
Screening of Gestational Diabetes and Its Risk Factors: Pregnancy Outcome of Women with Gestational Diabetes Risk Factors According to Glycose Tolerance Test Results


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
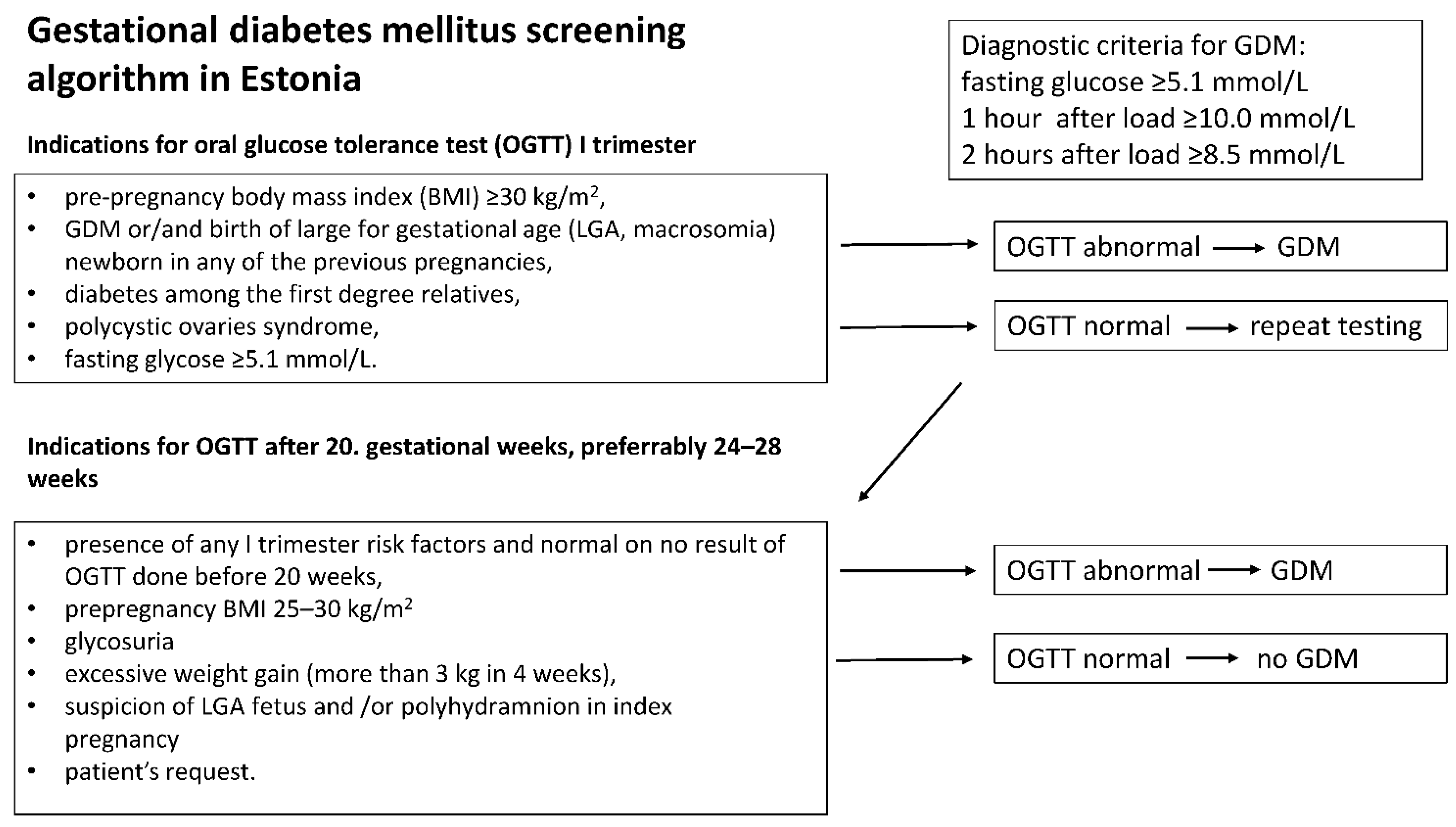
2.2. Patient Grouping and Diagnostic Criteria
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. The Prevalence of Gestational Diabetes and Its Risk Factors Has Increased during Seven Years
3.2. The Largest Babies Are Born to Mothers Who Undergo Correct GDM Screening Algorithm
3.3. Comparison of Maternal Characteristics and Pregnancy Course among High-Risk Pregnant Women with Normal or No OGTT Result
3.4. Pregnancy Course and Outcome of Women with GDM According to Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hyperglycemia in pregnancy: International Diabetes Federation. In IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019.
- He, X.J.; Qin, F.Y.; Hu, C.L.; Zhu, M.; Tian, C.Q.; Li, L. Is gestational diabetes mellitus an independent risk factor for macrosomia: A meta-analysis? Arch Gynecol. Obstet. 2015, 291, 729–735. [Google Scholar] [CrossRef]
- HAPO Study Cooperative Research Group. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Int. J. Gynaecol. Obstet. 2002, 78, 69–77. [Google Scholar] [CrossRef]
- HAPO Study Cooperative Research Group; Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Dyer, A.R.; Trimble, E.R.; Sheridan, B.; Hod, M.; Chen, R.; Yogev, Y.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar]
- Auvinen, A.M.; Luiro, K.; Jokelainen, J.; Järvelä, I.; Knip, M.; Auvinen, J.; Tapanainen, J.S. Type 1 and type 2 diabetes after gestational diabetes: A 23-year cohort study. Diabetologia 2020, 63, 2123–2128. [Google Scholar] [CrossRef]
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful dietary patterns and type 2 diabetes mellitus risk among women with a history of gestational diabetes mellitus. Arch. Intern. Med. 2012, 172, 1566–1572. [Google Scholar] [CrossRef]
- Benhalima, K.; Mathieu, C.; Van Assche, A.; Damm, P.; Devlieger, R.; Mahmood, T.; Dunne, F. Survey by the European Board and College of Obstetrics and Gynaecology on screening for gestational diabetes in Europe. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 201, 197–202. [Google Scholar] [CrossRef]
- Minschart, C.; Beunen, K.; Benhalima, K. An Update on Screening Strategies for Gestational Diabetes Mellitus: A Narrative Review. Diabetes Metab. Syndr. Obes. 2021, 14, 3047–3076. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- Benhalima, K.; Van Crombrugge, P.; Moyson, C.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Maes, T.; Dufraimont, E.; De Block, C.; et al. Risk factor screening for gestational diabetes mellitus based on the 2013 WHO criteria. Eur. J. Endocrinol. 2019, 180, 353–363. [Google Scholar] [CrossRef]
- Diabetes in Pregnancy: Management from Preconception to the Postnatal Period: NICE Guideline. Updated: 16 December. Available online: https://www.nice.org.uk/guidance/ng3/chapter/Recommendations (accessed on 13 June 2021).
- Yamamoto, J.M.; Kellett, J.E.; Balsells, M.; García-Patterson, A.; Hadar, E.; Solà, I.; Gich, I.; van der Beek, E.M.; Castañeda-Gutiérrez, E.; Heinonen, S.; et al. Gestational Diabetes Mellitus and Diet: A Systematic Review and Meta-analysis of Randomized Controlled Trials Examining the Impact of Modified Dietary Interventions on Maternal Glucose Control and Neonatal Birth Weight. Diabetes Care 2018, 41, 1346–1361. [Google Scholar] [CrossRef]
- Thayer, S.M.; Lo, J.O.; Caughey, A.B. Gestational Diabetes: Importance of Follow-up Screening for the Benefit of Long-term Health. Obstet. Gynecol. Clin. N. Am. 2020, 47, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Avalos, G.E.; Owens, L.A.; Dunne, F.; ATLANTIC DIP Collaborators. Applying current screening tools for gestational diabetes mellitus to a European population: Is it time for change? Diabetes Care 2013, 36, 3040–3044. [Google Scholar] [CrossRef] [PubMed]
- Kirss, A.; Lauren, L.; Rohejärv, M.; Rull, K. Gestatsioonidiabeet: Riskitegurid, esinemissagedus, perinataalne tulem ja sõeluuringu vastavus juhendile Tartu Ülikooli Kliinikumi naistekliinikus ajavahemikul 01.01.2012–19.06. East Arst 2015, 94, 75–82. (In Estonian) [Google Scholar]
- Ratnik, K.; Rull, K.; Hanson, E.; Kisand, K.; Laan, M. Single-Tube Multimarker Assay for Estimating the Risk to Develop Preeclampsia. J. Appl. Lab. Med. 2020, 5, 1156–1171. [Google Scholar] [CrossRef]
- Kikas, T.; Inno, R.; Ratnik, K.; Rull, K.; Laan, M. C-allele of rs4769613 Near FLT1 Represents a High-Confidence Placental Risk Factor for Preeclampsia. Hypertension 2020, 76, 884–891. [Google Scholar] [CrossRef]
- Hanson, E.; Rull, K.; Ratnik, K.; Vaas, P.; Teesalu, P.; Laan, M. Value of soluble fms-like tyrosine kinase-1/placental growth factor test in third trimester of pregnancy for predicting preeclampsia in asymptomatic women. J. Perinat. Med. 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Vaas, P.; Rull, K.; Põllumaa, S.; Kirss, A.; Meigas, D. Guideline for Antenatal Care (Raseduse Jälgimise Juhend). Estonian Gynaecologists Society 2011; vEstonian. Available online: https://www.ens.ee/ravijuhendid (accessed on 23 June 2019).
- Villar, J.; Papageorghiou, A.T.; Pang, R.; Ohuma, E.O.; Ismail, L.C.; Barros, F. The likeness of fetal growth and new-born size across non-isolated populations in the INTERGROWTH-21st Project: The Fetal Growth Longitudinal Study and Newborn Cross-Sectional Study. Lancet 2014, 2, 781–792. [Google Scholar]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef]
- Rasmussen, K.M.; Abrams, B.; Bodnar, L.M.; Butte, N.F.; Catalano, P.M.; Maria Siega-Riz, A. Recommendations for weight gain during pregnancy in the context of the obesity epidemic. Obstet. Gynecol. 2010, 116, 1191–1195. [Google Scholar] [CrossRef]
- Muin, D.A.; Pfeifer, B.; Helmer, H.; Oberaigner, W.; Leitner, H.; Kiss, H.; Neururer, S. Universal gestational diabetes screening and antepartum stillbirth rates in Austria-A population-based study. Acta Obstet. Gynecol. Scand. 2022, 101, 396–404. [Google Scholar] [CrossRef]
- Koivunen, S.; Viljakainen, M.; Männistö, T.; Gissler, M.; Pouta, A.; Kaaja, R.; Eriksson, J.; Laivuori, H.; Kajantie, E.; Vääräsmäki, M. Pregnancy outcomes according to the definition of gestational diabetes. PLoS ONE 2020, 15, e0229496. [Google Scholar] [CrossRef] [PubMed]
- Mohr Sasson, A.; Shats, M.; Goichberg, Z.; Mazaki-Tovi, S.; Morag, I.; Hendler, I. Oral glucose tolerance test for suspected late onset gestational diabetes. J. Matern. Fetal. Neonatal. Med. 2021, 34, 3928–3932. [Google Scholar] [CrossRef] [PubMed]
- Mo, X.; Gai Tobe, R.; Takahashi, Y.; Arata, N.; Liabsuetrakul, T.; Nakayama, T.; Mori, R. Economic Evaluations of Gestational Diabetes Mellitus Screening: A Systematic Review. J. Epidemiol. 2021, 31, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Xiang, A.H.; Kjos, S.L.; Takayanagi, M.; Trigo, E.; Buchanan, T.A. Detailed physiological characterization of the development of type 2 diabetes in Hispanic women with prior gestational diabetes mellitus. Diabetes 2010, 59, 2625–2630. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Ratner, R.E.; Christophi, C.A.; Metzger, B.E.; Dabelea, D.; Bennett, P.H.; Pi-Sunyer, X.; Fowler, S.; Kahn, S.E.; Diabetes Prevention Program Research Group. Prevention of diabetes in women with a history of gestational diabetes: Effects of metformin and lifestyle intervention. J. Clin. Endocrinol. Metab. 2008, 93, 4774–4779. [Google Scholar] [CrossRef]
- Zhao, R.; Xu, L.; Wu, M.L.; Huang, S.H.; Cao, X.J. Maternal pre-pregnancy body mass index, gestational weight gain influence birth weight. Women Birth 2018, 31, e20–e25. [Google Scholar] [CrossRef]
- Usta, A.; Usta, C.S.; Yildiz, A.; Ozcaglayan, R.; Dalkiran, E.S.; Savkli, A.; Taskiran, M. Frequency of fetal macrosomia and the associated risk factors in pregnancies without gestational diabetes mellitus. Pan Afr. Med. J. 2017, 26, 62. [Google Scholar] [CrossRef]
- Lin, L.H.; Lin, J.; Yan, J.Y. Interactive Affection of Pre-Pregnancy Overweight or Obesity, Excessive Gestational Weight Gain and Glucose Tolerance Test Characteristics on Adverse Pregnancy Outcomes Among Women with Gestational Diabetes Mellitus. Front. Endocrinol. 2022, 13, 942271. [Google Scholar] [CrossRef]
- Rasmussen, L.; Poulsen, C.W.; Kampmann, U.; Smedegaard, S.B.; Ovesen, P.G.; Fuglsang, J. Diet and Healthy Lifestyle in the Management of Gestational Diabetes Mellitus. Nutrients 2020, 12, 3050. [Google Scholar] [CrossRef]
- Peaceman, A.M.; Clifton, R.G.; Phelan, S.; Gallagher, D.; Evans, M.; Redman, L.M.; Knowler, W.C.; Joshipura, K.; Haire-Joshu, D.; Yanovski, S.Z.; et al. Lifestyle Interventions Limit Gestational Weight Gain in Women with Overweight or Obesity: LIFE-Moms Prospective Meta-Analysis. Obesity 2018, 26, 1396–1404. [Google Scholar] [CrossRef] [PubMed]
- Dodd, J.M.; Louise, J.; Deussen, A.R.; Grivell, R.M.; Dekker, G.; McPhee, A.J.; Hague, W. Effect of metformin in addition to dietary and lifestyle advice for pregnant women who are overweight or obese: The GRoW randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 15–24. [Google Scholar] [CrossRef]
- Zhu, Y.; Hedderson, M.M.; Sridhar, S.; Xu, F.; Feng, J.; Ferrara, A. Poor diet quality in pregnancy is associated with increased risk of excess fetal growth: A prospective multi-racial/ethnic cohort study. Int. J. Epidemiol. 2019, 48, 423–432. [Google Scholar] [CrossRef]
- Han, S.; Crowther, C.A.; Middleton, P. Interventions for pregnant women with hyperglycaemia not meeting gestational diabetes and type 2 diabetes diagnostic criteria. Cochrane Database Syst. Rev. 2012, 1, CD009037. [Google Scholar] [CrossRef] [PubMed]
- Munda, A.; Starčič Erjavec, M.; Molan, K.; Ambrožič Avguštin, J.; Žgur-Bertok, D.; Pongrac Barlovič, D. Association between pre-pregnancy body weight and dietary pattern with large-for-gestational-age infants in gestational diabetes. Diabetol. Metab. Syndr. 2019, 11, 68. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter 2 | I (n = 1073) | II (n = 2176) | III (n = 1772) | p Value 6 | ||
|---|---|---|---|---|---|---|
| Basic characteristics | I vs. II | I vs. III | II vs. III | |||
| Maternal age (years) | 28 (20–38) | 28 (20–38) | 29 (21–38) | n.s | 1.9 × 10−7 | 1.2 × 10−6 |
| Pre-pregnancy BMI (kg/m2) | 22.5 (18.0–32.8) | 22.3 (18.1–31.5) | 22.7 (18.5–33.6) | n.s | n.s | 1.9 × 10−5 |
| Multiparous 3 | NA | 1190 (54.7%) | 1114 (62.9%) | NA | NA | 2.2 × 10−7 |
| GDM risk factors | ||||||
| Risk factor carriers | 467 (43.5%) | 1227 (56.4%) | 1025 (57.8%) | 5.1 × 10−12 | 1.2 × 10−13 | n.s |
| Correctly tested among risk factor carriers | 291 (62.3%) | 702 (57.2%) | 787 (76.8%) | n.s | 1.5 × 10−4 | 3.5 × 10−9 |
| BMI 25–30 kg/m2 n (% of carriers) | 198 (42.4%) | 394 (32.1%) | 320 (31.2%) | n.s | n.s | n.s |
| BMI >30 kg/m2 | 92 (19.7%) | 185 (15.1%) | 210 (20.5%) | n.s | n.s | 2.0 × 10−4 |
| GDM previously 3 | 13 (2.8%) | 26 (2.1%) | 28 (2.7%) | n.s | n.s | n.s |
| Previous baby 4500 g | 30 (6.4%) | 36 (2.9%) | 39 (3.8%) | n.s | n.s | n.s |
| DM among first degree relatives | 78 (16.7%) | 224 (18.3%) | 161 (15.7%) | n.s | n.s | n.s |
| PCOS | 24 (5.1%) | 24 (2.0%) | 9 (0.9%) | n.s | 3.0 × 10−5 | n.s |
| Fasting glycose >5.1 mmol/L | 48 (10.3%) | 471 (38.4%) | 235 (22.9%) | 3.3 × 10−36 | 1.6 × 10−14 | 6.0 × 10−10 |
| Polyhydramnion | 19 (4.1%) | 42 (3.4%) | 40 (3.9%) | n.s | n.s | n.s |
| Other 4 | 68 (14.6%) | 116 (9.5%) | 245 (23.9%) | n.s | 6.1 × 10−10 | 3.2 × 10−20 |
| Pregnancy outcome | ||||||
| Gestational diabetes | 56 (5.2%) | 124 (5.7%) | 243 (13.7%) | n.s | 8.05 × 10−13 | 6.4 × 10−18 |
| Preterm birth | 50 (4.7%) | 110 (5.1%) | 87 (4.9%) | n.s | n.s | n.s |
| Gestational age at delivery (days) | 280 (259–287) | 281 (258–293) | 279 (259–291) | 1.38 × 10−17 | 3.69 × 10−10 | n.s |
| Birthweight (grams) | 3596 (2680–4360) | 3569 (2680–4366) | 3590 (2660–4302) | n.s | n.s | n.s |
| Cesarean section | 181 (16.9%) | 363 (16.7%) | 342 (19.3%) | n.s | n.s | n.s |
| LGA 5 | 202 (18.8%) | 341 (15.7%) | 286 (16.1%) | n.s | n.s | n.s |
| LGA + GDM | 23 (11.4%) | 30 (8.8%) | 57 (9.4%) | |||
| SGA 5 | 17 (1.6%) | 52 (2.4%) | 43 (2.4%) | n.s | n.s | n.s |
| Risk Factor | Carrier (n) | Tested Correctly (n/% of Carriers) | GDM (n/% of Correctly Tested) | OR (95% CI) | p-Value 3 |
|---|---|---|---|---|---|
| BMI 25.0–29.9 kg/m2 | 1385 | 857 (61.9%) | 252 (29.4%) | 1.7 (1.4–2.2) | 3.2 × 10−6 |
| BMI ≥ 30.0 kg/m2 | 482 | 362 (75.1%) | 139 (62.3%) | 6.3 (5.0–8.9) | 2.9 × 10−47 |
| GDM in previous pregnancy | 67 | 59 (88.1%) | 36 (62.7%) | 12.5 (7.5–20.6) | 6.0 × 10−21 |
| LGA 2 in previous pregnancy | 105 | 88 (83.8%) | 32 (38.2%) | 4.7 (3.1–7.2) | 3.0 × 10−10 |
| PCOS | 57 | 41 (71.9%) | 14 (53.3%) | 3.6 (2.0–6.9) | 2.4 × 10−4 |
| DM in relatives | 463 | 305 (65.9%) | 78 (25.6%) | 2.5 (1.9–3.2) | 6.1 × 10−10 |
| Fasting glycose >5.1 mmol/L | 755 | 436 (57.7%) | 175 (40.1%) | 5.0 (4.0–6.1) | 2.0 × 10−44 |
| Polyhydramnion | 97 | 63 (64.9%) | 16 (26.2%) | 2.1 (1.2–3.6) | 1.4 × 10−2 |
| Other | 431 | 402 (93.3%) | 59 (14.7%) | 1.8 (1.3–2.4) | 2.1 × 10−4 |
| Outcome 1 | Low Risk Pregnancies 5 | High Risk Pregnancies | Pairwise Comparisons | ||
|---|---|---|---|---|---|
| (Group 1) | No OGTT (Group 2) | OGTT Normal (Group 3) | GDM (Group 4) | Between Groups 6 p < 7.6 × 10−4 | |
| Number of women | 2302 | 939 | 1357 | 423 | |
| GA at delivery (days) | 280 (259–292) | 280 (255–292) | 280 (260–293) | 276 (252–289) | 1 vs. 4, 2 vs. 4, 3 vs. 4 |
| Birthweight (grams) | 3502 (2644–4233) | 3576 (2642–4320) | 3705 (2808–4468) | 3635 (2695–4430) | 1 vs. 2, 1 vs. 3, 1 vs. 4, 2 vs. 3 |
| Birth centile | 70.7 (13.7–97.3) | 75.7 (18.4–98.2) | 82.2 (25.0–99.3) | 82.6 (26.5–99.3) | 1 vs. 2, 1 vs. 3, 1 vs. 4, 2 vs. 3, 2 vs. 4 |
| LGA 2 | 243 (10.5%) | 160 (17.1%) | 315 (23.2%) | 110 (26.0%) | 1 vs. 2, 1 vs. 3, 1 vs. 4, 2 vs. 3, 2 vs. 4 |
| SGA 2 | 70 (3.0%) | 15 (1.6%) | 23 (1.7%) | 4 (0.95%) | n.s |
| Cesarean section | 322 (14.0%) | 175 (18.7%) | 274 (20.2%) | 114 (27.0%) | 1 vs. 3, 1 vs. 4; 2 vs. 4 |
| Preterm delivery | 104 (4.5%) | 55 (5.9%) | 58 (4.3%) | 27 (6.4%) | n.s |
| Shoulder dystocia 3,4 | 6/1468 (0.4%) | 3/627 (0.5%) | 6/883 (0.7%) | 1/266 (0.4%) | n.s |
| Perineal rupture ≥3 grade 3,4 | 14/1468 (1.0%) | 3/627 (0.5%) | 9/883 (1.0%) | 2/266 (0.8%) | n.s |
| Preeclampsia | 23 (1.04%) | 23 (2.5%) | 25 (1.8%) | 11 (2.6%) | 1 vs. 2, 1 vs. 3, 1 vs. 4 |
| Gestational hypertension 4 | 20/1699 (1.2%) | 26 (3.4%) | 50 (4.5%) | 25 (6.8%) | 1 vs. 4 |
| Outcome | Group | Number of Women | OR (95% CI) | AOR (95% CI) |
|---|---|---|---|---|
| LGA newborn 1,2 | ||||
| Low risk | 243 | 1 | 1 | |
| No OGTT | 160 | 1.8 (1.4–2.2) *** | 1.6 (1.2–2.2) *** | |
| Normal OGTT | 315 | 2.6 (2.1–3.1) *** | 2.3 (1.8–3.0) *** | |
| GDM | 110 | 3.0 (2.3–3.9) *** | 2.4 (1.7–3.4) *** | |
| SGA 2,3 | ||||
| Low risk | 70 | 1 | 1 | |
| No OGTT | 15 | 0.5 (0.3–0.9) * | 0.6 (0.3–1.1) | |
| Normal OGTT | 23 | 0.5 (0.3–0.9) * | 0.6 (0.4–1.0) * | |
| GDM | 4 | 0.3 (0.1–0.8) * | 0.3 (0.1–0.9) * | |
| Preeclampsia 4 | ||||
| Low risk | 23 | 1 | 1 | |
| No OGTT | 23 | 2.5 (1.4–4.5) ** | 1.4 (0.7–2.7) | |
| Normal OGTT | 25 | 1.9 (1.2–3.3) * | 1.1 (0.6–2.1) | |
| GDM | 11 | 2.6 (1.3–5.5) * | 1.3 (0.5–3.1) | |
| Cesarean Section 5 | ||||
| Low risk | 322 | 1 | 1 | |
| No OGTT | 175 | 1.4 (1.2–1.7) ** | 1.2 (0.9–1.5) | |
| Normal OGTT | 274 | 1.6 (1.3–1.9) *** | 1.3 (1.1–1.7) * | |
| GDM | 114 | 2.3 (1.8–2.9) *** | 1.5 (1.1–2.1) * |
| OGTT Normal N = 1357 | No OGTT N = 939 | p-Value 5 | |
|---|---|---|---|
| Basic characteristics1 | |||
| Age (years) | 28 (20–38) | 29 (21–39) | n.s |
| BMI (kg/m2) | 24.4 (18.7–34.6) | 25.3 (18.6–32.9) | n.s |
| Multiparous 2 | 48.5% | 49.3% | n.s |
| Risk factorsn (% of carriers) | |||
| Previous baby 4500 g | 60 (4.4%) | 13 (1.4%) | 1.2 × 10−4 |
| GDM previously | 25 (1.8%) | 4 (0.4%) | n.s |
| DM among first degree relatives | 243 (17.9%) | 142 (15.1%) | n.s |
| PCOS | 30 (2.2%) | 13 (1.4%) | n.s |
| Fasting glycose >5.1 mmol/L | 267 (19.7%) | 311 (33.1%) | 7.0 × 10−14 |
| Polyhydramnion | 47 (3.5%) | 38 (4.0%) | n.s |
| Other | 358 (26.4%) | 35 (3.7%) | 1.3 × 10−57 |
| Pregnancy course and outcome | |||
| Weight gain (0–23 g.w) (kg) | 7 (0–16) | 6 (−1–14) | 2.2 × 10−6 |
| Weight gain (24–42 g.w) (kg) | 11 (3.6–22) | 10 (2.9–17) | 2.0 × 10−5 |
| Total weight gain (kg) | 17.7 (4–36.5) | 15.8 (3–29.6) | 3.6 × 10−5 |
| Excessive weight gain 3 | 62.4% | 53.9% | 2.9 × 10−4 |
| GA at delivery (days) | 280 (260–293) | 280 (255–292) | n.s |
| Male newborn | 52.5% | 50.0% | n.s |
| Birthweight (grams) | 3705 (2808–4468) | 3578 (2642–4320) | 5.8 × 10−9 |
| LGA 4 | 315 (23.2%) | 161 (17.1%) | 4.2 × 10−4 |
| Birthweight centile | 82.2 (25–99.1) | 75.7 (18.4–98.2) | 5.2 × 10−9 |
| Cesarean section | 274 (20.2%) | 175 (18.6%) | n.s |
| If LGA (% of Cesarean sections) | 87 (31%) | 32 (18%) | 2.0 × 10−3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanson, E.; Ringmets, I.; Kirss, A.; Laan, M.; Rull, K. Screening of Gestational Diabetes and Its Risk Factors: Pregnancy Outcome of Women with Gestational Diabetes Risk Factors According to Glycose Tolerance Test Results. J. Clin. Med. 2022, 11, 4953. https://doi.org/10.3390/jcm11174953
Hanson E, Ringmets I, Kirss A, Laan M, Rull K. Screening of Gestational Diabetes and Its Risk Factors: Pregnancy Outcome of Women with Gestational Diabetes Risk Factors According to Glycose Tolerance Test Results. Journal of Clinical Medicine. 2022; 11(17):4953. https://doi.org/10.3390/jcm11174953
Chicago/Turabian StyleHanson, Ele, Inge Ringmets, Anne Kirss, Maris Laan, and Kristiina Rull. 2022. "Screening of Gestational Diabetes and Its Risk Factors: Pregnancy Outcome of Women with Gestational Diabetes Risk Factors According to Glycose Tolerance Test Results" Journal of Clinical Medicine 11, no. 17: 4953. https://doi.org/10.3390/jcm11174953