
Serum IL-13 Predicts Response to Golimumab in Bio-Naïve Ulcerative Colitis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcomes
2.3. Measurement of Serum Biomarkers
2.4. ECL for IL-1β, IL-5, IL-13, IL-15, IL-33, IL-12/IL-23p40, Eotaxin-1
2.5. ELISA for OSM, IL-4, IL-13Rα2, IL-17
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Efficacy Outcomes and Clinical Characteristics Associated with Clinical Remission
3.3. Relationship between Serum Molecules and Efficacy Outcomes
3.4. ROC Curve Analyses
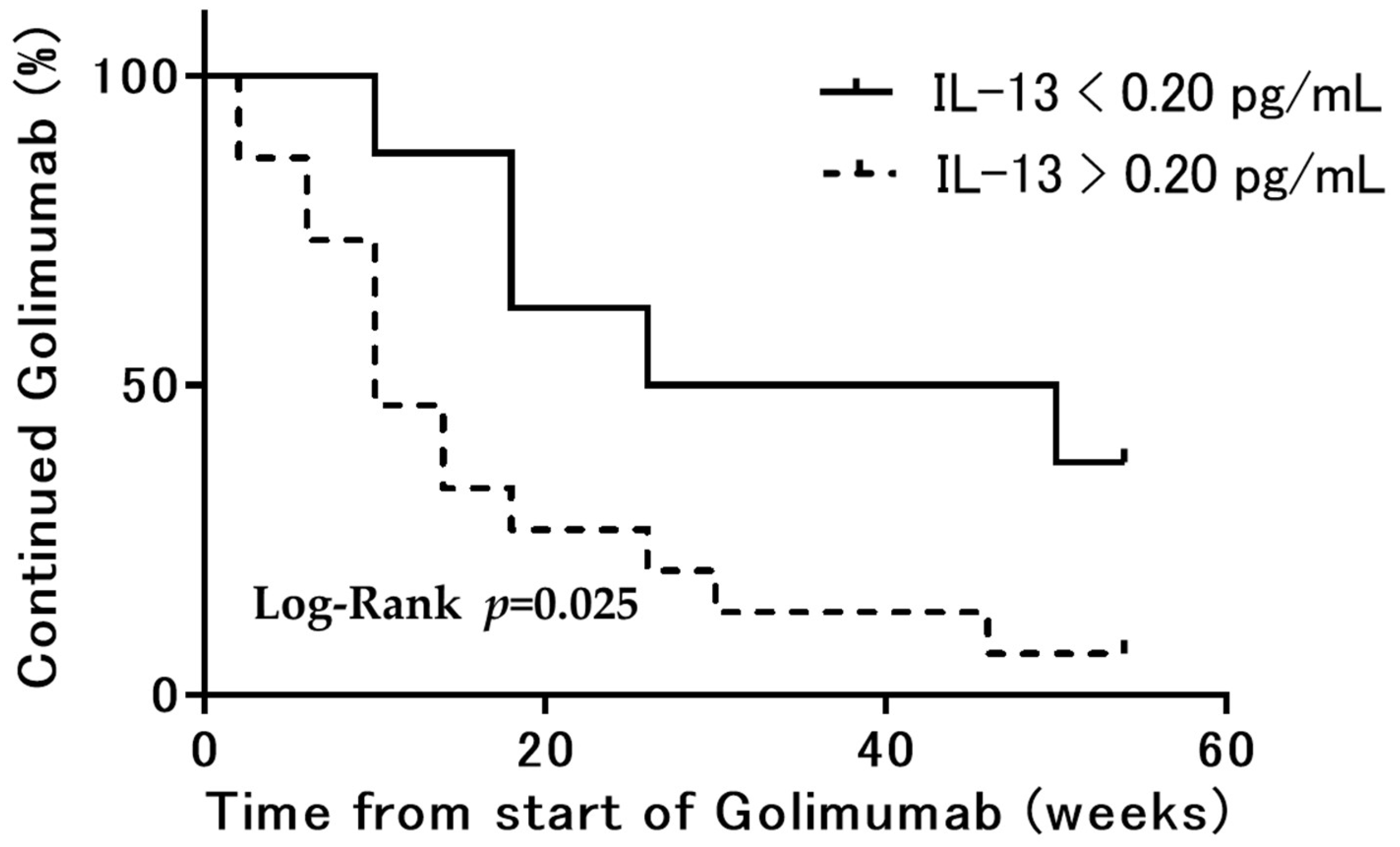
3.5. Kaplan–Meier Curve Analyses
3.6. Efficacy of GLM and Changes over Time
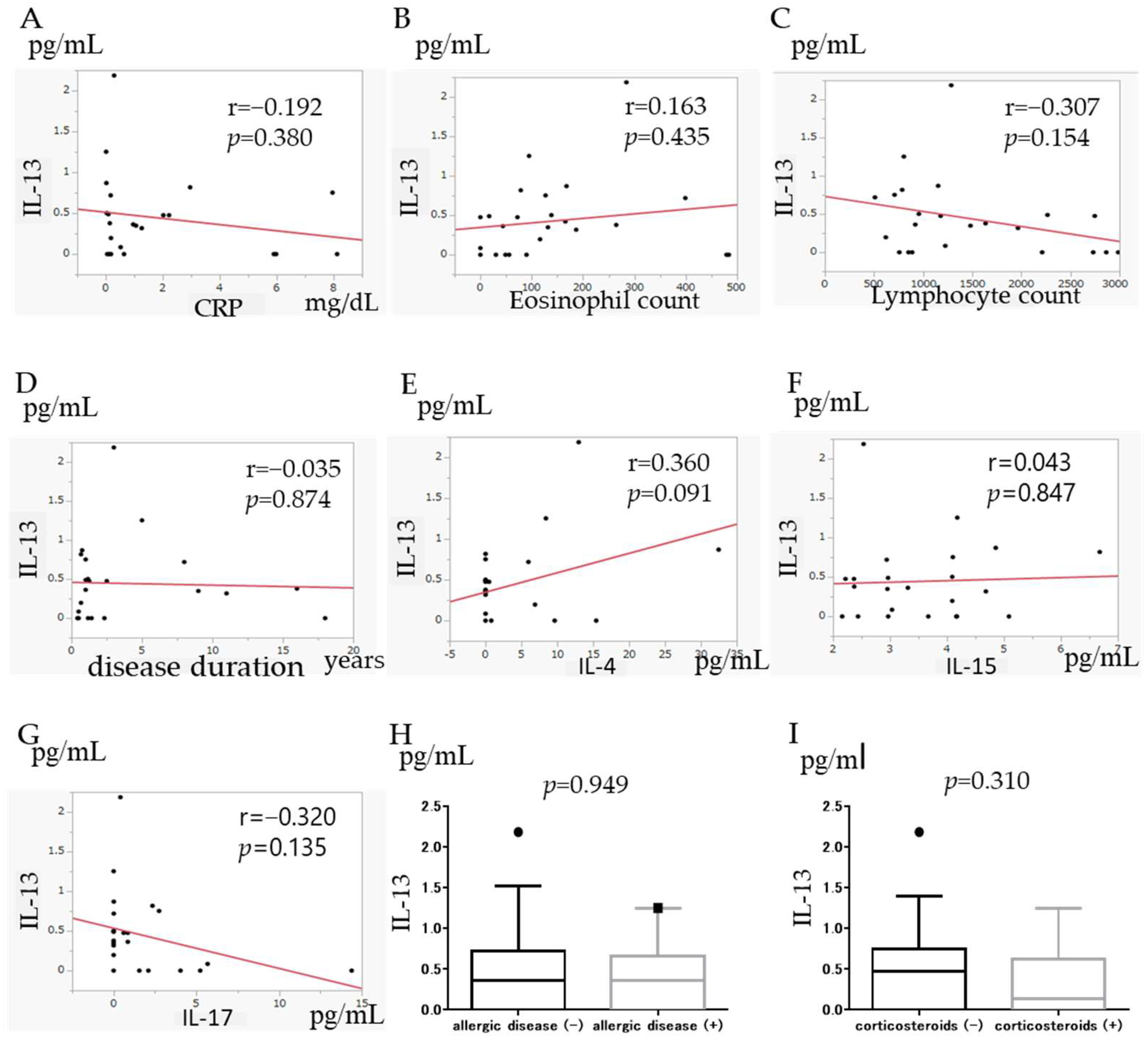
3.7. Correlation of IL-13 with Other Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Souza, H.S.; Fiocchi, C. Immunopathogenesis of IBD: Current state of the art. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Fiocchi, C. Ulcerative colitis. N. Engl. J. Med. 2011, 365, 1713–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neurath, M.F.; Finotto, S.; Glimcher, L.H. The role of Th1/Th2 polarization in mucosal immunity. Nat. Med. 2002, 8, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Danese, S. New therapies for inflammatory bowel disease: From the bench to the bedside. Gut 2012, 61, 918–932. [Google Scholar] [CrossRef] [PubMed]
- Ordas, I.; Eckmann, L.; Talamini, M.; Baumgart, D.C.; Sandborn, W.J. Ulcerative colitis. Lancet 2012, 380, 1606–1619. [Google Scholar] [CrossRef] [Green Version]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef] [Green Version]
- Reinisch, W.; Sandborn, W.J.; Hommes, D.W.; D’Haens, G.; Hanauer, S.; Schreiber, S.; Panaccione, R.; Fedorak, R.N.; Tighe, M.B.; Huang, B.; et al. Adalimumab for induction of clinical remission in moderate to severely active ulcerative colitis: Results of a randomized controlled trial. Gut 2011, 60, 780–787. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Marano, C.; Zhang, H.; Strauss, R.; Johanns, J.; Adedokun, O.J.; Guzzo, C.; Colombel, J.-F.; Reinisch, W.; et al. Subcutaneous golimumab induces clinical response and remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2014, 146, 85–95. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Marano, C.; Zhang, H.; Strauss, R.; Johanns, J.; Adedokun, O.J.; Guzzo, C.; Colombel, J.; Reinisch, W.; et al. Subcutaneous golimumab maintains clinical response in patients with moderate-to-severe ulcerative colitis. Gastroenterology 2014, 146, 96–109. [Google Scholar] [CrossRef]
- Garbers, C.; Hermanns, H.M.; Schaper, F.; Müller-Newen, G.; Grötzinger, J.; Rose-John, S.; Scheller, J. Plasticity and cross-talk of interleukin 6-type cytokines. Cytokine Growth Factor Rev. 2012, 23, 85–97. [Google Scholar] [CrossRef]
- West Nathaniel, N.; Hegazy, A.N.; Owens, B.M.; Bullers, S.J.; Linggi, B.; Buonocore, S.; Coccia, M.; Görtz, D.; This, S.; Stockenhuber, K.; et al. Oncostatin M drives intestinal inflammation and predicts response to tumor necrosis factor-neutralizing therapy in patients with inflammatory bowel disease. Nat. Med. 2017, 23, 579–589. [Google Scholar] [CrossRef]
- Verstockt, B.; Verstockt, S.; Creyns, B.; Tops, S.; Van Assche, G.; Gils, A.; Ceuppens, J.L.; Vermeire, S.; Ferrante, M.; Breynaert, C. Mucosal IL13RA2 expression predicts nonresponse to anti-TNF therapy in Crohn’s disease. Aliment. Pharmacol. Ther. 2019, 49, 572–581. [Google Scholar] [CrossRef]
- Kawashima, R.; Kawamura, Y.I.; Oshio, T.; Son, A.; Yamazaki, M.; Hagiwara, T.; Okada, T.; Inagaki–Ohara, K.; Wu, P.; Szak, S.; et al. Interleukin-13 Damages Intestinal Mucosa via TWEAK and Fn14 in Mice-A Pathway Associated with Ulcerative Colitis. Gastroenterology 2011, 141, 2119–2129. [Google Scholar] [CrossRef]
- Rosen, M.J.; Chaturvedi, R.; Washington, M.K.; Kuhnhein, L.A.; Moore, P.D.; Coggeshall, S.S.; McDonough, E.M.; Weitkamp, J.-H.; Singh, A.B.; Coburn, L.A.; et al. STAT6 Deficiency Ameliorates Severity of Oxazolone Colitis by Decreasing Expression of Claudin-2 and Th2-Inducing Cytokines. J. Immunol. 2013, 190, 1849–1858. [Google Scholar] [CrossRef] [Green Version]
- Bailey, J.R.; Bland, P.W.; Tarlton, J.F.; Peters, I.; Moorghen, M.; Sylvester, P.A.; Probert, C.S.; Whiting, C.V. IL-13 Promotoes Collagen Accumulation in Crohn’s Disease Fibrosis by Down-Regulation of Fibroblast MMP Synthesis: A Role for Innate Lymphoid Cells? PLoS ONE 2012, 7, e52332. [Google Scholar]
- Wright, K.; Kolios, G.; Westwick, J.; Ward, S.G. Cytokine-induced Apoptosis in Epithelial HT-29 Cells Is Independent of Nitric Oxide Formation. J. Biol. Chem. 1999, 24, 17193–17201. [Google Scholar] [CrossRef] [Green Version]
- Kissoon-Singh, V.; Moreau, F.; Trusevych, E.; Chadee, K. Entamoeba histolytica Exacerbates Epithelial Tight Junction Permeability and Proinflammatory Responses in Muc2−/− Mice. Am. J. Pathol. 2013, 182, 852–865. [Google Scholar] [CrossRef]
- Vitale, S.; Strisciuglio, C.; Pisapia, L.; Miele, E.; Barba, P.; Vitale, A.; Cenni, S.; Bassi, V.; Maglio, M.; Del Pozzo, G.; et al. Cytokine production profile in intestinal mucosa of paediatric inflammatory bowel disease. PLoS ONE 2017, 12, e0182313. [Google Scholar]
- Vainer, B.; Nielsen, O.H.; Hendel, J.; Horn, T.; Kirman, I. Colonic expression and synthesis of interleukin 13 and interleukin 15 in inflammatory bowel disease. Cytokine 2000, 12, 1531–1536. [Google Scholar] [CrossRef]
- Fujino, S.; Andoh, A.; Bamba, S.; Ogawa, A.; Hata, K.; Araki, Y.; Bamba, T.; Fujiyama, Y. Increased expression of interleukin 17 in inflammatory bowel disease. Gut 2003, 52, 65–70. [Google Scholar] [CrossRef]
- Műzes, G.; Molnár, B.; Tulassay, Z.; Sipos, F. Changes of the cytokine profile in inflammatory bowel diseases. World J. Gastroenterol. 2012, 18, 5848–5861. [Google Scholar] [CrossRef] [Green Version]
- Begue, B.; Wajant, H.; Bambou, J.; Dubuquoy, L.; Siegmund, D.; Beaulieu, J.; Canioni, D.; Berrebi, D.; Brousse, N.; Desreumaux, P.; et al. Implication of TNF-related apoptosis-inducing ligand in inflammatory intestinal epithelial lesions. Gastroenterology 2006, 130, 1962–1974. [Google Scholar] [CrossRef]
- He, Y.; Lin, L.J.; Zheng, C.Q.; Jin, Y.; Lin, Y. Cytokine expression and the role of Th17 cells in a mouse model of colitis. Mol. Med. Rep. 2012, 6, 1438–1442. [Google Scholar] [CrossRef] [Green Version]
- Nishiwaki, T.; Ina, K.; Goto, H.; Watanabe, O.; Tsuzuki, T.; Furuta, R.; Ando, T.; Hibi, K.; Kusugami, K. Possible involvement of the interleukin-15 and interleukin-15 receptor system in a heightened state of lamina propria B cell activation and differentiation in patients with inflammatory bowel disease. J. Gastroenterol. 2005, 40, 128–136. [Google Scholar] [CrossRef]
- Tosiek, M.J.; Fiette, L.; Daker, S.E.I.; Eberal, G.; Freitas, A.A. IL-15 dependent balance between Foxp3 and RORγt expression impacts inflammatory bowel disease. Nat. Commun. 2016, 7, 10888. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients, n | 23 |
|---|---|
| Male/Female, n | 13/10 |
| Age, year, median (IQR) | 47.0 (20–81) |
| Weight, kg, median (IQR) | 58.0 (41.9–88.8) |
| Duration of disease, year, median (IQR) | 1.17 (0.41–18) |
| UC location; Left side/Extensive, n | 6/17 |
| Medications for UC taken at baseline | |
| Aminosalicylates, n (%) | 19 (82.6) |
| Azathioprine, n (%) | 6 (26.1) |
| Corticosteroids, n (%) | 8 (34.7) |
| Corticosteroids dependent | 15 (65.2) |
| Corticosteroids refractory | 1 (4.3) |
| History of allegies, n (%) | 9 (39.1) |
| Partial Mayo score, median (IQR) | 7 (3–9) |
| WBC, /μL, median (IQR) | 8520 (3730–15,320) |
| Ly, %, median (IQR) | 20.8 (3.7–39.5) |
| Eo, %, median (IQR) | 1.4 (0–4.8) |
| Hb, g/dL, median (IQR) | 12.3 (8.8–16.2) |
| Platelet, 104/μL, median (IQR) | 33.1 (8.8–44.7) |
| Albumin, g/dL, median (IQR) | 3.9 (2.5–4.7) |
| CRP, mg/L, median (IQR) | 0.52 (0.01–8.17) |
| Number of Patients, n (%) | Remission 6 (26.1%) | Non-Remission 17 (65.3%) | p-Value |
|---|---|---|---|
| Male/Female, n | 2/4 | 11/6 | 0.341 |
| Age, year, median (IQR) | 31 (20–53) | 59 (24–81) | 0.023 |
| Duration of disease, year, median (IQR) | 0.835 (0.416–16) | 1.25 (0.5–18) | 0.247 |
| Clinical course; Relapse-remitting/chronic continuous, n | 6/0 | 13/4 | 0.539 |
| Medications for UC taken at baseline | |||
| Aminosalicylates, n (%) | 4 (66.7) | 15 (88.2) | 0.27 |
| Azathioprine, n (%) | 2 (33.3) | 4 (23.5) | 0.632 |
| Corticosteroids, n (%) | 4 (66.7) | 4 (23.5) | 0.131 |
| Corticosteroids dependent | 6 (100) | 9 (52.9) | 0.058 |
| Corticosteroids refractory | 0 (0) | 1 (5.9) | 1 |
| History of alergics, n (%) | 2 (33.3) | 7 (41.1) | 1 |
| Lichtiger index, median (IQR) | 11 (9–14) | 10.5 (5–16) | 0.367 |
| pMayo score, median (IQR) | 6.5 (5–8) | 7 (3–9) | 0.639 |
| WBC, /μL, median (IQR) | 8510 (4000–15,320) | 8520 (3730–13,760) | 1 |
| Ly, %, median (IQR) | 15.6 (8–39.5) | 20.8 (3.7–34.3) | 0.916 |
| Eo, %, median (IQR) | 0.2 (0–3.8) | 2.4 (0–4.8) | 0.073 |
| Hb, g/dL, median (IQR) | 12.7 (11.0–14.8) | 12.3 (8.8–16.2) | 0.506 |
| Albumin, g/dL, median (IQR) | 3.95 (2.7–4.6) | 3.75 (2.5–4.7) | 0.853 |
| CRP, mg/L, median (IQR) | 0.33 (0.05–8.12) | 0.64 (0.01–7.96) | 0.972 |
| Platlet, 109/L, median (IQR) | 38.3 (21.6–44.7) | 30.0 (8.8–43.4) | 0.074 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinoshita, N.; Kakimoto, K.; Shimizu, H.; Nishida, K.; Numa, K.; Kawasaki, Y.; Tawa, H.; Nakazawa, K.; Koshiba, R.; Hirata, Y.; et al. Serum IL-13 Predicts Response to Golimumab in Bio-Naïve Ulcerative Colitis. J. Clin. Med. 2022, 11, 4952. https://doi.org/10.3390/jcm11174952
Kinoshita N, Kakimoto K, Shimizu H, Nishida K, Numa K, Kawasaki Y, Tawa H, Nakazawa K, Koshiba R, Hirata Y, et al. Serum IL-13 Predicts Response to Golimumab in Bio-Naïve Ulcerative Colitis. Journal of Clinical Medicine. 2022; 11(17):4952. https://doi.org/10.3390/jcm11174952
Chicago/Turabian StyleKinoshita, Naohiko, Kazuki Kakimoto, Hikaru Shimizu, Koji Nishida, Keijiro Numa, Yuka Kawasaki, Hideki Tawa, Kei Nakazawa, Ryoji Koshiba, Yuki Hirata, and et al. 2022. "Serum IL-13 Predicts Response to Golimumab in Bio-Naïve Ulcerative Colitis" Journal of Clinical Medicine 11, no. 17: 4952. https://doi.org/10.3390/jcm11174952