
Cerebral Tissue Oxygen Saturation Correlates with Emergence from Propofol-Remifentanil Anesthesia: An Observational Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Study Procedures
2.4. Statistical Analysis
3. Results
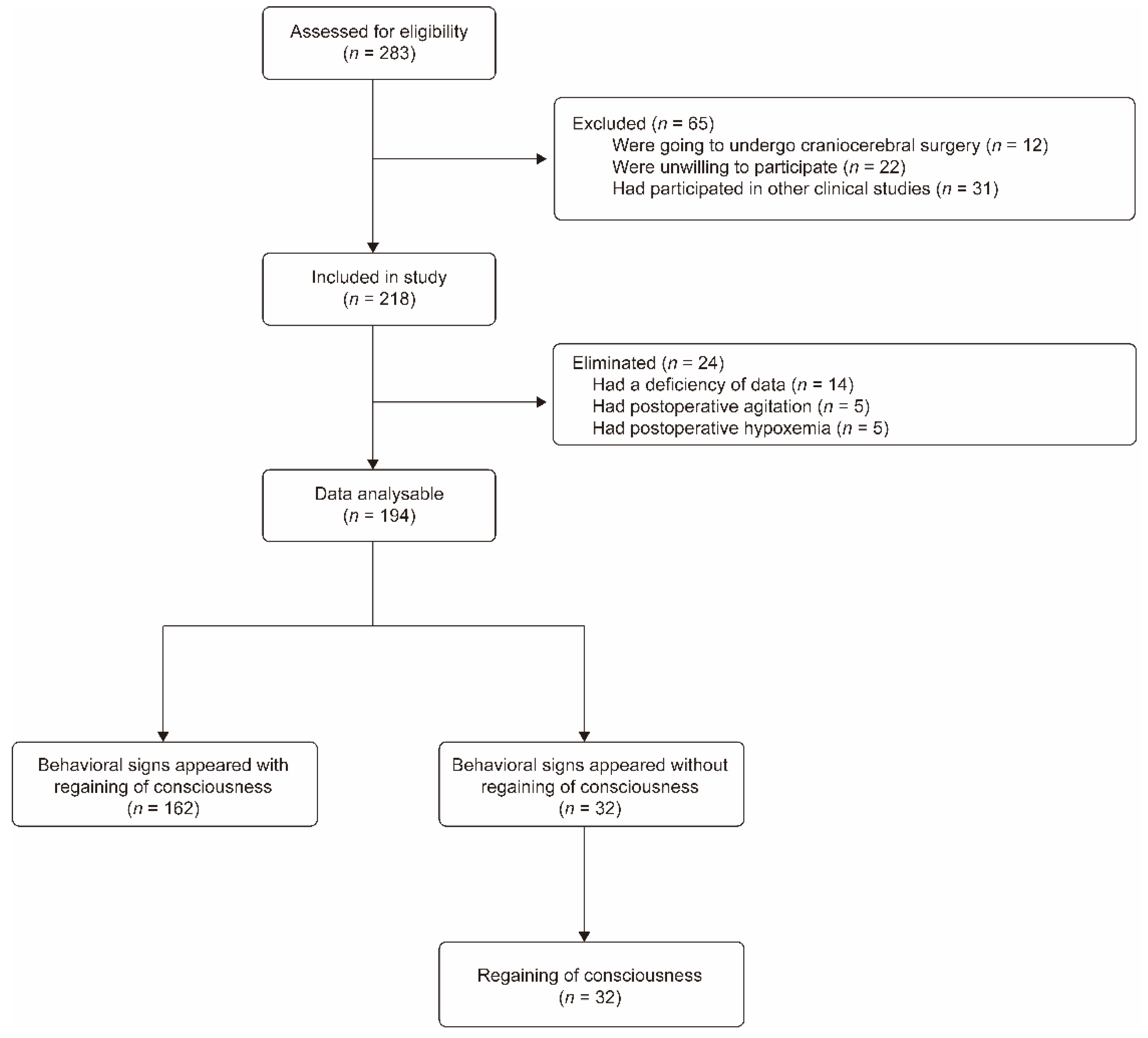
3.1. Study Population
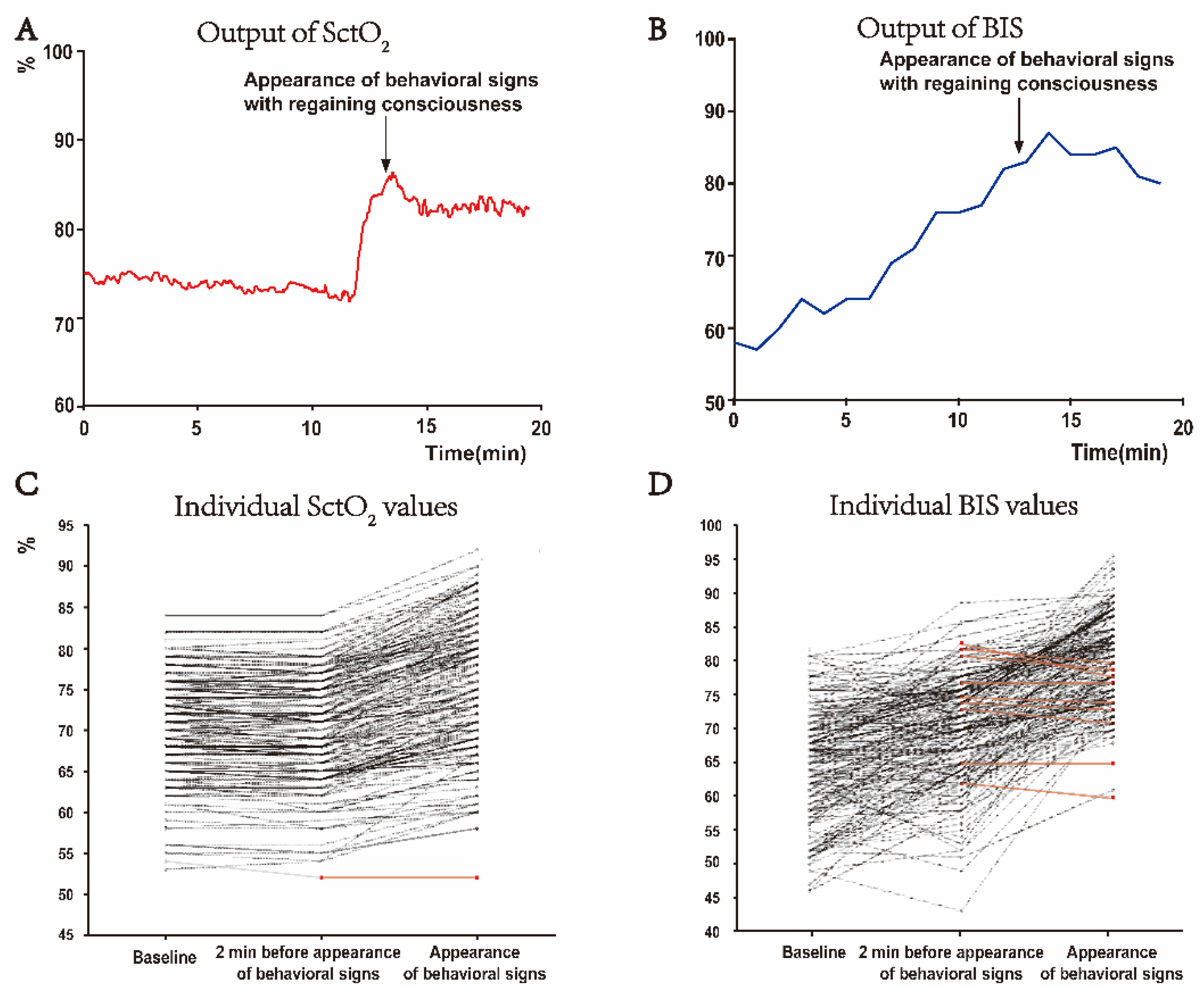
3.2. Appearing of Behavioral Signs during Emergence Is Associated with an Abrupt and Distinctive Increase in SctO2 Value
3.3. SctO2 Is a Prompt and More Reliable Indicator of Appearing Behavioral Signs during Anesthesia Emergence Than BIS, MAP, and HR
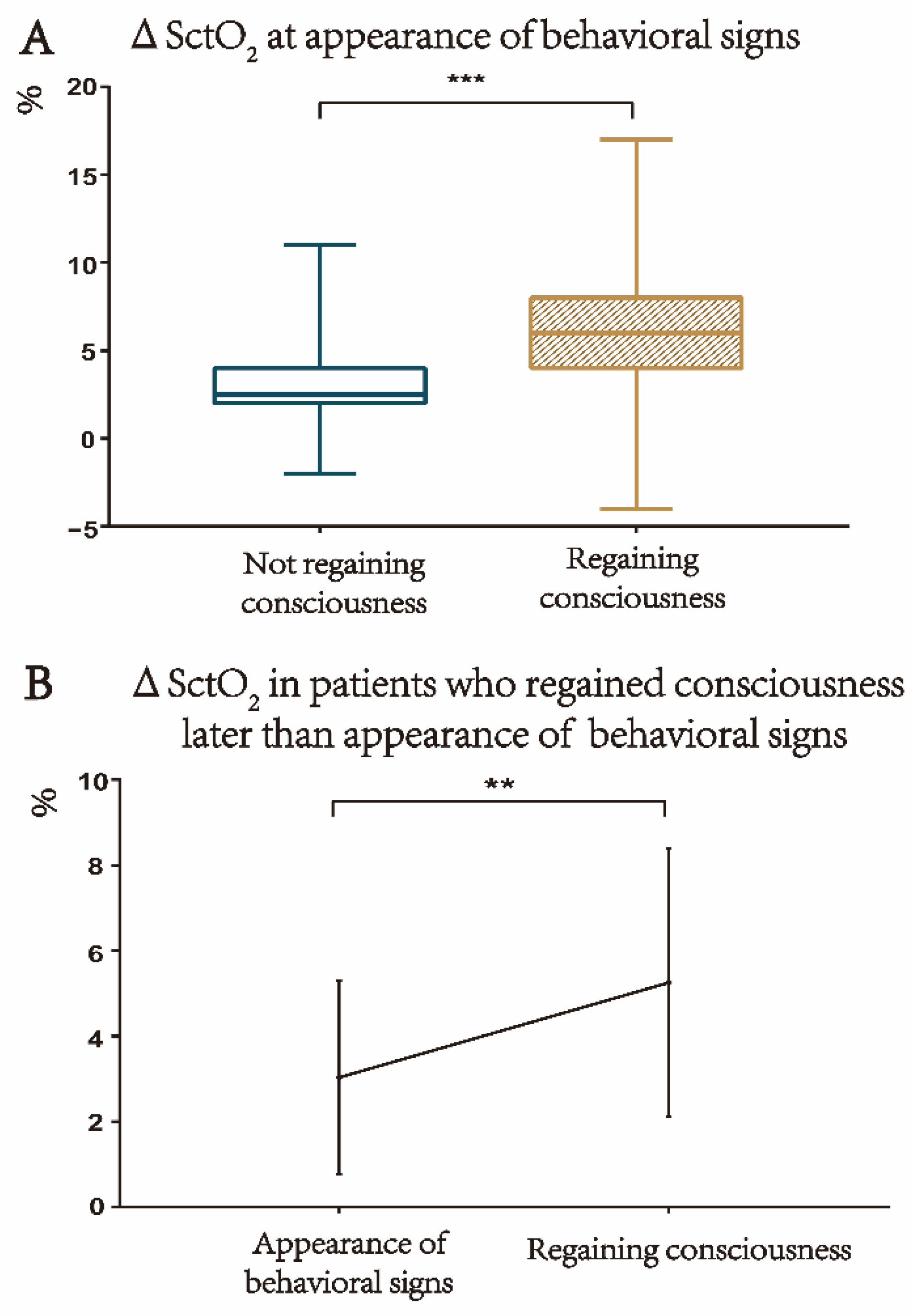
3.4. The SctO2 Is Further Increased from the Appearance of Behavioral Signs to the Regaining of Consciousness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reshef, E.R.; Schiff, N.D.; Brown, E.N. A Neurologic Examination for Anesthesiologists: Assessing Arousal Level during Induction, Maintenance, and Emergence. Anesthesiology 2019, 130, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, L.H.; Abrahams, S. Changes in cognition and behaviour in amyotrophic lateral sclerosis: Nature of impairment and implications for assessment. Lancet. Neurol. 2013, 12, 368–380. [Google Scholar] [CrossRef]
- McGuire, J.M.; Burkard, J.F. Risk factors for emergence delirium in U.S. military members. J. Perianesthesia Nurs. Off. J. Am. Soc. PeriAnesthesia Nurses 2010, 25, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.H.; Nittur, V.R.; Fleming, N.; Applegate, R.L., 2nd. Simultaneous comparison of depth of sedation performance between SedLine and BIS during general anesthesia using custom passive interface hardware: Study protocol for a prospective, non-blinded, non-randomized trial. BMC Anesthesiol. 2021, 21, 105. [Google Scholar] [CrossRef]
- Chen, W.; Jiang, F.; Chen, X.; Feng, Y.; Miao, J.; Chen, S.; Jiao, C.; Chen, H. Photoplethysmography-derived approximate entropy and sample entropy as measures of analgesia depth during propofol-remifentanil anesthesia. J. Clin. Monit. Comput. 2021, 35, 297–305. [Google Scholar] [CrossRef]
- Puchner, W.F.; Dünser, M.W.; Paulus, P.; Neuner, M.P.; Mayer, C.L.; Pomberger, I.M.; Hackl, R.; Meier, J.M. A comparative study on adequate anesthesia depth: Clinical judgement and the Narcotrend® measurement. Can. J. Anaesth. = J. Can. D’anesthesie 2020, 67, 664–673. [Google Scholar] [CrossRef]
- Kurita, T.; Doi, M.; Katoh, T.; Sano, H.; Sato, S.; Mantzaridis, H.; Kenny, G.N. Auditory evoked potential index predicts the depth of sedation and movement in response to skin incision during sevoflurane anesthesia. Anesthesiology 2001, 95, 364–370. [Google Scholar] [CrossRef]
- Lewis, S.R.; Pritchard, M.W.; Fawcett, L.J.; Punjasawadwong, Y. Bispectral index for improving intraoperative awareness and early postoperative recovery in adults. Cochrane Database Syst. Rev. 2019, 9, Cd003843. [Google Scholar] [CrossRef]
- Dennhardt, N.; Boethig, D.; Beck, C.; Heiderich, S.; Boehne, M.; Leffler, A.; Schultz, B.; Sümpelmann, R. Optimization of initial propofol bolus dose for EEG Narcotrend Index-guided transition from sevoflurane induction to intravenous anesthesia in children. Paediatr. Anaesth. 2017, 27, 425–432. [Google Scholar] [CrossRef]
- Hajat, Z.; Ahmad, N.; Andrzejowski, J. The role and limitations of EEG-based depth of anaesthesia monitoring in theatres and intensive care. Anaesthesia 2017, 72 (Suppl. 1), 38–47. [Google Scholar] [CrossRef]
- Recart, A.; Gasanova, I.; White, P.F.; Thomas, T.; Ogunnaike, B.; Hamza, M.; Wang, A. The effect of cerebral monitoring on recovery after general anesthesia: A comparison of the auditory evoked potential and bispectral index devices with standard clinical practice. Anesth. Analg. 2003, 97, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Kaskinoro, K.; Maksimow, A.; Långsjö, J.; Aantaa, R.; Jääskeläinen, S.; Kaisti, K.; Särkelä, M.; Scheinin, H. Wide inter-individual variability of bispectral index and spectral entropy at loss of consciousness during increasing concentrations of dexmedetomidine, propofol, and sevoflurane. Br. J. Anaesth. 2011, 107, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Tiefenthaler, W.; Colvin, J.; Steger, B.; Pfeiffer, K.P.; Moser, P.L.; Walde, J.; Lorenz, I.H.; Kolbitsch, C. How Bispectral Index Compares to Spectral Entropy of the EEG and A-line ARX Index in the Same Patient. Open Med. 2018, 13, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Mashour, G.A.; Palanca, B.J.; Basner, M.; Li, D.; Wang, W.; Blain-Moraes, S.; Lin, N.; Maier, K.; Muench, M.; Tarnal, V.; et al. Recovery of consciousness and cognition after general anesthesia in humans. eLife 2021, 10, e59525. [Google Scholar] [CrossRef] [PubMed]
- Kelz, M.B.; García, P.S.; Mashour, G.A.; Solt, K. Escape From Oblivion: Neural Mechanisms of Emergence From General Anesthesia. Anesth. Analg. 2019, 128, 726–736. [Google Scholar] [CrossRef]
- Xie, G.; Deschamps, A.; Backman, S.B.; Fiset, P.; Chartrand, D.; Dagher, A.; Plourde, G. Critical involvement of the thalamus and precuneus during restoration of consciousness with physostigmine in humans during propofol anaesthesia: A positron emission tomography study. Br. J. Anaesth. 2011, 106, 548–557. [Google Scholar] [CrossRef]
- Hudetz, A.G. General anesthesia and human brain connectivity. Brain Connect. 2012, 2, 291–302. [Google Scholar] [CrossRef]
- Drummond, J.C.; Dao, A.V.; Roth, D.M.; Cheng, C.R.; Atwater, B.I.; Minokadeh, A.; Pasco, L.C.; Patel, P.M. Effect of dexmedetomidine on cerebral blood flow velocity, cerebral metabolic rate, and carbon dioxide response in normal humans. Anesthesiology 2008, 108, 225–232. [Google Scholar] [CrossRef]
- Jöbsis, F.F. Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science 1977, 198, 1264–1267. [Google Scholar] [CrossRef]
- Murkin, J.M.; Arango, M. Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br. J. Anaesth. 2009, 103 (Suppl. 1), i3–i13. [Google Scholar] [CrossRef]
- Leontiev, O.; Dubowitz, D.J.; Buxton, R.B. CBF/CMRO2 coupling measured with calibrated BOLD fMRI: Sources of bias. NeuroImage 2007, 36, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Leithner, C.; Royl, G. The oxygen paradox of neurovascular coupling. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2014, 34, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Koch, K.U.; Zhao, X.; Mikkelsen, I.K.; Espelund, U.S.; Aanerud, J.; Rasmussen, M.; Meng, L. Correlation Between Cerebral Tissue Oxygen Saturation and Oxygen Extraction Fraction During Anesthesia: Monitoring Cerebral Metabolic Demand-supply Balance During Vasopressor Administration. J. Neurosurg. Anesthesiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Meza, G.; Izzetoglu, M.; Osbakken, M.; Green, M.; Abubakar, H.; Izzetoglu, K. Investigation of optical neuro-monitoring technique for detection of maintenance and emergence states during general anesthesia. J. Clin. Monit. Comput. 2018, 32, 147–163. [Google Scholar] [CrossRef] [PubMed]
- Leon-Dominguez, U.; Izzetoglu, M.; Leon-Carrion, J.; Solís-Marcos, I.; Garcia-Torrado, F.J.; Forastero-Rodríguez, A.; Mellado-Miras, P.; Villegas-Duque, D.; Lopez-Romero, J.L.; Onaral, B.; et al. Molecular concentration of deoxyHb in human prefrontal cortex predicts the emergence and suppression of consciousness. NeuroImage 2014, 85 Pt 1, 616–625. [Google Scholar] [CrossRef]
- Agha, R.; Abdall-Razak, A.; Crossley, E.; Dowlut, N.; Iosifidis, C.; Mathew, G. STROCSS 2019 Guideline: Strengthening the reporting of cohort studies in surgery. Int. J. Surg. 2019, 72, 156–165. [Google Scholar] [CrossRef]
- Davie, S.N.; Grocott, H.P. Impact of extracranial contamination on regional cerebral oxygen saturation: A comparison of three cerebral oximetry technologies. Anesthesiology 2012, 116, 834–840. [Google Scholar] [CrossRef]
- Cornelissen, L.; Donado, C.; Lee, J.M.; Liang, N.E.; Mills, I.; Tou, A.; Bilge, A.; Berde, C.B. Clinical signs and electroencephalographic patterns of emergence from sevoflurane anaesthesia in children: An observational study. Eur. J. Anaesthesiol. 2018, 35, 49–59. [Google Scholar] [CrossRef]
- Ledowski, T.; Bromilow, J.; Paech, M.J.; Storm, H.; Hacking, R.; Schug, S.A. Skin conductance monitoring compared with Bispectral Index to assess emergence from total i.v. anaesthesia using propofol and remifentanil. Br. J. Anaesth. 2006, 97, 817–821. [Google Scholar] [CrossRef]
- Ledowski, T.; Paech, M.J.; Storm, H.; Jones, R.; Schug, S.A. Skin conductance monitoring compared with bispectral index monitoring to assess emergence from general anaesthesia using sevoflurane and remifentanil. Br. J. Anaesth. 2006, 97, 187–191. [Google Scholar] [CrossRef]
- Smith, W.D.; Dutton, R.C.; Smith, N.T. Measuring the performance of anesthetic depth indicators. Anesthesiology 1996, 84, 38–51. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Grillo, P.; Bruder, N.; Auquier, P.; Pellissier, D.; Gouin, F. Esmolol blunts the cerebral blood flow velocity increase during emergence from anesthesia in neurosurgical patients. Anesth. Analg. 2003, 96, 1145–1149. [Google Scholar] [CrossRef]
- Chai, C.; Wang, H.; Chu, Z.; Li, J.; Qian, T.; Mark Haacke, E.; Xia, S.; Shen, W. Reduced regional cerebral venous oxygen saturation is a risk factor for the cognitive impairment in hemodialysis patients: A quantitative susceptibility mapping study. Brain Imaging Behav. 2020, 14, 1339–1349. [Google Scholar] [CrossRef] [PubMed]
- Picton, P.; Dering, A.; Alexander, A.; Neff, M.; Miller, B.S.; Shanks, A.; Housey, M.; Mashour, G.A. Influence of Ventilation Strategies and Anesthetic Techniques on Regional Cerebral Oximetry in the Beach Chair Position: A Prospective Interventional Study with a Randomized Comparison of Two Anesthetics. Anesthesiology 2015, 123, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Zanner, R.; Pilge, S.; Kochs, E.F.; Kreuzer, M.; Schneider, G. Time delay of electroencephalogram index calculation: Analysis of cerebral state, bispectral, and Narcotrend indices using perioperatively recorded electroencephalographic signals. Br. J. Anaesth. 2009, 103, 394–399. [Google Scholar] [CrossRef]
- Kwak, H.J.; Kim, J.Y.; Lee, K.C.; Kim, H.S.; Kim, J.Y. Effect of mild hypocapnia on hemodynamic and bispectral index responses to tracheal intubation during propofol anesthesia in children. J. Clin. Monit. Comput. 2015, 29, 29–33. [Google Scholar] [CrossRef]
- Channabasappa, S.M.; Shankarnarayana, P. A comparative study of hemodynamic changes between prone and supine emergence from anesthesia in lumbar disc surgery. Anesth. Essays Res. 2013, 7, 173–177. [Google Scholar] [CrossRef]
- Paloheimo, M.P.; Sahanne, S.; Uutela, K.H. Autonomic nervous system state: The effect of general anaesthesia and bilateral tonsillectomy after unilateral infiltration of lidocaine. Br. J. Anaesth. 2010, 104, 587–595. [Google Scholar] [CrossRef]
- Långsjö, J.W.; Alkire, M.T.; Kaskinoro, K.; Hayama, H.; Maksimow, A.; Kaisti, K.K.; Aalto, S.; Aantaa, R.; Jääskeläinen, S.K.; Revonsuo, A.; et al. Returning from oblivion: Imaging the neural core of consciousness. J. Neurosci. Off. J. Soc. Neurosci. 2012, 32, 4935–4943. [Google Scholar] [CrossRef]
- Brown, E.N.; Lydic, R.; Schiff, N.D. General anesthesia, sleep, and coma. N. Engl. J. Med. 2010, 363, 2638–2650. [Google Scholar] [CrossRef] [PubMed]
- Meex, I.; Vundelinckx, J.; Buyse, K.; Deburggraeve, F.; De Naeyer, S.; Desloovere, V.; Anné, L.; Truijen, J.; Vander Laenen, M.; Heylen, R.; et al. Cerebral tissue oxygen saturation values in volunteers and patients in the lateral decubitus and beach chair positions: A prospective observational study. Can. J. Anaesth. 2016, 63, 537–543. [Google Scholar] [CrossRef]
- Suehiro, K.; Okutai, R. Cerebral desaturation during single-lung ventilation is negatively correlated with preoperative respiratory functions. J. Cardiothorac. Vasc. Anesth. 2011, 25, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Kelz, M.B.; Sun, Y.; Chen, J.; Cheng Meng, Q.; Moore, J.T.; Veasey, S.C.; Dixon, S.; Thornton, M.; Funato, H.; Yanagisawa, M. An essential role for orexins in emergence from general anesthesia. Proc. Natl. Acad. Sci. USA 2008, 105, 1309–1314. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 194) |
|---|---|
| Age (y) | 49.41 ± 12.39 |
| Male, n (%) | 91 (46.91) |
| BMI (kg (m−2)−1) | 23.03 ± 2.86 |
| ASA classification, n (%) | |
| II | 120 (61.86) |
| III | 74 (38.14) |
| Comorbidities, n (%) | |
| Hypertension | 55 (28.35) |
| Current smoker | 54 (27.84) |
| Diabetes | 29 (14.95) |
| Coronary artery disease | 24 (12.37) |
| Asthma | 21 (10.82) |
| Chronic obstructive pulmonary disease | 12 (6.19) |
| Obesity a | 5 (2.58) |
| Type of surgery, n (%) | |
| Head and neck | 47 (24.23) |
| General | 63 (32.47) |
| Gynecological | 25 (12.89) |
| Thoracic | 18 (9.28) |
| Orthopedic | 8 (4.12) |
| Spinal | 7 (3.61) |
| Vascular | 7 (3.61) |
| Plastic | 5 (2.58) |
| Other | 14 (7.21) |
| Intraoperative medications | |
| Midazolam (mg) | 7.20 ± 1.99 |
| Sufentanil (µg) | 36.88 ± 9.55 |
| Cisatracurium (mg) | 16.62 ± 3.80 |
| Etomidate (mg) | 22.40 ± 14.60 |
| Propofol (mg kg−1) | 17.75 ± 9.44 |
| Remifentanil (µg kg−1) | 25.88 ± 13.84 |
| Duration of anesthesia (min) | 134.39 ± 67.20 |
| Baseline * | Changes over Baseline # | |||
|---|---|---|---|---|
| 2 Min before Appearance of Behavioral Signs & | Appearance of Behavioral Signs | p Values $ | ||
| SctO2 (%) | 70 ± 6 | 0 ± 1 | 6 ± 3 | <0.001 |
| BIS | 65 ± 8 | 6 ± 6 | 16 ± 9 | <0.001 |
| MAP (mmHg) | 89 ± 13 | 1 ± 5 | 5 ± 7 | <0.001 |
| HR (bpm) | 60 ± 10 | 1 ± 5 | 13 ± 10 | <0.001 |
| Pk | SE | AUC | 95% CI | |
|---|---|---|---|---|
| Δ SctO2 | 0.97 | 0.01 | 0.97 | 0.95–0.99 |
| Δ BIS | 0.81 *** | 0.02 | 0.81 ### | 0.77–0.85 |
| Δ MAP | 0.72 *** | 0.03 | 0.72 ### | 0.67–0.76 |
| Δ HR | 0.87 *** | 0.02 | 0.87 ### | 0.83–0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Cheng, Z.; Tian, Y.; Weng, L.; Zhang, Y.; Yang, X.; Schäfer, M.K.E.; Guo, Q.; Huang, C. Cerebral Tissue Oxygen Saturation Correlates with Emergence from Propofol-Remifentanil Anesthesia: An Observational Cohort Study. J. Clin. Med. 2022, 11, 4878. https://doi.org/10.3390/jcm11164878
Zhang J, Cheng Z, Tian Y, Weng L, Zhang Y, Yang X, Schäfer MKE, Guo Q, Huang C. Cerebral Tissue Oxygen Saturation Correlates with Emergence from Propofol-Remifentanil Anesthesia: An Observational Cohort Study. Journal of Clinical Medicine. 2022; 11(16):4878. https://doi.org/10.3390/jcm11164878
Chicago/Turabian StyleZhang, Jianxi, Zhigang Cheng, Ying Tian, Lili Weng, Yiying Zhang, Xin Yang, Michael K. E. Schäfer, Qulian Guo, and Changsheng Huang. 2022. "Cerebral Tissue Oxygen Saturation Correlates with Emergence from Propofol-Remifentanil Anesthesia: An Observational Cohort Study" Journal of Clinical Medicine 11, no. 16: 4878. https://doi.org/10.3390/jcm11164878