
Immediate versus Delayed Attachment Incorporation Impact on Prosthetic Aftercare among Mandibular Implant—Supported Overdenture Wearers

 ,
,  ,
,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
- Heathy individuals or with mild controlled systemic disease.
- Edentulous period of at least 12 months.
- Consecutive patients.
- Addressed the Oral Rehabilitation Department, School of Dentistry, Tel-Aviv University, Israel.
- Reduced stability of mandibular denture.
- Insufficient retention of mandibular denture.
- Classes III–VI resorption of the mandible according to Cawood and Howell [17].
- Presence of keratinized mucosa at the future implantation sites.
- Individuals with severe systemic uncontrolled disease.
- Stable mandibular denture without patient complaint.
- Lack of available data.
- Edentulous period < 12 months.
- Classes I-II resorption of the mandible according to Cawood and Howell [17].
- Absence of keratinized mucosa at the future implantation sites.
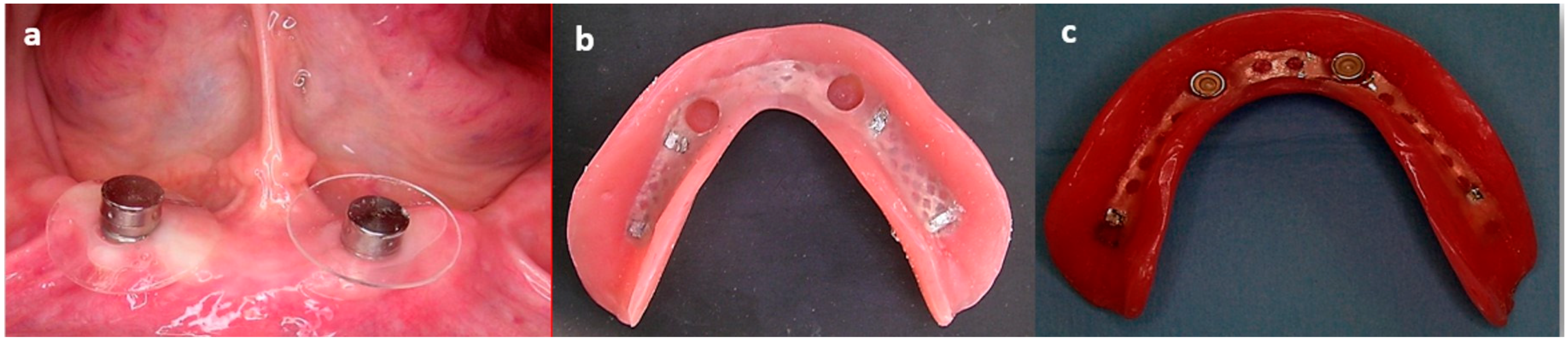
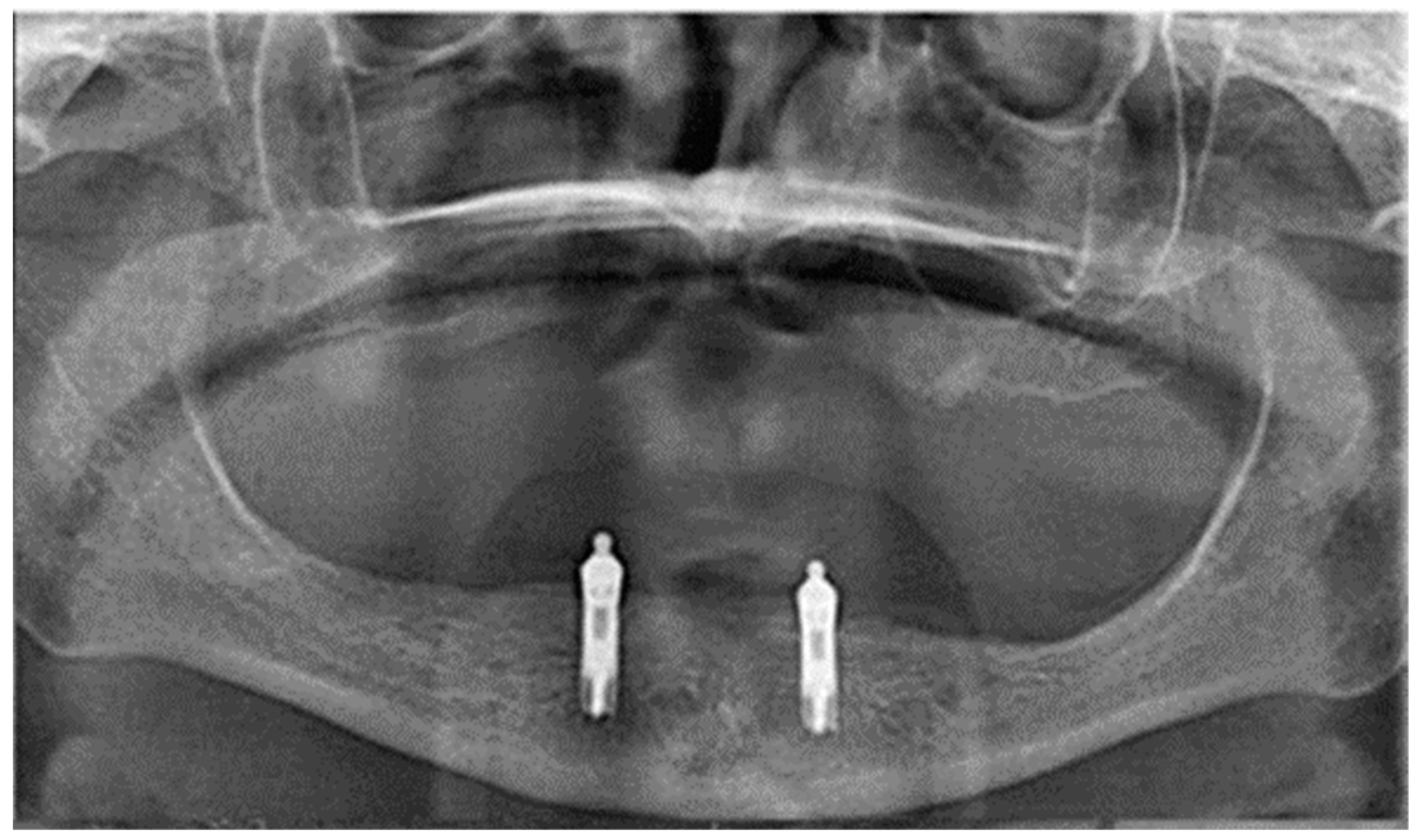
2.2. Surgical Treatment
2.3. Prosthetic Treatment
2.4. Follow-Up
2.5. Data Collection
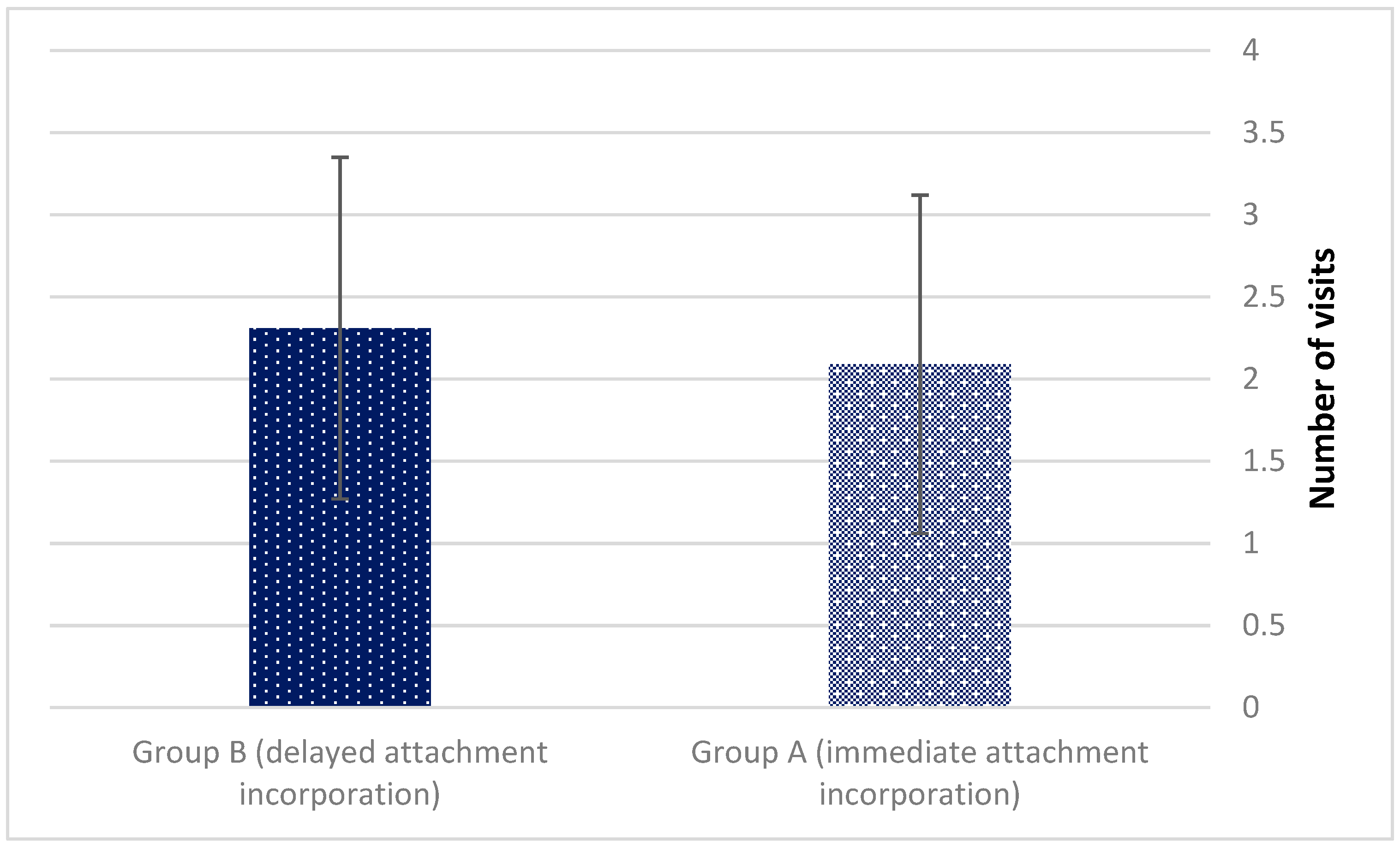
- Number of aftercare visits;
- Prosthetic dental treatment rendered:
- Pressure sores relieve;
- Liner changes due to loss of retention;
- Denture repair and reline.
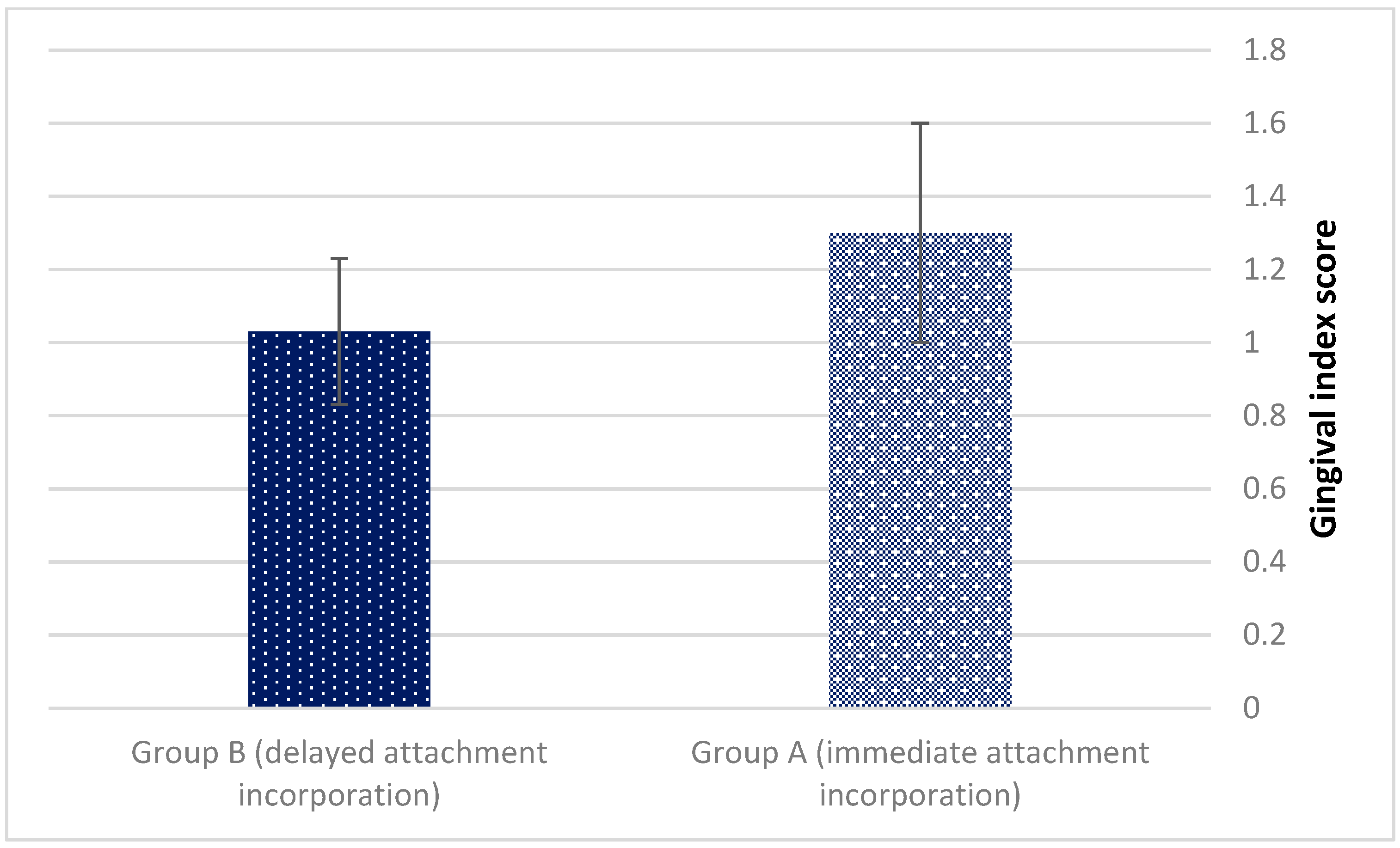
- Gingival index measurements (0–3) according to Loe and Silness [18]. The gingival index was used for the assessment of prevalence and severity of gingivitis. Score 0 = Normal gingiva; Score 1 = Mild inflammation—slight change in color, slight edema, no bleeding on probing; Score 2 = Moderate inflammation—redness, edema, glazing, bleeding on probing; Score 3 = Severe inflammation—marked redness and edema, ulceration, tendency toward spontaneous bleeding.
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tyrovolas, S.; Koyanagi, A.; Panagiotakos, D.B.; Haro, J.M.; Kassebaum, N.J.; Chrepa, V.; Kotsakis, G.A. Population prevalence of edentulism and its association with depression and self-rated health. Sci. Rep. 2016, 6, 37083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Feine, J.S.; Carlsson, G.E.; Awad, M.A.; Chehade, A.; Duncan, W.J.; Gizani, S.; Head, T.; Lund, J.P.; MacEntee, M.; Mericske-Stern, R.; et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology 2002, 19, 3–4. [Google Scholar]
- Assaf, A.; Daas, M.; Boittin, A.; Eid, N.; Postaire, M. Prosthetic maintenance of different mandibular implant overdentures: A systematic review. J. Prosthet. Dent. 2017, 118, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Krennmair, G.; Seemann, R.; Fazekas, A.; Ewers, R.; Piehslinger, E. Patient Preference and Satisfaction with Implant-Supported Mandibular Overdentures Retained with Ball or Locator Attachments: A Crossover Clinical Trial. Int. J. Oral Maxillofac. Implant. 2012, 27, 1560–1568. [Google Scholar]
- Leão, R.S.; Moraes, S.L.D.; Vasconcelos, B.C.E.; Lemos, C.A.A.; Pellizzer, E.P. Splinted and unsplinted overdenture attachment systems: A systematic review and meta-analysis. J. Oral Rehab. 2018, 45, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Nissan, J.; Oz-Ari, B.; Gross, O.; Ghelfan, O.; Chaushu, G. Long-term prosthetic aftercare of direct vs. indirect attachment incorporation techniques to mandibular implant-supported overdenture. Clin. Oral Implant. Res. 2011, 22, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Marinis, A.; Afshari, F.S.; Chia-Chun Yuan, J.; Lee, D.J.; Syros, G.; Knoernschild, K.L.; Campbell, S.D.; Sukotjo, C. Retrospective analysis of implant overdenture treatment in the advanced prosthodontic clinic at the university of Illinois at Chicago. J. Oral Implantol. 2016, 27, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackie, A.; Lyons, K.; Thomson, W.M.; Payne, A.G.T. Mandibular two implant overdentures: Three years prosthodontic maintenance using the locator attachment system. Int. J. Prosthodont. 2011, 21, 328–331. [Google Scholar]
- Matthys, C.; Vervaeke, S.; Besseler, J.; Doornewaard, R.; Dierens, M.; De Bruyn, H. Five year’s follow-up of mandibular 2-implant overdentures on locator or ball abutments: Implant results, patient-related outcome, and prosthetic aftercare. Clin. Implant Dent. Relat. Res. 2019, 21, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Brandt, S.; Lauer, H.-C.; Fehrenz, M.; Güth, J.-F.; Romanos, G.; Winter, A. Ball versus Locator® attachments: A retrospective study on prosthetic maintenance and effect on oral-health- related quality of life. Materials 2021, 14, 1051. [Google Scholar] [CrossRef]
- Cristache, C.M.; Muntianu, L.A.S.; Burlibasa, M.; Didilescu, A.C. Five-year clinical trial using three attachment systems for implant overdentures. Clin. Oral Impl. Res. 2014, 28, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.G.T.; Zarb, G. Prosthodontic Treatment for Edentulous Patients: Complete Dentures and Implant-Supported Prostheses; Elsevier: St Louis, MO, USA, 2013; pp. 330–331. [Google Scholar]
- Brigante, R.F. A cephalometric study of the settling and migration of dentures. J. Prosthet. Dent. 1965, 15, 277–284. [Google Scholar] [CrossRef]
- Utz, K.H. Studies of changes in occlusion after the insertion of complete dentures. Part 1. J. Oral Rehab. 1996, 23, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Boucher, C.O. Discussion of soft tissue displacement beneath removable partial and complete dentures. J. Prosthet. Dent. 1962, 12, 44–46. [Google Scholar] [CrossRef]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar] [CrossRef]
- Loe, H.; Silness, J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, M.; Kulak, Y.; De Baat, C.; Arikan, A.; Ucankale, M. The effect of a new denture adhesive on bite force until denture dislodgement. J. Prosthodont. 2005, 14, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Kimoto, S.; Kimoto, K.; Gunji, A.; Kawai, Y.; Murakami, H.; Tanaka, K.; Syu, K.; Aoki, H.; Tani, M.; Toyoda, M.; et al. Clinical effects of acrylic resilient denture liners applied to mandibular complete dentures on the alveolar ridge. J. Oral Rehab. 2007, 34, 862–869. [Google Scholar] [CrossRef]
- Wolff, A.; Gadre, A.; Begleiter, A.; Moskona, D.; Cardash, H. Correlation between patient satisfaction with complete dentures and denture quality, oral condition, and flow rate of submandibular/sublingual salivary glands. Int. J. Prosthodont. 2003, 16, 45–48. [Google Scholar]
- Isobe, A.; Sato, Y.; Kitagawa, N.; Shimodaira, O.; Hara, S.; Takeuchi, S. The influence of denture supporting tissue properties on pressurepain threshold—measurement in dentate subjects. J. Prosthodont. Res. 2013, 57, 275–283. [Google Scholar] [CrossRef]
- Tanaka, S. A study on creep of oral mucousa. J. Jpn. Prosthodont. Soc. 1973, 14, 358–378. [Google Scholar]
- Nakashima, T. Stress relaxation of palatal mucoperiostium. J. Jpn. Prosthodont. Soc. 1975, 19, 391–410. [Google Scholar] [CrossRef]
- Inoue, K.; Arikawa, H.; Fujii, K.; Shinohara, N.; Kawahata, N. Viscoelastic properties of oral soft tissue: 1. A method of determining elastic modulus of oral soft tissue. Dental Mater. J. 1985, 4, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Józefowicz, W. Results of studies on elasticity moduli of the soft tissues of the denture-bearing area. Protet. Stomatol. 1970, 20, 171–176. [Google Scholar]
- Chun, H.-J.; Park, D.-N.; Han, C.-H.; Heo, S.-J.; Heo, M.-S.; Koak, J.-Y. Stress distributions in maxillary bone surrounding overdenture implants with different overdenture attachments. J. Oral Rehabil. 2005, 32, 193–205. [Google Scholar] [CrossRef]
- Alsabeeha, N.H.M.; Swain, M.V.; Payne, A.G.T. Clinical performance and material properties of single implant overdenture attachment systems. Int. J. Prosthodont. 2011, 24, 247–254. [Google Scholar]
- Preti, G.; Bassi, F.; Barbero, P.; Lorenzetti, M.; Valente, G. Histological changes in edentulous oral mucosa under implant-supported overdentures. J. Oral Rehabil. 1996, 23, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Emami, E.; De Grandmont, P.; Rompré, P.H.; Barbeau, J.; Pan, S.; Feine, J.S. Favoring trauma as an etiological factor in denture stomatitis. J. Dent. Res. 2008, 87, 440–444. [Google Scholar] [CrossRef]
- Sato, H.; Kobayashi, T.; Nomura, T.; Tanabe, N.; Tagafuji, K.; Kihara, H.; Kondo, H. Oral mucosa pressure caused by mandibular implant overdenture with different types of attachments. J. Prosthodont. Res. 2019, 30, 1–7. [Google Scholar] [CrossRef]
- Kawano, F. A study on pressures of supporting tissues under complete denture during functions-concerning the effects of the arrangement of artificial posterior teeth. J. Jpn. Prosthodont. Soc. 1987, 31, 726–739. [Google Scholar] [CrossRef] [Green Version]
- Geckili, O.; Mumcu, E.; Bilhan, H. The effect of maximum bite force, implant number, and attachment type on marginal bone loss around implants supporting mandibular overdentures: A retrospective study. Clin. Implant Dent. Relat. Res. 2012, 14 (Suppl. 1), e91–e97. [Google Scholar] [CrossRef] [PubMed]
- Cehreli, M.C.; Karasoy, D.; Kökat, A.M.; Akça, K.; Ecker, S. A systematic review of marginal bone loss around implants retaining or supporting overdentures. Int. J. Oral Maxillofac. Implant 2010, 25, 266–277. [Google Scholar]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zenziper, E.; Rosner, O.; Ghelfan, O.; Nissan, J.; Blumer, S.; Ben-Izhack, G.; Davidovich, M.; Chaushu, L.; Kahn, A.; Naishlos, S. Immediate versus Delayed Attachment Incorporation Impact on Prosthetic Aftercare among Mandibular Implant—Supported Overdenture Wearers. J. Clin. Med. 2022, 11, 3524. https://doi.org/10.3390/jcm11123524
Zenziper E, Rosner O, Ghelfan O, Nissan J, Blumer S, Ben-Izhack G, Davidovich M, Chaushu L, Kahn A, Naishlos S. Immediate versus Delayed Attachment Incorporation Impact on Prosthetic Aftercare among Mandibular Implant—Supported Overdenture Wearers. Journal of Clinical Medicine. 2022; 11(12):3524. https://doi.org/10.3390/jcm11123524
Chicago/Turabian StyleZenziper, Eran, Ofir Rosner, Oded Ghelfan, Joseph Nissan, Sigalit Blumer, Gil Ben-Izhack, Moshe Davidovich, Liat Chaushu, Adrian Kahn, and Sarit Naishlos. 2022. "Immediate versus Delayed Attachment Incorporation Impact on Prosthetic Aftercare among Mandibular Implant—Supported Overdenture Wearers" Journal of Clinical Medicine 11, no. 12: 3524. https://doi.org/10.3390/jcm11123524