
Factors Associated with Variability in Pulse Wave Transit Time Using Pulse Oximetry: A Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Sources
2.2. Clinical Characteristics
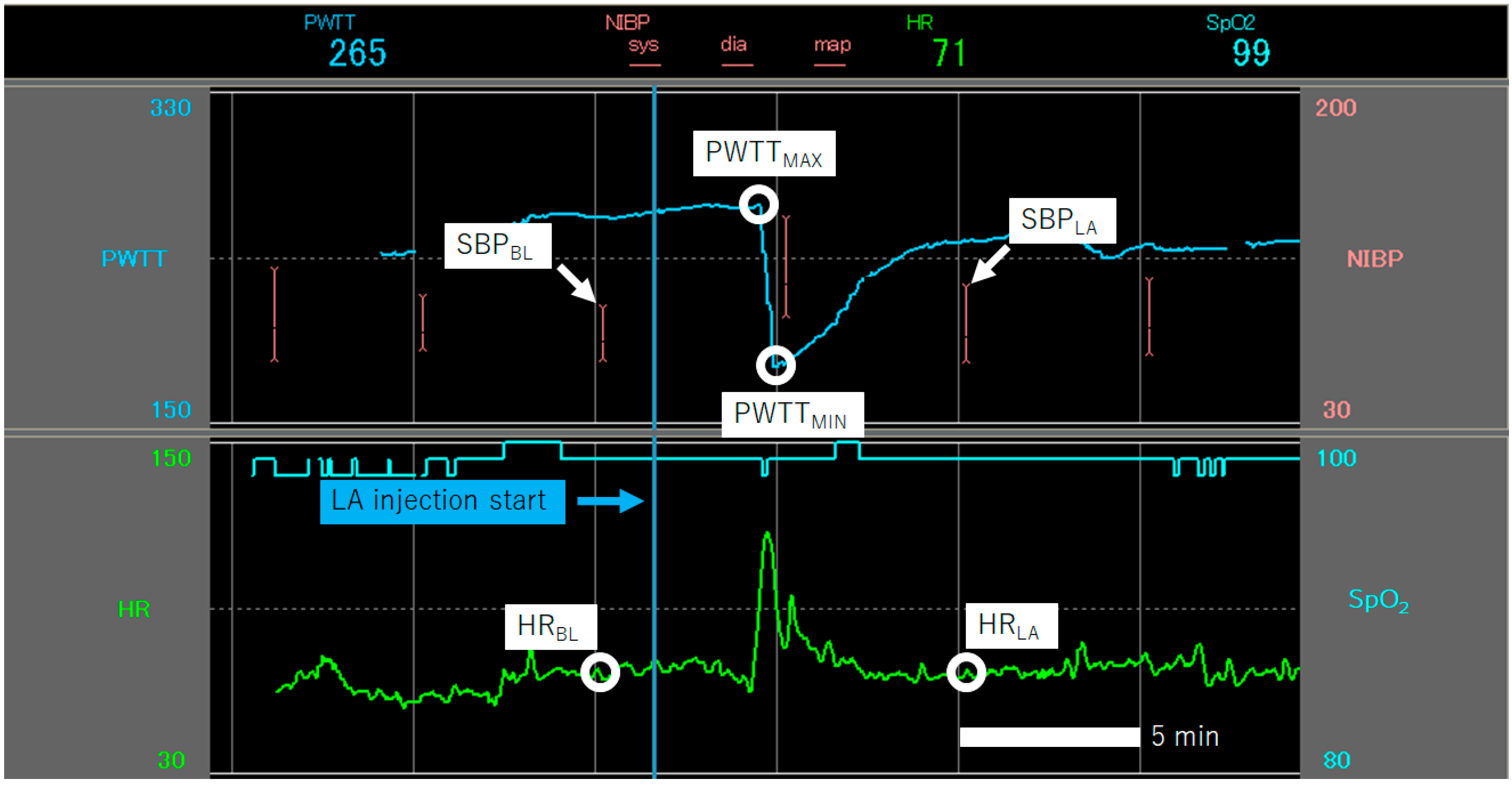
2.3. Variables from Recorded Segments
2.4. Statistical Analysis
3. Results
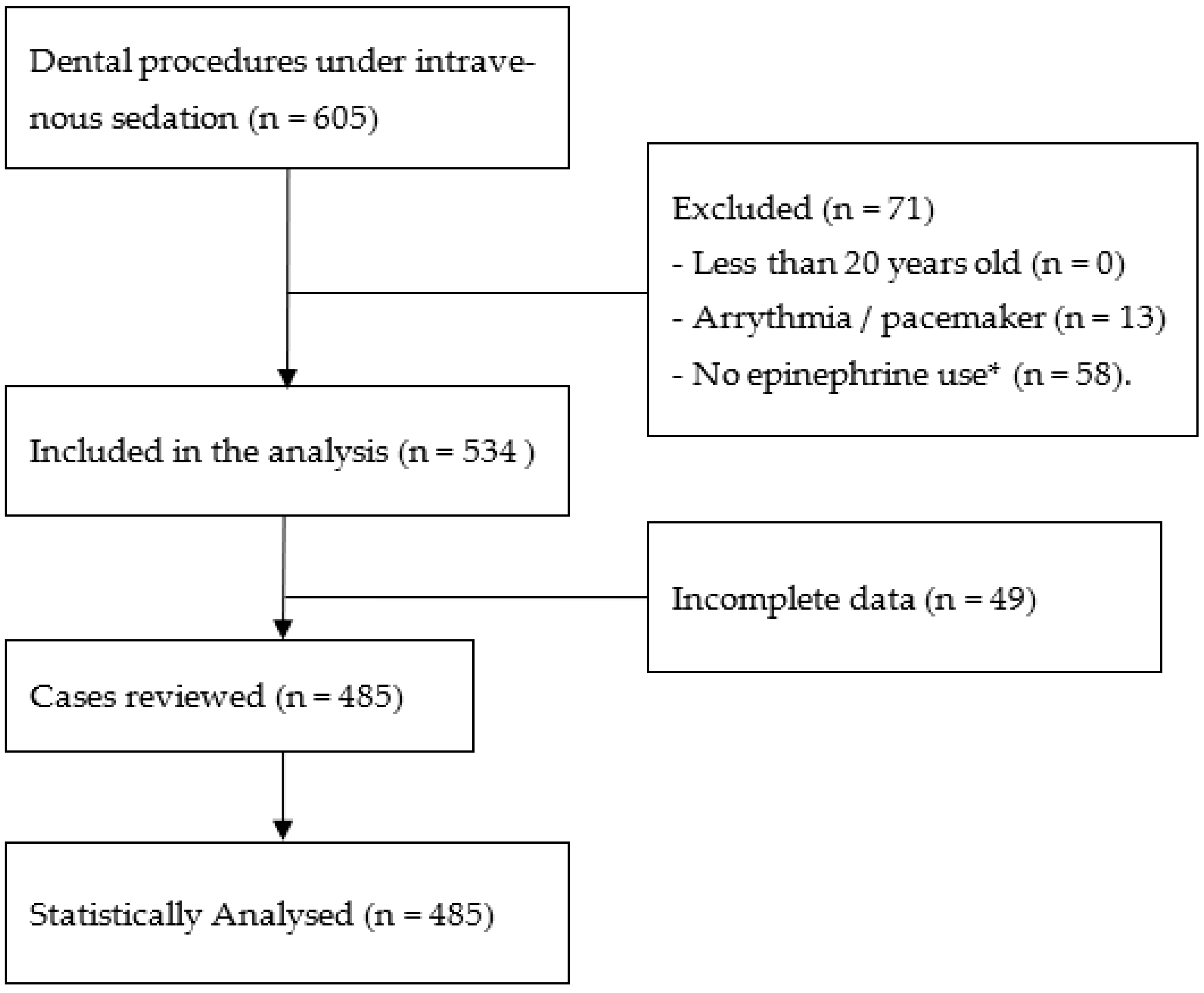
3.1. Primary Outcome and Summary of Inclusions
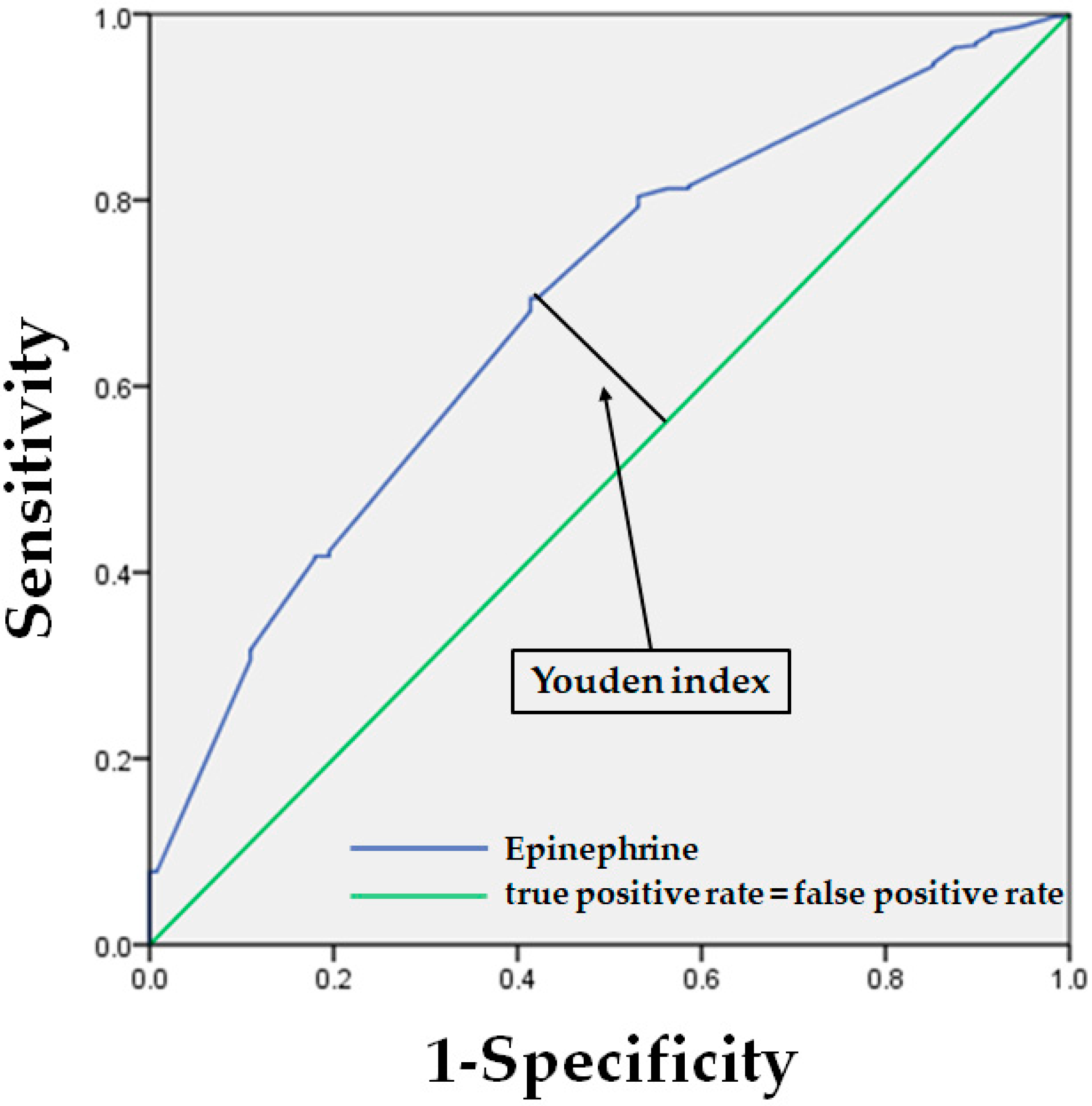
3.2. Results from Logistic Regression Analysis
Supplementary Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Newlin, D.B. Relationships of Pulse Transmission Times to Pre-ejection Period and Blood Pressure. Psychophysiology 1981, 18, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.P.; Phero, J.C.; Grau, W.H. Epinephrine: Systemic Effects and Varying Concentrations in Local Anesthesia. Anesth. Prog. 1986, 33, 289–297. [Google Scholar] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Age-Specific Relevance of Usual Blood Pressure to Vascular Mortality: A Meta-analysis of Individual Data for One Million Adults in 61 Prospective Studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Elmatite, W.; Mangla, C.; Upadhyay, S.; Yarmush, J. Perioperative Automated Noninvasive Blood Pressure-(NIBP-) Related Peripheral Nerve Injuries: An Anesthetist’s Dilemma-A Case Report and Review of the Literature. Case Rep. Anesthesiol. 2020, 2020, 5653481. [Google Scholar] [CrossRef]
- Meidert, A.S.; Saugel, B. Techniques for Non-invasive Monitoring of Arterial Blood Pressure. Front. Med. 2017, 4, 231. [Google Scholar] [CrossRef]
- Schaanning, S.G.; Skjaervold, N.K. Rapid Declines in Systolic Blood Pressure Are Associated with an Increase in Pulse Transit Time. PLoS ONE 2020, 15, e0240126. [Google Scholar] [CrossRef]
- Ochiai, R.; Takeda, J.; Hosaka, H.; Sugo, Y.; Tanaka, R.; Soma, T. The Relationship Between Modified Pulse Wave Transit Time and Cardiovascular Changes in Isoflurane Anesthetized Dogs. J. Clin. Monit. Comput. 1999, 15, 493–501. [Google Scholar] [CrossRef]
- Smith, R.P.; Argod, J.; Pépin, J.L.; Lévy, P.A. Pulse Transit Time: An Appraisal of Potential Clinical Applications. Thorax 1999, 54, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.N.; Gao, H.Q.; Li, B.Y.; Cheng, M.; Ma, Y.B.; Zhang, Z.M.; Gao, X.; Liu, Y.; Wang, M. Pulse Wave Velocity as a Marker of Arteriosclerosis and Its Comorbidities in Chinese Patients. Hypertens. Res. 2007, 30, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Abbott, D.; Howard, N.; Lim, K.; Ward, R.; Elgendi, M. How Effective Is Pulse Arrival Time for Evaluating Blood Pressure? Challenges and Recommendations from a Study Using the MIMIC Database. J. Clin. Med. 2019, 8, 337. [Google Scholar] [CrossRef] [Green Version]
- Yoneda, B.; Zuiki, M.; Komatsu, H. Utility of Pulse Wave Transit Time to Detect Blood Pressure Changes in Neonates. J. Jpn. Soc. Perinat. Neonatal Med. 2021, 57, 334–338. [Google Scholar] [CrossRef]
- Hiroko, I.; Takehiko, I.; Makoto, T.; Yasuhide, I.; Yoshihiro, S.; Katana, K. Examining the Effectiveness of NIBP Blood Pressure Measurement Using PWTT. In Proceedings of the Japanese Association for Clinical Monitoring, Yokohama, Japan, 17–21 November 2002; p. 41. [Google Scholar]
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan. Japan Society for the Study of Obesity New Criteria for ‘Obesity Disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takakura, M.; Miyagi, M.; Kyan, A. Time Trends of Socioeconomic Inequalities in Adolescent Smoking in Okinawa, Japan, 2008–2016: A Repeated Cross-Sectional Study. Environ. Health Prev. Med. 2021, 26, 24. [Google Scholar] [CrossRef]
- Ishihara, H.; Tsutsui, M. Impact of Changes in Systemic Vascular Resistance on a Novel Non-invasive Continuous Cardiac Output Measurement System Based on Pulse Wave Transit Time: A Report of Two Cases. J. Clin. Monit. Comput. 2014, 28, 423–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsui, M.; Araki, Y.; Masui, K.; Kazama, T.; Sugo, Y.; Archer, T.L.; Manecke, G.R., Jr. Pulse Wave Transit Time Measurements of Cardiac Output in Patients Undergoing Partial Hepatectomy: A Comparison of the esCCO System with Thermodilution. Anesth. Analg. 2013, 117, 1307–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturgill, M.G.; Kelly, M.; Notterman, D.A. Pharmacology of the Cardiovascular System. In Pediatric Critical Care, 4th ed.; Elsevier: Philadelphia, PA, USA, 2011; pp. 277–305. [Google Scholar]
- Trammel, J.; Sapra, A. Physiology, Systemic Vascular Resistance. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Niwa, H.; Sugimura, M.; Satoh, Y.; Tanimoto, A. Cardiovascular Response to Epinephrine-Containing Local Anesthesia in Patients with Cardiovascular Disease. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Stratton, J.R.; Pfeifer, M.A.; Ritchie, J.L.; Halter, J.B. Hemodynamic Effects of Epinephrine: Concentration-Effect Study in Humans. J. Appl. Physiol. 1985, 58, 1199–1206. [Google Scholar] [CrossRef]
- Wakita, R.; Ito, T.; Fukayama, H. Small Doses of Adrenaline Contained in The Local Anaesthetic may Result in Prolonged Increased Cardiac Function Even after The Vital Signs Return to Normal. Adv. Oral Maxillofac. Surg. 2021, 3, 100–104. [Google Scholar] [CrossRef]
- Mol, A.; Meskers, C.G.M.; Niehof, S.P.; Maier, A.B.; van Wezel, R.J.A. Pulse Transit Time as a Proxy for Vasoconstriction in Younger and Older Adults. Exp. Gerontol. 2020, 135, 110938. [Google Scholar] [CrossRef]
- Kimoto, E.; Shoji, T.; Shinohara, K.; Inaba, M.; Okuno, Y.; Miki, T.; Koyama, H.; Emoto, M.; Nishizawa, Y. Preferential Stiffening of Central over Peripheral Arteries in Type 2 Diabetes. Diabetes 2003, 52, 448–452. [Google Scholar] [CrossRef] [Green Version]
- Pagoulatou, S.; Adamopoulos, D.; Rovas, G.; Bikia, V.; Stergiopulos, N. Acute and Long-Term Effects of Aortic Compliance Decrease on Central Hemodynamics: A Modeling Analysis. Front. Physiol. 2021, 12, 701154. [Google Scholar] [CrossRef] [PubMed]
- Hey, S.; Gharbi, A.; Haaren, B.v.; Walter, K.; König, N.; Löffler, S. Continuous Noninvasive Pulse Transit Time Measurement for Psychophysiological Stress Monitoring. In Proceedings of the International Conference on Ehealth, Telemedicine, and Social Medicine, Cancun, Mexico, 1–7 February 2009; pp. 113–116. [Google Scholar] [CrossRef]
- Susilo, C.W.; Fauziah, E. Respiratory Rate as a Physiological Response to Dental Anxiety. In Proceedings of the 11th International Dentistry Scientific Meeting, Jakarta, Indonesia, 16–17 September 2018. [Google Scholar] [CrossRef] [Green Version]
- Dionne, R.A.; Goldstein, D.S.; Wirdzek, P.R. Effects of Diazepam Premedication and Epinephrine-Containing Local Anesthetic on Cardiovascular and Plasma Catecholamine Responses to Oral Surgery. Anesth. Analg. 1984, 63, 640–646. [Google Scholar] [CrossRef] [PubMed]
- McGaugh, J.L. The Amygdala Modulates the Consolidation of Memories of Emotionally Arousing Experiences. Annu. Rev. Neurosci. 2004, 27, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glannon, W. Psychopharmacology and Memory. J. Med. Ethics. 2006, 32, 74–78. [Google Scholar] [CrossRef]
- Tank, A.W.; Lee Wong, D. Peripheral and Central Effects of Circulating Catecholamines. Compr. Physiol. 2015, 5, 1–15. [Google Scholar] [CrossRef]
- Motiejunaite, J.; Amar, L.; Vidal-Petiot, E. Adrenergic Receptors and Cardiovascular Effects of Catecholamines. Ann. Endocrinol. 2021, 82, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.L.; Kim, S.H. Pulse Wave Velocity in Atherosclerosis. Front. Cardiovasc. Med. 2019, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Schneck, E.; Drubel, P.; Schürg, R.; Markmann, M.; Kohl, T.; Henrich, M.; Sander, M.; Koch, C. Evaluation of Pulse Wave Transit Time Analysis for Non-invasive Cardiac Output Quantification in Pregnant Patients. Sci. Rep. 2020, 10, 1857. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Descriptive Analysis | Univariate Analysis | ||
|---|---|---|---|---|
| Overall Cases (n = 485) | LPV (n = 357) | SPV (n = 128) | p Value | |
| Age (year) | 49 (17) | 48.1 (17) | 52.3 (17) | 0.018 * |
| Gender | <0.003 * | |||
| Male | 188 (38.8%) | 122 (64.9%) | 66 (35.1%) | |
| Female | 297 (61.2%) | 235 (79.1%) | 62 (20.9%) | |
| ASA | 0.008 * | |||
| I | 225 (46.4%) | 180 (37.1%) | 45 (9.3%) | |
| II | 256 (52.8%) | 175 (36.1%) | 81 (16.7%) | |
| III | 4 (0.8%) | 2 (0.4%) | 2 (0.4%) | |
| Weight (kg) | 60.5 (13) | 58.5 (13) | 62.5 (13) | 0.004 * |
| Height (m) | 1.6 (0.1) | 1.62 (0.1) | 1.64 (0.1) | 0.034 * |
| Body mass index (kg/m2) | 22.5 (4) | 22 (4) | 23 (4) | 0.019 * |
| Midazolam (mg) | 2 (0–5.9) | 2 (0–5.9) | 2 (0–5) | 0.973 |
| Epinephrine use in LA (µg) | 43 (20) | 49.9 (23) | 35.5 (17) | <0.001 * |
| PWTTMAX (ms) | 227 (168–301) | 228 (168–301) | 220 (179–269) | 0.048 * |
| PWTTMIN (ms) | 202 (146–270) | 198 (146–270) | 212 (168–265) | 0.551 |
| SBPBL (mmHg) | 115 (85–161) | 115 (85–160) | 117 (86–182) | 0.197 |
| SBPLA (mmHg) | 116 (79–182) | 117 (86–182) | 116 (79–173) | 0.536 |
| HRBL (bpm) | 72 (42–122) | 72 (42–122) | 72 (48–102) | 0.896 |
| HRLA (bpm) | 78 (45–128) | 78 (45–128) | 77 (45–112) | 0.766 |
| Variables | LPV | SPV | p Value |
|---|---|---|---|
| (n = 357) | (n = 128) | ||
| ΔPWTT (ms) | 31 ((−15)–(−88)) | 10 ((−14)–6) | <0.001 * |
| ΔSBP (mmHg) | 0 ((−39)–63) | −1 ((−43)–32) | 0.072 |
| ΔHR (bpm) | 5 ((−36)–180) | 3 ((−14)–179) | 0.626 |
| Variables 1 | Descriptive Analysis | Univariate Analysis | ||
|---|---|---|---|---|
| Overall Cases (n = 485) | LPV (n = 357) | SPV (n = 128) | p Value | |
| Hypertension | 128 (26.4%) | 77 (60.2%) | 51 (39.8%) | <0.001 * |
| Cardiac disease | 21 (4.3%) | 11 (52.4%) | 10 (47.6%) | 0.024 * |
| Hepatitis C | 2 (0.4%) | 0 (0%) | 2 (1.6%) | 0.018 * |
| Cerebral hemorrhage | 3 (0.6%) | 3 (100%) | 0 (0%) | 0.298 |
| Cerebral infarction | 3 (0.6%) | 2 (66.7%) | 1 (33.3%) | 0.784 |
| Epilepsy | 10 (2.1%) | 7 (70%) | 3 (30%) | 0.794 |
| Depression | 15 (3.1%) | 11 (73.3%) | 4 (26.7%) | 0.98 |
| Other mental illness | 44 (9.1%) | 32 (72.7%) | 12 (27.3%) | 0.69 |
| Asthma | 47 (9.7%) | 36 (76.6%) | 11 (23.4%) | 0.619 |
| Emphysema | 2 (0.4%) | 1 (50%) | 1 (50%) | 0.448 |
| Other respiratory disease | 18 (3.7%) | 14 (77.8%) | 4 (22.2%) | 0.683 |
| Liver/biliary tract disease | 1 (0.2%) | 1 (100%) | 0 (0%) | 0.549 |
| Kidney/urinary disease | 10 (2.1%) | 7 (70%) | 3 (30%) | 0.797 |
| Obesity 2 | 62 (12.7%) | 39 (62.9%) | 23 (37.1%) | 0.041 * |
| Diabetes | 21 (4.3%) | 12 (57.2%) | 9 (42.8%) | 0.08 |
| Other metabolic disease | 10 (2.1%) | 9 (90%) | 1 (10%) | 0.235 |
| Gynecological disease | 7 (1.4%) | 6 (85.7%) | 1 (14.3%) | 0.464 |
| Dental treatment phobia | 214 (44.1%) | 156 (72.9%) | 58 (27.1%) | 0.711 |
| Glaucoma | 20 (4.1%) | 13 (65%) | 7 (35%) | 0.372 |
| Hyperactive pharyngeal reflex | 46 (9.5%) | 32 (69.6%) | 14 (30.4%) | 0.513 |
| Hyperlipidemia | 45 (9.3%) | 30 (66.7%) | 15 (33.3%) | 0.267 |
| Autoimmune disease | 13 (2.7%) | 12 (92.3%) | 1 (7.7%) | 0.121 |
| Vasovagal syncope | 11 (2.3%) | 7 (63.6%) | 4 (36.4%) | 0.448 |
| Alcohol consumption | 141 (29.1%) | 103 (73%) | 38 (27%) | 0.833 |
| Smokers | 42 (8.6%) | 33 (78.6%) | 9 (21.4%) | 0.458 |
| Characteristics | B (sd) | Odds Ratio (95% CI) | p Value |
|---|---|---|---|
| Age (years) | −0.025 (0.009) | 0.974 (0.96–0.99) | 0.006 * |
| Local anesthesia cartridge (1.8 mL) | 0.868 (0.158) | 2.417 (1.7–3.2) | <0.001 * |
| Hypertension (Yes) | 0.663 (0.303) | 1.896 (1.07–3.5) | 0.028 * |
| Dental treatment phobia (Yes) | 0.591 (0.264) | 1.74 (1.07–3.03) | 0.025 * |
| Constant | −0.614 (1.221) | 0.541 (-) | 0.615 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budiman, H.; Wakita, R.; Ito, T.; Maeda, S. Factors Associated with Variability in Pulse Wave Transit Time Using Pulse Oximetry: A Retrospective Study. J. Clin. Med. 2022, 11, 3963. https://doi.org/10.3390/jcm11143963
Budiman H, Wakita R, Ito T, Maeda S. Factors Associated with Variability in Pulse Wave Transit Time Using Pulse Oximetry: A Retrospective Study. Journal of Clinical Medicine. 2022; 11(14):3963. https://doi.org/10.3390/jcm11143963
Chicago/Turabian StyleBudiman, Hilmanda, Ryo Wakita, Takaya Ito, and Shigeru Maeda. 2022. "Factors Associated with Variability in Pulse Wave Transit Time Using Pulse Oximetry: A Retrospective Study" Journal of Clinical Medicine 11, no. 14: 3963. https://doi.org/10.3390/jcm11143963