
Endovascular Treatment of Chronic Subdural Hematomas through Embolization: A Pilot Study with a Non-Adhesive Liquid Embolic Agent of Minimal Viscosity (Squid)

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Adherence to Ethical Standards
2.2. Inclusion and Exclusion Criteria
- -
- Patient with CSDH, confirmed by non-contrast computed tomography (NCCT) or MRI.
- -
- Patient being asymptomatic or symptomatic, without clinical signs of acutely increased ICP.
- -
- Patient without previous surgical treatment or.
- -
- Patient with recurrence after previous surgical treatment; no defined time interval between surgery and embolization was applied; a minimum depth of 10 mm was considered necessary to justify embolization.
- -
- Patient able to understand the purpose of the study.
- -
- Patient able to tolerate the endovascular procedure.
- -
- Patient > 18 years old.
- -
- Patient is not pregnant.
- -
- Patient with symptomatic CSDH, confirmed by NCCT or MRI, with clinical signs of acutely increased ICP (e.g., impaired consciousness, vomiting without nausea, papilledema).
- -
- Patient not able to understand the purpose of the study.
- -
- Patient not able to tolerate the endovascular procedure (e.g., severe allergy against contrast medium, severe renal insufficiency).
- -
- Patient < 18 years old.
- -
- Patient is pregnant.
- -
- Visible anastomosis between the MMA and the ophthalmic artery.
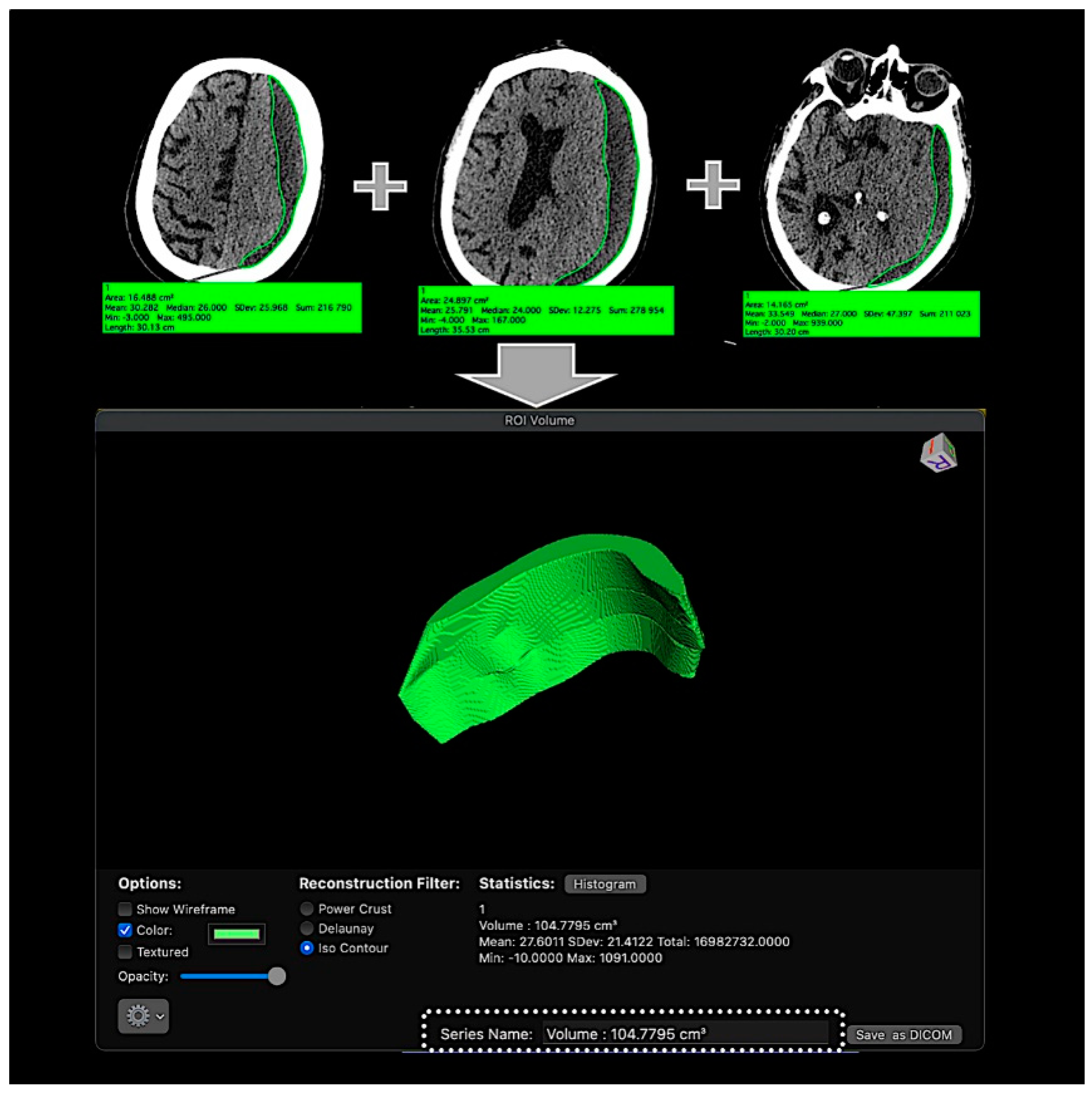
2.3. CSDH Volume Measurement
2.4. Endovascular Treatment Strategy and Technique
- -
- Direct embolization of the distal MMA branches in a single session.
- -
- Avoidance of reflux into proximal segments of the MMA in order to avoid the dissemination of Squid through dangerous anastomoses.
- -
- Termination of blood supply to the vessels of the CSDH capsule through occlusion of the meningeal arteries and of the vessels of the capsule of the CSDH by non-adhesive embolizing material of low viscosity in order to prevent recurrence and increase the hematoma volume.
- -
- Penetration of the non-adhesive embolizing agent through collaterals to distal branches of the opposite MMA, preventing blood supply of the CSDH capsule from the opposite side.
- -
- Acceleration of the processes of hematoma absorption and decompression of the adjacent brain.
- -
- Far distal catheterization of the frontal and parietal branch of the middle meningeal artery, almost to the level where the outer diameter of the microcatheter coincides with the inner lumen of the artery.
- -
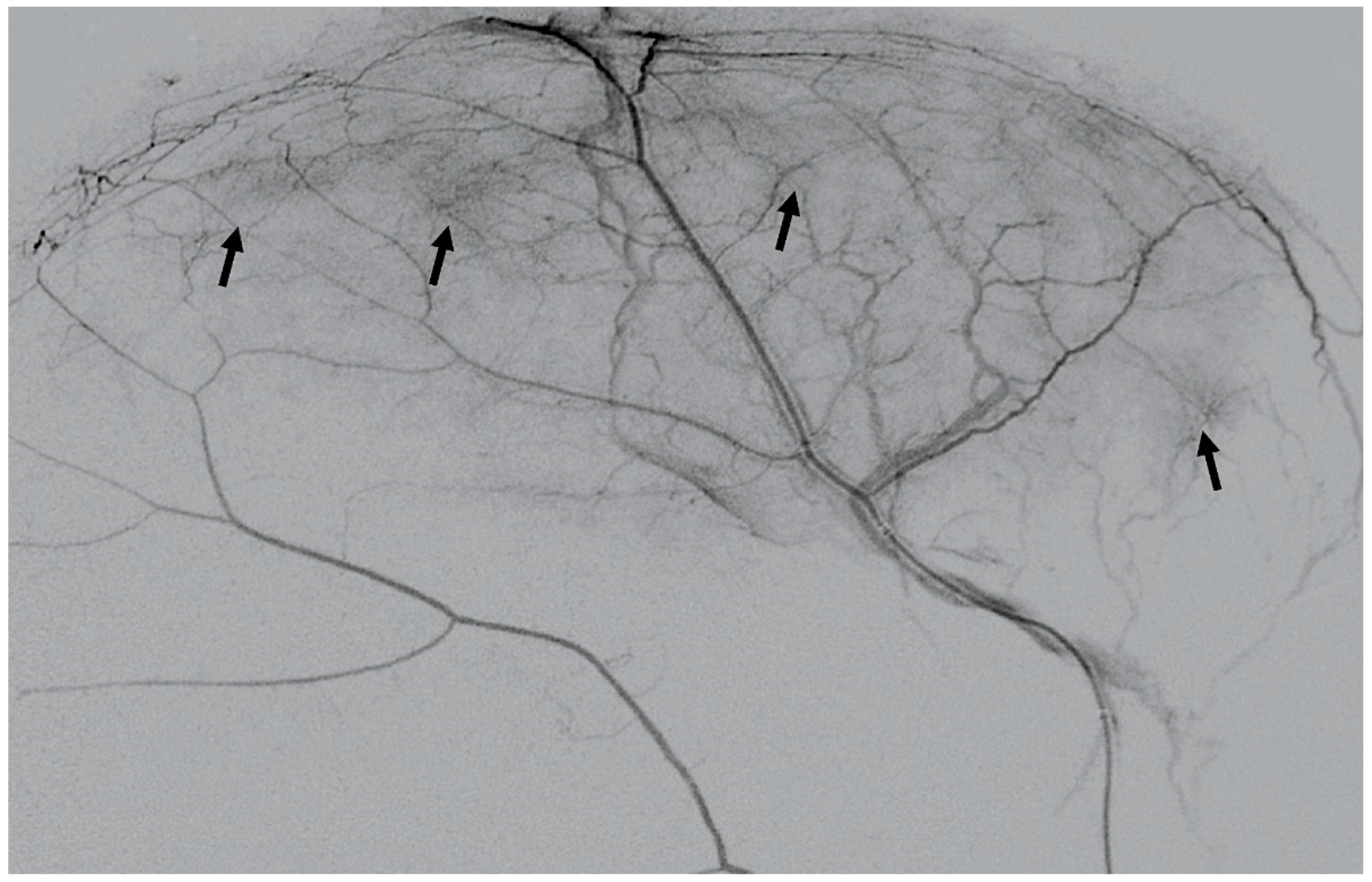
- DSA with contrast medium injection via the microcatheter in the MMA, demonstrating the “cotton wool” areas of neovascularization.
- -
- From this wedged position, the first portion of Squid 12 is injected to obliterate all MMA branches distal to the catheter tip, including the CSDH capsule’s angioneogenic vessels.
2.5. Follow-Up Examinations
2.6. Study Endpoints
2.6.1. Primary Endpoint (Safety Endpoint)
2.6.2. Secondary Endpoint (Efficacy Endpoint)
3. Results
3.1. Patient Population
- -
- A 70-year-old patient with left-handed CSDH and a midline shift of 12 mm, motor aphasia, and right-hand hemiparesis.
- -
- A 42-year-old patient with bilateral CSDH that progressively increased during 1.5 months from 54 mL to 69 mL on the right-hand side and from 68 mL to 83 mL on the left-hand side, causing significant compression of both hemispheres and neurological deterioration.
- -
- An 89-year-old patient with bilateral CSDH (no midline shift). There was no apparent connection with an antecedent head injury. However, the patient’s relatives reported that the patient did periodically fall. At the time of admission, the patient presented tetraparesis and a decreased level of consciousness.
3.2. CSDH Volumes
3.3. Follow-Up Examinations
3.3.1. Safety Endpoints
3.3.2. Efficacy Endpoint
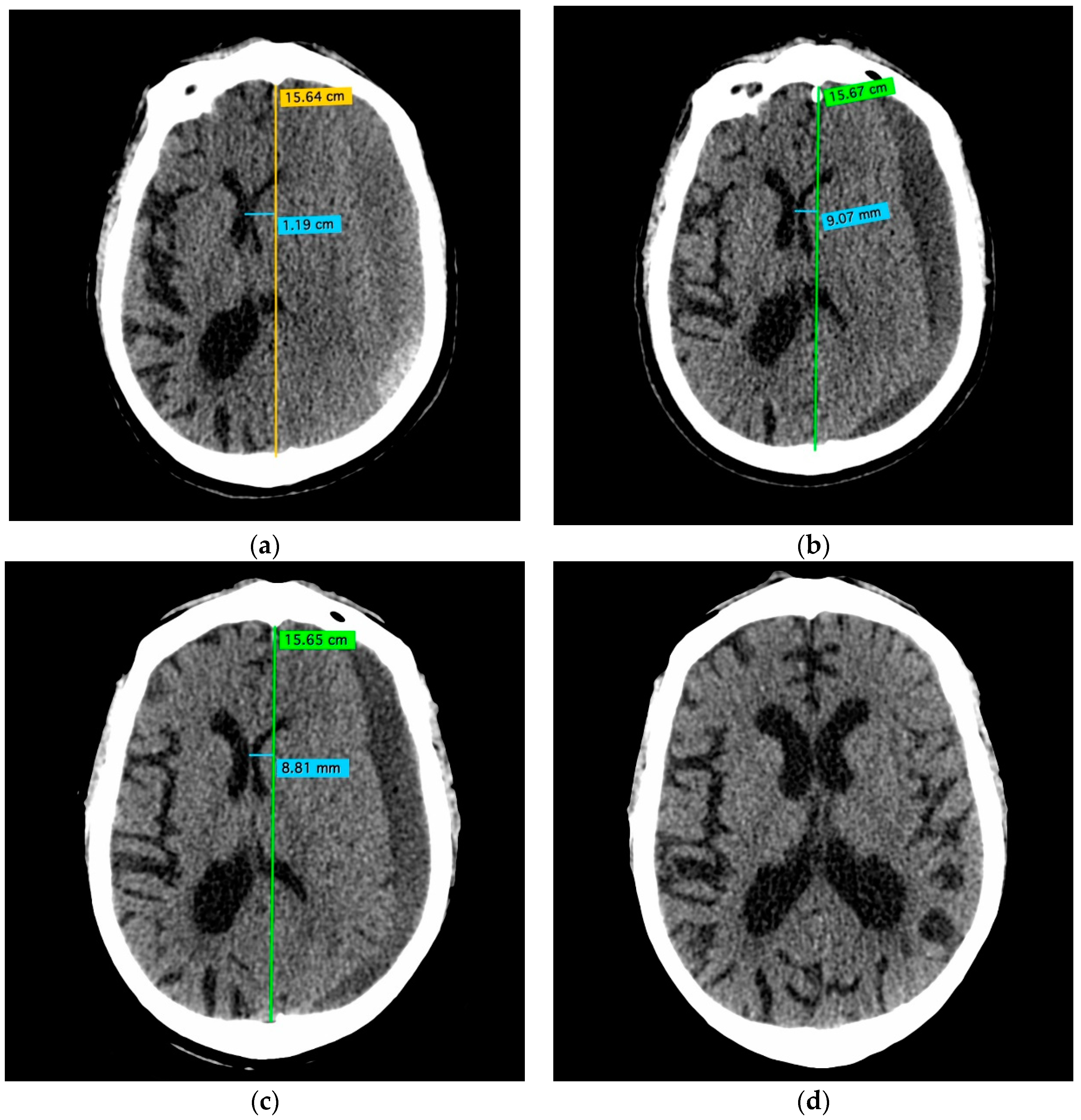
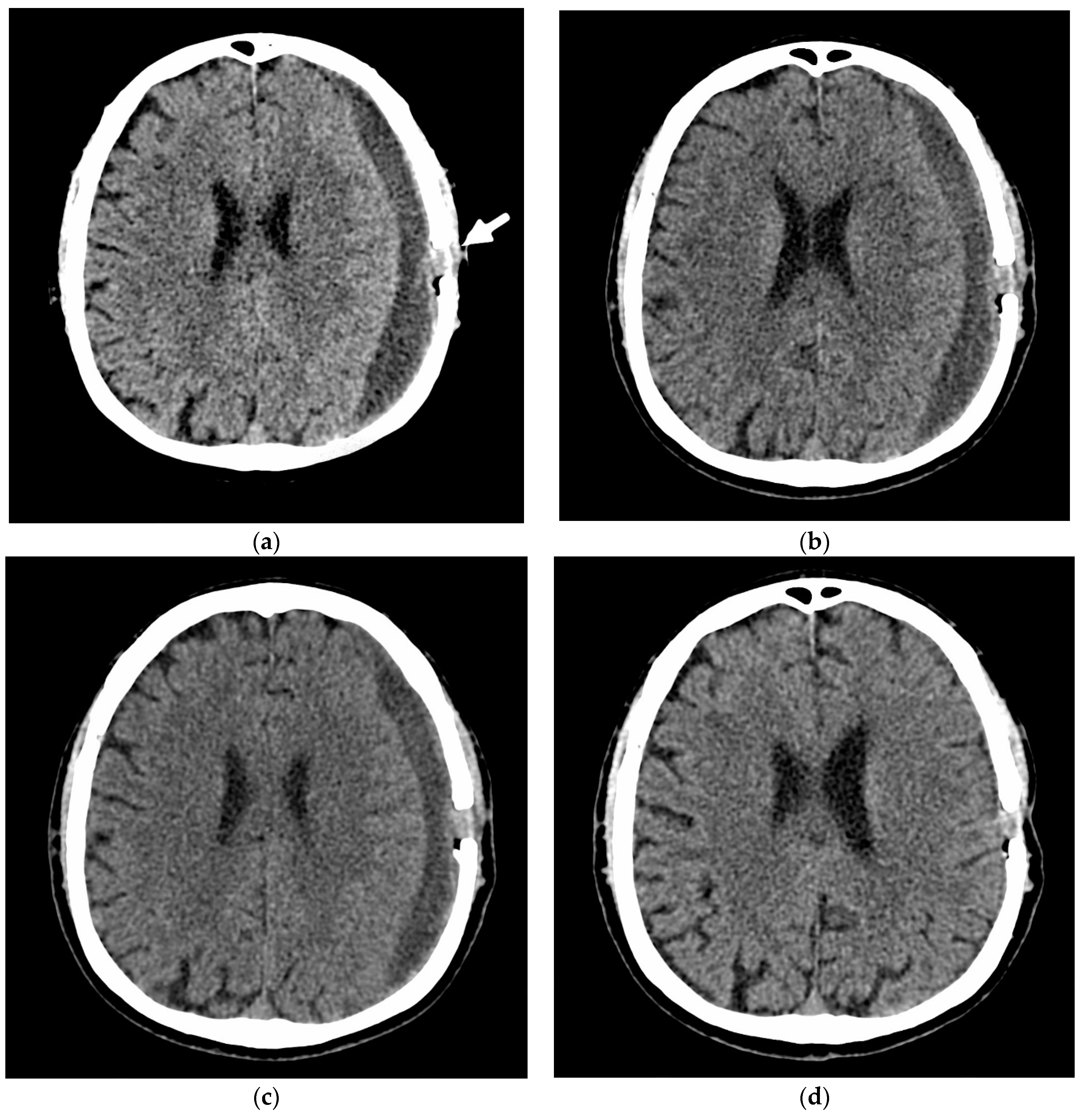
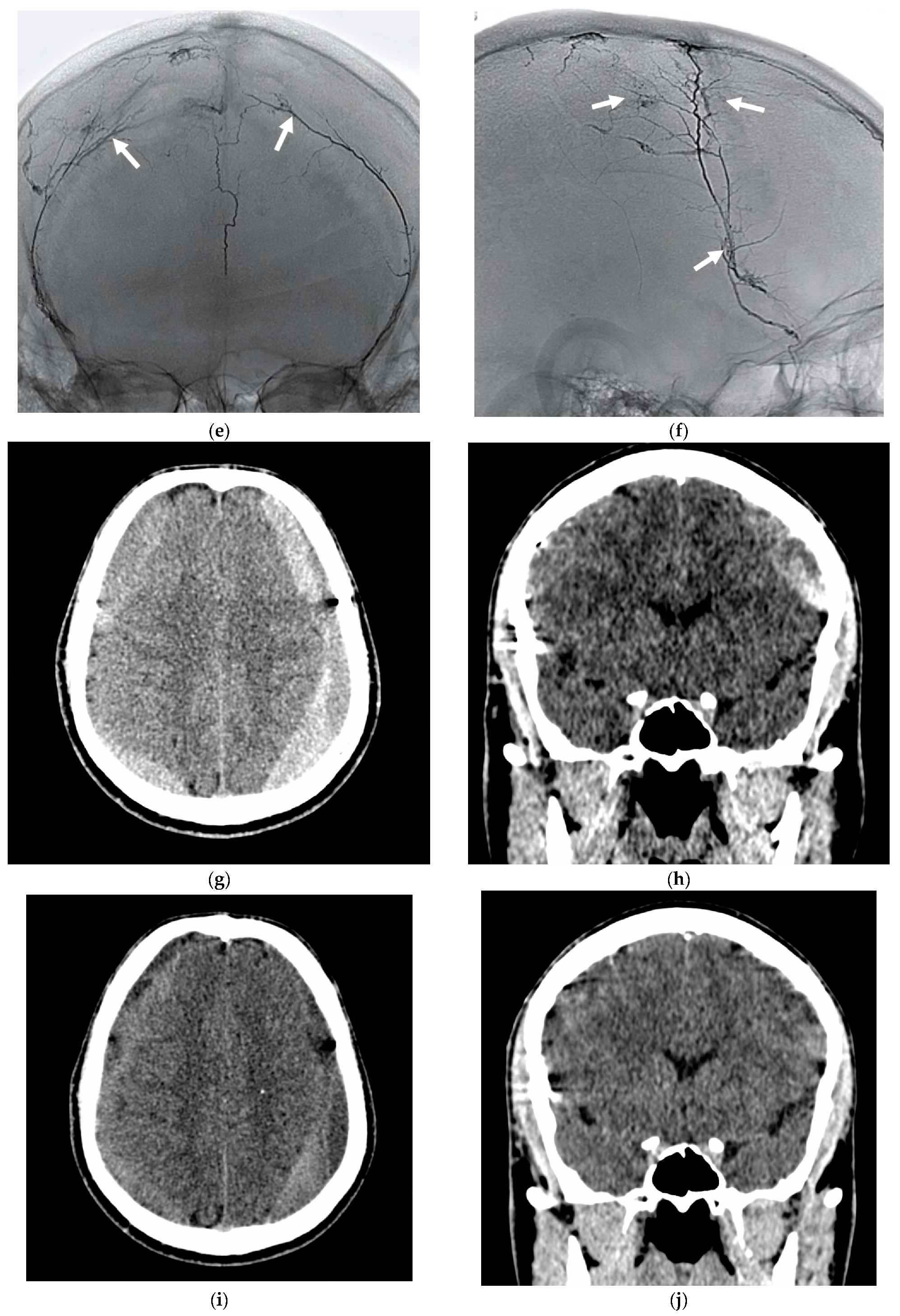
3.4. Illustrative Cases
4. Discussion
- -
- Giant capillaries and macrophage infiltration in the outer layer and the inner layer.
- -
- Tiny newly formed capillaries with highly permeable endothelial gap junctions.
- -
- Endothelial cells expressing high levels of vascular endothelial growth factor (VEGF) and PEGF (placental endothelial growth factor).
- -
- Proliferating fibroblasts forming fibrous granulation tissue with collagen deposition.
- -
- Chronic lymphoplasmacytic and histiocytic inflammation.
- -
- Macrophages containing hemosiderin.
4.1. How to Do It?
- -
- -
- -
- -
- -
- Absolute alcohol [44]
- -
- -
- Phil: Pending
- -
- Squid: Pending
- -
4.2. Is It Safe to Embolize the MMA as a Treatment for CSDH?
4.3. Does the MMA Embolization Work, and Will the CSDH Disappear?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Mureb, M.C.; Kondziolka, D.; Shapiro, M.; Raz, E.; Nossek, E.; Haynes, J.; Farkas, J.; Riina, H.A.; Tanweer, O. DynaCT Enhancement of subdural membranes after middle meningeal artery embolization: Insights into pathophysiology. World Neurosurg. 2020, 139, e265–e270. [Google Scholar] [CrossRef]
- Link, T.W.; Rapoport, B.I.; Paine, S.M.; Kamel, H.; Knopman, J. Middle meningeal artery embolization for chronic subdural hematoma: Endovascular technique and radiographic findings. Interv. Neuroradiol. 2018, 24, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Entezami, P.; Boulos, A.; Paul, A.; Nourollahzadeh, E.; Dalfino, J. Contrast enhancement of chronic subdural hematomas after embolization of the middle meningeal artery. Interv. Neuroradiol. 2019, 25, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Santarius, T.; Kirkpatrick, P.J.; Kolias, A.G.; Hutchinson, P.J. Working toward rational and evidence-based treatment of chronic subdural hematoma. Clin. Neurosurg. 2010, 57, 112–122. [Google Scholar] [PubMed]
- Asghar, M.; Adhiyaman, V.; Greenway, M.W.; Bhowmick, B.K.; Bates, A. Chronic subdural haematoma in the elderly—A North Wales experience. J. R. Soc. Med. 2002, 95, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Li, Y.; Huang, J.; Zhang, H.; Wang, X.; Dong, L.; Yan, Z.; She, L. Chronic subdural haematoma in antithrombotic cohorts: Characteristics, surgical outcomes, and recurrence. Br. J. Neurosurg. 2020, 34, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Huang, J. Chronic subdural hematoma: Epidemiology and natural history. Neurosurg. Clin. N. Am. 2017, 28, 205–210. [Google Scholar] [CrossRef]
- White, M.; Mathieson, C.S.; Campbell, E.; Lindsay, K.W.; Murray, L. Treatment of chronic subdural haematomas–a retrospective comparison of minicraniectomy versus burrhole drainage. Br. J. Neurosurg. 2010, 24, 257–260. [Google Scholar] [CrossRef]
- Ivamoto, H.S.; Lemos, H.P.; Atallah, A.N. Surgical treatments for chronic subdural hematomas: A comprehensive systematic review. World Neurosurg. 2016, 86, 399–418. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Loos, F.; Dünisch, P.; Sakr, Y.; Safatli, D.A.; Kalff, R.; Ewald, C. Risk factors for reoperation after initial burr hole trephination in chronic subdural hematomas. Clin. Neurol. Neurosurg. 2015, 138, 66–71. [Google Scholar] [CrossRef]
- Maher Hulou, M.; McLouth, C.J.; Hayden, C.S.; Sheldrake, A.K.; Parekh, M.; Dillen, W.L.; Wheeler, G.R.; Fraser, J.F. Predictors of re-operation in the setting of non-acute subdural hematomas: A 12-year single center retrospective study. J. Clin. Neurosci. 2020, 81, 334–339. [Google Scholar] [CrossRef]
- Torihashi, K.; Sadamasa, N.; Yoshida, K.; Narumi, O.; Chin, M.; Yamagata, S. Independent predictors for recurrence of chronic subdural hematoma: A review of 343 consecutive surgical cases. Neurosurgery 2008, 63, 1125–1129, discussion 1129. [Google Scholar] [CrossRef]
- Nakagawa, I.; Park, H.S.; Kotsugi, M.; Wada, T.; Takeshima, Y.; Matsuda, R.; Nishimura, F.; Yamada, S.; Motoyama, Y.; Park, Y.S.; et al. Enhanced hematoma membrane on DynaCT images during middle meningeal artery embolization for persistently recurrent chronic subdural hematoma. World Neurosurg. 2019, 126, e473–e479. [Google Scholar] [CrossRef] [PubMed]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of chronic subdural haematoma: Inflammation, angiogenesis and implications for pharmacotherapy. J. Neuroinflamm. 2017, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- Moshayedi, P.; Liebeskind, D.S. Middle meningeal artery embolization in chronic subdural hematoma: Implications of pathophysiology in trial design. Front. Neurol. 2020, 11, 923. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Fujimoto, S.; Saitoh, K.; Satoh, S.; Nagamatsu, K.; Midorikawa, H. Superselective angiographic findings of ipsilateral middle meningeal artery of chronic subdural hematoma in adults. No Shinkei Geka 1998, 26, 339–347. [Google Scholar]
- Pouvelle, A.; Pouliquen, G.; Premat, K.; Chougar, L.; Lenck, S.; Degos, V.; Sourour, N.-A.; Mathon, B.; Clarençon, F.; Shotar, E. Larger middle meningeal arteries on computed tomography angiography in patients with chronic subdural hematomas as compared with matched controls. J. Neurotrauma 2020, 37, 2703–2708. [Google Scholar] [CrossRef]
- Ishihara, H.; Ishihara, S.; Kohyama, S.; Yamane, F.; Ogawa, M.; Sato, A.; Matsutani, M. Experience in endovascular treatment of recurrent chronic subdural hematoma. Interv. Neuroradiol. 2007, 13 (Suppl. S1), 141–144. [Google Scholar] [CrossRef] [Green Version]
- Ban, S.P.; Hwang, G.; Byoun, H.S.; Kim, T.; Lee, S.U.; Bang, J.S.; Han, J.H.; Kim, C.-Y.; Kwon, O.-K.; Oh, C.W. Middle meningeal artery embolization for chronic subdural hematoma. Radiology 2018, 286, 992–999. [Google Scholar] [CrossRef]
- Fiorella, D.; Arthur, A.S. Middle meningeal artery embolization for the management of chronic subdural hematoma. J. Neurointerv. Surg. 2019, 11, 912–915. [Google Scholar] [CrossRef]
- Vollherbst, D.F.; Chapot, R.; Bendszus, M.; Möhlenbruch, M.A. Glue, Onyx, Squid or PHIL? Liquid embolic agents for the embolization of cerebral arteriovenous malformations and dural arteriovenous fistulas. Clin. Neuroradiol. 2021. [Google Scholar] [CrossRef]
- Shotar, E.; Premat, K.; Lenck, S.; Degos, V.; Marijon, P.; Pouvelle, A.; Pouliquen, G.; Mouyal, S.; Jaoude, S.A.; Sourour, N.-A.; et al. Angiographic anatomy of the middle meningeal artery in relation to chronic subdural hematoma embolization. Clin. Neuroradiol. 2021. [Google Scholar] [CrossRef]
- Virchow, R. Das Hämatom der Dura mater. Verhandlungen der Physikalisch-Medizinischen Gesellschaft zu Würzburg 1857, 7, 134–142. [Google Scholar]
- Hohenstein, A.; Erber, R.; Schilling, L.; Weigel, R. Increased MRNA Expression of VEGF within the hematoma and imbalance of angiopoietin-1 and -2 MRNA within the neomembranes of chronic subdural hematoma. J. Neurotrauma 2005, 22, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Ohashi, T.; Watanabe, D.; Koyama, S.; Namatame, H.; Izawa, H.; Haraoka, R.; Okada, H.; Ichimasu, N.; Akimoto, J.; et al. Usefulness of embolization of the middle meningeal artery for refractory chronic subdural hematomas. Surg. Neurol. Int. 2013, 4, 104. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, J. Advances in surgical treatment of chronic subdural hematoma. Chin. J. Traumatol. 2003, 6, 41–44. [Google Scholar] [PubMed]
- Mehta, V.; Harward, S.C.; Sankey, E.W.; Nayar, G.; Codd, P.J. Evidence based diagnosis and management of chronic subdural hematoma: A review of the literature. J. Clin. Neurosci. 2018, 50, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, A.; Rock, M.; Dowlati, E.; Miller, C.; Mai, J.C.; Liu, A.-H.; Armonda, R.A.; Felbaum, D.R. Middle meningeal artery embolization with subdural evacuating port system for primary management of chronic subdural hematomas. Neurosurg. Rev. 2021. [Google Scholar] [CrossRef]
- Ng, S.; Derraz, I.; Boetto, J.; Dargazanli, C.; Poulen, G.; Gascou, G.; Lefevre, P.-H.; Molinari, N.; Lonjon, N.; Costalat, V. Middle meningeal artery embolization as an adjuvant treatment to surgery for symptomatic chronic subdural hematoma: A pilot study assessing hematoma volume resorption. J. NeuroInterv. Surg. 2020, 12, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, J.; Carnevale, J.A.; Goldberg, J.L.; Ramos, A.D.; Link, T.W.; Knopman, J. Perioperative prophylactic middle meningeal artery embolization for chronic subdural hematoma: A Series of 44 Cases. J. Neurosurg. 2021, 1–9. [Google Scholar] [CrossRef]
- Yokoya, S.; Nishii, S.; Takezawa, H.; Katsumori, T.; Takagi, Y.; Goto, Y.; Oka, H.; Shiomi, N.; Hino, A. Organized chronic subdural hematoma treated with middle meningeal artery embolization and small craniotomy: Two case reports. Asian J. Neurosurg. 2020, 15, 421. [Google Scholar] [CrossRef] [PubMed]
- Scerrati, A.; Visani, J.; Ricciardi, L.; Dones, F.; Rustemi, O.; Cavallo, M.A.; Bonis, P.D. To drill or not to drill, that is the question: Nonsurgical treatment of chronic subdural hematoma in the elderly. A systematic review. Neurosurg. Focus 2020, 49, E7. [Google Scholar] [CrossRef]
- Poulsen, F.R.; Munthe, S.; Søe, M.; Halle, B. Perindopril and residual chronic subdural hematoma volumes six weeks after burr hole surgery: A randomized trial. Clin. Neurol. Neurosurg. 2014, 123, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Lodewijkx, R.; Immenga, S.; Berg, R.V.D.; Post, R.; Westerink, L.G.; Nabuurs, R.J.A.; Can, A.; Vandertop, W.P.; Verbaan, D. Tranexamic acid for chronic subdural hematoma. Br. J. Neurosurg. 2021, 12, 1–6. [Google Scholar] [CrossRef]
- Rajah, G.B.; Waqas, M.; Dossani, R.H.; Vakharia, K.; Gong, A.D.; Rho, K.; Housley, S.B.; Rai, H.H.; Chin, F.; Tso, M.K.; et al. Transradial middle meningeal artery embolization for chronic subdural hematoma using onyx: Case series. J. NeuroInterv. Surg. 2020, 12, 1214–1218. [Google Scholar] [CrossRef]
- Yajima, H.; Kanaya, H.; Ogino, M.; Ueki, K.; Kim, P. Middle meningeal artery embolization for chronic subdural hematoma with high risk of recurrence: A single institution experience. Clin. Neurol. Neurosurg. 2020, 197, 106097. [Google Scholar] [CrossRef] [PubMed]
- Hirai, S.; Ono, J.; Odaki, M.; Serizawa, T.; Nagano, O. Embolization of the middle meningeal artery for refractory chronic subdural haematoma: Usefulness for patients under anticoagulant therapy. Interv. Neuroradiol. 2004, 10, 101–104. [Google Scholar] [CrossRef]
- Kim, E. Embolization therapy for refractory hemorrhage in patients with chronic subdural hematomas. World Neurosurg. 2017, 101, 520–527. [Google Scholar] [CrossRef]
- Okuma, Y.; Hirotsune, N.; Sato, Y.; Tanabe, T.; Muraoka, K.; Nishino, S. Midterm follow-up of patients with middle meningeal artery embolization in intractable chronic subdural hematoma. World Neurosurg. 2019, 126, e671–e678. [Google Scholar] [CrossRef]
- Tiwari, A.; Dmytriw, A.A.; Bo, R.; Farkas, N.; Ye, P.; Gordon, D.S.; Arcot, K.M.; Turkel-Parrella, D.; Farkas, J. Recurrence and coniglobus volumetric resolution of subacute and chronic subdural hematoma post-middle meningeal artery embolization. Diagnostics 2021, 11, 257. [Google Scholar] [CrossRef]
- Matsumoto, H.; Hanayama, H.; Okada, T.; Sakurai, Y.; Minami, H.; Masuda, A.; Tominaga, S.; Miyaji, K.; Yamaura, I.; Yoshida, Y. Which surgical procedure is effective for refractory chronic subdural hematoma? Analysis of our surgical procedures and literature review. J. Clin. Neurosci. 2018, 49, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Mandai, S.; Sakurai, M.; Matsumoto, Y. Middle meningeal artery embolization for refractory chronic subdural hematoma: Case report. J. Neurosurg. 2000, 93, 686–688. [Google Scholar] [CrossRef]
- Al-Mufti, F.; Kaur, G.; Amuluru, K.; Cooper, J.B.; Dakay, K.; El-Ghanem, M.; Pisapia, J.; Muh, C.; Tyagi, R.; Bowers, C.; et al. Middle meningeal artery embolization using combined particle embolization and n-BCA with the dextrose 5% in water push technique for chronic subdural hematomas: A prospective safety and feasibility study. Am. J. Neuroradiol. 2021, 42, 916–920. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Wang, H.; Ding, J.; Xu, C.; Liu, Y.; Wang, C.; Li, Z. Application of absolute alcohol in the treatment of traumatic intracranial hemorrhage via interventional embolization of middle meningeal artery. Front. Neurol. 2020, 11, 824. [Google Scholar] [CrossRef]
- Waqas, M.; Vakhari, K.; Weimer, P.V.; Hashmi, E.; Davies, J.M.; Siddiqui, A.H. Safety and effectiveness of embolization for chronic subdural hematoma: Systematic review and case series. World Neurosurg. 2019, 126, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Faber, R.; Feller, C.N.; Gofman, N.; Fletcher, J.; Hedayat, H.S. Pediatric middle meningeal artery embolization for chronic subdural hematoma: A case report. Surg. Neurol. Int. 2021, 12, 239. [Google Scholar] [CrossRef]
- Kang, J.; Whang, K.; Hong, S.-K.; Pyen, J.-S.; Cho, S.-M.; Kim, J.-Y.; Kim, S.-H.; Oh, J.-W. Middle meningeal artery embolization in recurrent chronic subdural hematoma combined with arachnoid cyst. Korean J. Neurotrauma 2015, 11, 187–190. [Google Scholar] [CrossRef] [Green Version]
- Catapano, J.S.; Ducruet, A.F.; Nguyen, C.L.; Baranoski, J.F.; Cole, T.S.; Majmundar, N.; Wilkinson, D.A.; Fredrickson, V.L.; Cavalcanti, D.D.; Albuquerque, F.C. Middle meningeal artery embolization for chronic subdural hematoma: An institutional technical analysis. J. NeuroInterv. Surg. 2021, 13, 657–660. [Google Scholar] [CrossRef]
- Kan, P.; Maragkos, G.A.; Srivatsan, A.; Srinivasan, V.; Johnson, J.; Burkhardt, J.-K.; Robinson, T.M.; Salem, M.M.; Chen, S.; Riina, H.A.; et al. Middle meningeal artery embolization for chronic subdural hematoma: A multi-center experience of 154 consecutive embolizations. Neurosurgery 2021, 88, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Link, T.W.; Boddu, S.; Paine, S.M.; Kamel, H.; Knopman, J. Middle meningeal artery embolization for chronic subdural hematoma: A series of 60 cases. Neurosurgery 2019, 85, 801–807. [Google Scholar] [CrossRef]
- Martinez-Perez, R.; Rayo, N.; Tsimpas, A. Embolización endovascular de la arteria meníngea media para el tratamiento de hematomas subdurales crónicos: Efectividad, seguridad y controversia actual. Revisión sistemática. Neurología 2020. [Google Scholar] [CrossRef] [PubMed]
- Jumah, F.; Osama, M.; Islim, A.I.; Jumah, A.; Patra, D.P.; Kosty, J.; Narayan, V.; Nanda, A.; Gupta, G.; Dossani, R.H. Efficacy and safety of middle meningeal artery embolization in the management of refractory or chronic subdural hematomas: A systematic review and meta-analysis. Acta Neurochir. 2020, 162, 499–507. [Google Scholar] [CrossRef]
- Joyce, E.; Bounajem, M.T.; Scoville, J.; Thomas, A.J.; Ogilvy, C.S.; Riina, H.A.; Tanweer, O.; Levy, E.I.; Spiotta, A.M.; Gross, B.A.; et al. Middle meningeal artery embolization treatment of nonacute subdural hematomas in the elderly: A multiinstitutional experience of 151 cases. Neurosurg. Focus 2020, 49, E5. [Google Scholar] [CrossRef]
- Piergallini, L.; Dargazanli, C.; Derraz, I.; Costalat, V. Immediate development of dural arteriovenous fistula after middle meningeal artery embolization: First angiographic demonstration. World Neurosurg. 2019, 128, 606–610. [Google Scholar] [CrossRef]
- Raviskanthan, S.; Mortensen, P.W.; Zhang, Y.J.; Lee, A.G. Bilateral abducens nerve palsies after middle meningeal artery embolization for chronic subdural hematoma. J. Neuroophthalmol. 2021. [Google Scholar] [CrossRef]
- Gomez-Paz, S.; Akamatsu, Y.; Salem, M.M.; Enriquez-Marulanda, A.; Robinson, T.M.; Ogilvy, C.S.; Thomas, A.J.; Moore, J.M. Upfront middle meningeal artery embolization for treatment of chronic subdural hematomas in patients with or without midline shift. Interv. Neuroradiol. 2020, 27, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Chihara, H.; Imamura, H.; Ogura, T.; Adachi, H.; Imai, Y.; Sakai, N. Recurrence of a refractory chronic subdural hematoma after middle meningeal artery embolization that required craniotomy. NMC Case Rep. J. 2014, 1, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, H.; Tanaka, M.; Hadeishi, H. Angiogenesis in the septum and inner membrane of refractory chronic subdural hematomas: Consideration of findings after middle meningeal artery embolization with low-concentration n-butyl-2-cyanoacrylate. NMC Case Rep. J. 2019, 6, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Wang, C.; Li, Z. Recurrent bilateral chronic subdural hematoma after interventional embolization combined with drilling and drainage treatment. J. Craniofac. Surg. 2020, 31, e171. [Google Scholar] [CrossRef] [PubMed]
- Haldrup, M.; Ketharanathan, B.; Debrabant, B.; Schwartz, O.S.; Mikkelsen, R.; Fugleholm, K.; Poulsen, F.R.; Jensen, T.S.R.; Thaarup, L.V.; Bergholt, B. Embolization of the middle meningeal artery in patients with chronic subdural hematoma—a systematic review and meta-analysis. Acta Neurochir. 2020, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Dian, J.; Linton, J.; Shankar, J.J. Risk of recurrence of subdural hematoma after EMMA vs surgical drainage—Systematic review and meta-analysis. Interv. Neuroradiol. 2021, 27, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Srivatsan, A.; Mohanty, A.; Nascimento, F.A.; Hafeez, M.U.; Srinivasan, V.M.; Thomas, A.; Chen, S.R.; Johnson, J.N.; Kan, P. Middle meningeal artery embolization for chronic subdural hematoma: Meta-analysis and systematic review. World Neurosurg. 2019, 122, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Marulanda, A.; Gomez-Paz, S.; Salem, M.M.; Mallick, A.; Motiei-Langroudi, R.; Arle, J.E.; Stippler, M.; Papavassiliou, E.; Alterman, R.L.; Ogilvy, C.S.; et al. Middle meningeal artery embolization versus conventional treatment of chronic subdural hematomas. Neurosurgery 2021, 89, 486–495. [Google Scholar] [CrossRef]
- Edlmann, E.; Holl, D.C.; Lingsma, H.F.; Bartek, J.; Bartley, A.; Duerinck, J.; Jensen, T.S.R.; Soleman, J.; Shanbhag, N.C.; Devi, B.I.; et al. Systematic review of current randomised control trials in chronic subdural haematoma and proposal for an international collaborative approach. Acta Neurochir (Wien) 2020, 162, 763–776. [Google Scholar] [CrossRef] [PubMed]
- Benitez, R. Pilot Study to Evaluate Safety of and Efficacy of Middle Meningeal Artery (MMA) Embolization Compared to Traditional Surgical Strategies to Treat Chronic Subdural Hematomas (CSDH). 2019. Available online: clinicaltrials.gov (accessed on 20 August 2021).
- Calnan, D.R. A Single Center Randomized Control Trial to Evaluate the Efficacy of Middle Meningeal Artery Embolization in the Treatment of Chronic Subdural Hematomas. 2021. Available online: clinicaltrials.gov (accessed on 20 August 2021).
- Assistance Publique–Hôpitaux de Paris. Embolization of the Middle Meningeal Artery for the Prevention of Chronic Subdural Hematoma Recurrence in High Risk Patients, a Randomized Controlled Trial. 2021. Available online: clinicaltrials.gov (accessed on 20 August 2021).
- Augusta University. Endovascular Embolization for Chronic Subdural Hematomas Following Surgical Evacuation. 2020. Available online: clinicaltrials.gov (accessed on 20 August 2021).
- Osbun, J.W. Middle Meningeal Artery (MMA) Embolization for Patients With Chronic Subdural Hematoma (cSDH). 2019. Available online: clinicaltrials.gov (accessed on 20 August 2021).
- Medtronic Neurovascular Clinical Affairs. A Study of the Embolization of the Middle Meningeal Artery with ONYXTM Liquid Embolic System in the Treatment of Subacute and Chronic Subdural HEmatoma (EMBOLISE). 2021. Available online: clinicaltrials.gov (accessed on 20 August 2021).
- Balt USA. The SQUID Trial for the Embolization of the Middle Meningeal Artery for Treatment of Chronic Subdural Hematoma (STEM). 2021. Available online: clinicaltrials.gov (accessed on 20 August 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient # Age (Years) Gender | Side Symptoms | VolumePre Embol (mL) | Days Post Embol | Volume Post Embol (mL) | Surgery | Complication Outcome |
|---|---|---|---|---|---|---|
| 1, 44, f | bilateral headache, nausea | right 18 left 9 | 2 | right 16 | pre embol | none mRS 0 |
| left 6 | ||||||
| 15 | right 9 | |||||
| left 5 | ||||||
| 64 | 0 | |||||
| 2, 56, m | bilateral headache, nausea | right 22 left 25 | 1 | right 21 | none | none mRS 0 |
| left 23 | ||||||
| 5 | right 21 | |||||
| left 38 | ||||||
| 57 | 0 | |||||
| 3, 42, m | bilateral headache, nausea | right 69 left 83 | 1 | right 68 | none | none mRS 0 |
| left 71 | ||||||
| 8 | right 55 | |||||
| left 74 | ||||||
| 29 | right 47 | |||||
| left 42 | ||||||
| 180 | 0 | |||||
| 4, 74, m | left headache, nausea | 88 | 4 | 63 | pre embol | none mRS 0 |
| 8 | 35 | |||||
| 120 | 0 | |||||
| 5, 80, m | bilateral headache, nausea | right 44 left 54 | 1 | right 39 | pre embol (right side) | none mRS 0 |
| left 44 | ||||||
| 12 | right 33 | |||||
| left 29 | ||||||
| 16 | right 28 | |||||
| left 25 | ||||||
| 45 | right 15 | |||||
| left 19 | ||||||
| 210 | 0 | |||||
| 6, 70, m | left mild right-handed hemiparesis up to 4 points, seizures | 105 | 1 | 96 | none | none mRS 1 |
| 6 | 85 | |||||
| 10 | 79 | |||||
| 17 | 76 | |||||
| 180 | 0 | |||||
| 7, 89, f | bilateral tetraparesis (muscle strength up to 1–2 points on the right, up to 3 points on the left, depression of consciousness, obtundation) | right 55 left 67 | 1 | right 53 | none | none mRS 0 |
| left 66 | ||||||
| 3 | right 49 | |||||
| left 62 | ||||||
| 23 | right 38 | |||||
| left 56 | ||||||
| 31 | right 25 | |||||
| left 32 | ||||||
| 90 | 0 | |||||
| 8, 75, m | left mild right-handed hemiparesis, aphasia, headaches, nausea | 169 | 1 | 155 | pre embol | none mRS 0 |
| 5 | 142 | |||||
| 8 | 138 | |||||
| 60 | 0 | |||||
| 9, 59, f | right headache, nausea | 65 | 1 | 47 | pre embol | none mRS 0 |
| 5 | 33 | |||||
| 90 | 0 | |||||
| 10, 71, m | left headache, nausea | 77 | 2 | 68 | none | none mRS 0 |
| 60 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrov, A.; Ivanov, A.; Rozhchenko, L.; Petrova, A.; Bhogal, P.; Cimpoca, A.; Henkes, H. Endovascular Treatment of Chronic Subdural Hematomas through Embolization: A Pilot Study with a Non-Adhesive Liquid Embolic Agent of Minimal Viscosity (Squid). J. Clin. Med. 2021, 10, 4436. https://doi.org/10.3390/jcm10194436
Petrov A, Ivanov A, Rozhchenko L, Petrova A, Bhogal P, Cimpoca A, Henkes H. Endovascular Treatment of Chronic Subdural Hematomas through Embolization: A Pilot Study with a Non-Adhesive Liquid Embolic Agent of Minimal Viscosity (Squid). Journal of Clinical Medicine. 2021; 10(19):4436. https://doi.org/10.3390/jcm10194436
Chicago/Turabian StylePetrov, Andrey, Arkady Ivanov, Larisa Rozhchenko, Anna Petrova, Pervinder Bhogal, Alexandru Cimpoca, and Hans Henkes. 2021. "Endovascular Treatment of Chronic Subdural Hematomas through Embolization: A Pilot Study with a Non-Adhesive Liquid Embolic Agent of Minimal Viscosity (Squid)" Journal of Clinical Medicine 10, no. 19: 4436. https://doi.org/10.3390/jcm10194436