
Anterior Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Transmuscular Quadratus Lumborum Block for Analgesia after Elective Cesarean Section: A Randomized Controlled Trial


 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Subjects
2.3. Anesthesia Management
2.4. Study Intervention
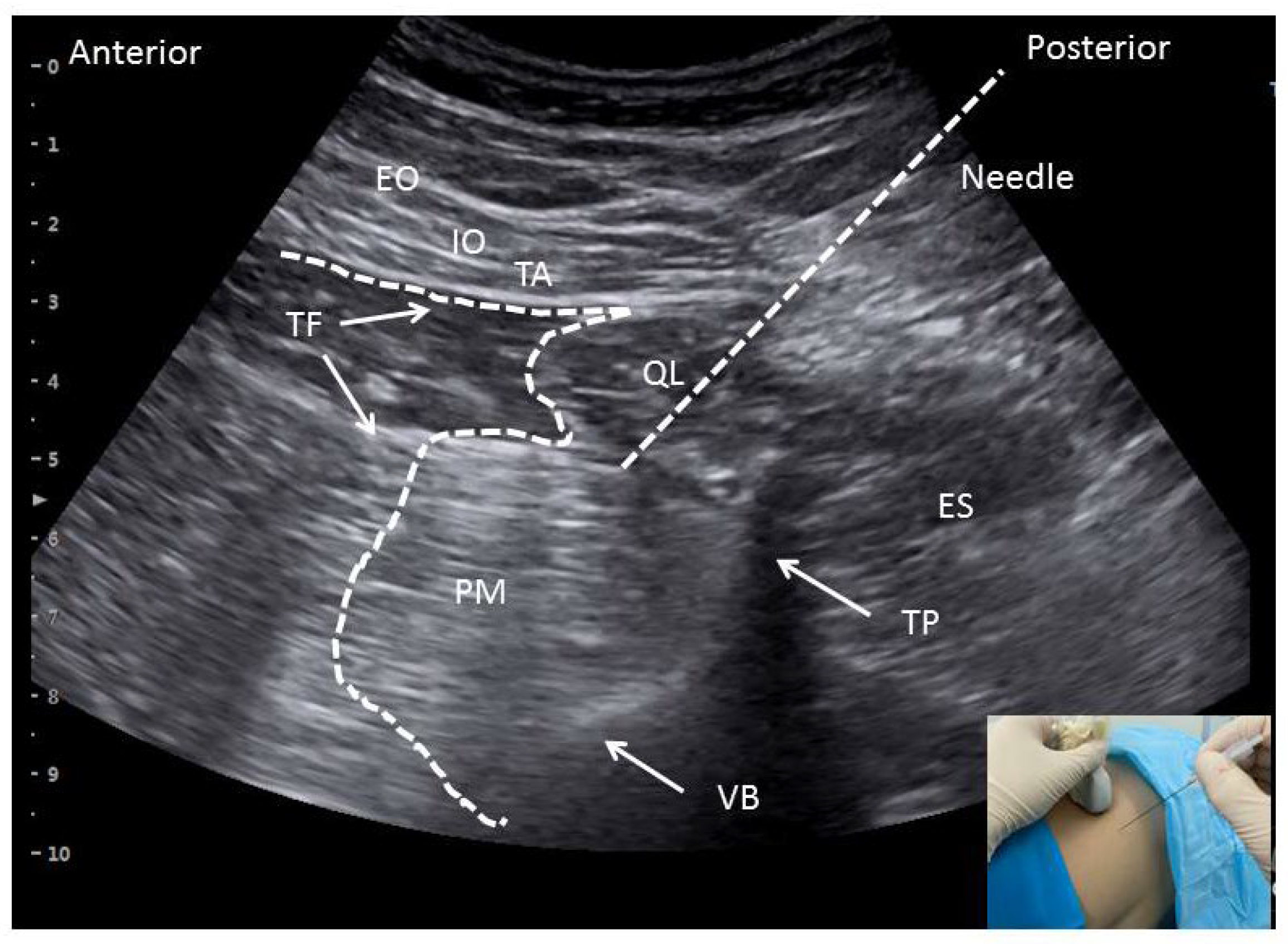
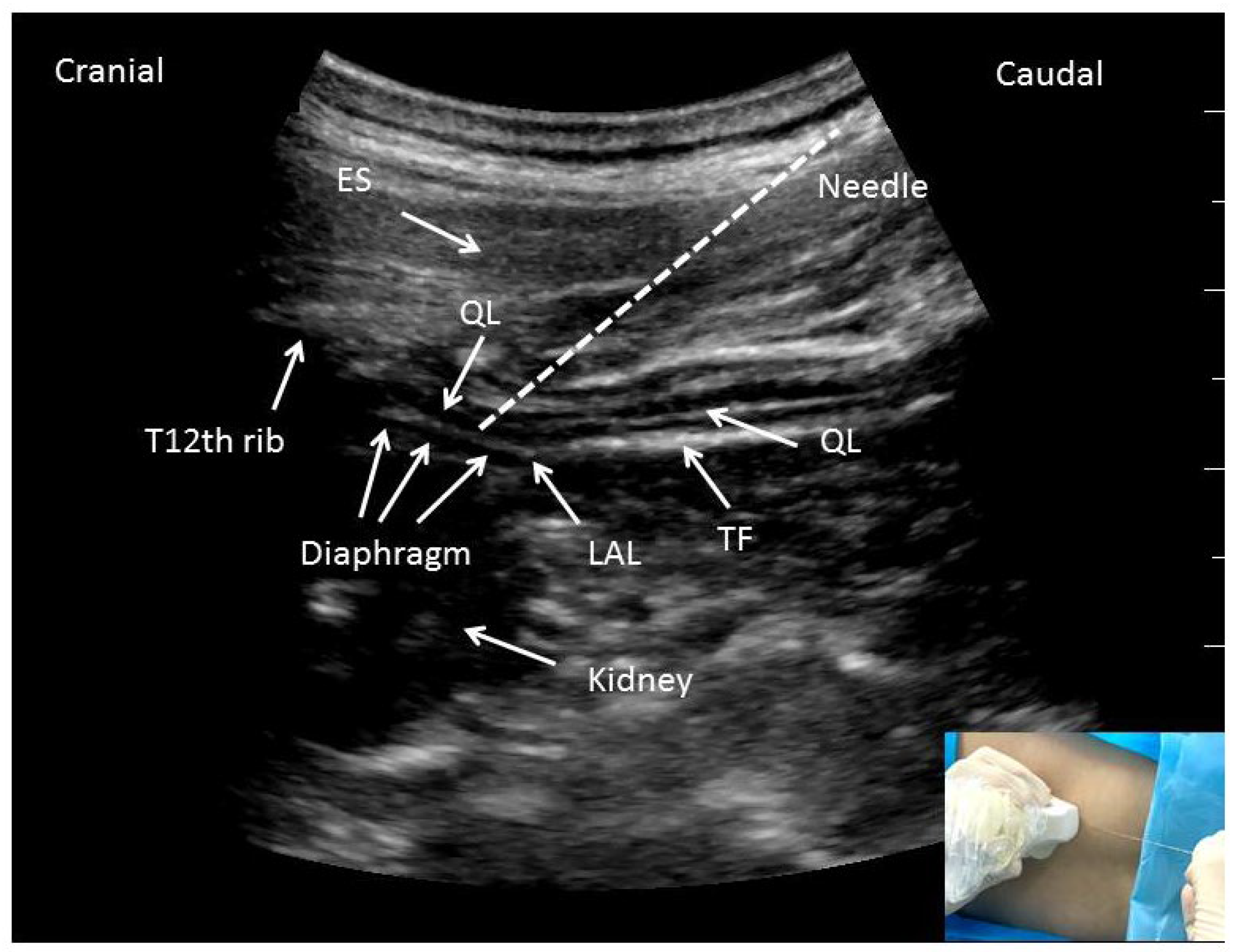
2.5. Surgery and Block Procedure
2.6. Postoperative Pain Management and Outcomes Assessments
2.7. Sample Size Calculation and Statistical Analysis
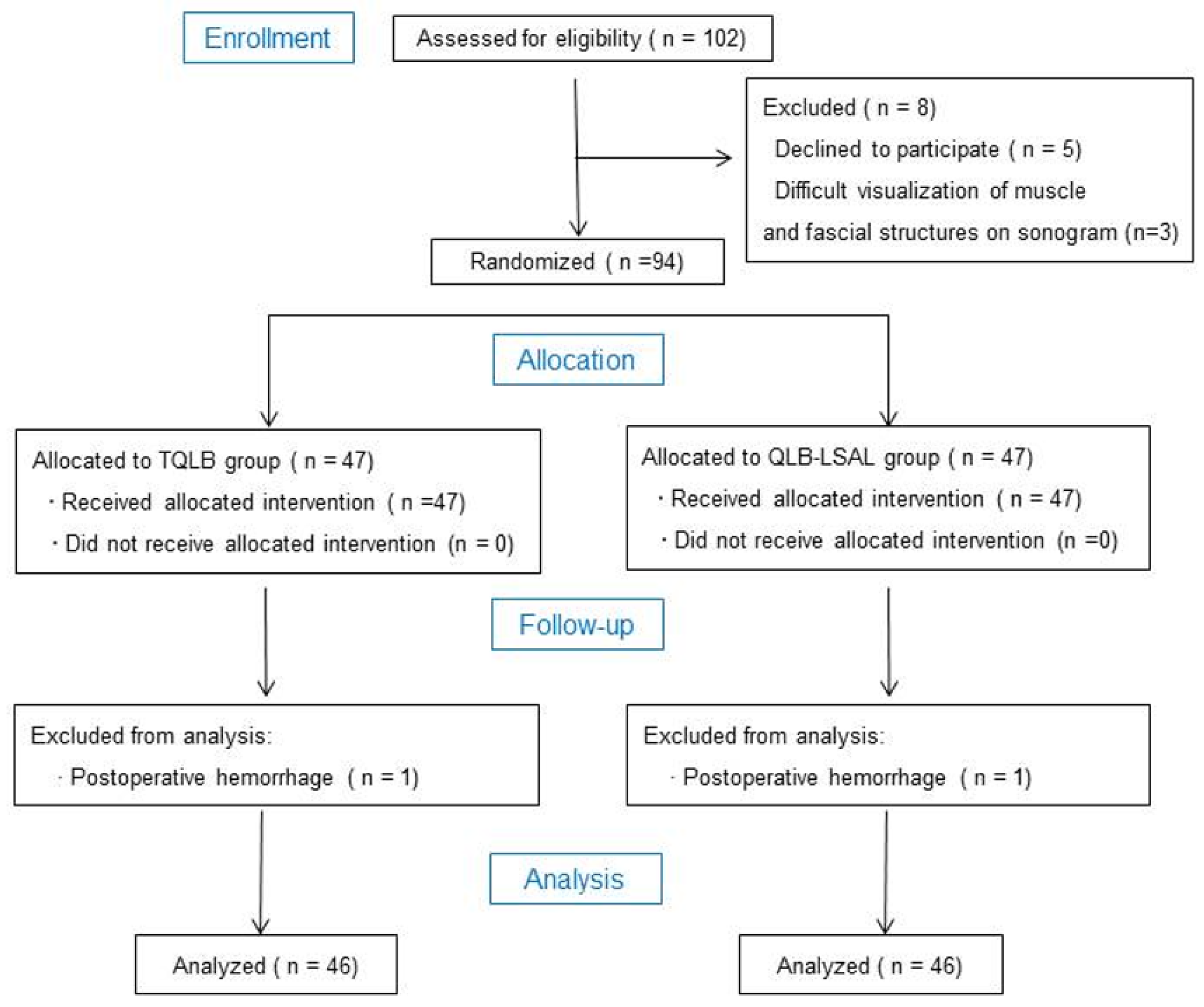
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Clinical Trial Registry
References
- Jasim, H.H.; Sulaiman, S.A.B.S.; Khan, A.H. Factors Affecting Post Caesarean Pain Intensity among Women in the Northern Peninsular of Malaysia. J. Clin. Diagn. Res. JCDR 2017, 11, IC07–IC11. [Google Scholar] [CrossRef] [PubMed]
- Roofthooft, E.; Joshi, G.; Rawal, N.; Van de Velde, M. PROSPECT guideline for elective caesarean section: Updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia 2021, 76, 665–680. [Google Scholar] [CrossRef]
- Huang, J.; Cao, C.; Nelson, G.; Wilson, R. A Review of Enhanced Recovery after Surgery Principles Used for Scheduled Caesarean Delivery. J. Obstet. Gynaecol. Can. JOGC 2019, 41, 1775–1788. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, B.; Butwick, A. Postcesarean delivery analgesia. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 69–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, N.P.; Makkar, J.K.; Borle, A.; Monks, D.; Goudra, B.G.; Zorrilla-Vaca, A.; Singh, P.M. The analgesic efficacy of quadratus lumborum block in caesarean delivery: A meta-analysis and trial sequential analysis. J. Anesth. 2020, 34, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Fay, E.E.; Hitti, J.E.; Delgado, C.M.; Savitsky, L.M.; Mills, E.B.; Slater, J.L.; Bollag, L.A. An enhanced recovery after surgery pathway for cesarean delivery decreases hospital stay and cost. Am. J. Obstet. Gynecol. 2019, 221, e1–e349. [Google Scholar] [CrossRef]
- Teigen, N.C.; Sahasrabudhe, N.; Doulaveris, G.; Xie, X.; Negassa, A.; Bernstein, J.; Bernstein, P.S. Enhanced recovery after surgery at cesarean delivery to reduce postoperative length of stay: A randomized controlled trial. Am. J. Obstet. Gynecol. 2020, 222, e1–e372. [Google Scholar] [CrossRef]
- Riemma, G.; Schiattarella, A.; Cianci, S.; La Verde, M.; Morlando, M.; Sisti, G.; Esposito, I.; Della Corte, L.; Sansone, P.; De Franciscis, P. Transversus abdominis plane block versus wound infiltration for post-cesarean section analgesia: A systematic review and meta-analysis of randomized controlled trials. Int. J. Gynaecol. Obstet. 2021, 153, 383–392. [Google Scholar] [CrossRef]
- Fusco, P.; Cofini, V.; Petrucci, E.; Scimia, P.; Pozone, T.; Paladini, G.; Carta, G.; Necozione, S.; Borghi, B.; Marinangeli, F. Transversus Abdominis Plane Block in the Management of Acute Postoperative Pain Syndrome after Caesarean Section: A Randomized Controlled Clinical Trial. Pain Physician 2016, 19, 583–591. [Google Scholar]
- Blanco, R.; Ansari, T.; Riad, W.; Shetty, N. Quadratus Lumborum Block Versus Transversus Abdominis Plane Block for Postoperative Pain after Cesarean Delivery: A Randomized Controlled Trial. Reg. Anesth. Pain Med. 2016, 41, 757–762. [Google Scholar] [CrossRef]
- Rincón, C.; Moreno, D.; Moore, A. Erector spinae plane block for post-cesarean delivery analgesia. Int. J. Obstet. Anesth. 2020, 41, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.K.; Dam, M.; Steingrimsdottir, G.E.; Laier, G.H.; Lebech, M.; Poulsen, T.D.; Chan, V.W.; Wolmarans, M.; Bendtsen, T.F.; Børglum, J. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: A double-blind randomized trial. Reg. Anesth. Pain Med. 2019, 44, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.; Lu, D.; Yang, X.; Zhou, Z.; Chen, X.; Chen, K.; Zhou, X.; Feng, X. Postoperative analgesic effects of various quadratus lumborum block approaches following cesarean section: A randomized controlled trial. J. Pain Res. 2019, 12, 2305–2312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brglum, J.; Moriggl, B.; Lnnqvist, P.A.; Christensen, A.F.; Bendtsen, T.F. Ultrasound-Guided Transmuscular Quadratus Lumborum Blockade. BJA Br. J. Anaesth. 2013, 111. [Google Scholar] [CrossRef]
- Li, H.; Liang, J.; Shao, P.; Zheng, J.; Shi, R.; Wang, Y. Supra-Arcuate Ligament Blocks: Anatomy, Mechanisms, and Techniques. J. Pain Res. 2021, 14, 3837–3848. [Google Scholar] [CrossRef]
- Li, H.; Shi, R.; Shi, D.; Wang, R.; Liu, Y.; Wang, Y. Anterior quadratus lumborum block at the lateral supra-arcuate ligament versus transmuscular quadratus lumborum block for postoperative analgesia in patients undergoing laparoscopic nephrectomy: A randomized controlled trial. J. Clin. Anesth. 2021, 75, 110561. [Google Scholar] [CrossRef]
- Shi, R.; Li, H.; Wang, Y. Dermatomal coverage of single-injection ultrasound-guided parasagittal approach to anterior quadratus lumborum block at the lateral supra-arcuate ligament. J. Anesth. 2021, 35, 307–310. [Google Scholar] [CrossRef]
- Nielsen, M.; Bendtsen, T.; Børglum, J. Superiority of ultrasound-guided Shamrock lumbar plexus block. Minerva Anestesiol. 2018, 84, 115–121. [Google Scholar] [CrossRef]
- Dam, M.; Hansen, C.K.; Poulsen, T.D.; Azawi, N.H.; Wolmarans, M.; Chan, V.; Laier, G.H.; Bendtsen, T.F.; Børglum, J. Transmuscular quadratus lumborum block for percutaneous nephrolithotomy reduces opioid consumption and speeds ambulation and discharge from hospital: A single centre randomised controlled trial. Br. J. Anaesth. 2019, 123, e350–e358. [Google Scholar] [CrossRef]
- Huang, X.; Sun, Y.; Shi, R.; Ma, D.; Wu, A.; Wang, Y.; Yang, Y. Comparison of ultrasound-guided anterior quadratus lumborum block at the lateral supra-arcuate ligament with posterior quadratus lumborum block for perioperative analgesia in laparoscopic nephrectomy: A protocol for a randomised, prospective, parallel group, non-inferior trial. BMJ Open 2021, 11, e048490. [Google Scholar]
- Suzuki, H.; Kamiya, Y.; Fujiwara, T.; Yoshida, T.; Takamatsu, M.; Sato, K. Intrathecal morphine versus epidural ropivacaine infusion for analgesia after Cesarean section: A retrospective study. JA Clin. Rep. 2015, 1, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stopar-Pintaric, T.; Blajic, I.; Visic, U.; Znider, M.; Plesnicar, A.; Vlassakov, K.; Lucovnik, M. Posteromedial quadratus lumborum block versus wound infiltration after caesarean section: A randomised, double-blind, controlled study. Eur. J. Anaesthesiol. 2021, 38, S138–S144. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Taylor, C.; Weikel, D.; Barton, K.; Habib, A. Quadratus lumborum block for postoperative analgesia after cesarean delivery: A systematic review with meta-analysis and trial-sequential analysis. J. Clin. Anesth. 2020, 67, 110003. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.; Dam, M.; Bendtsen, T.; Børglum, J. Ultrasound-Guided Quadratus Lumborum Blocks: Definition of the Clinical Relevant Endpoint of Injection and the Safest Approach. AA Pract. 2016, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawy, H.; El-Boghdadly, K.; Barrington, M. Quadratus Lumborum Block: Anatomical Concepts, Mechanisms, and Techniques. Anesthesiology 2019, 130, 322–335. [Google Scholar] [CrossRef]
- Elsharkawy, H.; El-Boghdadly, K.; Kolli, S.; Esa, W.A.; DeGrande, S.; Soliman, L.M.; Drake, R.L. Injectate spread following anterior sub-costal and posterior approaches to the quadratus lumborum block: A comparative cadaveric study. Eur. J. Anaesthesiol. 2017, 34, 587–595. [Google Scholar] [CrossRef]
- Steingrímsdóttir, G.; Hansen, C.; Børglum, J. Ultrasound-guided transmuscular quadratus lumborum catheters for elective caesarean section: A protocol for a single-centre, double-blind randomised trial. Acta Anaesthesiol. Scand. 2020, 64, 1218–1223. [Google Scholar] [CrossRef]
- Koksal, E.; Aygun, H.; Genç, C.; Kaya, C.; Dost, B. Comparison of the analgesic effects of two quadratus lumborum blocks (QLBs), QLB type II vs QLB type III, in caesarean delivery: A randomised study. Int. J. Clin. Pract. 2021, 75, e14513. [Google Scholar] [CrossRef]
- Li, H.; Shi, R.; Wang, Y. Use of transmuscular quadratus lumborum block for postoperative analgesia after laparoscopic nephrectomy. Reg. Anesth. Pain Med. 2021, 46, 1118–1119. [Google Scholar] [CrossRef]
- Roda, R.; Uppal, V.; Allen, V.; Woolcott, C.; McKeen, D. The addition of lateral quadratus lumborum block to a multimodal analgesic regimen that includes intrathecal morphine is associated with a longer time to first analgesic request for elective cesarean section. J. Clin. Anesth. 2020, 61, 109667. [Google Scholar] [CrossRef]
- Adhikary, S.; Short, A.; El-Boghdadly, K.; Abdelmalak, M.; Chin, K. Transmuscular quadratus lumborum versus lumbar plexus block for total hip arthroplasty: A retrospective propensity score matched cohort study. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 372–378. [Google Scholar] [PubMed]
- Uppal, V.; Retter, S.; Kehoe, E.; McKeen, D. Quadratus lumborum block for postoperative analgesia: A systematic review and meta-analysis. Can. J. Anaesth./J. Can. D’anesthesie 2020, 67, 1557–1575. [Google Scholar] [CrossRef] [PubMed]
- Hussain, N.; Brull, R.; Weaver, T.; Zhou, M.; Essandoh, M.; Abdallah, F.W. Postoperative Analgesic Effectiveness of Quadratus Lumborum Block for Cesarean Delivery under Spinal Anesthesia. Anesthesiology 2021, 134, 72–87. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | TQLB Group | QLB-LSAL Group |
|---|---|---|
| Number | 46 | 46 |
| Age (years) | 31.7 ± 4.6 | 32.7 ± 3.6 |
| Height (cm) | 160.3 ± 5.4 | 159.8 ± 4.8 |
| Weight (kg) | 70.1 ± 8.8 | 70.5 ± 8.0 |
| BMI (kg/m2) | 27.4 ± 6.5 | 27.9 ± 4.6 |
| ASA classification, n (%) | ||
| ASA class I–II | 43 (93.5%) | 42 (91.3%) |
| ASA class III | 3 (6.5%) | 4 (8.7%) |
| Duration of surgery (min) | 41.5 ± 8.3 | 43.2 ± 6.8 |
| Blood loss (mL) | 320.6 ± 42.5 | 312.8 ± 36.4 |
| TQLB Group | QLB-LSAL Group | p | |
|---|---|---|---|
| Intravenous sufentanil consumption in first 24 h after surgery (μg) | 39.4 ± 9.6 | 29.4 ± 5.7 | p < 0.001 |
| Number of cases requiring rescue analgesia during initial 24 h (%) | 5 (10.8%) | 4 (8.7%) | 0.727 |
| Postoperative pain intensity at rest, median (IQR) | |||
| NRS at 4 h | 2.0 (1.0–3.3) | 1.8 (1.2–2.4) | 0.191 |
| NRS at 8 h | 2.2(1.2–3.1) | 2.1 (1.4–2.8) | 0.761 |
| NRS at 12 h | 2.3 (1.6–3.0) | 1.8 (1.2–2.7) | 0.064 |
| NRS at 24 h | 2.3 (1.5–3.7) | 2.2 (1.4–3.2) | 0.305 |
| Postoperative pain intensity on movement, median (IQR) | |||
| NRS at 4 h | 2.9 (1.5–4.9) | 2.6 (1.9–3.5) | 0.417 |
| NRS at 8 h | 3.2 (2.6–4.2) | 2.9 (2.3–4.4) | 0.400 |
| NRS at 12 h | 3.5 (2.7–4.4) | 3.2 (2.5–4.4) | 0.351 |
| NRS at 24 h | 3.7 (2.5–5.2) | 3.6 (2.9–4.5) | 0.635 |
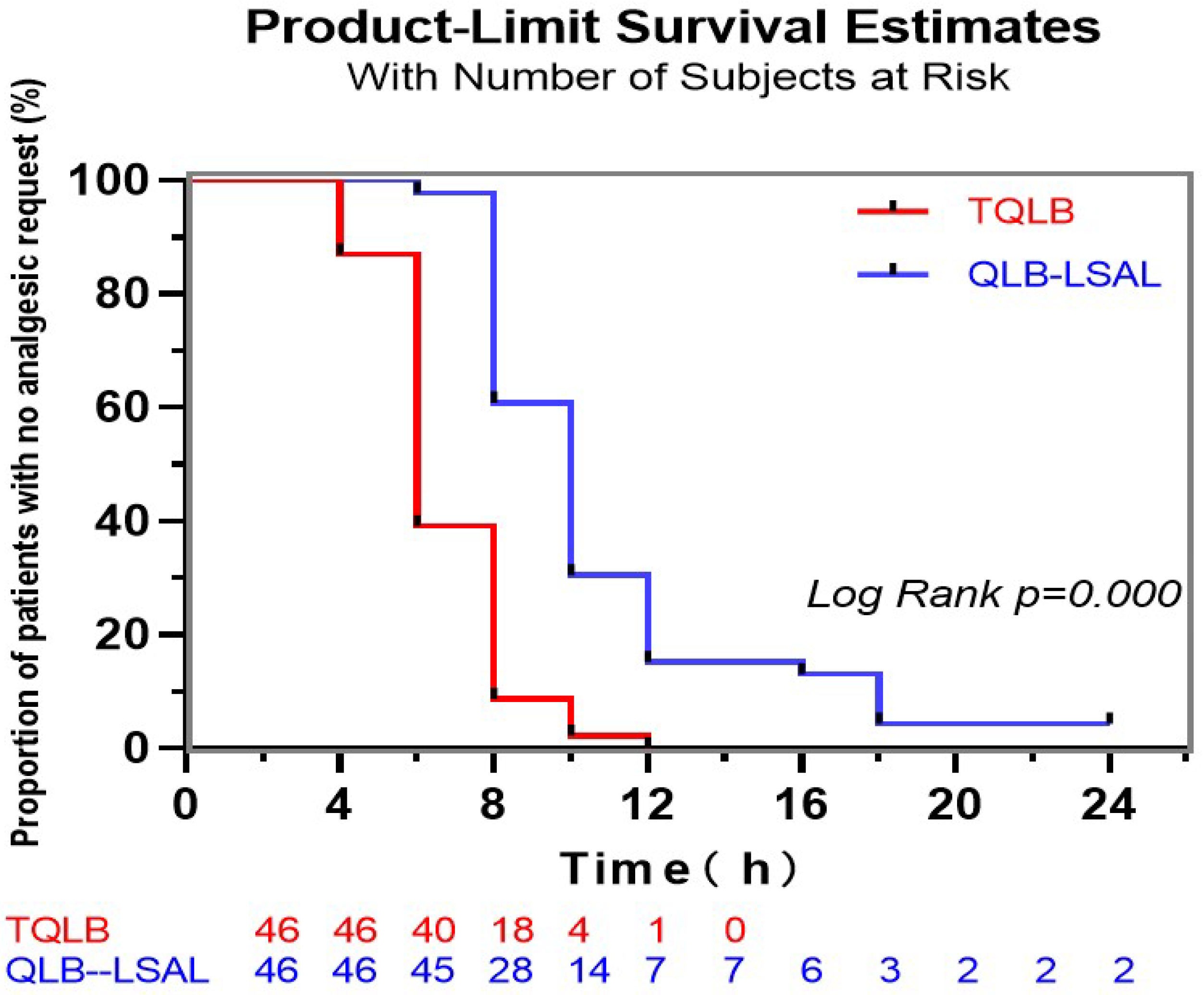
| First time to opioid request (h) | 6.7 ± 1.8 | 10.9 ± 4.1 | p < 0.001 |
| Postoperative nausea | 2 (4.3%) | 3 (6.5%) | 0.647 |
| Episodes of vomiting | 2 (4.3%) | 2 (4.3%) | 1.000 |
| Pruritus | 2 (4.3%) | 2 (4.3%) | 1.000 |
| lower limb weakness | 1 (2.2%) | 0 (0.0%) | 0.317 |
| Patient satisfaction score, median (IQR) | 1 (1–2) | 1 (1–2) | 0.525 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, M.; Lei, B.; Li, H.; Gao, X.; Zhang, T.; Liang, Z.; Wang, Y.; Wang, L. Anterior Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Transmuscular Quadratus Lumborum Block for Analgesia after Elective Cesarean Section: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 3827. https://doi.org/10.3390/jcm11133827
Guo M, Lei B, Li H, Gao X, Zhang T, Liang Z, Wang Y, Wang L. Anterior Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Transmuscular Quadratus Lumborum Block for Analgesia after Elective Cesarean Section: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(13):3827. https://doi.org/10.3390/jcm11133827
Chicago/Turabian StyleGuo, Min, Bo Lei, Huili Li, Xiaoru Gao, Tianshu Zhang, Ziwei Liang, Yun Wang, and Lei Wang. 2022. "Anterior Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Transmuscular Quadratus Lumborum Block for Analgesia after Elective Cesarean Section: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 13: 3827. https://doi.org/10.3390/jcm11133827