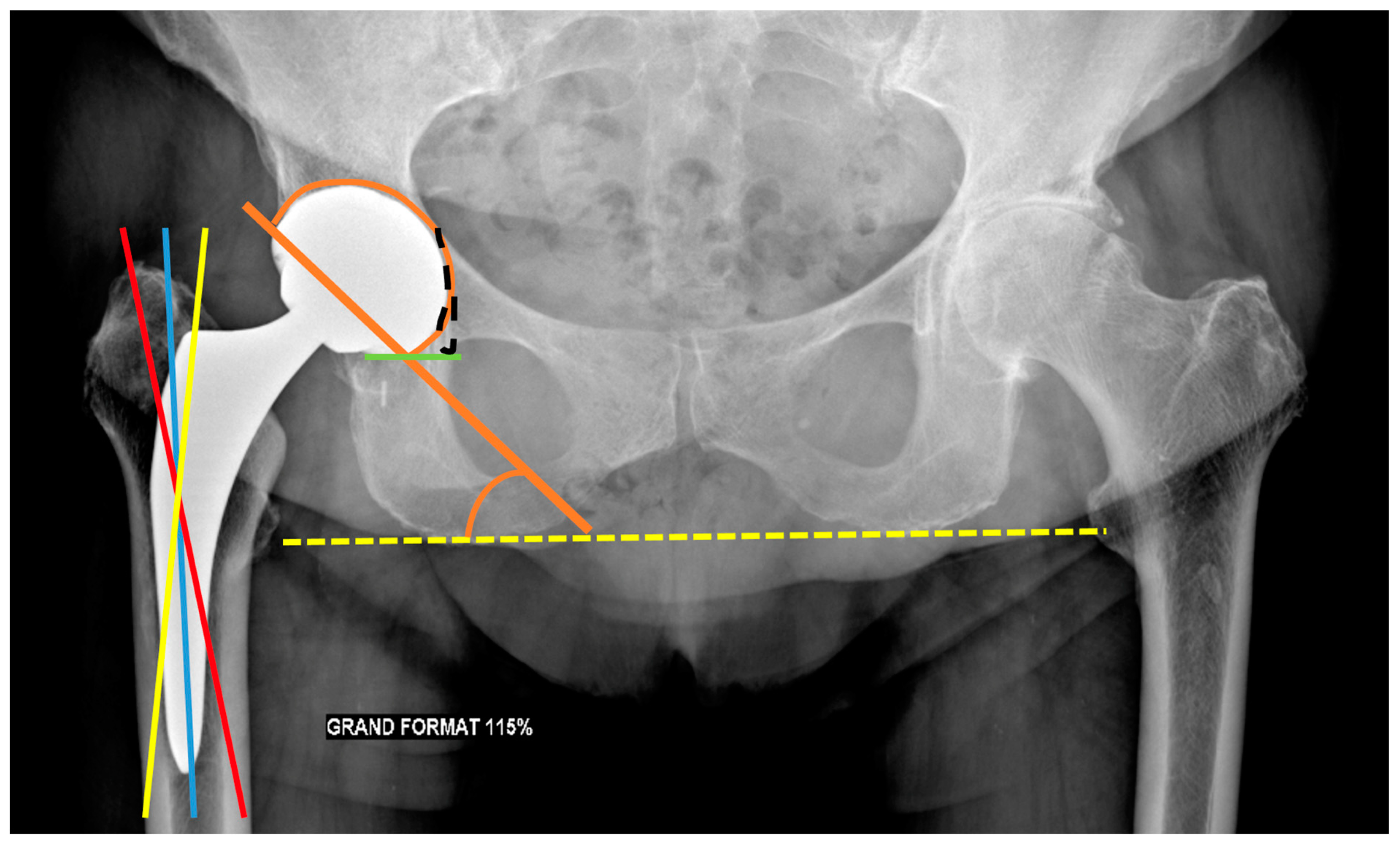
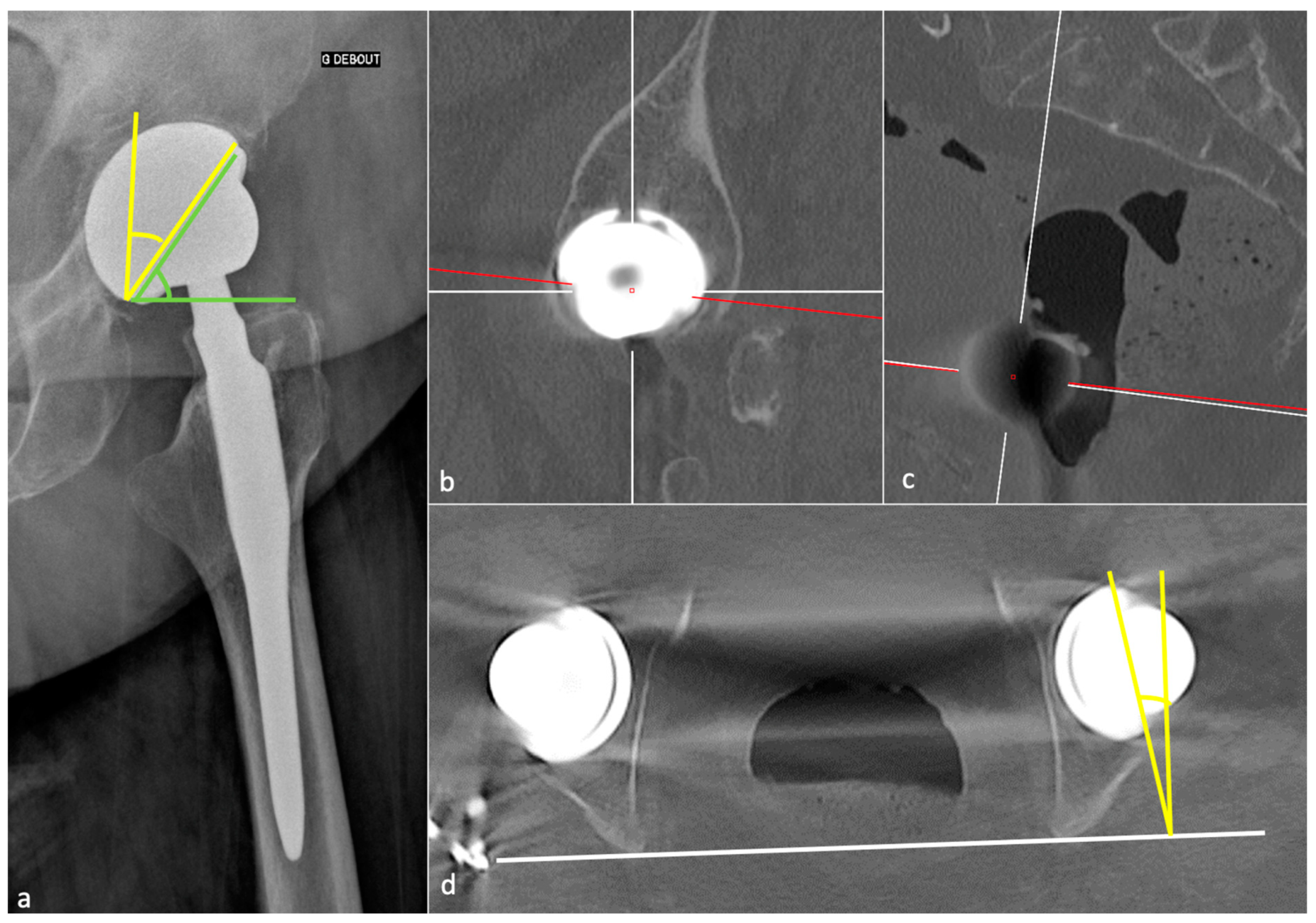
3.3.1. Acetabular Side
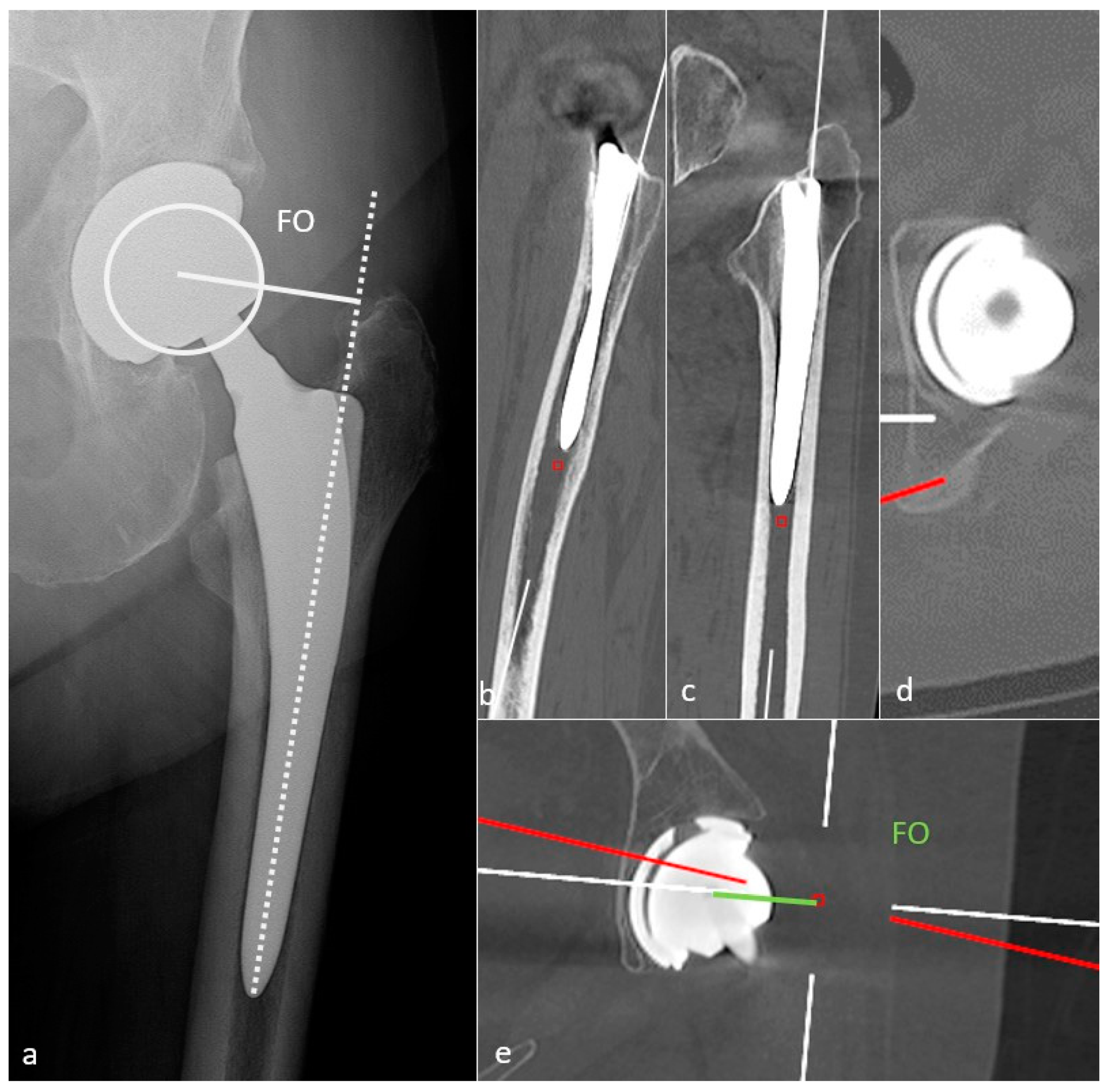
3.3.2. Femoral Side
3.4. Normal Imaging Findings
3.4.1. Radiolucent Zones (Radiographs, Tomosynthesis and CT)
3.4.2. Adaptative Changes (Radiographs, Tomosynthesis and CT)
3.4.3. MRI
- Bone marrow edema was frequent all over the femoral stem and in the central acetabular zone at 3 and 6 months after surgery, decreased during follow-up, and sometimes persisted in Gruen zones 1 and 7 overtime, but often in only one area;
- Inferomedial edema in the acetabulum was infrequent and should raise suspicion for pathology;
- Periprosthetic bone resorption was frequent during the second post-operative year in Gruen zones 1 and 8 but never thicker than 2 mm;
- Periosteal edema was shared on the femoral side with a decrease over time, rarely present at two years, and only in non-adjacent Gruen zones, without acetabular side attempt;
- In the first six months, soft-tissue edema was a constant feature in the surgical access route but never occurred in the second year;
- Joint effusion was decreasing over time but could be present in the lateral aspect of the joint capsule at two years [19].
4. Complications
4.1. Dislocation
4.1.1. Background
4.1.2. Imaging
4.1.3. Imaging Perspectives
4.2. Ergonomics
4.2.1. Background
4.2.2. Imaging
4.3. Osteolysis and Loosening
4.3.1. Background
4.3.2. Imaging
4.3.3. Radiographs, Tomosynthesis, and CT
4.3.4. MRI
4.4. Infection
4.4.1. Background
4.4.2. Septic versus Aseptic Loosening Imaging Signs
4.5. Synovitis
4.5.1. Background
4.5.2. Classification and Contribution of Imaging Methods
- Metallosis results from the shedding of metallic debris (secondary to a MoM prosthesis with corrosion, a conflict between a metallic acetabular cup and the prosthetic neck, or a contact between a metallic head and an acetabular metal back in case of PE wear or dislocation) that induces synovitis and an indolent pattern of osteolysis, potentially leading to loosening (i.e., potentially looking similar to osteolysis and PE wear). Synovitis may contain low-signal intensity or metallic density debris, causing MRI artifacts and bone erosion, best depicted on CT-MAR (Figure 20). Such debris might also be located in periprosthetic soft tissue and lymph nodes [54,57]. Metallic debris presence might also accentuate PE wear (i.e., third fragment wear) [54]. Of note, high serum metal-ion levels can be found in symptomatic and asymptomatic patients and would be associated with pseudo-tumors, so that such a biological finding should lead to the prescription of an MRI to rule out a pseudo-tumor even in asymptomatic patients [6,103].
- Additionally, referred to as trunnionosis, trunnion corrosion corresponds to a soft-tissue reaction to metal debris released from micromotion and mechanical wear at the head–neck or neck–stem junction of modular MoP HA. On MRI, it manifests as an adverse local reaction associated with medial calcar resorption [11,104].
4.5.3. MRI Focus
4.6. Psoas Impingement
4.6.1. Background
4.6.2. Imaging
4.7. Squeaking
4.8. Muscle Pathology
4.8.1. Background
4.8.2. Imaging
4.9. Neurovascular Complications
4.10. Peri-Prosthetic Fractures and Stress Reactions
4.10.1. Background
4.10.2. Imaging
4.11. Heterotopic Ossification
4.12. Implant Failure
4.13. Resurfacing Arthroplasties
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AO | Acetabular offset |
| CE | Contrast-enhanced |
| CoC | Ceramic-on-ceramic |
| CoP | Ceramic-on-polyethylene |
| CT | Computed tomography |
| FNA | Femoral neck anteversion |
| FO | Femoral offset |
| FOV | Field of view |
| FSE | Fast-spin echo |
| HA | Hip arthroplasty |
| MAR | Metal artifact reduction |
| MoM | Metal-on-metal |
| MoP | Metal-on-polyethylene |
| PE | Polyethylene |
| PJI | Prosthetic joint infection |
| RLZ | Radiolucent zone |
| SE | Spin echo |
| SPECT-CT | Single-photon emission computed tomography |
| STIR | Short TI inversion recovery |
| THA | Total hip arthroplasty |
References
- Wylde, V.; Hewlett, S.; Learmonth, I.D.; Dieppe, P. Persistent Pain after Joint Replacement: Prevalence, Sensory Qualities, and Postoperative Determinants. Pain 2011, 152, 566–572. [Google Scholar] [CrossRef]
- Labek, G.; Thaler, M.; Janda, W.; Agreiter, M.; Stöckl, B. Revision Rates after Total Joint Replacement: Cumulative Results from Worldwide Joint Register Datasets. J. Bone Jt. Surg. Br. 2011, 93, 293–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolajsen, L.; Brandsborg, B.; Lucht, U.; Jensen, T.S.; Kehlet, H. Chronic Pain Following Total Hip Arthroplasty: A Nationwide Questionnaire Study. Acta Anaesthesiol. Scand. 2006, 50, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Beswick, A.D.; Wylde, V.; Gooberman-Hill, R.; Blom, A.; Dieppe, P. What Proportion of Patients Report Long-Term Pain after Total Hip or Knee Replacement for Osteoarthritis? A Systematic Review of Prospective Studies in Unselected Patients. BMJ Open 2012, 2, e000435. [Google Scholar] [CrossRef]
- Pincus, D.; Jenkinson, R.; Paterson, M.; Leroux, T.; Ravi, B. Association Between Surgical Approach and Major Surgical Complications in Patients Undergoing Total Hip Arthroplasty. JAMA 2020, 323, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef]
- Department of Orthopaedics and Traumatology, Princess Margaret Hospital, Laichikok, Hong Kong; Lam, Y.; Chan, P.; Fu, H.; Yan, C.; Chiu, K. A Review of the Clinical Approach to Persistent Pain Following Total Hip Replacement. Hong Kong Med. J. 2016, 22, 600–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agten, C.A.; Sutter, R.; Dora, C.; Pfirrmann, C.W.A. MR Imaging of Soft Tissue Alterations after Total Hip Arthroplasty: Comparison of Classic Surgical Approaches. Eur. Radiol. 2017, 27, 1312–1321. [Google Scholar] [CrossRef]
- Bäcker, H.C.; Steurer-Dober, I.; Beck, M.; Agten, C.A.; Decking, J.; Herzog, R.F.; Geller, J.A.; Bhure, U.; Roos, J.E.; Strobel, K. Magnetic Resonance Imaging (MRI) versus Single Photon Emission Computed Tomography (SPECT/CT) in Painful Total Hip Arthroplasty: A Comparative Multi-Institutional Analysis. BJR 2020, 93, 20190738. [Google Scholar] [CrossRef] [PubMed]
- Belzunce, M.A.; Henckel, J.; Di Laura, A.; Hart, A. Uncemented Femoral Stem Orientation and Position in Total Hip Arthroplasty: A CT Study. J. Orthop. Res. 2020, 38, 1486–1496. [Google Scholar] [CrossRef]
- Berkowitz, J.L.; Potter, H.G. Advanced MRI Techniques for the Hip Joint: Focus on the Postoperative Hip. Am. J. Roentgenol. 2017, 23, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozza, N.; Guindani, N.; Pezzotta, G.; Alberto, F.; Castelli, C.C. 15-Year follow-up of MoM 36-Mm THA: Clinical, Laboratory, and Radiological (CT and MRI) Prospective Assessment. HIP Int. 2020, 30, 42–51. [Google Scholar] [CrossRef]
- Burge, A. Total Hip Arthroplasty: MR Imaging of Complications Unrelated to Metal Wear. Semin. Musculoskelet. Radiol. 2015, 19, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh, S.; Omar, I.M. Imaging of Hip Arthroplasties: Normal Findings and Hardware Complications. Semin. Musculoskelet. Radiol. 2019, 23, 162–176. [Google Scholar] [CrossRef] [PubMed]
- Docking, S.I.; Cook, J.; Chen, S.; Scarvell, J.; Cormick, W.; Smith, P.; Fearon, A. Identification and Differentiation of Gluteus Medius Tendon Pathology Using Ultrasound and Magnetic Resonance Imaging. Musculoskelet. Sci. Pract. 2019, 41, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Filli, L.; Jungmann, P.M.; Zingg, P.O.; Rüdiger, H.A.; Galley, J.; Sutter, R.; Pfirrmann, C.W.A. MRI with State-of-the-Art Metal Artifact Reduction after Total Hip Arthroplasty: Periprosthetic Findings in Asymptomatic and Symptomatic Patients. Eur. Radiol. 2020, 30, 2241–2252. [Google Scholar] [CrossRef] [PubMed]
- Galea, V.P.; Laaksonen, I.; Connelly, J.W.; Matuszak, S.J.; Nortje, M.; Madanat, R.; Muratoglu, O.; Malchau, H. What Is the Clinical Presentation of Adverse Local Tissue Reaction in Metal-on-Metal Hip Arthroplasty? An MRI Study. Clin. Orthop. Relat. Res. 2019, 477, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Galley, J.; Sutter, R.; Stern, C.; Filli, L.; Rahm, S.; Pfirrmann, C.W.A. Diagnosis of Periprosthetic Hip Joint Infection Using MRI with Metal Artifact Reduction at 1.5 T. Radiology 2020, 296, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Germann, C.; Filli, L.; Jungmann, P.M.; Graf, D.N.; Fritz, J.; Pfirrmann, C.W.A.; Sutter, R. Prospective and Longitudinal Evolution of Postoperative Periprosthetic Findings on Metal Artifact-Reduced MR Imaging in Asymptomatic Patients after Uncemented Total Hip Arthroplasty. Skelet. Radiol. 2020, 50, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Giori, N.J. CORR Insights®: MRI of THA Correlates with Implant Wear and Tissue Reactions: A Cross-Sectional Study. Clin. Orthop. Relat. Res. 2019, 477, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Hargunani, R.; Madani, H.; Khoo, M.; Fotiadou, A.; Pressney, I.; Calleja, M.; O’Donnell, P. Imaging of the Painful Hip Arthroplasty. Can. Assoc. Radiol. J. 2016, 67, 345–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, J.M.; Czuczman, G.J.; Johnson, R.M.; Dennis, D.A. Metal Artifact Reduction Sequence Magnetic Resonance Imaging Abnormalities in Asymptomatic Patients with a Ceramic-on-Ceramic Total Hip Replacement. J. Arthroplast. 2021, 36, 612–615. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, P.M.; Bensler, S.; Zingg, P.; Fritz, B.; Pfirrmann, C.W.; Sutter, R. Improved Visualization of Juxtaprosthetic Tissue Using Metal Artifact Reduction Magnetic Resonance Imaging: Experimental and Clinical Optimization of Compressed Sensing SEMAC. Investig. Radiol. 2019, 54, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khodarahmi, I.; Fritz, J. Advanced MR Imaging after Total Hip Arthroplasty: The Clinical Impact. Semin. Musculoskelet. Radiol. 2017, 21, 616–629. [Google Scholar] [CrossRef] [PubMed]
- Khodarahmi, I.; Nittka, M.; Fritz, J. Leaps in Technology: Advanced MR Imaging after Total Hip Arthroplasty. Semin. Musculoskelet. Radiol. 2017, 21, 604–615. [Google Scholar] [CrossRef] [PubMed]
- Khodarahmi, I.; Rajan, S.; Sterling, R.; Koch, K.; Kirsch, J.; Fritz, J. Heating of Hip Arthroplasty Implants During Metal Artifact Reduction MRI at 1.5- and 3.0-T Field Strengths. Investig. Radiol. 2020, 56, 232–243. [Google Scholar] [CrossRef]
- Klemt, C.; Simeone, F.J.; Melnic, C.M.; Tirumala, V.; Xiong, L.; Kwon, Y.-M. MARS MRI Assessment of Fatty Degeneration of the Gluteal Muscles in Patients with THA: Reliability and Accuracy of Commonly Used Classification Systems. Skelet. Radiol. 2020, 50, 665–672. [Google Scholar] [CrossRef]
- Koff, M.F.; Esposito, C.; Shah, P.; Mfa, M.M.; Bs, E.B.; Fields, K.; Bauer, T.; Padgett, D.E.; Wright, T.; Potter, H.G. MRI of THA Correlates with Implant Wear and Tissue Reactions: A Cross-Sectional Study. Clin. Orthop. Relat. Res. 2018, 477, 16. [Google Scholar] [CrossRef] [PubMed]
- Kovalak, E.; Özdemir, H.; Ermutlu, C.; Obut, A. Assessment of Hip Abductors by MRI after Total Hip Arthroplasty and Effect of Fatty Atrophy on Functional Outcome. Acta Orthop. Traumatol. Turc. 2018, 52, 196–200. [Google Scholar] [CrossRef]
- Mahajan, J.; Bonner, B.; Oganesyan, R.; Yeo, I.; Klemt, C.; Kwon, Y.-M. MARS MRI Characteristics of Adverse Local Tissue Reactions in Taper Corrosion of Metal-On-Polyethylene THA Differ from Metal-On-Metal THA. J. Arthroplast. 2020, 35, 3338–3342. [Google Scholar] [CrossRef]
- Marchica, D.; Gallazzi, E.; Materazzi, G.; Battaglia, G.A.; Zagra, L. MRI Findings, Metal Ion Levels and Clinical Outcome of a Complete Series of Large Metal on Metal THA: What’s Really Going on? HIP Int. 2018, 28, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Mulcahy, H.; Chew, F.S. Current Concepts of Hip Arthroplasty for Radiologists: Part 1, Features and Radiographic Assessment. Am. J. Roentgenol. 2012, 199, 559–569. [Google Scholar] [CrossRef]
- Mulcahy, H.; Chew, F.S. Current Concepts of Hip Arthroplasty for Radiologists: Part 2, Revisions and Complications. Am. J. Roentgenol. 2012, 199, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Müller, G.M.; Månsson, S.; Müller, M.F.; von Schewelov, T.; Nittka, M.; Ekberg, O.; Lundin, B. MR Imaging with Metal Artifact-Reducing Sequences and Gadolinium Contrast Agent in a Case-Control Study of Periprosthetic Abnormalities in Patients with Metal-on-Metal Hip Prostheses. Skelet. Radiol. 2014, 43, 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Nam, D.; Barrack, R.L.; Potter, H.G. What Are the Advantages and Disadvantages of Imaging Modalities to Diagnose Wear-Related Corrosion Problems? Clin. Orthop. Relat. Res. 2014, 472, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanò, C.L.; Petrosillo, N.; Argento, G.; Sconfienza, L.M.; Treglia, G.; Alavi, A. The Role of Imaging Techniques to Define a Peri-Prosthetic Hip and Knee Joint Infection: Multidisciplinary Consensus Statements. J. Clin. Med. 2020, 9, 2548. [Google Scholar] [CrossRef] [PubMed]
- Roth, T.D.; Maertz, N.A.; Parr, J.A.; Buckwalter, K.A.; Choplin, R.H. CT of the Hip Prosthesis: Appearance of Components, Fixation, and Complications. RadioGraphics 2012, 32, 1089–1107. [Google Scholar] [CrossRef]
- Schwaiger, B.J.; Gassert, F.T.; Suren, C.; Gersing, A.S.; Haller, B.; Pfeiffer, D.; Dangelmaier-Dawirs, J.; Roski, F.; von Eisenhart-Rothe, R.; Prodinger, P.M.; et al. Diagnostic Accuracy of MRI with Metal Artifact Reduction for the Detection of Periprosthetic Joint Infection and Aseptic Loosening of Total Hip Arthroplasty. Eur. J. Radiol. 2020, 131, 109253. [Google Scholar] [CrossRef] [PubMed]
- Zochowski, K.C.; Miranda, M.A.; Cheung, J.; Argentieri, E.C.; Lin, B.; Kaushik, S.S.; Burge, A.J.; Potter, H.G.; Koff, M.F. MRI of Hip Arthroplasties: Comparison of Isotropic Multiacquisition Variable-Resonance Image Combination Selective (MAVRIC SL) Acquisitions with a Conventional MAVRIC SL Acquisition. Am. J. Roentgenol. 2019, 213, W277–W286. [Google Scholar] [CrossRef] [PubMed]
- Choplin, R.H.; Henley, C.N.; Edds, E.M.; Capello, W.; Rankin, J.L.; Buckwalter, K.A. Total Hip Arthroplasty in Patients with Bone Deficiency of the Acetabulum. RadioGraphics 2008, 28, 771–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chughtai, M.; Mistry, J.B.; Diedrich, A.M.; Jauregui, J.J.; Elmallah, R.K.; Bonutti, P.M.; Harwin, S.F.; Malkani, A.L.; Kolisek, F.R.; Mont, M.A. Low Frequency of Early Complications with Dual-Mobility Acetabular Cups in Cementless Primary THA. Clin. Orthop. Relat. Res. 2016, 474, 2181–2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymanski, C.; Guériot, S.; Boniface, O.; Deladerrière, J.-Y.; Luneau, S.; Maynou, C. Taux de fracture des inserts de céramique « sandwich » dans un cotyle ATLAS IIITM: Étude de 144 prothèses totales de hanche de première intention à 74 mois de recul. Rev. Chir. Orthop. Traumatol. 2011, 97, 485–492. [Google Scholar] [CrossRef]
- Gulow, J.; Scholz, R.; Freiherr von Salis-Soglio, G. Short-stemmed endoprostheses in total hip arthroplasty. Orthopade 2007, 36, 353–359. [Google Scholar] [CrossRef]
- Tottas, S.; Ververidis, A.; Kougioumtzis, I.; Tilkeridis, K.; Tsigalou, C.; Karaglani, M.; Drosos, G. MINIMA Short Stem versus Standard Profemur (TL) Stem in Primary Total Hip Replacement: A Comparative Study. Cureus 2022, 14, e23771. [Google Scholar] [CrossRef] [PubMed]
- Pluot, E.; Davis, E.T.; Revell, M.; Davies, A.M.; James, S.L.J. Hip Arthroplasty. Part 1: Prosthesis Terminology and Classification. Clin. Radiol. 2009, 64, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Erschbamer, M.; Zdravkovic, V.; Erhardt, J.; Öhlschlegel, C.; Grob, K. Osteolytic Changes around Biodegradable Cement Restrictors in Hip Surgery. Acta Orthop. 2016, 87, 239–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusserow, A.; Ficklscherer, A.; Kreuz, P.C.; Finze, S.; Mittelmeier, W.; Jansson, V.; Milz, S.; Wegener, B. Importance of a Distal Centralizer in Experimental Malpositioning of Cemented Stems. A Biomechanical Study on Human Femora. Arch. Med. Sci. 2015, 11, 1324–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, E.; Olsson, C.; Kesteris, U.; Flivik, G. Is a Hollow Centralizer Necessary When Using a Polished, Tapered, Cemented Femoral Stem? Acta Orthop. 2017, 88, 377–382. [Google Scholar] [CrossRef] [Green Version]
- Fischer, T. Impact of Stem Design and Cementation on Postoperative Femoral Antetorsion in 227 Patients with Total Hip Arthroplasty (THA). Skelet. Radiol. 2020, 9, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Coden, G.; Matzko, C.; Hushmendy, S.; Macaulay, W.; Hepinstall, M. Impact of Acetabular Implant Design on Aseptic Failure in Total Hip Arthroplasty. Arthroplast. Today 2021, 7, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Raja, B.S.; Gowda, A.K.S.; Singh, S.; Ansari, S.; Kalia, R.B.; Paul, S. Comparison of Functional Outcomes and Complications of Cemented vs. Uncemented Total Hip Arthroplasty in the Elderly Neck of Femur Fracture Patients: A Systematic Review and Meta-Analysis. J. Clin. Orthop. Trauma 2022, 29, 101876. [Google Scholar] [CrossRef] [PubMed]
- Shim, B.-J.; Park, S.-J.; Park, C.H. The Wear Rate and Survivorship in Total Hip Arthroplasty Using a Third-Generation Ceramic Head on a Conventional Polyethylene Liner: A Minimum of 15-Year Follow-Up. Hip Pelvis 2022, 34, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Matharu, G.S.; Judge, A.; Eskelinen, A.; Murray, D.W.; Pandit, H.G. What Is Appropriate Surveillance for Metal-on-Metal Hip Arthroplasty Patients?: A Clinical Update. Acta Orthop. 2018, 89, 29–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fantino, O.; Tayot, O.; Sans, N.; Cyteval, C. Imaging of total hip arthroplasty: Normal and pathological imaging features, role of ultrasound, CT and MRI. J. Radiol. 2011, 92, 594–620. [Google Scholar] [CrossRef] [PubMed]
- Gillet, R.; Teixeira, P.; Bonarelli, C.; Coudane, H.; Sirveaux, F.; Louis, M.; Blum, A. Comparison of Radiographs, Tomosynthesis and CT with Metal Artifact Reduction for the Detection of Hip Prosthetic Loosening. Eur. Radiol. 2019, 29, 1258–1266. [Google Scholar] [CrossRef]
- Blum, A.; Gillet, R.; Rauch, A.; Urbaneja, A.; Biouichi, H.; Dodin, G.; Germain, E.; Lombard, C.; Jaquet, P.; Louis, M.; et al. 3D Reconstructions, 4D Imaging and Postprocessing with CT in Musculoskeletal Disorders: Past, Present and Future. Diagn. Interv. Imaging 2020, 101, S2211568420302254. [Google Scholar] [CrossRef]
- Fritz, J.; Lurie, B.; Miller, T.T.; Potter, H.G. MR Imaging of Hip Arthroplasty Implants. RadioGraphics 2014, 34, E106–E132. [Google Scholar] [CrossRef] [Green Version]
- Koff, M.F.; Burge, A.; Koch, K.M.; Potter, H.G. Magnetic Resonance Imaging Near Orthopaedic Hardware. J. Magn. Reson. Imaging 2017, 46, 24–39. [Google Scholar] [CrossRef]
- Guerini, H. IRM Des Ptohèses de Hanche. In La Hanche; SIMS; Sauramps: Montpellier, France, 2019; Volume 46, pp. 233–247. [Google Scholar]
- Lecerf, G.; Fessy, M.H.; Philippot, R.; Massin, P.; Giraud, F.; Flecher, X.; Girard, J.; Mertl, P.; Marchetti, E.; Stindel, E. Femoral Offset: Anatomical Concept, Definition, Assessment, Implications for Preoperative Templating and Hip Arthroplasty. Orthop. Traumatol. Surg. Res. 2009, 95, 210–219. [Google Scholar] [CrossRef]
- Meneghini, R.M. Investigation of the Unstable Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 1325–1327. [Google Scholar] [CrossRef]
- Geijer, M.; Kiernan, S.; Sundberg, M.; Flivik, G. Pre- and Postoperative Offset and Femoral Neck Version Measurements and Validation Using 3D Computed Tomography in Total Hip Arthroplasty. Acta Radiol. Open 2020, 9, 2058460120964911. [Google Scholar] [CrossRef] [PubMed]
- Tsang, H.; Bouz, T.; Kwan, K.; French, M. The Intraoperative Pelvic Radiograph during Total Hip Arthroplasty: Is It Reliable to Estimate Leg Length? Arthroplast. Today 2022, 16, 9–14. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.; Kernohan, G.; Fitzpatrick, C.; Hill, J.; Beverland, D. Perception of Imposed Leg Length Inequality in Normal Subjects. HIP Int. 2010, 20, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Renkawitz, T.; Weber, T.; Dullien, S.; Woerner, M.; Dendorfer, S.; Grifka, J.; Weber, M. Leg Length and Offset Differences above 5mm after Total Hip Arthroplasty Are Associated with Altered Gait Kinematics. Gait Posture 2016, 49, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-R.; Lee, J.-H.; Kim, D.-S.; Ryu, H.; Kim, J.; Yon, C.-J.; Lee, S.-W. The Comparison of Lower Extremity Length and Angle between Computed Radiography-Based Teleoroentgenogram and EOS® Imaging System. Diagnostics 2022, 12, 1052. [Google Scholar] [CrossRef] [PubMed]
- Ponsot, A. Analyse Du Positionnement Des Pièces Prothétiques et Complications Précoces. In La Hanche; SIMS; Sauramps: Montpellier, France, 2019; Volume 46, pp. 187–205. [Google Scholar]
- Fouque, O. Prothèse Totale de Hanche: Quelles Mesures Essentielles Le Radiologue Doit-Il Connaître? In Savoir Faire en Radiologie Ostéo-Articulaire: Hanche et Ceinture Pelvienne; Sauramps: Montpellier, France, 2018; Volume 20, pp. 211–223. [Google Scholar]
- Bendaya, S.; Anglin, C.; Lazennec, J.-Y.; Allena, R.; Thoumie, P.; Skalli, W. Good vs. Poor Results after Total Hip Arthroplasty: An Analysis Method Using Implant and Anatomic Parameters with the EOS Imaging System. J. Arthroplast. 2016, 31, 2043–2052. [Google Scholar] [CrossRef] [Green Version]
- Pour, A.E.; Schwarzkopf, R.; Patel, K.P.K.; Anjaria, M.P.; Lazennec, J.Y.; Dorr, L.D. How Much Change in Pelvic Sagittal Tilt Can Result in Hip Dislocation Due to Prosthetic Impingement? A Computer Simulation Study. J. Orthop. Res. 2021, 39, 2604–2614. [Google Scholar] [CrossRef]
- Lazennec, J.Y.; Clark, I.C.; Folinais, D.; Tahar, I.N.; Pour, A.E. What Is the Impact of a Spinal Fusion on Acetabular Implant Orientation in Functional Standing and Sitting Positions? J. Arthroplast. 2017, 32, 3184–3190. [Google Scholar] [CrossRef]
- Lazennec, J.Y.; Kim, Y.; Folinais, D.; Pour, A.E. Sagittal Spinopelvic Translation Is Combined with Pelvic Tilt During the Standing to Sitting Position: Pelvic Incidence Is a Key Factor in Patients Who Underwent THA. Arthroplast. Today 2020, 6, 672–681. [Google Scholar] [CrossRef]
- Lazennec, J.-Y.; Rousseau, M.-A.; Brusson, A.; Folinais, D.; Amel, M.; Clarke, I.; Pour, A.E. Total Hip Prostheses in Standing, Sitting and Squatting Positions: An Overview of Our 8 Years Practice Using the EOS Imaging Technology. Open Orthop. J. 2015, 9, 26–44. [Google Scholar] [CrossRef] [Green Version]
- Perronne, L.; Haehnel, O.; Chevret, S.; Wybier, M.; Hannouche, D.; Nizard, R.; Bousson, V. How Is Quality of Life after Total Hip Replacement Related to the Reconstructed Anatomy? A Study with Low-Dose Stereoradiography. Diagn. Interv. Imaging 2021, 102, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Fackler, C.D.; Poss, R. Dislocation in Total Hip Arthroplasties. Clin. Orthop. Relat. Res. 1980, 169–178. [Google Scholar] [CrossRef]
- Fischer, T.; Stern, C.; Fritz, B.; Zingg, P.O.; Pfirrmann, C.W.; Sutter, R. MRI Findings of Ischiofemoral Impingement after Total Hip Arthroplasty Are Associated with Increased Femoral Antetorsion. Acta Radiol. 2021, 63, 2841851211021044. [Google Scholar] [CrossRef]
- Pluot, E.; Davis, E.T.; Revell, M.; Davies, A.M.; James, S.L.J. Hip Arthroplasty. Part 2: Normal and Abnormal Radiographic Findings. Clin. Radiol. 2009, 64, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, H.C.; Beaulé, P.E.; Dorey, F.J.; Le Duff, M.J.; Campbell, P.A.; Gruen, T.A. Metal-on-Metal Hybrid Surface Arthroplasty: Two to Six-Year Follow-up Study. J. Bone Jt. Surg. Am. 2004, 86, 28–39. [Google Scholar] [CrossRef] [Green Version]
- Amstutz, C.; Duff, M.J.L.; Campbell, P.A.; Gruen, T.A.; Wisk, L.E. Clinical and Radiographic Results of Metal-on-Metal Hip Resurfacing with a Minimum Ten-Year Follow-Up. J. Bone Jt. Surg. Am. 2010, 92, 2663–2671. [Google Scholar] [CrossRef] [PubMed]
- Blum, A. Prothèse Douloureuse: L’interface Osseuse. In La Hanche; SIMS; Sauramps: Montpellier, France, 2019; Volume 46, pp. 215–231. [Google Scholar]
- Blum, A.; Gondim-Teixeira, P.; Gabiache, E.; Roche, O.; Sirveaux, F.; Olivier, P.; Coudane, H.; Raymond, A.; Louis, M.; Grandhaye, M.; et al. Developments in Imaging Methods Used in Hip Arthroplasty: A Diagnostic Algorithm. Diagn. Interv. Imaging 2016, 97, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Rogmark, C.; Nåtman, J.; Jobory, A.; Hailer, N.P.; Cnudde, P. The Association of Surgical Approach and Bearing Size and Type with Dislocation in Total Hip Arthroplasty for Acute Hip Fracture. Bone Jt. J. 2022, 104-B, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Pelissou, C.; Miquel, A.; Phan, C.; Paycha, F.; Sautet, A.; Arrivé, L. L’imagerie des prothèses de hanche: Complications communes et spécifiques des différents couples de frottements. J. D’imagerie Diagn. Interv. 2020, 3, 47–66. [Google Scholar] [CrossRef]
- Sutphen, S.A.; Lipman, J.D.; Jerabek, S.A.; Mayman, D.J.; Esposito, C.I. Treatment of Recurrent Dislocation after Total Hip Arthroplasty Using Advanced Imaging and Three-Dimensional Modeling Techniques: A Case Series. HSS J. 2020, 16, 245–255. [Google Scholar] [CrossRef] [Green Version]
- De Martino, I.; D’Apolito, R.; Waddell, B.S.; McLawhorn, A.S.; Sculco, P.K.; Sculco, T.P. Early Intraprosthetic Dislocation in Dual-Mobility Implants: A Systematic Review. Arthroplast. Today 2017, 3, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchetti, E.; Krantz, N.; Berton, C.; Bocquet, D.; Fouilleron, N.; Migaud, H.; Girard, J. Component Impingement in Total Hip Arthroplasty: Frequency and Risk Factors. A Continuous Retrieval Analysis Series of 416 Cup. Orthop. Traumatol. Surg. Res. 2011, 97, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazennec, J.Y.; Brusson, A.; Rousseau, M.A. Lumbar-Pelvic-Femoral Balance on Sitting and Standing Lateral Radiographs. Orthop. Traumatol. Surg. Res. 2013, 99, S87–S103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phan, D.; Bederman, S.S.; Schwarzkopf, R. The Influence of Sagittal Spinal Deformity on Anteversion of the Acetabular Component in Total Hip Arthroplasty. Bone Jt. J. 2015, 97-B, 1017–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsukayama, D.T.; Estrada, R.; Gustilo, R.B. Infection after Total Hip Arthroplasty. A Study of the Treatment of One Hundred and Six Infections. J. Bone Jt. Surg. Am. 1996, 78, 512–523. [Google Scholar] [CrossRef]
- Barrack, R.L.; Mulroy, R.D.; Harris, W.H. Improved Cementing Techniques and Femoral Component Loosening in Young Patients with Hip Arthroplasty. A 12-Year Radiographic Review. J. Bone Jt. Surg. Br. 1992, 74, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Huang, X.; Cheng, X.; Yang, D.; Huang, Y.; Zhou, Y. Evaluation of Peri-Prosthetic Radiolucent Lines Surrounding the Cementless Femoral Stem Using Digital Tomosynthesis with Metal Artifact Reduction: A Cadaveric Study in Comparison with Radiography and Computed Tomography. Quant. Imaging Med. Surg. 2020, 10, 1786–1800. [Google Scholar] [CrossRef]
- Hodgkinson, J.P.; Shelley, P.; Wroblewski, B.M. The Correlation between the Roentgenographic Appearance and Operative Findings at the Bone-Cement Junction of the Socket in Charnley Low Friction Arthroplasties. Clin. Orthop. Relat. Res. 1988, 228, 105–109. [Google Scholar] [CrossRef]
- Engh, C.A.; Massin, P.; Suthers, K.E. Roentgenographic Assessment of the Biologic Fixation of Porous-Surfaced Femoral Components. Clin. Orthop. Relat. Res. 1990, 257, 107–128. [Google Scholar] [CrossRef]
- Roche, O.; Girard, J.; Canovas, F.; Migaud, H.; Bonnomet, F.; Goldschild, M.; Le Béguec, P. Assessment of Fixation in Cementless Femoral Revision of Total Hip Arthroplasty: Comparison of the Engh Score versus Radiolucent Line Measurement. Int. Orthop. 2016, 40, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Canovas, F.; Putman, S.; Girard, J.; Roche, O.; Bonnomet, F.; Le Béguec, P. Global Radiological Score for Femoral Cementless Revision Stem. Int. Orthop. 2018, 42, 1007–1013. [Google Scholar] [CrossRef]
- Van den Wyngaert, T.; Paycha, F.; Strobel, K.; Kampen, W.U.; Kuwert, T.; van der Bruggen, W.; Gnanasegaran, G. SPECT/CT in Postoperative Painful Hip Arthroplasty. Semin. Nucl. Med. 2018, 48, 425–438. [Google Scholar] [CrossRef]
- Goswami, K.; Clarkson, S.; Phillips, C.D.; Dennis, D.A.; Klatt, B.A.; O’Malley, M.J.; Smith, E.L.; Gililland, J.M.; Pelt, C.E.; Peters, C.L.; et al. An Enhanced Understanding of Culture-Negative Periprosthetic Joint Infection with Next-Generation Sequencing: A Multicenter Study. J. Bone Jt. Surg. Am. 2022. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Zagra, L.; Andreata, M.; De Vecchi, E.; Gitto, S.; Sconfienza, L.M. Failed Total Hip Arthroplasty: Diagnostic Performance of Conventional MRI Features and Locoregional Lymphadenopathy to Identify Infected Implants. J. Magn. Reson. Imaging 2021, 53, 201–210. [Google Scholar] [CrossRef]
- Scharfenberger, A.; Clark, M.; Lavoie, G.; O’Connor, G.; Masson, E.; Beaupre, L.A. Treatment of an Infected Total Hip Replacement with the PROSTALAC System. Part 1: Infection Resolution. Can. J. Surg. 2007, 50, 24–28. [Google Scholar]
- Kwon, Y.-M.; MacAuliffe, J.; Arauz, P.G.; Peng, Y. Sensitivity and Specificity of Metal Ion Level in Predicting Adverse Local Tissue Reactions due to Head-Neck Taper Corrosion in Primary Metal-on-Polyethylene Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 3025–3029. [Google Scholar] [CrossRef]
- Kwon, Y.-M.; Tsai, T.-Y.; Leone, W.A.; Liow, M.H.L. Sensitivity and Specificity of Metal Ion Levels in Predicting “Pseudotumors” due to Taper Corrosion in Patients with Dual Taper Modular Total Hip Arthroplasty. J. Arthroplast. 2017, 32, 996–1000. [Google Scholar] [CrossRef]
- Kwon, Y.-M.; Khormaee, S.; Liow, M.H.L.; Tsai, T.-Y.; Freiberg, A.A.; Rubash, H.E. Asymptomatic Pseudotumors in Patients with Taper Corrosion of a Dual-Taper Modular Femoral Stem: MARS-MRI and Metal Ion Study. J. Bone Jt. Surg. Am. 2016, 98, 1735–1740. [Google Scholar] [CrossRef]
- Mistry, J.B.; Chughtai, M.; Elmallah, R.K.; Diedrich, A.; Le, S.; Thomas, M.; Mont, M.A. Trunnionosis in Total Hip Arthroplasty: A Review. J. Orthop. Traumatol. 2016, 17, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Petscavage-Thomas, J.M.; Ha, A. Best Practices: Best Imaging Modality for Surveillance of Metal-on-Metal Hip Arthroplasty. AJR Am. J. Roentgenol. 2021, 216, 311–317. [Google Scholar] [CrossRef]
- Nawabi, D.H.; Gold, S.; Lyman, S.; Fields, K.; Padgett, D.E.; Potter, H.G. MRI Predicts ALVAL and Tissue Damage in Metal-on-Metal Hip Arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Anderson, H.; Toms, A.P.; Cahir, J.G.; Goodwin, R.W.; Wimhurst, J.; Nolan, J.F. Grading the Severity of Soft Tissue Changes Associated with Metal-on-Metal Hip Replacements: Reliability of an MR Grading System. Skelet. Radiol. 2011, 40, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Matthies, A.K.; Skinner, J.A.; Osmani, H.; Henckel, J.; Hart, A.J. Pseudotumors Are Common in Well-Positioned Low-Wearing Metal-on-Metal Hips. Clin. Orthop. Relat. Res. 2012, 470, 1895–1906. [Google Scholar] [CrossRef] [Green Version]
- Hauptfleisch, J.; Pandit, H.; Grammatopoulos, G.; Gill, H.S.; Murray, D.W.; Ostlere, S. A MRI Classification of Periprosthetic Soft Tissue Masses (Pseudotumours) Associated with Metal-on-Metal Resurfacing Hip Arthroplasty. Skelet. Radiol. 2012, 41, 149–155. [Google Scholar] [CrossRef]
- Smeekes, C. Pseudotumor in Metal-on-Metal Hip Arthroplasty: A Comparison Study of Three Grading Systems with MRI. Skelet. Radiol. 2018, 47, 1099–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avasarala, S.K.; Ahsan, S.T. Bilateral Lower-Extremity Edema Caused by Iliopsoas Bursal Distention after Hip Arthroplasty. Tex. Heart Inst. J. 2016, 43, 550–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czuczman, G.J.; Mandell, J.C.; Khurana, B. Iliopsoas Bursal Extension of Lipohemarthrosis: A Novel Imaging Finding Associated with Hip Fracture. Skelet. Radiol. 2017, 46, 253–257. [Google Scholar] [CrossRef]
- El-Desouky, I.I.; Helal, A.H.; Mansour, A.M.R. Ten-Year Survival of Ceramic-on-Ceramic Total Hip Arthroplasty in Patients Younger than 60 Years: A Systematic Review and Meta-Analysis. J. Orthop. Surg. Res. 2021, 16, 679. [Google Scholar] [CrossRef]
- Rosinsky, P.J.; Bheem, R.; Meghpara, M.B.; Haden, M.; Shapira, J.; Maldonado, D.R.; Lall, A.C.; Domb, B.G. Asymptomatic Gluteal Tendinopathies Negatively Impact Outcomes of Total Hip Arthroplasty: A Propensity Score-Matched Study. J. Arthroplast. 2021, 36, 242–249. [Google Scholar] [CrossRef]
- Requicha, F.; Edwards, S.M.; Rickman, M.S.; Comley, A.S. Outcomes Analysis of Anterior and Lateral Approach for Open Repair of Hip Abductor Tendons. HIP Int. 2022, 11207000221103440. [Google Scholar] [CrossRef] [PubMed]
- Vasarhelyi, E.M.; Williams, H.A.; Howard, J.L.; Petis, S.; Barfett, J.; Lanting, B.A. The Effect of Total Hip Arthroplasty Surgical Technique on Postoperative Muscle Atrophy. Orthopedics 2020, 43, 361–366. [Google Scholar] [CrossRef]
- Wang, T.; Shao, L.; Xu, W.; Li, F.; Huang, W. Surgical Injury and Repair of Hip External Rotators in THA via Posterior Approach: A Three-Dimensional MRI-Evident Quantitative Prospective Study. BMC Musculoskelet. Disord. 2019, 20, 22. [Google Scholar] [CrossRef]
- Pfirrmann, C.W.A.; Notzli, H.P.; Dora, C.; Hodler, J.; Zanetti, M. Abductor Tendons and Muscles Assessed at MR Imaging after Total Hip Arthroplasty in Asymptomatic and Symptomatic Patients1. Radiology 2005, 235, 969–976. [Google Scholar] [CrossRef]
- Hasegawa, K.; Kabata, T.; Kajino, Y.; Inoue, D.; Tsuchiya, H. Periprosthetic Occult Fractures of the Acetabulum Occur Frequently During Primary THA. Clin. Orthop. Relat. Res. 2017, 475, 484–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Pandit, H.; Taylor, A.; Gill, H.; Murray, D.; Ostlere, S. Metal-on-Metal Hip Resurfacings—A Radiological Perspective. Eur. Radiol. 2011, 21, 485–491. [Google Scholar] [CrossRef] [Green Version]
- He, B.; Li, X.; Dong, R.; Tong, P.; Sun, J. A Multi-Center Retrospective Comparative Study of Third Generation Ceramic-on- Ceramic Total Hip Arthroplasty in Patients Younger than 45 Years with or without the Sandwich Liner: A Ten-Year Minimum. J. Orthop. Surg. 2022, 30, 10225536221109960. [Google Scholar] [CrossRef]
- ACR. ACR–SPR–SSR Practice Parameter for the Performance and Interpretation of Magnetic Resonance Imaging (MRI) of the Hip and Pelvis for Musculoskeletal Disorders. Practice Parameters and Technical Standards. Available online: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/mr-hip-pelvis.pdf (accessed on 10 January 2021).























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | Normal Value | Consequences of Mispositioning |
|---|---|---|
| Leg Length | < 0.5–1 cm of differences between both sides | Increased discrepancy: gluteal and iliopsoas muscles affection |
| Acetabular side | ||
| Frontal acetabular inclination | 40 ± 15° | - Decreased: hip abduction limitation |
| - Increased: dislocation risk | ||
| Sagittal acetabular inclination | 35–40 ± 10° in standing position | - Increased: posterior impingement, anterior dislocation |
| 52 ± 11° in sitting position | - Decreased: anterior impingement between the cup and the neck, posterior dislocation | |
| Acetabular anteversion | 5–25° | - Lack of anteversion or retroversion: posterior dislocation, iliopsoas impingement |
| - Excessive anteversion: anterior dislocation | ||
| Acetabular center of rotation position | Similar to the contralateral hip | Lateralized: dislocation risk |
| Femoral Offset | 41–44 mm (or similar to contralateral hip) | - Decreased: limping, mobility limitation, and dislocation by gluteal muscles weakness |
| - Increased: gluteal muscles pain and polyethylene wear | ||
| Femoral side | ||
| Femoral Stem position | Neutral or slight valgus | Periprosthetic fracture and stress reaction in case of varus |
| Femoral Neck Anteversion | 10–15° | - Increased: anterior dislocation and ischio-femoral impingement |
| - Decreased: posterior dislocation | ||
| Femoral Head | Centered or slightly inferiorly located | - Particle disease if located upwards (wear) |
| Stage | Radiological Aspect |
|---|---|
| A | Complete filling of the medullary canal |
| B | RLZ inferior to 50% of the cement-bone interface |
| C | RLZ of 50–99% of the cement-bone interface |
| D | Complete RLZ at the cement-bone interface |
| Type | Imaging and Operative Findings |
|---|---|
| I | Acetabular rim and columns intact |
| Almost complete host bone support of the component | |
| II | Superior migration inferior to 3 cm |
| Distorted acetabular rim withtout columns attempt | |
| Host bone support superior to 50% | |
| IIA | Superior and medial cavitation. Intact rim |
| IIB | Segmental supero-lateral defect (less than 1/3 of circumference) |
| IIC | Medial wall lysis with acetabular protrusion |
| III | Migration superior to 3 cm |
| IIIA | Missing bone in the 10 AM-2 PM positions, teardrop lsysis |
| Walls compromised | |
| Columns nonsupportive | |
| Superior migration | |
| IIIB | Missing bone in the 9 AM-5 PM positions, teardrop lysis |
| Walls compromised | |
| Columns nonsupportive | |
| Superior or medial migration | |
| Pelvic Discontinuity | Fracture line through columns |
| Obturator foramen asymetry on AP pelvis radiograph | |
| Superior and inferior hemipelvis separation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombard, C.; Gillet, P.; Germain, E.; Boubaker, F.; Blum, A.; Gondim Teixeira, P.A.; Gillet, R. Imaging in Hip Arthroplasty Management Part 2: Postoperative Diagnostic Imaging Strategy. J. Clin. Med. 2022, 11, 4416. https://doi.org/10.3390/jcm11154416
Lombard C, Gillet P, Germain E, Boubaker F, Blum A, Gondim Teixeira PA, Gillet R. Imaging in Hip Arthroplasty Management Part 2: Postoperative Diagnostic Imaging Strategy. Journal of Clinical Medicine. 2022; 11(15):4416. https://doi.org/10.3390/jcm11154416
Chicago/Turabian StyleLombard, Charles, Pierre Gillet, Edouard Germain, Fatma Boubaker, Alain Blum, Pedro Augusto Gondim Teixeira, and Romain Gillet. 2022. "Imaging in Hip Arthroplasty Management Part 2: Postoperative Diagnostic Imaging Strategy" Journal of Clinical Medicine 11, no. 15: 4416. https://doi.org/10.3390/jcm11154416