
Investigation of the Effect of Imatinib and Hydroxyurea Combination Therapy on Hematological Parameters and Gene Expression in Chronic Myeloid Leukemia (CML) Patients

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Cancer and Leukemia
1.2. Chronic Myeloid Leukemia (CML)
1.3. Treatment of CML
1.4. Genes Involved in CML
2. Materials and Methods
2.1. Ethical Approval
2.2. Consent to Participate
2.3. Patient Cohort Criteria
2.4. Patients’ Collection Sample and Ethical Consideration
2.5. Gene Expression
2.5.1. Extraction of Ribonucleic Acid (RNA) and Synthesis of Complementary Deoxyribonucleic Acid (cDNA)
2.5.2. Primer Design
2.5.3. Gene Expression Analysis
2.6. Statistical Analysis
3. Results
3.1. Patient Cohort Demographic Data
3.2. Gene Expression
3.2.1. BCL2 Expression
3.2.2. PP2A Expression
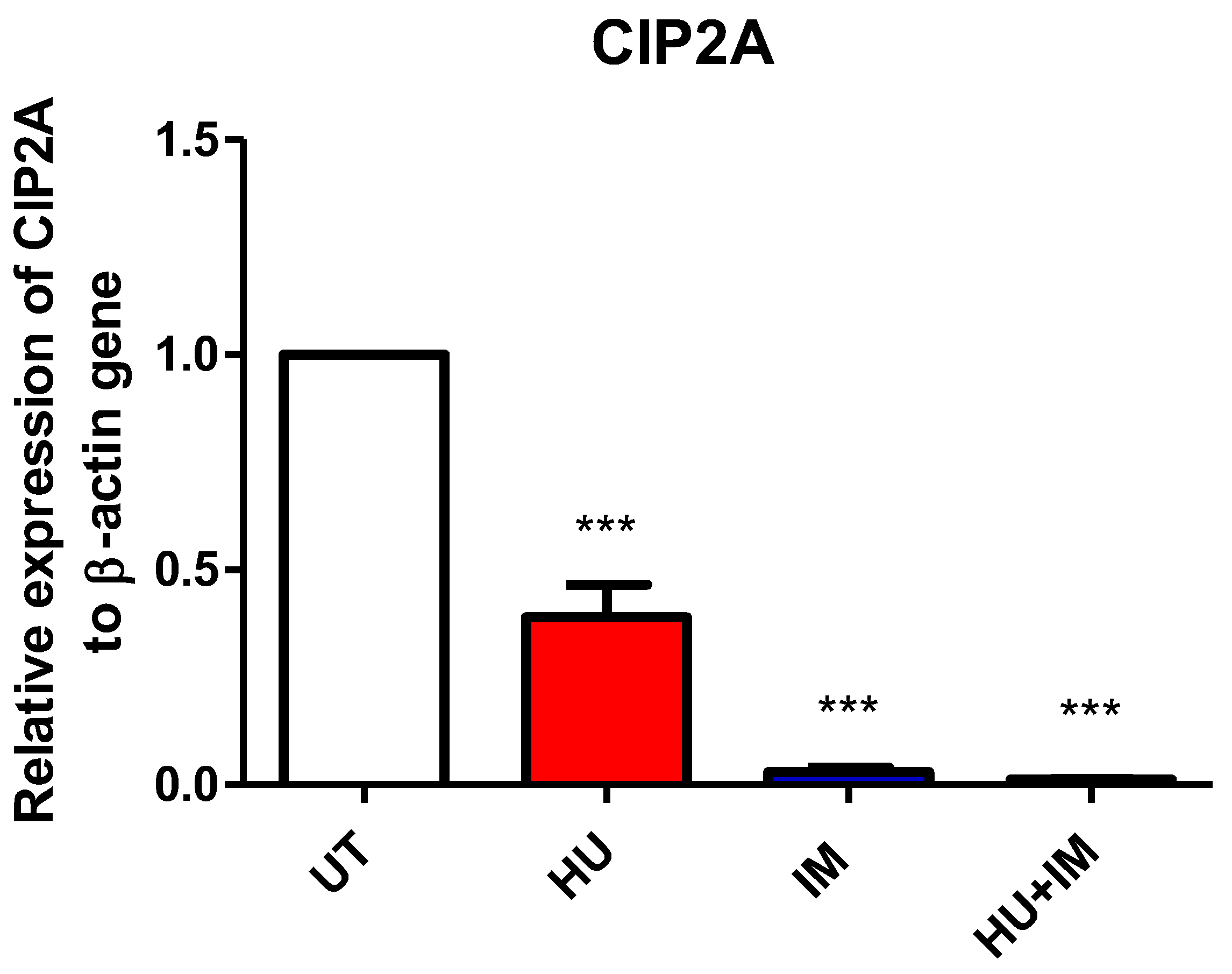
3.2.3. CIP2A Expression
3.2.4. WT1 Expression
3.3. Hematological Parameters for Study Patients
3.4. Correlation Analysis of Gene Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 2G TKI | Second-generation tyrosine kinase inhibitors |
| AP | Accelerated phase |
| Ara-C | Cytosine arabinoside |
| ATP | Adenosine triphosphate |
| B-ALL | B acute Lymphoblastic Leukemia |
| Baso | Basophils |
| BCL-2 | B-cell lymphoma 2 |
| BCR | B-cell receptor |
| BM | Bone marrow |
| BP | Blastic phase |
| cDNA | Complementary deoxyribonucleic acid |
| CGL | Chronic granulocytic leukemia |
| CIP2A | Cancerous inhibitor of protein phosphatase 2A |
| CML | Chronic myeloid leukemia |
| C-MYC | Cellular-Myelocytomatosis |
| CP | Chronic phase |
| DNA | Deoxyribonucleic acid |
| E2F1 | E2 promoter binding factor 1 |
| EDTA | Ethylenediamine tetra acetic acid |
| Eosino | Eosinophils |
| ERK1/2 | Extracellular signal-regulated kinases 1 and 2 |
| FDA | Food and Drug Administration |
| FISH | Fluorescence in Situ Hybridization |
| GRB2 | Growth Factor Receptor Bound Protein 2 |
| HB | Hemoglobin |
| Hb F | Fetal hemoglobin |
| HFLC | Lymphocytes with strong fluorescence |
| HHT | Hereditary hemorrhagic telangiectasia |
| HU | Hydroxyurea |
| IM | Imatinib |
| JAK2 | Janus kinase 2 |
| Lymph | Lymphocyte |
| MCH | Mean corpuscular hemoglobin |
| MCHC | Mean corpuscular hemoglobin Concentration |
| MCV | Mean cell volume |
| Mono | Monocytes |
| MPV | Mean platelet volume |
| MRD | Minimal residual disease |
| mRNA | Messenger ribonucleic acid |
| NCB | Normal cord blood |
| Neutro | Neutrophils |
| NRBC | Nucleated red blood cell |
| PADs’ | PP2A-activating drugs |
| PCR | Polymerase chain reaction |
| PCT | Plateletcrit |
| PCV | Packed Cell Volume |
| PDGFR | Platelet-derived growth factor |
| PDGFRA | Platelet-derived growth factor receptor A |
| PDW | Platelet distribution width |
| PLT | Platelet |
| PP1 | Protein phosphatase 1 |
| PP2 | Protein phosphatase 2A |
| RDW-CV | Red blood cell distribution width -cell volume |
| RDW-SD | Red blood cell distribution width—standard division |
| RNA | Ribonucleic acid |
| RNA Seq | RNA sequencing |
| RNR | Ribonucleotide reductase |
| RR M2 subunit | Ribonucleotide reductase regulatory subunit M2 |
| RT-qPCR | Quantitative reverse transcription—Polymerase chain reaction |
| RT-PCR | Reverse transcription- Polymerase chain reaction |
| SSC | Side scatter light |
| STAT | Signal transducer and activator of transcription 5 |
| TKI | Tyrosine kinase inhibitors |
| Tm | Melting temperatures |
| UT | Untreated |
| WBC | White blood cell |
| WHO | World health organization |
| WNR channels | White cell nucleated |
| WDF channels | WBC differential |
| WT1 | Wilms’ tumor protein |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, M.R.; Campbell, P.J.; Futreal, P.A. The cancer genome. Nature 2009, 458, 719–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awad, A.A.A.R. Assessment of Complete Blood Count among Patients Receiving Chemotherapy at Tumor Therapy and Cancer Research Center in Shendi Town. 2018. Available online: http://localhost:8080/xmlui/handle/123456789/539 (accessed on 1 July 2022).
- Chennamadhavuni, A.; Lyengar, V.; Shimanovsky, A. Leukemia. StatPearls. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560490/ (accessed on 1 July 2022).
- Bain, B.J. Rodak’s Hematology: Clinical Principles and Applications. By E.M. Keohane, L.J. Smith and J.M. Walenga (Eds), Elsevier, St Louis, 2016. Br. J. Haematol. 2017, 177, 662. [Google Scholar] [CrossRef] [Green Version]
- McKenzie, S.B.; Williams, J.L. Clinical Laboratory Hematology, 3rd ed.; Pearson PLC: London, UK, 2015. [Google Scholar]
- Mo, Y.; Wan, R.; Zhang, Q. Application of reverse transcription-PCR and real-time PCR in nanotoxicity research. Methods Mol. Biol. 2012, 926, 99–112. [Google Scholar] [CrossRef] [Green Version]
- Cortes, J.; Kantarjian, H. How I treat newly diagnosed chronic phase CML. Blood 2012, 120, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Suttorp, M.; Bornhäuser, M.; Metzler, M.; Millot, F.; Schleyer, E. Pharmacology and pharmacokinetics of imatinib in pediatric patients. Expert Rev. Clin. Pharmacol. 2018, 11, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Oertel, S.; Krempien, R.; Lindel, K.; Zabel, A.; Milker-Zabel, S.; Bischof, M.; Lipson, K.E.; Peschke, P.; Debus, J.; Abdollahi, A.; et al. Human glioblastoma and carcinoma xenograft tumors treated by combined radiation and imatinib (Gleevec®). Strahlenther. Und Onkol. 2006, 182, 400–407. [Google Scholar] [CrossRef]
- Delhi, I.G.; Battu, S.; Gandu, V.; Nenavathu, B.P. Simple spectrophotometric method for estimation of drugs using chloraminet and indigo caramine dye couple. Asian J. Biomed. Pharm. Sci. 2020, 10, 19–24. [Google Scholar] [CrossRef]
- Amraoui, N.; Meziane, M.; Gallouj, S.; Bono, W.; Abid, H.; Elmrini, A.; Mernissi, F.Z. Hydroxyurea-induced Amyopathic Dermatomyositis. J. Clin. Med. Res. 2021, 3, 1–7. [Google Scholar] [CrossRef]
- Santos, S.S.; Gomes, I.; Santos, D.; Vasconcelos Da Silva, C.; Cristina, E.; Cazedey, L. Qualitative Analysis of Hydroxyurea. Drug Anal. Res. 2020, 4, 18–21. [Google Scholar] [CrossRef]
- Saban, N.; Bujak, M. Hydroxyurea and hydroxamic acid derivatives as antitumor drugs. Cancer Chemother. Pharmacol. 2009, 64, 213–221. [Google Scholar] [CrossRef]
- Singh, A.; Xu, Y.J. The cell killing mechanisms of hydroxyurea. Genes 2016, 7, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junttila, M.R.; Puustinen, P.; Niemelä, M.; Ahola, R.; Arnold, H.; Böttzauw, T.; Ala-Aho, R.; Nielsen, C.; Ivaska, J.; Taya, Y.; et al. CIP2A Inhibits PP2A in human malignancies. Cell 2007, 130, 51–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimmino, A.; Calin, G.A.; Fabbri, M.; Iorio, M.V.; Ferracin, M.; Shimizu, M.; Wojcik, S.E.; Aqeilan, R.I.; Zupo, S.; Dono, M.; et al. miR-15 and miR-16 induce apoptosis by targeting BCL2. Proc. Natl. Acad. Sci. USA 2005, 102, 13944–13949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiyama, H. WT1 (Wilms’ tumor gene 1): Biology and cancer immunotherapy. Jpn. J. Clin. Oncol. 2010, 40, 377–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Cao, W.; Qin, S.; Zhang, T.; Zheng, J.; Dong, Y.; Ming, P.; Cheng, Q.; Lu, Z.; Guo, Y.; et al. Overexpression of CIP2A is associated with poor prognosis in multiple myeloma. Cancerous inhibitor of protein phosphatase 2A (CIP2A), an endogenous protein phosphatase 2A (PP2A) inhibitor. Signal Transduct. Target. Ther. 2017, 2, 17013. [Google Scholar] [CrossRef] [PubMed]
- Gotwals, P.; Cameron, S.; Cipolletta, D.; Cremasco, V.; Crystal, A.; Hewes, B.; Mueller, B.; Quaratino, S.; Sabatos-Peyton, C.; Petruzzelli, L.; et al. Prospects for combining targeted and conventional cancer therapy with immunotherapy. Nat. Rev. Cancer 2017, 17, 286–301. [Google Scholar] [CrossRef]
- Longley, D.B.; Johnston, P.G. Molecular mechanisms of drug resistance. J. Pathol. 2005, 205, 275–292. [Google Scholar] [CrossRef] [PubMed]
- Knox, S.S. From “omics” to complex disease: A systems biology approach to gene-environment interactions in cancer. Cancer Cell Int. 2010, 10, 11. [Google Scholar] [CrossRef] [Green Version]
- Kapor, S.; Čokić, V.; Santibanez, J.F. Mechanisms of Hydroxyurea-Induced Cellular Senescence: An oxidative stress connection? Oxidative Med. Cell. Longev. 2021, 2021, 7753857. [Google Scholar] [CrossRef]
- Alvarez, R.H.; Kantarjian, H.; Cortes, J.E. The biology of chronic myelogenous leukemia: Implications for Imatinib therapy. Semin. Hematol. 2007, 44, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.Z.; Mak, P.Y.; Mu, H.; Zhou, H.; Mak, D.H.; Schober, W.; Leverson, J.D.; Zhang, B.; Bhatia, R.; Huang, X.; et al. Combined targeting of BCL-2 and BCR-ABL tyrosine kinase eradicates chronic myeloid leukemia stem cells. Sci. Transl. Med. 2016, 8, 355ra117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, D.; Chen, M.; Su, J.; Liu, X.; Rothe, K.; Hu, K.; Forrest, D.L.; Eaves, C.J.; Morin, G.B.; Jiang, X. PP2A inhibition sensitizes cancer stem cells to ABL tyrosine kinase inhibitors in BCR-ABL+ human leukemia. Sci. Transl. Med. 2018, 10, eaan8735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Huang, T.; Sun, J.; Yu, Y.; Liu, Z.; Li, W.; Jia, J.; Chen, C. CIP2A is overexpressed and involved in the pathogenesis of chronic myelocytic leukemia by interacting with breakpoint cluster region-Abelson leukemia virus. Med. Oncol. 2014, 31, 112. [Google Scholar] [CrossRef]
- El-Menoufy, M.A.; Ahmed, M.A. Wilms’ tumor gene 1 expression can predict sudden disease progression to blast crisis in patients with chronic myeloid leukemia receiving imatinib therapy. Egypt. J. Haematol. 2018, 43, 38. [Google Scholar] [CrossRef]
- Latagliata, R.; Breccia, M.; Carmosino, I.; Cannella, L.; De Cuia, R.; Diverio, D.; Frustaci, A.; Loglisci, G.; Mancini, M.; Santopietro, M.; et al. “Real-life” results of front-line treatment with Imatinib in older patients (≥65 years) with newly diagnosed chronic myelogenous leukemia. Leuk. Res. 2010, 34, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Catellani, S.; Pierri, I.; Gobbi, M.; Poggi, A.; Zocchi, M.R. Imatinib treatment induces CD5+ B Lymphocytes and IgM natural antibodies with anti-leukemic reactivity in patients with chronic myelogenous leukemia. PLoS ONE 2011, 6, e18925. [Google Scholar] [CrossRef]
- Lazzaro, A.; Bernuzzi, P.; Trabacchi, E.; Vallisa, D.; Arcari, A.; Bertè, R.; Moroni, C.F.; Anselmi, E.; Cavanna, L. Imatinib-related neutropenia in chronic-phase chronic myelogenous leukaemia: Safety and efficacy of granulocyte-colony-stimulating factor (Filgrastim) Use. Blood 2005, 106, 4864. [Google Scholar] [CrossRef]
- Akay, O.M.; Mutlu, F.; Gülbaş, Z. Platelet dysfunction in patients with chronic myeloid leukemia: Does Imatinib mesylate improve it? Turk. J. Hematol. 2016, 33, 127. [Google Scholar] [CrossRef] [PubMed]
- Iriyama, N.; Hatta, Y.; Kobayashi, S.; Uchino, Y.; Miura, K.; Kurita, D.; Kodaira, H.; Takahashi, H.; Iizuka, Y.; Inoue, M.; et al. Higher red blood cell distribution width is an adverse prognostic factor in chronic-phase chronic myeloid leukemia patients treated with tyrosine kinase inhibitors. Anticancer Res. 2015, 35, 5473–5478. [Google Scholar]
- Perrotti, D.; Neviani, P. Protein phosphatase 2A (PP2A), a drugable tumor suppressor in Ph1(+) leukemias. Cancer Metastasis Rev. 2008, 27, 159–168. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Forward | Reverse |
|---|---|---|
| B-actin | CGG GAC CTG ACT GAC TAC C | TGA AGG TAG TTT CGT GGA TGC |
| Bcl2 | ATC GCC CTG TGG ATG ACT GAG T | GCC AGG AGA AAT CAA ACA GAG GC |
| Cip2a | TGC GGC ACT TGG AGG TAA TTT | AGC TCT ACA AGG CAA CTC AAG C |
| Pp2a | GGT GGT CTC TCG CCA TCT ATA G | CTG GAT CTG ACC ACA GCA AGT C |
| Wt1 | GAA AAT AGG GGA TGG TCC AG | CAA TGG ATT TCC TCA CCC AG |
| Gene Expression | Treatments | ||
|---|---|---|---|
| HU | IM | Combination | |
| PP2A vs. CIP2A | −0.18433 | −0.30453 | −0.20241 |
| BCL2 vs. CIP2A | −0.33206 | 0.991093 | −0.40355 |
| BCL2 vs. PP2A | −0.22445 | −0.35362 | −0.64193 |
| WT1 vs. PP2A | 0.324249 | −0.54996 | −0.76978 |
| WT1 vs. CIP2A | −0.6094 | 0.939511 | 0.509226 |
| WT1 vs. BCL2 | −0.34197 | 0.967696 | 0.579199 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Amleh, E.K.; Al-Sanabra, O.M.; Alqaisi, K.M.; Alqaraleh, M.; Al-Nahal, J.; Hamadneh, L.; Malki, M.I.; Alhmoud, J.F. Investigation of the Effect of Imatinib and Hydroxyurea Combination Therapy on Hematological Parameters and Gene Expression in Chronic Myeloid Leukemia (CML) Patients. J. Clin. Med. 2022, 11, 4954. https://doi.org/10.3390/jcm11174954
Al-Amleh EK, Al-Sanabra OM, Alqaisi KM, Alqaraleh M, Al-Nahal J, Hamadneh L, Malki MI, Alhmoud JF. Investigation of the Effect of Imatinib and Hydroxyurea Combination Therapy on Hematological Parameters and Gene Expression in Chronic Myeloid Leukemia (CML) Patients. Journal of Clinical Medicine. 2022; 11(17):4954. https://doi.org/10.3390/jcm11174954
Chicago/Turabian StyleAl-Amleh, Esraa K., Ola M. Al-Sanabra, Khalid M. Alqaisi, Moath Alqaraleh, Jumana Al-Nahal, Lama Hamadneh, Mohammed Imad Malki, and Jehad F. Alhmoud. 2022. "Investigation of the Effect of Imatinib and Hydroxyurea Combination Therapy on Hematological Parameters and Gene Expression in Chronic Myeloid Leukemia (CML) Patients" Journal of Clinical Medicine 11, no. 17: 4954. https://doi.org/10.3390/jcm11174954