
Age-Adjusted D-Dimer Levels May Improve Diagnostic Assessment for Pulmonary Embolism in COVID-19 Patients

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Laboratory Analysis
2.2. Imaging Studies
2.3. Bova Score Calculation
2.4. Data Storing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gong, X.; Yuan, B.; Yuan, Y. Incidence and prognostic value of pulmonary embolism in COVID-19: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0263580. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, S.; Coppens, M.; Van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1995–2002. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Capitán, C.; Barba, R.; Díaz-Pedroche, M.D.C.; Sigüenza, P.; Demelo-Rodriguez, P.; Siniscalchi, C.; Pedrajas, J.M.; Farfán-Sedano, A.I.; Olivera, P.E.; Gómez-Cuervo, C.; et al. Presenting Characteristics, Treatment Patterns, and Outcomes among Patients with Venous Thromboembolism during Hospitalization for COVID-19. Semin. Thromb. Hemost. 2021, 47, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Stals, M.A.M.; Kaptein, F.; Kroft, L.; Klok, F.; Huisman, M.V. Challenges in the diagnostic approach of suspected pulmonary embolism in COVID-19 patients. Postgrad Med. 2021, 133 (Suppl. S1), 36–41. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar]
- Schulman, S.; Kearon, C. The Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinalproducts in nonsurgical patients. J. Thromb. Haemostasis. 2005, 3, 692–694. [Google Scholar]
- Szymański, P.; Gackowski, A.; Mizia-Stec, K.; Kasprzak, J.D.; Lipczyńska, M.; Lipiec, P. Echocardiography during the coronavirus disease 2019 pandemic—The impact of the vaccination program. A 2021 update of the expert opinion of the Working Group on Echocardiography of the Polish Cardiac Society. Kardiol. Pol. 2021, 79, 595–603. [Google Scholar]
- Bova, C.; Sanchez, O.; Prandoni, P.; Lankeit, M.; Konstantinides, S.; Vanni, S.; Jimenez, D. Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur. Respir. J. 2014, 44, 694–703. [Google Scholar] [CrossRef] [Green Version]
- Pencina, M.J.; D’Agostino, R.B.; Steyerberg, E.W. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat. Med. 2011, 30, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Thachil, J.; Giannis, D.; et al. Subcommittee on Perioperative, Critical Care Thrombosis, Haemostasis of the Scientific, Standardization Committee of the International Society on Thrombosis and Haemostasis. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1859–1865. [Google Scholar] [PubMed]
- Planquette, B.; Khider, L.; Le Berre, A.; Soudet, S.; Pernod, G.; Le Mao, R.; Besutti, M.; Gendron, N.; Yannoutsos, A.; Smadja, D.M.; et al. Adjusting D-dimer to lung disease extent to exclude Pulmonary Embolism in COVID-19 patients (Co-LEAD). Thromb. Haemost. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Cormier, P.; Patel, P.Y.; Hadied, M.O.; Bhargava, P.; Khanna, K.; Nadig, J.; Keimig, T.; Spizarny, D.; Reeser, N.; et al. Acute pulmonary embolism and COVID-19. Radiology 2020, 297, 201955. [Google Scholar] [CrossRef] [PubMed]
- Planquette, B.; Le Berre, A.; Khider, L.; Yannoutsos, A.; Gendron, N.; de Torcy, M.; Mohamedi, N.; Jouveshomme, S.; Smadja, D.M.; Lazareth, I.; et al. Prevalence and characteristics of pulmonary embolism in 1042 COVID-19 patients with respiratory symptoms: A nested case-control study. Thromb. Res. 2021, 197, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Gómez, C.A.; Sun, C.-K.; Tsai, I.-T.; Chang, Y.-P.; Lin, M.-C.; Hung, I.-Y.; Chang, Y.-J.; Wang, L.-K.; Lin, Y.-T.; Hung, K.-C. Mortality and risk factors associated with pulmonary embolism in coronavirus disease 2019 patients: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16025. [Google Scholar] [CrossRef]
- Chocron, R.; Duceau, B.; Gendron, N.; Ezzouhairi, N.; Khider, L.; Trimaille, A.; Goudot, G.; Weizman, O.; Alsac, J.M.; Pommier, T.; et al. D-dimer at hospital admission for COVID-19 are associated with in-hospital mortality, independent of venous thromboembolism: Insights from a French multicenter cohort study. Arch. Cardiovasc. Dis. 2021, 114, 381–393. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Kwee, R.M.; Adams, H.J.A.; Kwee, T.C. Pulmonary embolism in patients with COVID-19 and value of D-dimer assessment: A meta-analysis. Eur. Radiol. 2021, 31, 8168–8186. [Google Scholar] [CrossRef] [PubMed]
- Zuin, M.; Rigatelli, G.; Zuliani, G.; Roncon, L. Age-adjusted D-dimer cutoffs to guide anticoagulation in COVID-19. Lancet 2021, 398, 1303–1304. [Google Scholar] [CrossRef]
- Skowrońska, M.; Furdyna, A.; Ciurzyński, M.; Pacho, S.; Bienias, P.; Palczewski, P.; Kurnicka, K.; Jankowski, K.; Lipińska, A.; Uchacz, K.; et al. D-dimer levels enhance the discriminatory capacity of bleeding risk scores for predicting in-hospital bleeding events in acute pulmonary embolism. Eur. J. Intern. Med. 2019, 69, 8–13. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
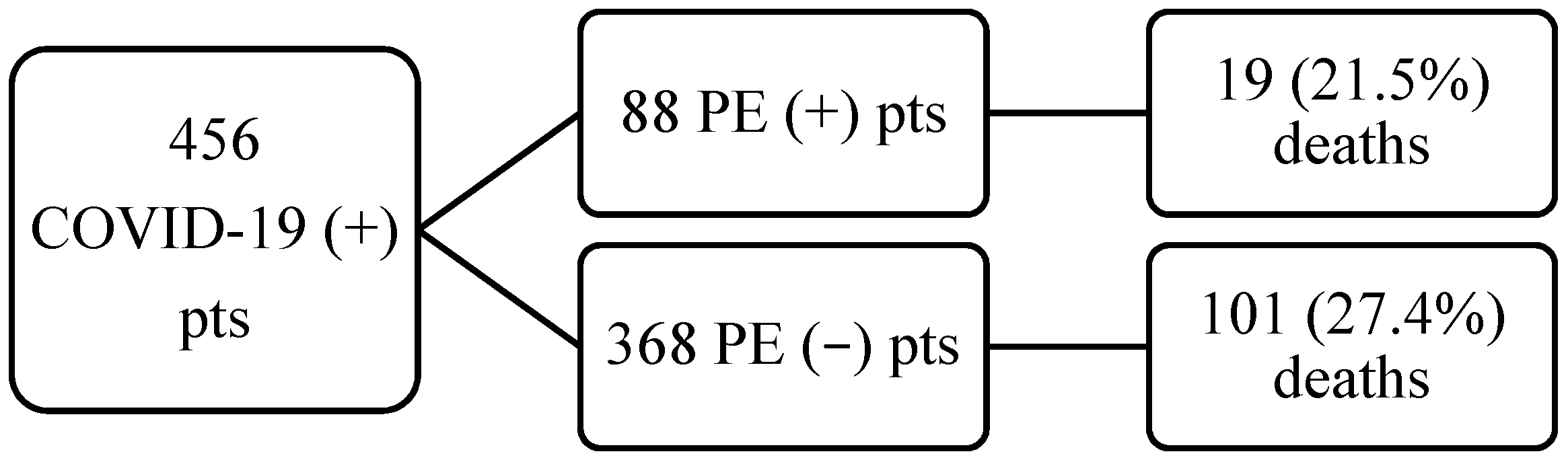
| All N = 456 | PE (−) N = 368 | PE (+) N = 88 | p Value PE (+) vs. PE (−) | |
|---|---|---|---|---|
| Age (years) | 69 (61–78) | 69 (61–77) | 69 (58–78.5) | 0.98 |
| Female (n, %) | 162, 35.5 | 138, 37.5 | 24, 27.3 | 0.7 |
| Length of hospitalization (days) | 10 (5–14.5) | 9 (4–14) | 11 (6–15.5) | 0.01 |
| CT lung involvement (%) | 40 (20–65) | 40 (20–60) | 47.5 (20–60) | 0.87 |
| D-dimer (ng/mL) | 1317 (728–3948) | 1117.5 (625.5–2120) | 6764 (1973–21,548) | <0.001 |
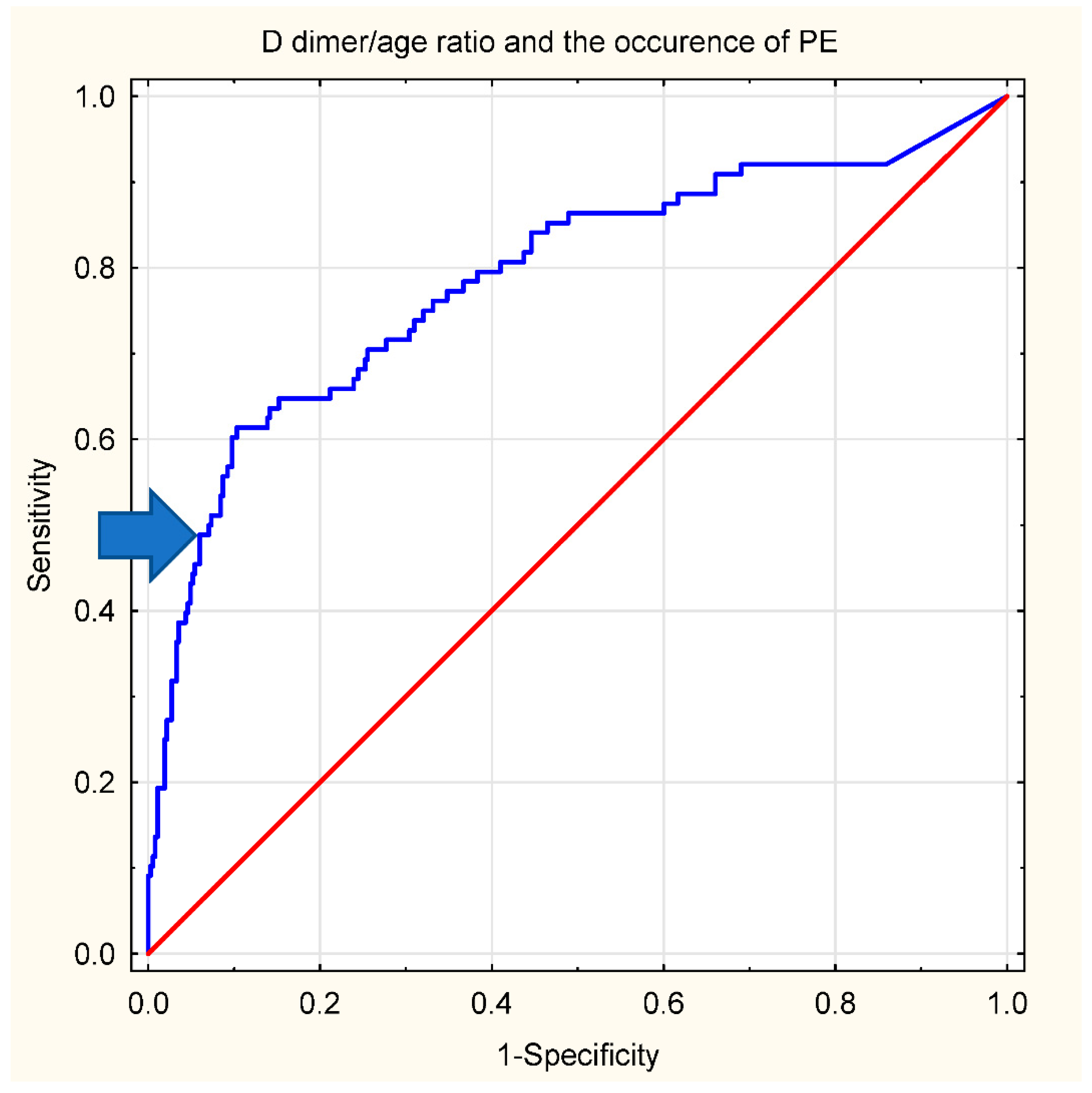
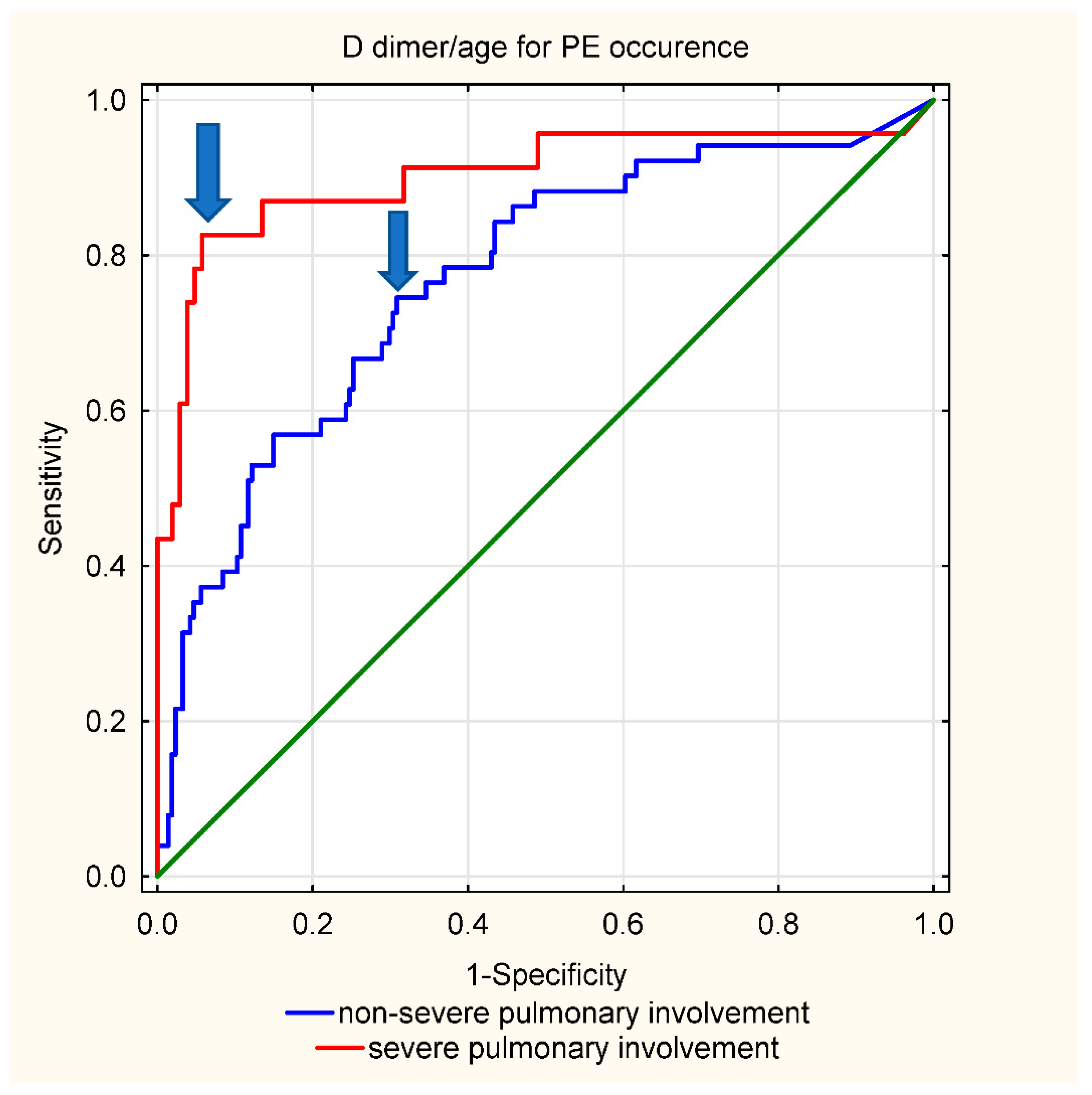
| D-dimer/age ratio | 16.9 (7.8–42.6) | 13.8 (6.8–28.7) | 87 (21.9–303.0) | <0.001 |
| Troponin T (ng/mL) | 0.027 (0.012–0.087) | 0.027 (0.012–0.086) | 0.027 (0.012–0.09) | 0.66 |
| Mortality (n;%) | 120; 26 | 101; 27.4 | 19; 21.5 | 0.26 |
| PE (−) N = 368; Death = 101 vs. Survivors = 267 | PE (+) N = 88, Death = 19 vs. Survivors = 69 | |
|---|---|---|
| Age (years) | 74 (65–82) vs. 67 (58–75), p < 0.001 | 73 (70–81) vs. 66 (55–77), p = 0.006 |
| Male (n, %) | 70 (70%) vs. 160 (60%), p = 0.09 | 14 (73%) vs. 50 (72%), p = 0.9 |
| Length of follow-up for all (days) | 6 (2–10) vs. 10 (5–15), p < 0.001 | 9 (5–12) vs. 12 (7–16), p = 0.06 |
| CT lung involvement (%) | 50 (40–75) vs. 40 (20–60), p < 0.001 | 30 (20–75) vs. 50 (30–60), p = 0.62 |
| D-dimer (ng/mL) | 2014 (906–4549) vs. 959 (553–1594), p < 0.001 | 7497 (2326–30,484) vs. 6443 (1921–17,726), p = 0.28 |
| Troponin T (ng/mL) | 0.056 (0.024–0.201) vs. 0.02 (0.009–0.059), p < 0.001 | 0.040 (0.026–0.240) vs. 0.024 (0.012–0.08), p = 0.03 |
| Mortality (n;%) | 101; 27.4 | 19; 21.5 |
| Bova points | NA | 2 (2–3) vs. 2 (1–2), p = 0.04 |
| Predictor | PE (+) Patients OR; p-Value | PE (−) Patients OR; p-Value |
|---|---|---|
| Age (years) | 1.06 (1.00–1.11); 0.04 | 1.07 (1.03–1.08); <0.001 |
| CT lung involvement (%) | 0.99 (0.97–1.02); 0.51 | 1.04 (1.02–1.05); <0.001 |
| D-dimer (ng/mL) | 1.000 (1.000–1.000); 0.2 | 1.002 (1.0001–1.003); 0.002 |
| Troponin T (ng/mL) | 1.06 (0.26–4.30); 0.93 | 1.6 (0.77–3.6); 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machowski, M.; Polańska, A.; Gałecka-Nowak, M.; Mamzer, A.; Skowrońska, M.; Perzanowska-Brzeszkiewicz, K.; Zając, B.; Ou-Pokrzewińska, A.; Pruszczyk, P.; Kasprzak, J.D. Age-Adjusted D-Dimer Levels May Improve Diagnostic Assessment for Pulmonary Embolism in COVID-19 Patients. J. Clin. Med. 2022, 11, 3298. https://doi.org/10.3390/jcm11123298
Machowski M, Polańska A, Gałecka-Nowak M, Mamzer A, Skowrońska M, Perzanowska-Brzeszkiewicz K, Zając B, Ou-Pokrzewińska A, Pruszczyk P, Kasprzak JD. Age-Adjusted D-Dimer Levels May Improve Diagnostic Assessment for Pulmonary Embolism in COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(12):3298. https://doi.org/10.3390/jcm11123298
Chicago/Turabian StyleMachowski, Michał, Anna Polańska, Magdalena Gałecka-Nowak, Aleksandra Mamzer, Marta Skowrońska, Katarzyna Perzanowska-Brzeszkiewicz, Barbara Zając, Aisha Ou-Pokrzewińska, Piotr Pruszczyk, and Jarosław D. Kasprzak. 2022. "Age-Adjusted D-Dimer Levels May Improve Diagnostic Assessment for Pulmonary Embolism in COVID-19 Patients" Journal of Clinical Medicine 11, no. 12: 3298. https://doi.org/10.3390/jcm11123298