
Association between Low Ankle-Brachial Index and Poor Outcomes in Patients with Embolic Stroke of Undetermined Source

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
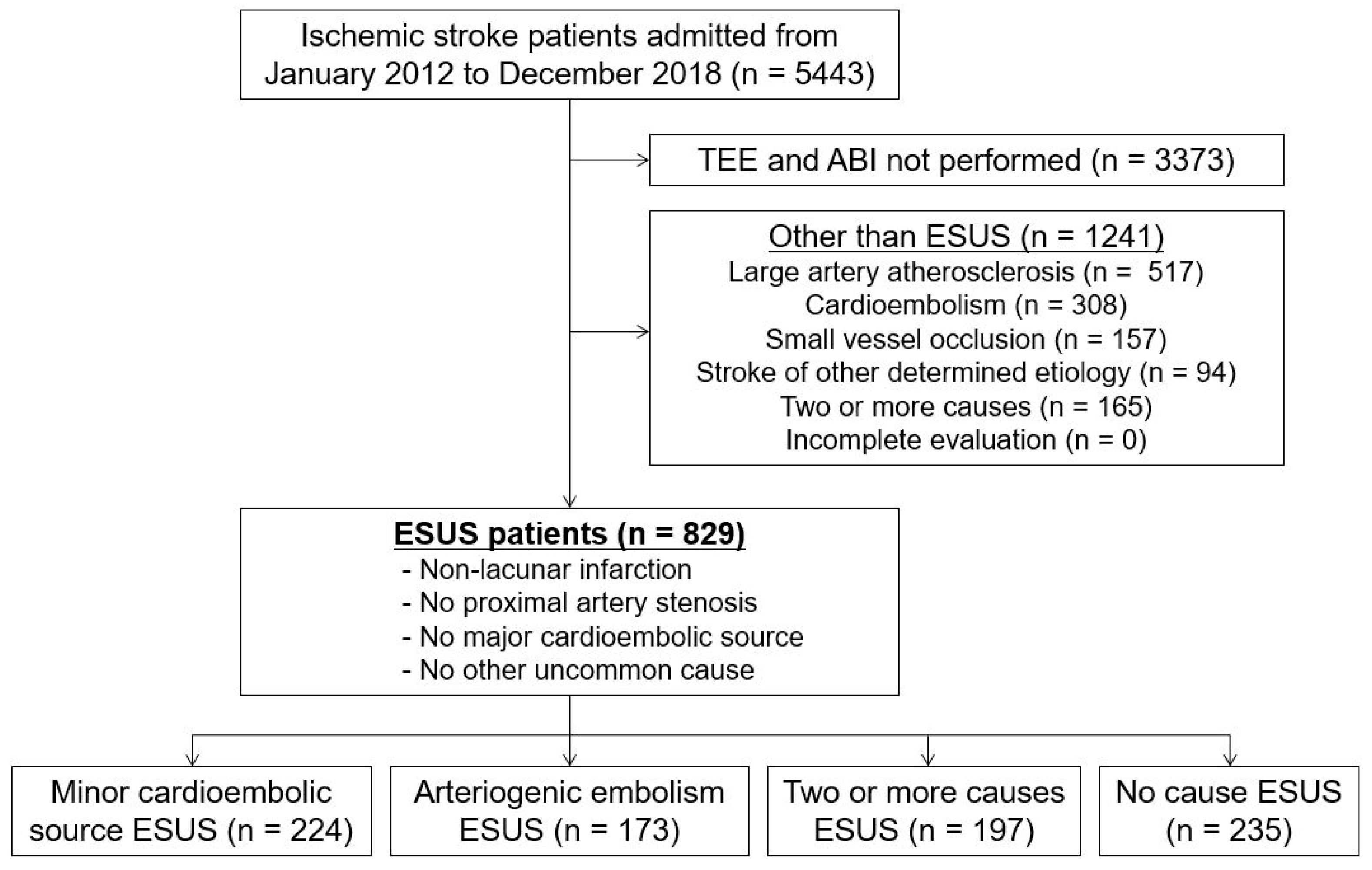
2.1. Study Population
2.2. Clinical Variables
2.3. ABI Measurement
2.4. Follow-Up and Outcomes
2.5. Statistical Analysis
2.6. Standard Protocol Approvals, Registrations and Patient Consent
2.7. Data Availability
3. Results
3.1. Demographic Characteristics
3.2. Relation of ABI with Long-Term Outcomes
3.3. Association between ABI and Outcomes by Arteriogenic Embolism Type
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hart, R.G.; Diener, H.C.; Coutts, S.B.; Easton, J.D.; Granger, C.B.; O’Donnell, M.J.; Sacco, R.L.; Connolly, S.J. Embolic strokes of undetermined source: The case for a new clinical construct. Lancet Neurol. 2014, 13, 429–438. [Google Scholar] [CrossRef]
- Hart, R.G.; Catanese, L.; Perera, K.S.; Ntaios, G.; Connolly, S.J. Embolic stroke of undetermined source: A systematic review and clinical update. Stroke 2017, 48, 867–872. [Google Scholar] [CrossRef]
- Diener, H.C.; Sacco, R.L.; Easton, J.D.; Granger, C.B.; Bernstein, R.A.; Uchiyama, S.; Kreuzer, J.; Cronin, L.; Cotton, D.; Grauer, C.; et al. Dabigatran for prevention of stroke after embolic stroke of undetermined source. N. Engl. J. Med. 2019, 38, 1906–1917. [Google Scholar] [CrossRef]
- Hart, R.G.; Sharma, M.; Mundl, H.; Kasner, S.E.; Bangdiwala, S.I.; Berkowitz, S.D.; Swaminathan, B.; Lavados, P.; Wang, Y.; Wang, Y.; et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N. Engl. J. Med. 2018, 378, 2191–2201. [Google Scholar] [CrossRef]
- Ntaios, G.; Pearce, L.A.; Veltkamp, R.; Sharma, M.; Kasner, S.E.; Korompoki, E.; Milionis, H.; Mundl, H.; Berkowitz, S.D.; Connolly, S.J.; et al. Potential embolic sources and outcomes in embolic stroke of undetermined source in the navigate-esus trial. Stroke 2020, 51, 1797–1804. [Google Scholar] [CrossRef]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.; Hamburg, N.M.; Kinlay, S.; et al. 2016 aha/acc guideline on the management of patients with lower extremity peripheral artery disease: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation 2017, 135, e726–e779. [Google Scholar]
- Fowkes, F.G.; Murray, G.D.; Butcher, I.; Heald, C.L.; Lee, R.J.; Chambless, L.E.; Folsom, A.R.; Hirsch, A.T.; Dramaix, M.; deBacker, G.; et al. Ankle brachial index combined with framingham risk score to predict cardiovascular events and mortality: A meta-analysis. JAMA 2008, 300, 197–208. [Google Scholar]
- Lee, D.H.; Kim, J.; Lee, H.S.; Cha, M.J.; Kim, Y.D.; Nam, H.S.; Nam, C.M.; Heo, J.H. Low ankle-brachial index is a predictive factor for initial severity of acute ischaemic stroke. Eur. J. Neurol. 2012, 19, 892–898. [Google Scholar] [CrossRef]
- Hong, J.B.; Leonards, C.O.; Endres, M.; Siegerink, B.; Liman, T.G. Ankle-brachial index and recurrent stroke risk: Meta-analysis. Stroke 2016, 47, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Abboud, H.; Monteiro Tavares, L.; Labreuche, J.; Arauz, A.; Bryer, A.; Lavados, P.M.; Massaro, A.; Munoz Collazos, M.; Steg, P.G.; Yamout, B.I.; et al. Impact of low ankle-brachial index on the risk of recurrent vascular events. Stroke 2019, 50, 853–858. [Google Scholar] [CrossRef]
- Han, M.; Baik, M.; Kim, Y.D.; Choi, J.; Seo, K.; Park, E.; Heo, J.H.; Nam, H.S. Low ankle-brachial index is associated with stroke recurrence in ischemic stroke patients with atrial fibrillation. Front. Neurol. 2021, 12, 705904. [Google Scholar] [CrossRef]
- Amarenco, P.; Cohen, A.; Tzourio, C.; Bertrand, B.; Hommel, M.; Besson, G.; Chauvel, C.; Touboul, P.J.; Bousser, M.G. Atherosclerotic disease of the aortic arch and the risk of ischemic stroke. N. Engl. J. Med. 1994, 331, 1474–1479. [Google Scholar] [CrossRef]
- Tao, L.; Li, X.Q.; Hou, X.W.; Yang, B.Q.; Xia, C.; Ntaios, G.; Chen, H.S. Intracranial atherosclerotic plaque as a potential cause of embolic stroke of undetermined source. J. Am. Coll. Cardiol. 2021, 77, 680–691. [Google Scholar] [CrossRef]
- Song, T.J.; Kim, Y.D.; Yoo, J.; Kim, J.; Chang, H.J.; Hong, G.R.; Shim, C.Y.; Song, D.; Heo, J.H.; Nam, H.S. Association between aortic atheroma and cerebral small vessel disease in patients with ischemic stroke. J. Stroke 2016, 18, 312–320. [Google Scholar] [CrossRef]
- Nam, H.S.; Kim, H.C.; Kim, Y.D.; Lee, H.S.; Kim, J.; Lee, D.H.; Heo, J.H. Long-term mortality in patients with stroke of undetermined etiology. Stroke 2012, 43, 2948–2956. [Google Scholar] [CrossRef] [Green Version]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. Toast. Trial of org 10172 in acute stroke treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Perera, K.S.; Vanassche, T.; Bosch, J.; Giruparajah, M.; Swaminathan, B.; Mattina, K.R.; Berkowitz, S.D.; Arauz, A.; O’Donnell, M.J.; Ameriso, S.F.; et al. Embolic strokes of undetermined source: Prevalence and patient features in the esus global registry. Int. J. Stroke 2016, 11, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Ntaios, G. Embolic stroke of undetermined source: Jacc review topic of the week. J. Am. Coll. Cardiol. 2020, 75, 333–340. [Google Scholar] [CrossRef]
- Ntaios, G.; Perlepe, K.; Lambrou, D.; Sirimarco, G.; Strambo, D.; Eskandari, A.; Karagkiozi, E.; Vemmou, A.; Koroboki, E.; Manios, E.; et al. Prevalence and overlap of potential embolic sources in patients with embolic stroke of undetermined source. J. Am. Heart Assoc. 2019, 8, e012858. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Lee, D.H.; Cha, M.J.; Song, T.J.; Park, J.H.; Lee, H.S.; Nam, C.M.; Nam, H.S.; Kim, Y.D.; Heo, J.H. Low ankle-brachial index is an independent predictor of poor functional outcome in acute cerebral infarction. Atherosclerosis 2012, 224, 113–117. [Google Scholar] [CrossRef]
- Ratanakorn, D.; Keandoungchun, J.; Tegeler, C.H. Coexistent extra- and intracranial stenosis, cervical atherosclerosis, and abnormal ankle brachial index in acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2012, 21, 782–789. [Google Scholar] [CrossRef]
- Nam, H.S.; Han, S.W.; Lee, J.Y.; Ahn, S.H.; Ha, J.W.; Rim, S.J.; Lee, B.I.; Heo, J.H. Association of aortic plaque with intracranial atherosclerosis in patients with stroke. Neurology 2006, 67, 1184–1188. [Google Scholar] [CrossRef]
- Fazio, G.P.; Redberg, R.F.; Winslow, T.; Schiller, N.B. Transesophageal echocardiographically detected atherosclerotic aortic plaque is a marker for coronary artery disease. J. Am. Coll. Cardiol. 1993, 21, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Ntaios, G.; Lip, G.Y.H.; Vemmos, K.; Koroboki, E.; Manios, E.; Vemmou, A.; Rodríguez Campello, A.; Cuadrado Godia, E.; Roquer, J.; Arnao, V.; et al. Age- and sex-specific analysis of patients with embolic stroke of undetermined source. Neurology 2017, 89, 532–539. [Google Scholar] [CrossRef]
- Saver, J.L. Clinical practice. Cryptogenic stroke. N. Engl. J. Med. 2016, 374, 2065–2074. [Google Scholar] [CrossRef]
- Sacco, R.L. Risk factors, outcomes, and stroke subtypes for ischemic stroke. Neurology 1997, 49, S39–S44. [Google Scholar] [CrossRef]
- Ntaios, G.; Pearce, L.A.; Meseguer, E.; Endres, M.; Amarenco, P.; Ozturk, S.; Lang, W.; Bornstein, N.M.; Molina, C.A.; Pagola, J.; et al. Aortic arch atherosclerosis in patients with embolic stroke of undetermined source: An exploratory analysis of the navigate esus trial. Stroke 2019, 50, 3184–3190. [Google Scholar] [CrossRef]
- Ntaios, G.; Swaminathan, B.; Berkowitz, S.D.; Gagliardi, R.J.; Lang, W.; Siegler, J.E.; Lavados, P.; Mundl, H.; Bornstein, N.; Meseguer, E.; et al. Efficacy and safety of rivaroxaban versus aspirin in embolic stroke of undetermined source and carotid atherosclerosis. Stroke 2019, 50, 2477–2485. [Google Scholar] [CrossRef]
- Viedma-Guiard, E.; Guidoux, C.; Amarenco, P.; Meseguer, E. Aortic sources of embolism. Front. Neurol. 2020, 11, 606663. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline from the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Bhole, R.; Frogoudaki, A.; Giannopoulos, S.; Goyal, N.; Vrettou, A.R.; Ikonomidis, I.; Paraskevaidis, I.; Pappas, K.; Parissis, J.; et al. The value of transesophageal echocardiography for embolic strokes of undetermined source. Neurology 2016, 87, 988–995. [Google Scholar] [CrossRef] [Green Version]
- Thomalla, G.; Upneja, M.; Camen, S.; Jensen, M.; Schröder, J.; Barow, E.; Boskamp, S.; Ostermeier, B.; Kissling, S.; Leinisch, E.; et al. Treatment-relevant findings in transesophageal echocardiography after stroke: A prospective multicenter cohort study. Stroke 2022, 53, 177–184. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Spring, M.; Dorian, P.; Panzov, V.; Thorpe, K.E.; Hall, J.; Vaid, H.; O’Donnell, M.; Laupacis, A.; Côté, R.; et al. Atrial fibrillation in patients with cryptogenic stroke. N. Engl. J. Med. 2014, 370, 2467–2477. [Google Scholar] [CrossRef] [Green Version]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the subcommittee of professional and public education of the american heart association council on high blood pressure research. Circulation 2005, 111, 697–716. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 829) | ABI < 0.9 (n = 42) | ABI ≥ 0.9 (n = 787) | p Value | |
|---|---|---|---|---|
| Age, y | 63.3 ± 13.1 | 67.7 ± 13.0 | 63.0 ± 13.1 | 0.024 |
| Men | 517 (62.4) | 37 (88.1) | 480 (61.0) | <0.001 |
| NIHSS score at admission | 2.0 [1.0, 4.0] | 2.0 [0.0, 4.0] | 2.0 [1.0, 4.0] | 0.705 |
| Arteriogenic embolism | 370 (44.6) | 30 (71.4) | 340 (43.2) | <0.001 |
| CAP | 146 (17.6) | 18 (42.9) | 128 (16.3) | <0.001 |
| NAP | 224 (27.0) | 12 (28.6) | 212 (26.9) | 0.816 |
| Risk factors | ||||
| Hypertension | 605 (73.0) | 31 (73.8) | 574 (72.9) | 0.901 |
| Diabetes mellitus | 237 (28.6) | 21 (50.0) | 216 (27.4) | 0.002 |
| Hypercholesterolemia | 151 (18.2) | 9 (21.4) | 142 (18.0) | 0.580 |
| Current smoking | 207 (25.0) | 15 (35.7) | 192 (24.4) | 0.099 |
| Coronary artery disease | 287 (34.6) | 18 (42.9) | 269 (34.2) | 0.236 |
| Previous TIA/infarction | 119 (14.4) | 5 (11.9) | 114 (14.5) | 0.642 |
| Laboratory findings | ||||
| Total cholesterol, mmol/L (mg/dL) | 4.6 ± 2.1 (179.1 ± 80.5) | 4.5 ± 1.3 (173.2 ± 49.4) | 4.6 ± 2.1 (179.3 ± 81.7) | 0.629 |
| LDL-cholesterol, mmol/L (mg/dL) | 2.7 ± 1.0 (105.8 ± 37.4) | 2.8 ± 1.1 (109.4 ± 42.4) | 2.7 ± 1.0 (105.6 ± 37.2) | 0.518 |
| HDL-cholesterol, mmol/L (mg/dL) | 1.1 ± 0.3 (43.5 ± 12.8) | 1.0 ± 0.3 (38.4 ± 9.8) | 1.1 ± 0.3 (43.8 ± 13.0) | 0.008 |
| Triglyceride, mmol/L (mg/dL) | 1.4 ± 1.1 (126.3 ± 92.6) | 1.5 ± 0.8 (131.4 ± 70.3) | 1.4 ± 1.1 (125.8 ± 93.6) | 0.703 |
| ABI measurements | ||||
| Heart rate, bpm | 68.7 ± 11.6 | 67.9 ± 10.8 | 68.8 ± 11.7 | 0.626 |
| Brachial SBP, mmHg | 145.9 ± 21.8 | 148.7 ± 20.2 | 145.8 ± 21.9 | 0.400 |
| Brachial DBP, mmHg | 83.4 ± 13.2 | 79.4 ± 13.3 | 83.6 ± 13.2 | 0.040 |
| Ankle SBP, mmHg | 167.0 ± 27.8 | 135.0 ± 29.7 | 168.7 ± 26.7 | <0.001 |
| Ankle DBP, mmHg | 81.9 ± 14.3 | 70.0 ± 13.8 | 82.5 ± 14.0 | <0.001 |
| ABI | 1.09 ± 0.12 | 0.77 ± 0.12 | 1.11 ± 0.09 | <0.001 |
| MACE * | All-Cause Mortality * | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| All patients (n = 829) | ||||
| ABI | 0.146 (0.036–0.592) | 0.007 | 0.037 (0.005–0.285) | 0.002 |
| ABI < 0.9 | 2.038 (1.093–3.801) | 0.025 | 3.608 (1.538–8.465) | 0.003 |
| With arteriogenic embolism (n = 370) | ||||
| ABI | 0.099 (0.019–0.520) | 0.006 | 0.007 (0.001–0.066) | <0.001 |
| ABI < 0.9 | 2.513 (1.257–5.023) | 0.009 | 5.681 (2.151–15.008) | <0.001 |
| Without arteriogenic embolism (n = 459) | ||||
| ABI | 0.423 (0.028–6.376) | 0.535 | 54.379 (0.310–9543.781) | 0.130 |
| ABI < 0.9 | 0.841 (0.111–6.383) | 0.867 | 0.000 (0.000–NA) | 0.984 |
| MACE * | All-Cause Mortality * | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| CAP (n = 146) | ||||
| ABI | 0.043 (0.003–0.587) | 0.018 | 0.002 (0.000–0.110) | 0.002 |
| ABI < 0.9 | 2.977 (1.164–7.611) | 0.023 | 4.812 (1.391–16.647) | 0.013 |
| NAP (n = 224) | ||||
| ABI | 0.162 (0.011–2.502) | 0.193 | 0.016 (0.000–0.581) | 0.024 |
| ABI < 0.9 | 2.223 (0.630–7.844) | 0.214 | 12.014 (1.613–89.459) | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, M.; Heo, J.; Jung, J.W.; Lee, I.H.; Kim, J.H.; Lee, H.; Kim, Y.D.; Nam, H.S. Association between Low Ankle-Brachial Index and Poor Outcomes in Patients with Embolic Stroke of Undetermined Source. J. Clin. Med. 2022, 11, 3073. https://doi.org/10.3390/jcm11113073
Han M, Heo J, Jung JW, Lee IH, Kim JH, Lee H, Kim YD, Nam HS. Association between Low Ankle-Brachial Index and Poor Outcomes in Patients with Embolic Stroke of Undetermined Source. Journal of Clinical Medicine. 2022; 11(11):3073. https://doi.org/10.3390/jcm11113073
Chicago/Turabian StyleHan, Minho, JoonNyung Heo, Jae Wook Jung, Il Hyung Lee, Joon Ho Kim, Hyungwoo Lee, Young Dae Kim, and Hyo Suk Nam. 2022. "Association between Low Ankle-Brachial Index and Poor Outcomes in Patients with Embolic Stroke of Undetermined Source" Journal of Clinical Medicine 11, no. 11: 3073. https://doi.org/10.3390/jcm11113073