
Syndrome of Undifferentiated Recurrent Fever (SURF): An Emerging Group of Autoinflammatory Recurrent Fevers


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Studies Selection and Main Characteristics
3.2. Genotype-Phenotype Assessment
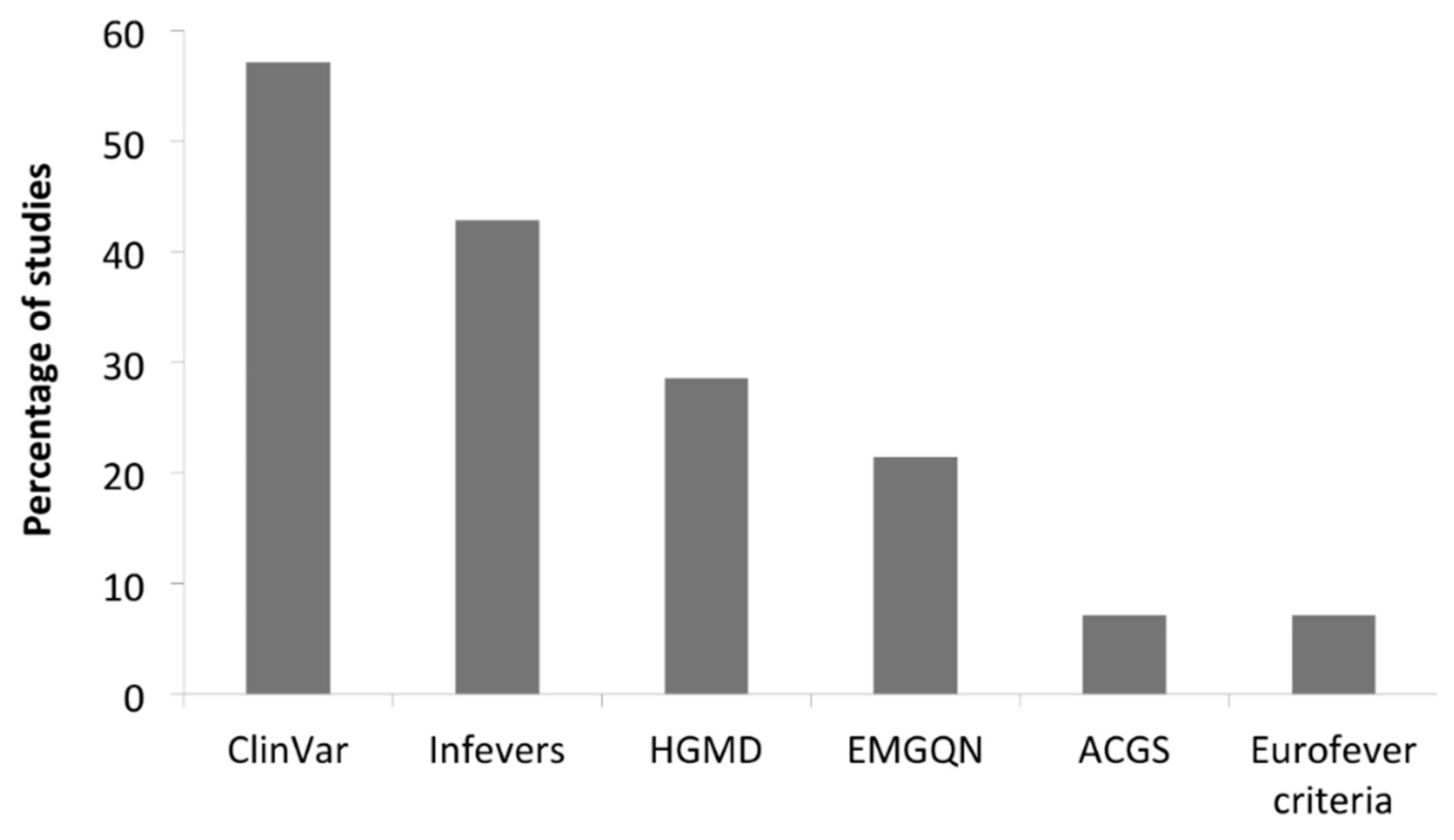
3.3. Variants Characteristics
3.4. Clinical Manifestations
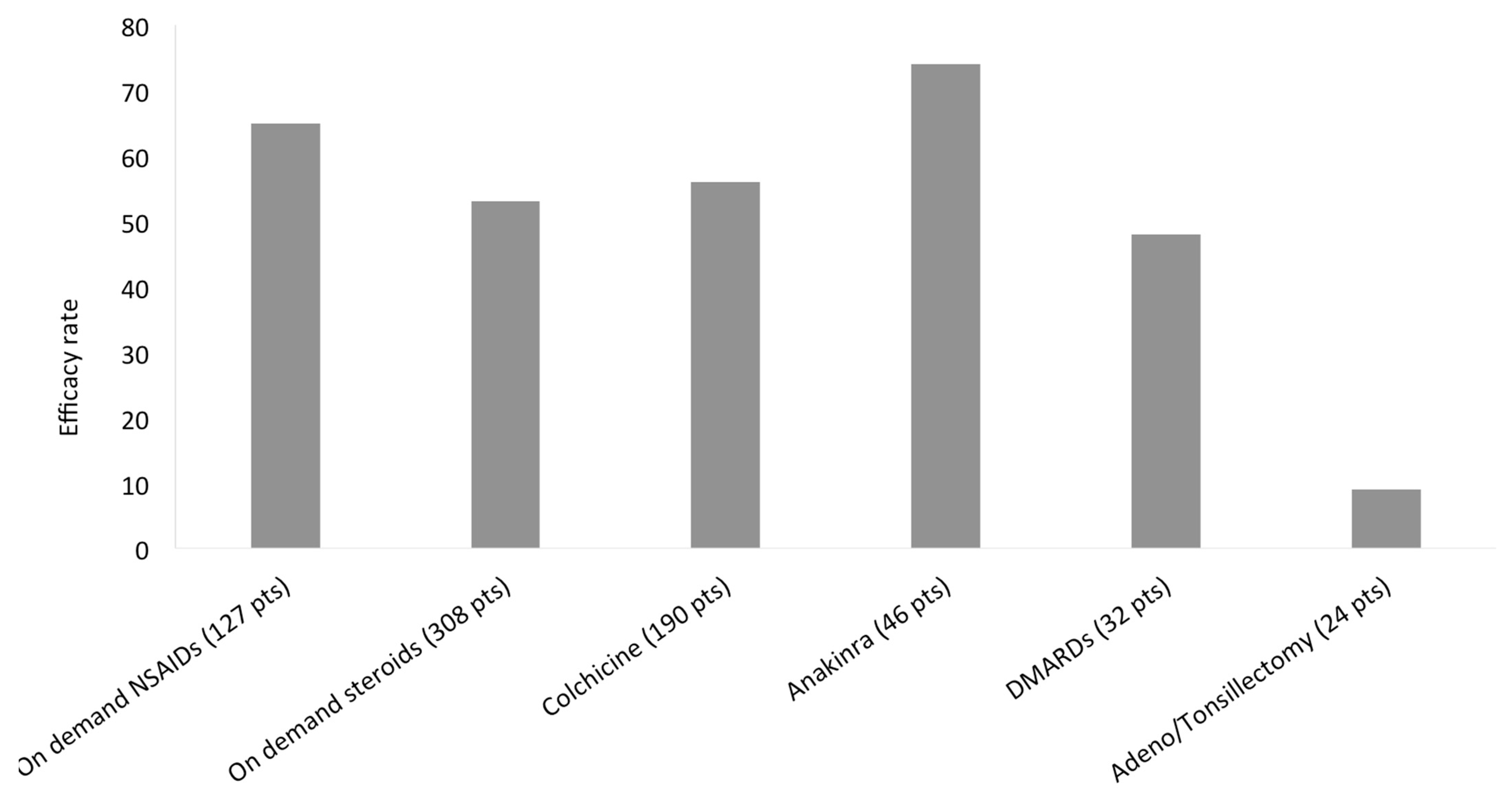
3.5. Treatment Response

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Chandrakasan et al. [5] | Harrison et al. [24] | De Pauli et al. [22] | Ozyilmaz et al. [11] | Ter Haar et al. [21] | Garg et al. [23] | Papa et al. [3] | Hidaka et al. [16] | Demir et al. [19] |
|---|---|---|---|---|---|---|---|---|---|
| Year | 2014 | 2016 | 2018 | 2019 | 2019 | 2019 | 2020 | 2020 | 2020 |
| Patients | 25 | 11 | 23 | 9 | 180 | 22 | 34 | 133 | 49 |
| Ethnicity (patients) | Caucasian (14), African (7), others (5) | Caucasian (10), Jewish (1) | Caucasian (20), Middle Eastern (2), others (1) | Middle Eastern | Mixed | Caucasian (11), Asian (5), Jewish (1), African (1), others (4) | Caucasian | Asian | Caucasian, Middle Eastern |
| Age at enrollment, median (range), years | 2.5 (0–9) | ND | 4.3 (2–9) | 18 (1–47) | ND | ND | ND | 39.9 (22–57) | 5.9 (3–9) |
| Age at onset, median (range), years | 1.4 (0–5) | 35 (24–76) | 0 (0–2) | ND | 4.3 (1–12) ** | 0.61 (0–13.5) | ND | 33.4 (13–53) | 3 (1–6) |
| Adults onset | 0 (0) | 11 (100) | 0 (0) | 0 (0) | 65 (35) ** | 0 (0) | ND | ND | ND |
| Gender, M:F | 16:9 | 5:6 | 5:18 | 5:4 | 51:49 ** | 8:14 | ND | 66:67 | 34:15 |
| Positive family history | 0 (0) | 0 (0) | ND | 1 (11) | 24 (13) ** | 7 (32) | ND | ND | 12 (24) |
| Attacks/year, median (range) | 8 (4–12) | ND | ND | ND | 12 (5–14.5) | ND | 12 (7–24) | ND ^ | 10 (6–12) |
| Attacks duration, median (range), days | 4 (3–5) | ND | ND | ND | 4 (3–7) | ND | 5.9 (4.5–7.3) | ND ^ | 3 (2–4) |
| Clinical manifestations | 25 (100) | 11 (100) | 23 (100) | 9 (100) | 180 (100) | 22 (100) | 34 (100) | 133 (100) | 49 (100) |
| Fever | 25 (100) | 11 (100) | ND | 6 (67) | 180 (100) | 13 (59) | 34 (100) | 133 (100) | 49 (100) |
| Abdominal pain | 1 (4) | 2 (18) *** | 12 (52) | 8 (89) | 87 (48) | 4 (18) | 17 (50) | ND | 31 (63) |
| Nausea/Vomiting | ND | 2 (18) *** | ND | ND | 44 (24) | 5 (23) | 3 (9) | ND | 8 (16) |
| Diarrhea | 2 (8) | 2 (18) *** | ND | ND | 30 (17) | 3 (14) | 3 (9) | 40 (30) | 5 (10) |
| Rash/Erythema | 3 (12) | 9 (82) | ND | ND | 35 (20) | 12 (55) | 11 (32) | 10 (8) | 22 (45) |
| Genital ulcers | ND | 1 (9) | ND | ND | ND | ND | ND | ND | ND |
| Oral ulcers | 1 (4) | 3 (27) | 12 (52) | ND | 53 (29) | ND | 13 (38) | ND | 14 (29) |
| Pharyngitis/Tonsillitis | 1 (4) | ND | 13 (57) | ND | 47 (18) | ND | 13 (38) | ND | 5 (10) |
| Eye manifestations | ND | ND | ND | ND | ND | 14 (64) | ND | ND | 11 (22) |
| Arthritis | 2 (8) | 5 (46) | ND | 1 (11) | 12 (7) | 12 (55) | 7 (21) | ND | 4 (8) |
| Arthralgia | ND | 8 (72) | ND | ND | 107 (59) | 10 (46) | 12 (35) | 57 (43) | 27 (55) |
| Myalgia | ND | 8 (72) | 15 (65) | ND | 80 (44) | 13 (59) | 9 (27) | 25 (19) | 23 (47) |
| Headache | 1 (4) | 5 (46) | ND | 1 (11) | 67 (37) | 1 (5) | 7 (20) | ND | 10 (20) |
| Morning headache | ND | ND | ND | ND | 22 (12) | ND | ND | ND | ND |
| Fatigue | ND | 11 (100) *** | ND | ND | 106 (59) | ND | ND | ND | ND |
| Malaise | ND | 11 (100) *** | ND | ND | 99 (55) | ND | ND | ND | ND |
| Lymphadenopathy | 1 (4) | 4 (36) | ND | ND | 76 (42) | 12 (55) | 6 (18) | ND | ND |
| Splenomegaly | ND | ND | ND | ND | 20 (11) | ND | 5 (15) *** | ND | 1 (2) |
| Hepatomegaly | ND | ND | ND | ND | 21 (12) | ND | 5 (15) *** | ND | ND |
| Chest pain | ND | 1 (9) | 0 (0) | 0 (0) | 21 (12) | 5 (23) | ND | 17 (13) | 4 (8) |
| Pericarditis | ND | 2 (18) | ND | ND | 10 (6) | ND | ND | ND | 1 (2) |
| Urethritis/cystitis | ND | ND | ND | ND | 6 (3) | ND | ND | ND | ND |
| Gonadal pain | ND | ND | ND | ND | 3 (2) | ND | ND | ND | ND |
| Neck stiffness | 1 (4) | ND | ND | ND | ND | ND | ND | ND | ND |
| Sinusitis | ND | 6 (55) | ND | ND | ND | ND | ND | ND | ND |
| Febrile seizure | ND | ND | ND | ND | ND | ND | ND | ND | 4 (8) |
| Pleuritis | ND | ND | ND | ND | ND | ND | ND | ND | 1 (2) |
| Proteinuria | ND | ND | ND | ND | ND | ND | ND | ND | 1 (2) |
| Amyloidosis | ND | ND | ND | ND | ND | ND | ND | ND | 1 (2) |
| Sensorineural hearing loss | ND | ND | ND | 0 (0) | ND | ND | ND | ND | 0 (0) |
| Patients with information about the response to treatment | 25 (100) | 11 (100) | ND | ND | ND | 22 (100) | 18 (53) | 133 (100) | 49 (100) |
| On demand NSAIDs | ND | ND | ND | ND | 80/105 (76%) | 3/22 (14%) | ND | ND | ND |
| On demand steroids | ND | 6/10 (60%) | 16/21 (76%) | ND | 85/104 (82%) | 11/22 (50%) | 17/18 (94%) | 29/133 (22%) | ND |
| Colchicine | 15/25 (60%) | 0/3 (0) | 6/13 (46%) | ND | 29/49 (59%) | ND | 14/18 (78%) | 44/133 (33%) | 31/49 (63%) |
| DMARDs | ND | 0/10 (0) | ND | ND | 7/10 (70%) | 13/22 (59%) | ND | ND | ND |
| Anakinra | ND | 10/11 (90%) | ND | ND | 8/13 (62%) | 16/22 (73%) | ND | ND | ND |
| Tonsillectomy/Adenoidectomy | ND | ND | 0/12 (0) | ND | 2/12 (17%) | ND | ND | ND | ND |
4. Discussion
5. Footnote
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Broderick, L.; Hoffman, H.M. Pediatric Recurrent Fever and Autoinflammation from the Perspective of an Allergist/Immunologist. J. Allergy Clin. Immunol. 2020, 146, 960–966.e2. [Google Scholar] [CrossRef]
- Rusmini, M.; Federici, S.; Caroli, F.; Grossi, A.; Baldi, M.; Obici, L.; Insalaco, A.; Tommasini, A.; Caorsi, R.; Gallo, E.; et al. Next-Generation Sequencing and Its Initial Applications for Molecular Diagnosis of Systemic Auto-Inflammatory Diseases. Ann. Rheum. Dis. 2016, 75, 1550–1557. [Google Scholar] [CrossRef]
- Papa, R.; Rusmini, M.; Volpi, S.; Caorsi, R.; Picco, P.; Grossi, A.; Caroli, F.; Bovis, F.; Musso, V.; Obici, L.; et al. Next Generation Sequencing Panel in Undifferentiated Autoinflammatory Diseases Identifies Patients with Colchicine-Responder Recurrent Fevers. Rheumatology 2020, 59, 344–360. [Google Scholar] [CrossRef]
- Orange, D.E.; Yao, V.; Sawicka, K.; Fak, J.; Frank, M.O.; Parveen, S.; Blachere, N.E.; Hale, C.; Zhang, F.; Raychaudhuri, S.; et al. RNA Identification of PRIME Cells Predicting Rheumatoid Arthritis Flares. N. Engl. J. Med. 2020, 383, 218–228. [Google Scholar] [CrossRef]
- Chandrakasan, S.; Chiwane, S.; Adams, M.; Fathalla, B.M. Clinical and Genetic Profile of Children with Periodic Fever Syndromes from a Single Medical Center in South East Michigan. J. Clin. Immunol. 2014, 34, 104–113. [Google Scholar] [CrossRef] [PubMed]
- De Pieri, C.; Vuch, J.; De Martino, E.; Bianco, A.M.; Ronfani, L.; Athanasakis, E.; Bortot, B.; Crovella, S.; Taddio, A.; Severini, G.M.; et al. Genetic Profiling of Autoinflammatory Disorders in Patients with Periodic Fever: A Prospective Study. Pediatr. Rheumatol. Online J. 2015, 13, 11. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, M.; Oda, H.; Nakagawa, K.; Yasumi, T.; Kawai, T.; Izawa, K.; Nishikomori, R.; Heike, T.; Ohara, O. Accurate Clinical Genetic Testing for Autoinflammatory Diseases Using the Next-Generation Sequencing Platform MiSeq. Biochem. Biophys. Rep. 2017, 9, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Omoyinmi, E.; Standing, A.; Keylock, A.; Price-Kuehne, F.; Melo Gomes, S.; Rowczenio, D.; Nanthapisal, S.; Cullup, T.; Nyanhete, R.; Ashton, E.; et al. Clinical Impact of a Targeted Next-Generation Sequencing Gene Panel for Autoinflammation and Vasculitis. PLoS ONE 2017, 12, e0181874. [Google Scholar] [CrossRef] [Green Version]
- Kostik, M.M.; Suspitsin, E.N.; Guseva, M.N.; Levina, A.S.; Kazantseva, A.Y.; Sokolenko, A.P.; Imyanitov, E.N. Multigene Sequencing Reveals Heterogeneity of NLRP12-Related Autoinflammatory Disorders. Rheumatol. Int. 2018, 38, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Karacan, İ.; Balamir, A.; Uğurlu, S.; Aydın, A.K.; Everest, E.; Zor, S.; Önen, M.Ö.; Daşdemir, S.; Özkaya, O.; Sözeri, B.; et al. Diagnostic Utility of a Targeted Next-Generation Sequencing Gene Panel in the Clinical Suspicion of Systemic Autoinflammatory Diseases: A Multi-Center Study. Rheumatol. Int. 2019, 39, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Ozyilmaz, B.; Kirbiyik, O.; Koc, A.; Ozdemir, T.R.; Kaya Ozer, O.; Kutbay, Y.B.; Erdogan, K.M.; Saka Guvenc, M.; Ozturk, C. Molecular Genetic Evaluation of NLRP3, MVK and TNFRSF1A Associated Periodic Fever Syndromes. Int. J. Immunogenet. 2019, 46, 232–240. [Google Scholar] [CrossRef]
- Hua, Y.; Wu, D.; Shen, M.; Yu, K.; Zhang, W.; Zeng, X. Phenotypes and Genotypes of Chinese Adult Patients with Systemic Autoinflammatory Diseases. Semin. Arthritis Rheum. 2019, 49, 446–452. [Google Scholar] [CrossRef]
- Boursier, G.; Rittore, C.; Georgin-Lavialle, S.; Belot, A.; Galeotti, C.; Hachulla, E.; Hentgen, V.; Rossi-Semerano, L.; Sarrabay, G.; Touitou, I. Positive Impact of Expert Reference Center Validation on Performance of Next-Generation Sequencing for Genetic Diagnosis of Autoinflammatory Diseases. J. Clin. Med. 2019, 8, 1729. [Google Scholar] [CrossRef] [Green Version]
- Suspitsin, E.N.; Guseva, M.N.; Kostik, M.M.; Sokolenko, A.P.; Skripchenko, N.V.; Levina, A.S.; Goleva, O.V.; Dubko, M.F.; Tumakova, A.V.; Makhova, M.A.; et al. Next Generation Sequencing Analysis of Consecutive Russian Patients with Clinical Suspicion of Inborn Errors of Immunity. Clin. Genet. 2020, 98, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Sözeri, B.; Demir, F.; Sönmez, H.E.; Karadağ, Ş.G.; Demirkol, Y.K.; Doğan, Ö.A.; Doğanay, H.L.; Ayaz, N.A. Comparison of the Clinical Diagnostic Criteria and the Results of the Next-Generation Sequence Gene Panel in Patients with Monogenic Systemic Autoinflammatory Diseases. Clin. Rheumatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hidaka, Y.; Fujimoto, K.; Matsuo, N.; Koga, T.; Kaieda, S.; Yamasaki, S.; Nakashima, M.; Migita, K.; Nakayama, M.; Ohara, O.; et al. Clinical Phenotypes and Genetic Analyses for Diagnosis of Systemic Autoinflammatory Diseases in Adult Patients with Unexplained Fever. Mod. Rheumatol. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kosukcu, C.; Taskiran, E.Z.; Batu, E.D.; Sag, E.; Bilginer, Y.; Alikasifoglu, M.; Ozen, S. Whole Exome Sequencing in Unclassified Autoinflammatory Diseases: More Monogenic Diseases in the Pipeline? Rheumatology 2020. [Google Scholar] [CrossRef]
- Wang, W.; Yu, Z.; Gou, L.; Zhong, L.; Li, J.; Ma, M.; Wang, C.; Zhou, Y.; Ru, Y.; Sun, Z.; et al. Single-Center Overview of Pediatric Monogenic Autoinflammatory Diseases in the Past Decade: A Summary and Beyond. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef]
- Demir, F.; Doğan, Ö.A.; Demirkol, Y.K.; Tekkuş, K.E.; Canbek, S.; Karadağ, Ş.G.; Sönmez, H.E.; Ayaz, N.A.; Doğanay, H.L.; Sözeri, B. Genetic Panel Screening in Patients with Clinically Unclassified Systemic Autoinflammatory Diseases. Clin. Rheumatol. 2020, 39, 3733–3745. [Google Scholar] [CrossRef] [PubMed]
- Rama, M.; Mura, T.; Kone-Paut, I.; Boursier, G.; Aouinti, S.; Touitou, I.; Sarrabay, G. Is Gene Panel Sequencing More Efficient than Clinical-Based Gene Sequencing to Diagnose Autoinflammatory Diseases? A Randomized Study. Clin. Exp. Immunol. 2021, 203, 105–114. [Google Scholar] [CrossRef]
- Ter Haar, N.M.; Eijkelboom, C.; Cantarini, L.; Papa, R.; Brogan, P.A.; Kone-Paut, I.; Modesto, C.; Hofer, M.; Iagaru, N.; Fingerhutová, S.; et al. Eurofever registry and the Pediatric Rheumatology International Trial Organization (PRINTO). Clinical Characteristics and Genetic Analyses of 187 Patients with Undefined Autoinflammatory Diseases. Ann. Rheum. Dis. 2019, 78, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- De Pauli, S.; Lega, S.; Pastore, S.; Grasso, D.L.; Bianco, A.M.R.; Severini, G.M.; Tommasini, A.; Taddio, A. Neither Hereditary Periodic Fever nor Periodic Fever, Aphthae, Pharingitis, Adenitis: Undifferentiated Periodic Fever in a Tertiary Pediatric Center. World J. Clin. Pediatr. 2018, 7, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.; Wynne, K.; Omoyinmi, E.; Eleftheriou, D.; Brogan, P. Efficacy and Safety of Anakinra for Undifferentiated Autoinflammatory Diseases in Children: A Retrospective Case Review. Rheumatol. Adv. Pract. 2019, 3, rkz004. [Google Scholar] [CrossRef] [Green Version]
- Harrison, S.R.; McGonagle, D.; Nizam, S.; Jarrett, S.; van der Hilst, J.; McDermott, M.F.; Savic, S. Anakinra as a Diagnostic Challenge and Treatment Option for Systemic Autoinflammatory Disorders of Undefined Etiology. JCI Insight 2016, 1, e86336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, K.T.; Feder, H.M.; Lawton, A.R.; Edwards, K.M. Periodic Fever Syndrome in Children. J. Pediatr. 1999, 135, 15–21. [Google Scholar] [CrossRef]
- Gattorno, M.; Hofer, M.; Federici, S.; Vanoni, F.; Bovis, F.; Aksentijevich, I.; Anton, J.; Arostegui, J.I.; Barron, K.; Ben-Cherit, E.; et al. Eurofever Registry and the Paediatric Rheumatology International Trials Organisation (PRINTO). Classification Criteria for Autoinflammatory Recurrent Fevers. Ann. Rheum. Dis. 2019, 78, 1025–1032. [Google Scholar] [CrossRef] [Green Version]
- Masters, S.L.; Simon, A.; Aksentijevich, I.; Kastner, D.L. Horror Autoinflammaticus: The Molecular Pathophysiology of Autoinflammatory Disease (*). Ann. Rev. Immunol. 2009, 27, 621–668. [Google Scholar] [CrossRef] [Green Version]
- Papa, R.; Picco, P.; Gattorno, M. The Expanding Pathways of Autoinflammation: A Lesson from the First 100 Genes Related to Autoinflammatory Manifestations. Adv. Protein Chem. Struct. Biol. 2020, 120, 1–44. [Google Scholar] [CrossRef]
- Papa, R.; Penco, F.; Volpi, S.; Gattorno, M. Actin Remodeling Defects Leading to Autoinflammation and Immune Dysregulation. Front. Immunol. 2020, 11, 604206. [Google Scholar] [CrossRef] [PubMed]







| N° | Study | Date | Enrollment Criteria | Pts | Ethnicity | Genes | MAF | Predictive in Silico Tools | Variant Classification Tools | Sanger Confirmation | Variants | Variants for Pts, Median (Range) | Pts with Clearly Pathogenic Variants | Pts with Likely Pathogenic Variants | Pts with VUS | Pts with Likely Benign or Benign Variants | Pts without Variants |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Chandrakasan et al. [5] | 2014 | Periodic fever | 66 * | Caucasian (14), African (7), others (5)° | 7 | ND | ND | Infevers | Yes | 44 | 0.8 (0–4) * | 25 (42) | 0 (0) | 6 (10) | 0 (0) | 28 (48) |
| 2 | De Pieri et al. [6] | 2015 | Periodic fever with negative or indefinite genetic analysis; PFAPA syndrome with very early onset and/or poor response to steroids or tonsillectomy | 42 | Caucasian | 5 | Any | SIFT, PP2, MT, MutationAssesor, HSF, NNSplice | EMGQN | Yes | 38 | 0.9 (0–4) | 0 (0) | 0 (0) | 24 (57) | 5 (12) | 13 (31) |
| 3 | Rusmini et al. [2] | 2016 | Systemic AID with at least one mutation in one AID-related gene by Sanger sequencing | 50 ** | Caucasian | 10 | <5% | SIFT, PP2 | ND | Yes | 254 | 5(ND) | 23 (68) | 7 (21) | 4 (12) | 0 (0) | 0 (0) |
| 4 | Nakayama et al. [7] | 2017 | Clinical diagnosis of AID | 108 | Asian | 12 | <1% | ND | ND | Yes | 27 | 0.25(ND) | ND | ND | ND | ND | ND |
| 5 | Omoyinmi et al. [8] | 2017 | Undiagnosed inflammatory diseases with clinician suspicion of a genetic cause and negative conventional genetic tests | 50 | Mixed | 166 | <1% ^ | SIFT, PP2, MT | ACGS | Only VUS | 325 | 6.5 (1–16) | 6 (12) | 11 (22) | 31 (62) | 0 (0) | 2 (4) |
| 6 | Kostik et al. [9] | 2018 | Clinical suspicious of primary immunodeficiency with periodic fever | 65 | ND | 302 | <3% | SIFT, PP2, MT, CADD | ClinVar | ND | ND | ND | ND | ND | ND | ND | ND |
| 7 | Karacan et al. [10] | 2019 | Symptoms suggestive of a systemic AID; exclusion of typical FMF | 196 | Middle Eastern | 15 | <1% | ND | ClinVar, Infevers, HGMD | ND | ND | ND | 14 (10) | 27 (14) | 97 (50) § | 97 (50) § | 58 (30) |
| 8 | Ozyilmaz et al. [11] | 2019 | Periodic fever | 64 | Middle Eastern | 3 | Any | ND | ClinVar | ND | 13 | 0.2 (0–1) | 4 (6) | 0 (0) | 3 (5) | 6 (9) | 51 (80) |
| 9 | Hua et al. [12] | 2019 | Chinese adults suspected of systemic AID | 92 | Asian | 5 | ND | ND | EMGQN, Infevers | ND | 49 | 0.5 (0–4) | 5 (5) | 0 (0) | 33 (36) | 0 (0) | 54 (59) |
| 10 | Boursier et al. [13] | 2019 | Suspected monogenic AID (except FMF, DADA2 and MKD after March 2018) | 631 | ND | 55 | ND | SIFT, PP2, MT, MES, HSF, NNSplice, SSF, | Infevers | ND | 176 | 0.3 (ND) | 44 (7) | 50 (8) | 63 (10) | 0 (0) | 474 (75) |
| 11 | Papa et al. [3] | 2020 | Pediatric onset systemic AID; exclusion of PFAPA syndrome and others etiologies; negative or not conclusive Sanger sequencing of suspected genes | 50 | Caucasian | 41 | <3% | SIFT, MT, FATHMM, MetaSVM, PROVEAN, CADD | ClinVar | Yes | 100 | 2 (0–6) | 3 (8) | 3 (8) | 25 (50) | 10 (20) | 9 (18) |
| 12 | Suspitsin et al. [14] | 2020 | Periodic fever | 56 | ND | 354 | ND | ND | ClinVar | Yes | ND | ND | 9 (16) § | 9 (16) § | 7 (13) | 40 (71) § | 40 (71) § |
| 13 | Sözeri et al. [15] | 2020 | Symptoms suggestive of a systemic AID; exclusion of FMF, PFAPA syndrome and other common etiologies; positive Eurofever score for MKD, TRAPS and CAPS | 71 | Caucasian, Middle Eastern | 16 | <1% | SIFT, PP2, MT, GERP | EMGQN, ClinVar, HGMD, Eurofever criteria | ND | 74 | 1 (0–3) | 35 (49) | 0 (0) | 36 (51) § | 36 (51) § | 36 (51) § |
| 14 | Hidaka et al. [16] | 2020 | Unexplained fever | 176 | Asian | 11 | <1% | ND | ND | ND | ND | ND | 29 (17) | 0 (0) | 53 (30) | 0 (0) | 94 (53) |
| 15 | Kosukcu et al. [17] | 2020 | Recurrent fever and high C-reactive protein along with clinical features of inflammation with a possible AID; infections excluded; negative analysis of 14 AID-related genes | 11 | Middle Eastern | WES | <1% | SIFT, PP2, MT, CADD, REVEL, VEST4 | ND | ND | ND | ND | 4 (36) § | 4 (36) § | 7 (64) | 0 (0) | 0 (0) |
| 16 | Wang et al. [18] | 2020 | Pediatric patients suspected of monogenic AID | 288 | Asian | 3/347/WES | <1% | SIFT, PP2, MT, CADD, UMD-Predictor | ClinVar, Infevers, HGMD | Yes | ND | ND | 79 (27) | ND | ND | ND | ND |
| 17 | Demir et al. [19] | 2020 | Symptoms suggestive of a systemic AID; exclusion of FMF, PFAPA syndrome, Blau syndrome, infantile sarcoidosis and other common etiologies; positive Eurofever score for MKD, TRAPS and CAPS | 64 | Caucasian, Middle Eastern | 16 | <1% | SIFT, PP2, MT, GERP | ClinVar, HGMD | Yes | ND | ND | 15 (23) | 21 (33) § | 21 (33) § | 28 (44) § | 28 (44) § |
| 18 | Rama et al. [20] | 2021 | Symptoms of AID (>3 attacks, elevated CRP, age of onset <30 years); exclusion of Armenian, Turkish, Sephardic and Arabic when mentioned and other causes of inflammation | 99 | ND | 55 | <1% | SIFT, PP2, MT, MES, HSF, NNSplice, GVGD, Grantham score | Infevers | Yes | ND | ND | 10 (10) § | 10 (10) § | 20 (20) | 69 (70) § | 69 (70) § |
| Mandatory features |
|---|
| Recurrent fever with elevated inflammatory markers 1 |
| Negative criteria for PFAPA 2 |
| Negative genotype for HRF 3 |
| Additional supporting features |
| Monthly attacks |
| Attacks duration of 3–5 days |
| Fatigue/malaise |
| Arthralgia/myalgia |
| Abdominal pain |
| Eye manifestations 4 |
| Continuous colchicine/anti-IL1 response 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papa, R.; Penco, F.; Volpi, S.; Sutera, D.; Caorsi, R.; Gattorno, M. Syndrome of Undifferentiated Recurrent Fever (SURF): An Emerging Group of Autoinflammatory Recurrent Fevers. J. Clin. Med. 2021, 10, 1963. https://doi.org/10.3390/jcm10091963
Papa R, Penco F, Volpi S, Sutera D, Caorsi R, Gattorno M. Syndrome of Undifferentiated Recurrent Fever (SURF): An Emerging Group of Autoinflammatory Recurrent Fevers. Journal of Clinical Medicine. 2021; 10(9):1963. https://doi.org/10.3390/jcm10091963
Chicago/Turabian StylePapa, Riccardo, Federica Penco, Stefano Volpi, Diana Sutera, Roberta Caorsi, and Marco Gattorno. 2021. "Syndrome of Undifferentiated Recurrent Fever (SURF): An Emerging Group of Autoinflammatory Recurrent Fevers" Journal of Clinical Medicine 10, no. 9: 1963. https://doi.org/10.3390/jcm10091963