
Does an Adjustable-Loop Device Loosen following ACL Reconstruction with a Hamstring Graft? A Retrospective Study with a Follow-Up of Two Years


 , ,
, ,
Abstract
:1. Introduction
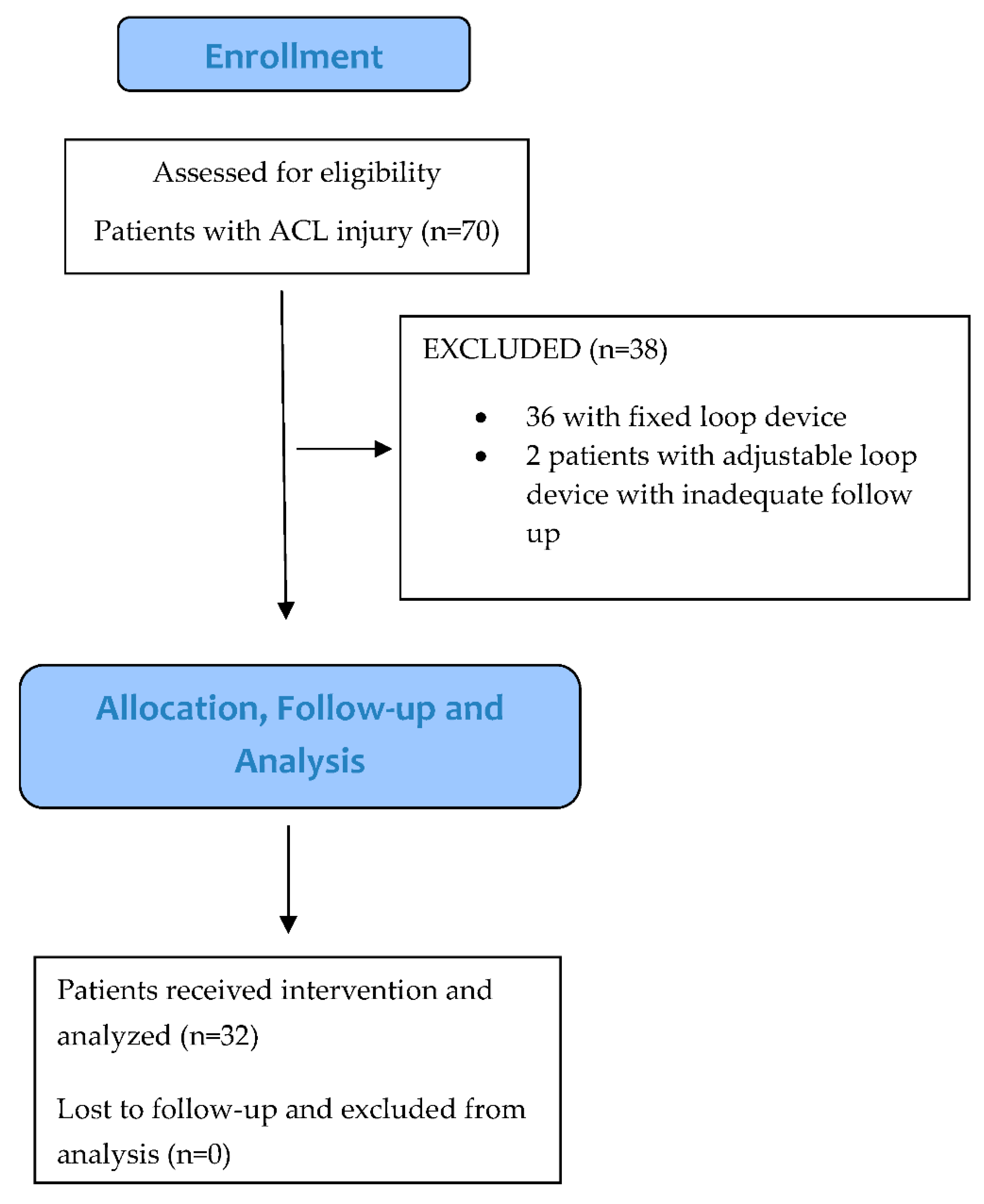
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eguchi, A.; Ochi, M.; Adachi, N.; Deie, M.; Nakamae, A.; Usman, M.A. Mechanical properties of suspensory fixation devices for anterior cruciate ligament reconstruction: Comparison of the fixed-length loop device versus the adjustable-length loop device. Knee 2014, 21, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Barrow, A.E.; Pilia, M.; Guda, T.; Kadrmas, W.R.; Burns, T.C. Femoral suspension devices for anterior cruciate ligament reconstruction: Do adjustable loops lengthen? Am. J. Sports Med. 2014, 42, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Lubowitz, J.H.; Amhad, C.H.; Anderson, K. All-inside anterior cruciate ligament graft-link technique: Second-generation, no-incision anterior cruciate ligament reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.-H.; Yang, B.-S.; Victoroff, B.N. Clinical and radiological outcomes after hamstring anterior cruciate ligament reconstructions: Comparison between fixed-loop and adjustable-loop cortical suspension devices. Am. J. Sports Med. 2017, 45, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.S.; Smith, S.D.; LaPrade, C.M.; Turnbull, T.L.; LaPrade, R.F.; Wijdicks, C.A. A biomechanical comparison of femoral cortical suspension devices for soft tissue anterior cruciate ligament reconstruction under high loads. Am. J. Sports Med. 2015, 43, 154–160. [Google Scholar] [CrossRef]
- Petre, B.M.; Smith, S.D.; Jansson, K.S.; de Meijer, P.-P.; Hackett, T.R.; LaPrade, R.F.; Wijdicks, C.A. Femoral cortical suspension devices for soft tissue anterior cruciate ligament reconstruction: A comparative biomechanical study. Am. J. Sports Med. 2013, 41, 416–422. [Google Scholar] [CrossRef]
- Noonan, B.C.; Dines, J.S.; Allen, A.A.; Altchek, D.W.; Bedi, A. Biomechanical evaluation of an adjustable loop suspensory anterior cruciate ligament reconstruction fixation device: The value of retensioning and knot tying. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 2050–2059. [Google Scholar] [CrossRef]
- Singh, S.; Shaunak, S.; Shaw, S.C.; Anderson, J.L.; Mandalia, V. Adjustable loop femoral cortical suspension devices for anterior cruciate ligament reconstruction: A systematic review. Indian J. Orthop. 2020, 54, 426–443. [Google Scholar] [CrossRef]
- Agrawal, N.K.; Khan, M.J.; Sherwani, M.K.A.; Zahid, M.; Ahmad, S.; Shukla, I. Short-course perioperative antibiotic prophylaxis to prevent surgical site infection in elective orthopedic surgery. J. Orthop. Traumatol. Rehabil. 2018, 10, 67. [Google Scholar]
- Wang, J.H.; Lee, E.S.; Lee, B.H. Paradoxical tunnel enlargement after ACL reconstruction with hamstring autografts when using β-TCP containing interference screws for tibial aperture fixation- prospectively comparative study. BMC Musculoskelet. Disord. 2017, 18, 398. [Google Scholar] [CrossRef]
- Collins, N.J.; Misra, D.; Felson, D.T.; Crossley, K.M.; Roos, E.M. Measures of knee function: International knee documentation committee (IKDC) subjective knee evaluation form, knee injury and osteoarthritis outcome score (KOOS), knee injury and osteoarthritis outcome score physical function short form (KOOS-PS), knee outcome survey activities of daily living scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res. 2011, 63 (Suppl. 11), S208–S228. [Google Scholar]
- Mulligan, E.P.; McGuffie, D.Q.; Coyner, K.; Khazzam, M. The reliability and diagnostic accuracy of assessing the translation endpoint during the lachman test. Int. J. Sports Phys. Ther. 2015, 10, 52. [Google Scholar] [PubMed]
- Seo, S.S.; Kim, C.W.; Kim, J.G.; Jin, S.Y. Clinical results comparing transtibial technique and outside in technique in single bundle anterior cruciate ligament reconstruction. Knee Surg. Relat. Res. 2013, 25, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angthong, C.; Chernchujit, B.; Apivatgaroon, A.; Chaijenkit, K.; Nualon, P.; Suchao-in, K. The anterior cruciate ligament reconstruction with the peroneus longus tendon: A biomechanical and clinical evaluation of the donor ankle morbidity. J. Med. Assoc. Thail. 2015, 98, 555–560. [Google Scholar]
- Plaweski, S.; Rossi, J.; Merloz, P. Anterior cruciate ligament reconstruction: Assessment of the hamstring autograft femoral fixation using the EndoButton CL®. Orthop. Traumatol. Surg. Res. 2009, 95, 606–613. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, S.A.-R.; Al-Kussary, I.M.; Al-Misfer, A.R.K.; Al-Mutairi, H.Q.; Ghafar, S.A.; El Noor, T.A. Clinical evaluation of arthroscopically assisted anterior cruciate ligament reconstruction: Patellar tendon versus gracilis and semitendinosus autograft. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 412–417. [Google Scholar] [CrossRef]
- Williams III, R.J.; Hyman, J.; Petrigliano, F.; Rozental, T.; Wickiewicz, T.L. Anterior cruciate ligament reconstruction with a four-strand hamstring tendon autograft. J. Bone Jt. Surg. Am. 2004, 86, 225–232. [Google Scholar] [CrossRef]
- Shahpari, O.; FallahKezabi, M.; Kalati, H.H.; Bagheri, F.; Ebrahimzadeh, M.H. Clinical outcome of anatomical transportal arthroscopic anterior cruciate ligament reconstruction with hamstring tendon autograft. Arch. Bone Jt. Surg. 2018, 6, 130. [Google Scholar]
- Khan, R.; Prasad, V.; Gangone, R.; Kinmont, J. Anterior cruciate ligament reconstruction in patients over 40 years using hamstring autograft. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 68–72. [Google Scholar] [CrossRef]
- Charlton, W.P.; Randolph, D.A.; Lemos, S.; Shields, C.L. Clinical outcome of anterior cruciate ligament reconstruction with quadrupled hamstring tendon graft and bioabsorbable interference screw fixation. Am. J. Sports Med. 2003, 31, 518–521. [Google Scholar] [CrossRef]
- Xu, Y.; Li, F.; Lu, H. Reconstruction of anterior cruciate ligament with different grafts under arthroscope in 68 cases. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2007, 21, 1163–1166. [Google Scholar] [PubMed]
- Kamien, P.M.; Hydrick, J.M.; Replogle, W.H.; Go, L.T.; Barrett, G.R. Age, graft size, and Tegner activity level as predictors of failure in anterior cruciate ligament reconstruction with hamstring autograft. Am. J. Sports Med. 2013, 41, 1808–1812. [Google Scholar] [CrossRef] [PubMed]
- Glasbrenner, J.; Domnick, C.; Raschke, M.J.; Willinghöfer, T.; Kittl, C.; Michel, P.; Wähnert, D.; Herbort, M. Adjustable buttons for ACL graft cortical fixation partially fail with cyclic loading and unloading. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2530–2536. [Google Scholar] [CrossRef] [PubMed]
- Boyle, M.J.; Vovos, T.J.; Walker, C.G.; Stabile, K.J.; Roth, J.M.; Garrett, W.E., Jr. Does adjustable-loop femoral cortical suspension loosen after anterior cruciate ligament reconstruction? A retrospective comparative study. Knee 2015, 22, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, R.; Gaba, S.; Goel, L.; Asif, N.; Kalra, M.; Kumar, R.; Kumar, A. In vivo comparison of a fixed loop (EndoButton CL) with an adjustable loop (TightRope RT) device for femoral fixation of the graft in ACL reconstruction: A prospective randomized study and a literature review. J. Orthop. Surg. 2018, 26, 2309499018799787. [Google Scholar] [CrossRef] [Green Version]
- Conner, C.S.; Perez, B.A.; Morris, R.P.; Buckner, J.W.; Buford, W.L., Jr.; Ivey, F.M. Three femoral fixation devices for anterior cruciate ligament reconstruction: Comparison of fixation on the lateral cortex versus the anterior cortex. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 796–807. [Google Scholar] [CrossRef]
- Weiler, A.; Peine, R.; Pashmineh-Azar, A.; Abel, C.; Südkamp, N.P.; Hoffmann, R.F. Tendon healing in a bone tunnel. Part I: Biomechanical results after biodegradable interference fit fixation in a model of anterior cruciate ligament reconstruction in sheep. Arthrosc. J. Arthrosc. Relat. Surg. 2002, 18, 113–123. [Google Scholar] [CrossRef]
- Tomita, F.; Yasuda, K.; Mikami, S.; Sakai, T.; Yamazaki, S.; Tohyama, H. Comparisons of intraosseous graft healing between the doubled flexor tendon graft and the bone–patellar tendon–bone graft in anterior cruciate ligament reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2001, 17, 461–476. [Google Scholar] [CrossRef]
- Toutoungi, D.; Lu, T.; Leardini, A.; Catani, F.; O’connor, J. Cruciate ligament forces in the human knee during rehabilitation exercises. Clin. Biomech. 2000, 15, 176–187. [Google Scholar] [CrossRef]
- Shelburne, K.B.; Torry, M.R.; Pandy, M.G. Muscle, ligament, and joint-contact forces at the knee during walking. Med. Sci. Sports Exerc. 2005, 37, 1948–1956. [Google Scholar] [CrossRef] [Green Version]
- Wise, B.T.; Patel, N.N.; Wier, G.; Labib, S.A. Outcomes of ACL reconstruction with fixed versus variable loop button fixation. Orthopedics 2017, 40, e275–e280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, L.D.; Taylor, M.K.; Park, D.; Ghodadra, N.; Marchant, M.; Pietrobon, R.; Cook, C.; International Knee Documentation Committee. Reliability and validity of the International Knee Documentation Committee (IKDC) Subjective Knee Form. Jt. Bone Spine 2007, 74, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Kilinc, B.E.; Kara, A.; Celik, H.; Oc, Y.; Camur, S. Evaluation of the accuracy of Lachman and Anterior Drawer Tests with KT1000 ın the follow-up of anterior cruciate ligament surgery. J. Exerc. Rehabil. 2016, 12, 363–367. [Google Scholar] [CrossRef] [PubMed]
- König, D.P.; Rütt, J.; Kumm, D.; Breidenbach, E. Diagnosis of anterior knee instability. Comparison between the lachman test, the kt-1,000 arthrometer and the ultrasound lachman test. Unfallchirurg 1998, 101, 209–213. [Google Scholar] [CrossRef]
- Wiertsema, S.H.; van Hooff, H.J.A.; Migchelsen, L.A.A.; Steultjens, M.P.M. Reliability of the KT1000 arthrometer and the Lachman test in patients with an ACL rupture. Knee 2008, 15, 107–110. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Mean | Number |
|---|---|---|
| Gender | ||
| Male (number) | 29 | |
| Female (number) | 03 | |
| Age (years) | 26.0 ± 7.2 (18–43) | |
| Time since the injury to surgery (months) | 10.3 ± 4.3 (3–18) | |
| Side involved | ||
| Right (number) | 21 (65.6%) | |
| Left (number) | 11 (34.4%) | |
| Medial meniscus tear (number of subjects) | 10 (31.2%) | |
| Lateral meniscus tear (number of subjects) | 4 (12.5%) | |
| Femoral tunnel length (mm) | 39.5 ± 3.8 (33–45) | |
| Graft diameter (mm) | 8.4 ± 0.64 (7.0–9.5) | |
| Quadrupled graft (mm) | 90.8 ± 8.1 (80–110) | |
| Follow-up period (months) | 34.2 ± 5.4 (26–44) | |
| Mechanism of injury (number of subjects) | ||
| Sports | 20 | |
| RTA | 08 | |
| Injury during daily routine activities | 04 |
| Pre-Operative | Post-Operative | p-Value | |
|---|---|---|---|
| Lachman Test | <0.001 a,* | ||
| Grade 0 | 0 (0%) | 27 (84.4%) | |
| Grade 1 | 1 (3.1%) | 5 (15.6%) | |
| Grade 2 | 5 (15.6%) | 0 | |
| Grade 3 | 26 (81.3%) | 0 | |
| Pivot Shift Test | 0.003 a,* | ||
| Grade 0 | 0 (0%) | 28 (87.5%) | |
| Grade 1 | 1 (3.1%) | 4 (12.5%) | |
| Grade 2 | 22 (68.8%) | 0 | |
| Grade 3 | 9 (28.1%) | 0 | |
| IKDC Score | 55.8 ± 8.1 (40.2–66.7) | 91.4 ± 3.6 (87.4–96.6) | <0.001 b,* |
| Lysholm Score | 73.0 ± 4.6 (65–80) | 96.9 ± 1.69 (95–100) | <0.001 b,* |
| Thigh Circumference (cm) | 1.8 ± 0.9 (1.0–4.0) | 1.0 ± 0.5 (0–2.5) | <0.001 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, M.J.; Asif, N.; Aziz, M.H.; Raza, A.; Anwar, S.; Nuhmani, S.; Alghadir, A.H.; Khan, M. Does an Adjustable-Loop Device Loosen following ACL Reconstruction with a Hamstring Graft? A Retrospective Study with a Follow-Up of Two Years. J. Clin. Med. 2022, 11, 3648. https://doi.org/10.3390/jcm11133648
Khan MJ, Asif N, Aziz MH, Raza A, Anwar S, Nuhmani S, Alghadir AH, Khan M. Does an Adjustable-Loop Device Loosen following ACL Reconstruction with a Hamstring Graft? A Retrospective Study with a Follow-Up of Two Years. Journal of Clinical Medicine. 2022; 11(13):3648. https://doi.org/10.3390/jcm11133648
Chicago/Turabian StyleKhan, Mohammad Jesan, Naiyer Asif, Mohd Hadi Aziz, Ariz Raza, Shahzad Anwar, Shibili Nuhmani, Ahmad H. Alghadir, and Masood Khan. 2022. "Does an Adjustable-Loop Device Loosen following ACL Reconstruction with a Hamstring Graft? A Retrospective Study with a Follow-Up of Two Years" Journal of Clinical Medicine 11, no. 13: 3648. https://doi.org/10.3390/jcm11133648