
Clinical Significance of Tumor Microenvironment in Acral Melanoma: A Large Single-Institution Study of Caucasians


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
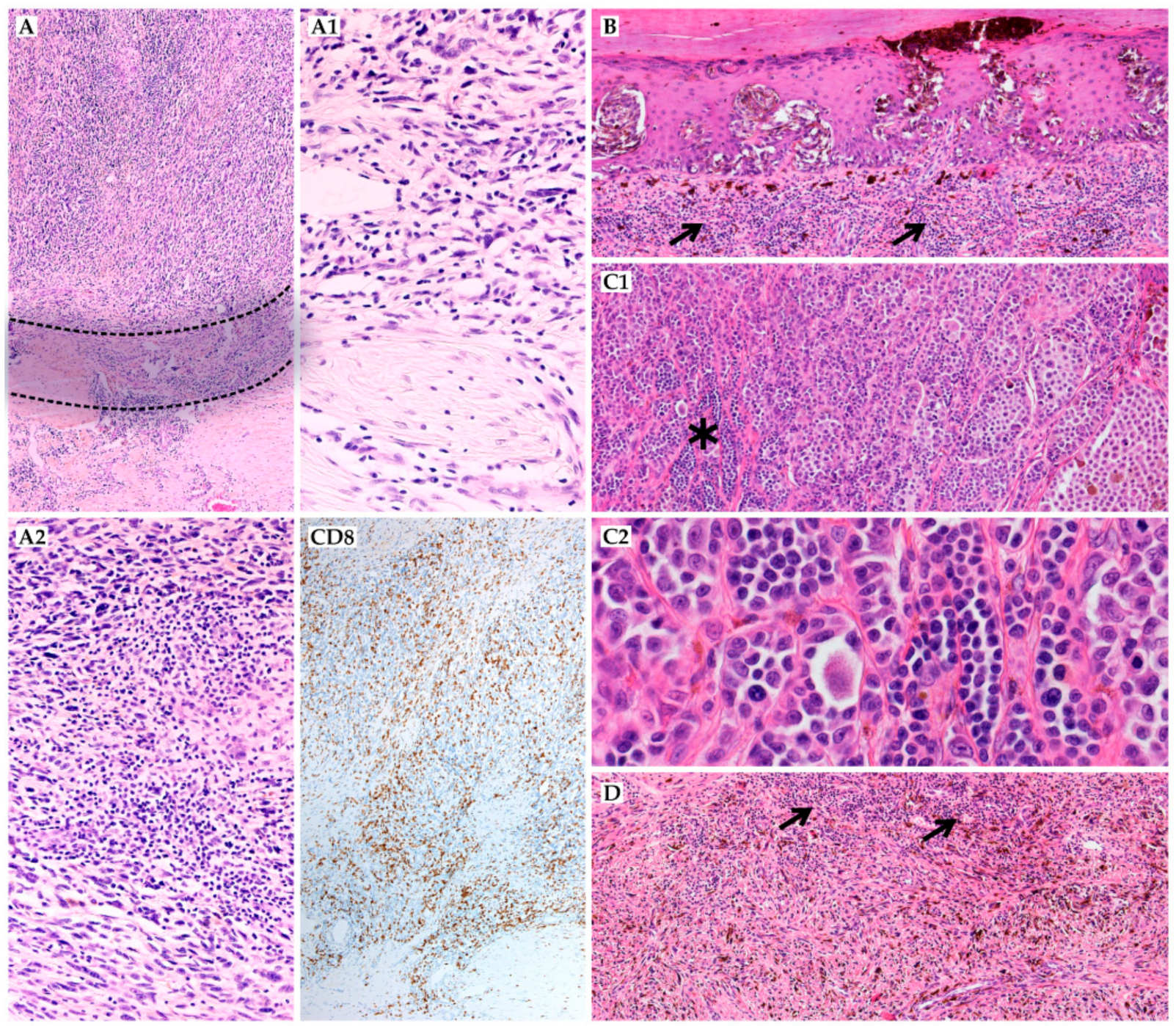
2.2. Histopathological Evaluation
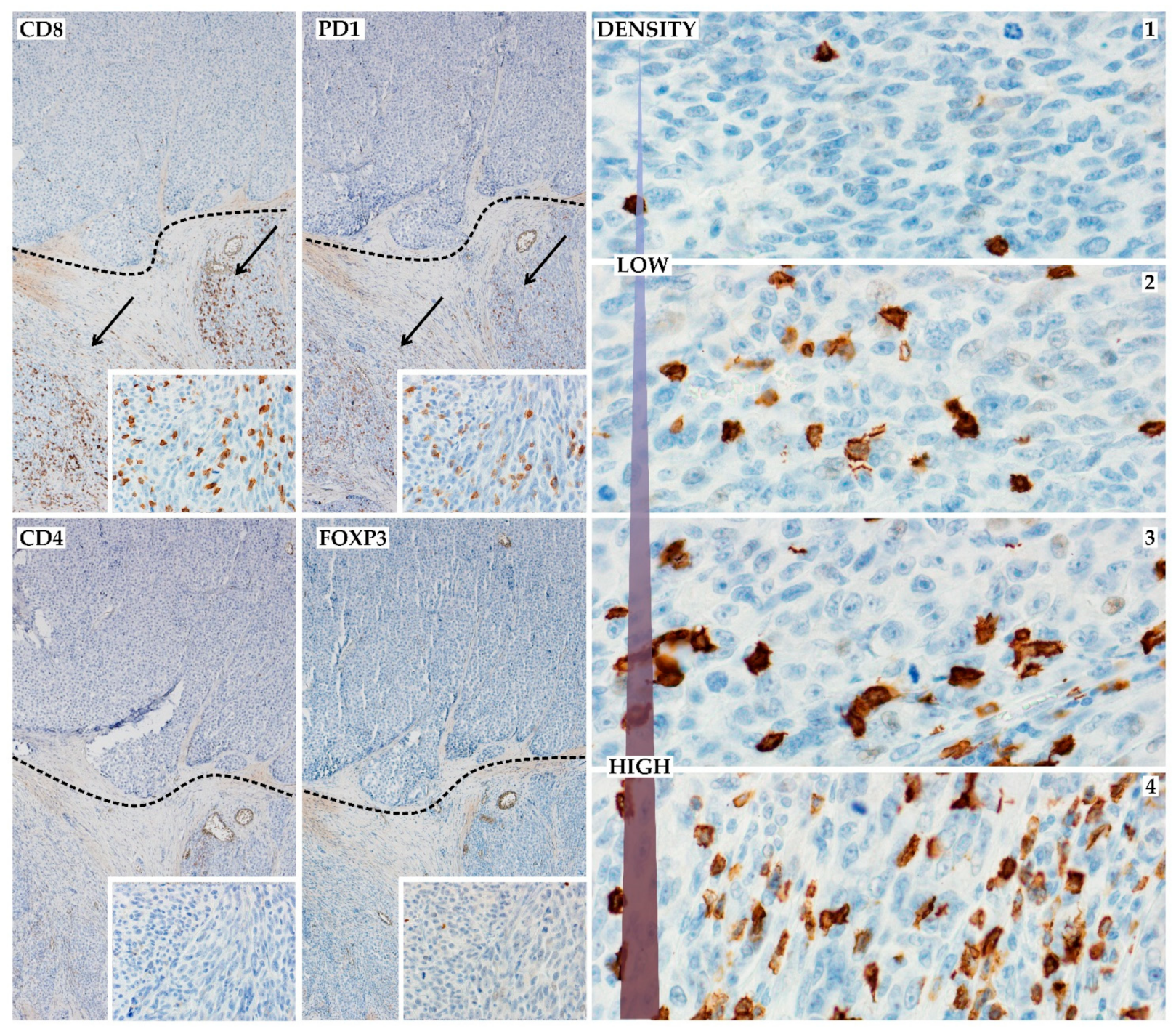
2.3. Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. Clinicopathological Features
3.2. Histopathological and Immunohistochemical Features
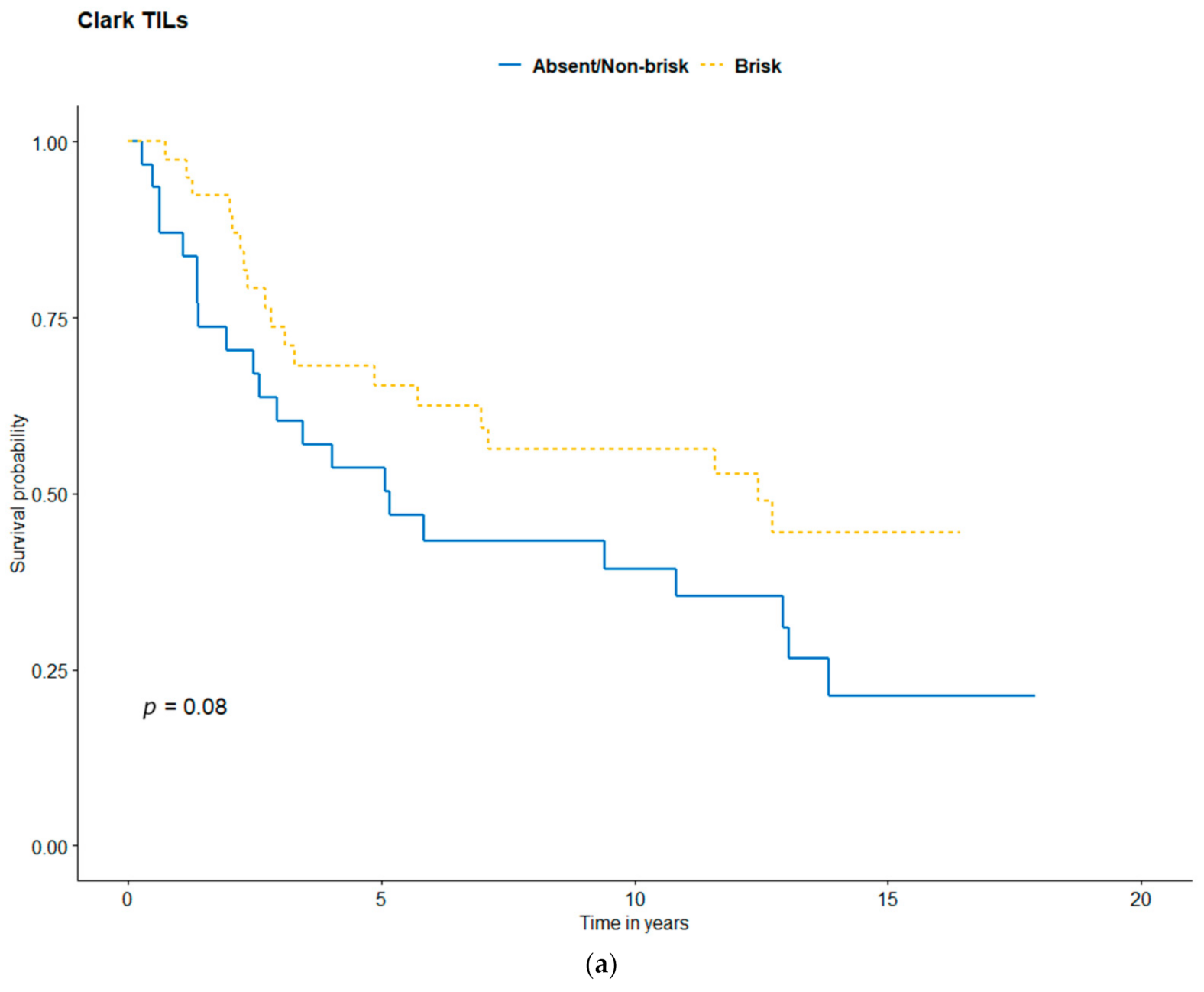
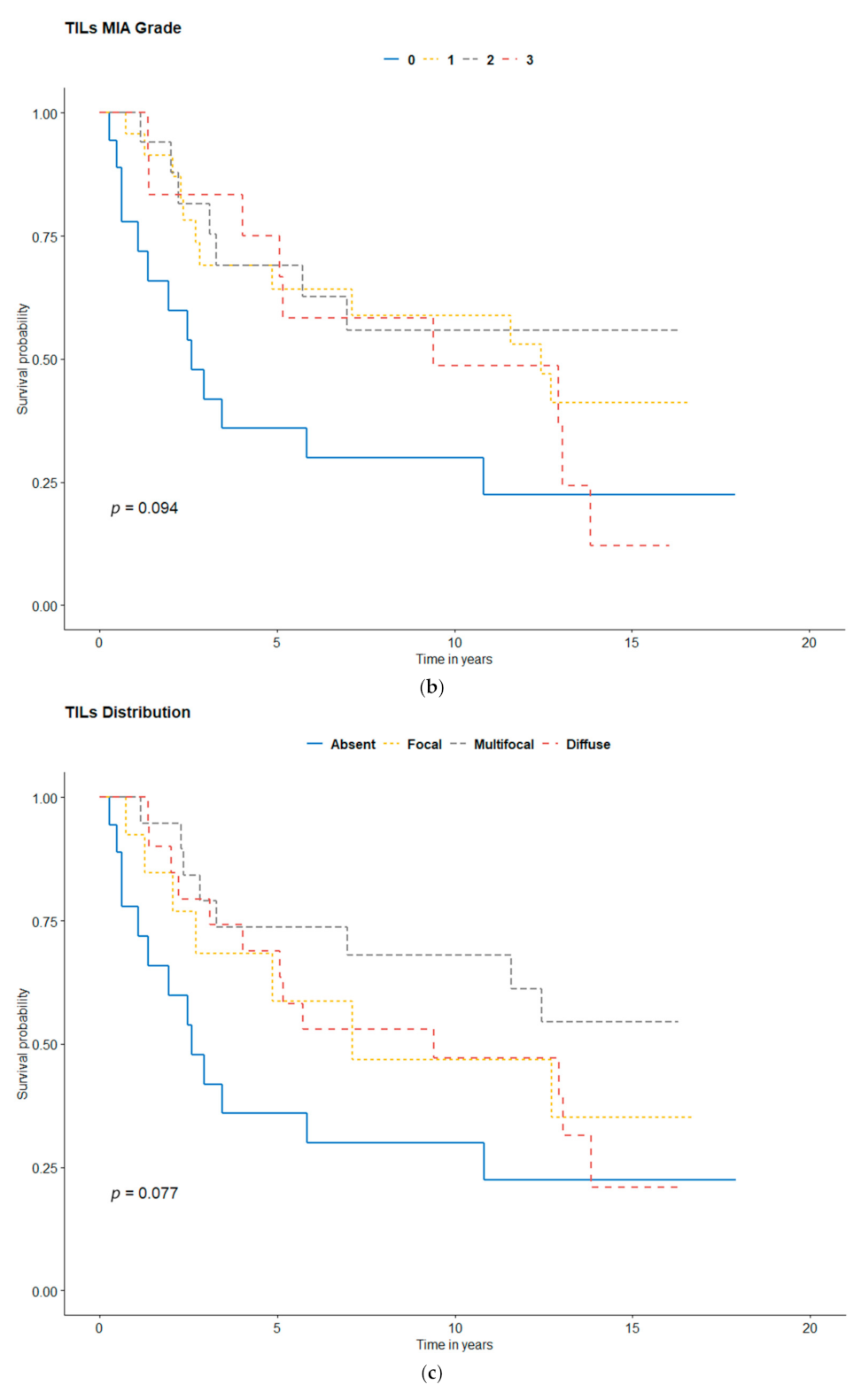
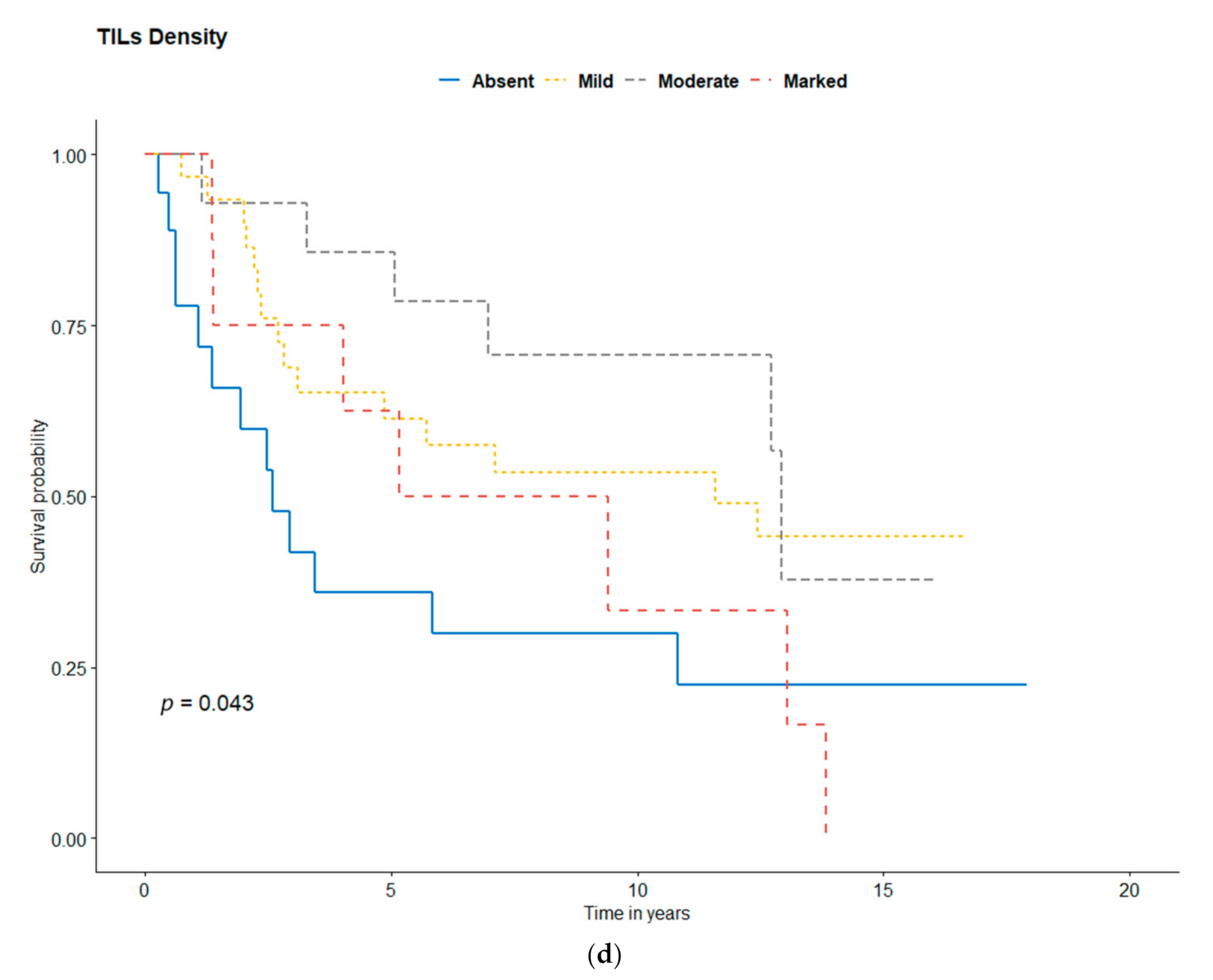
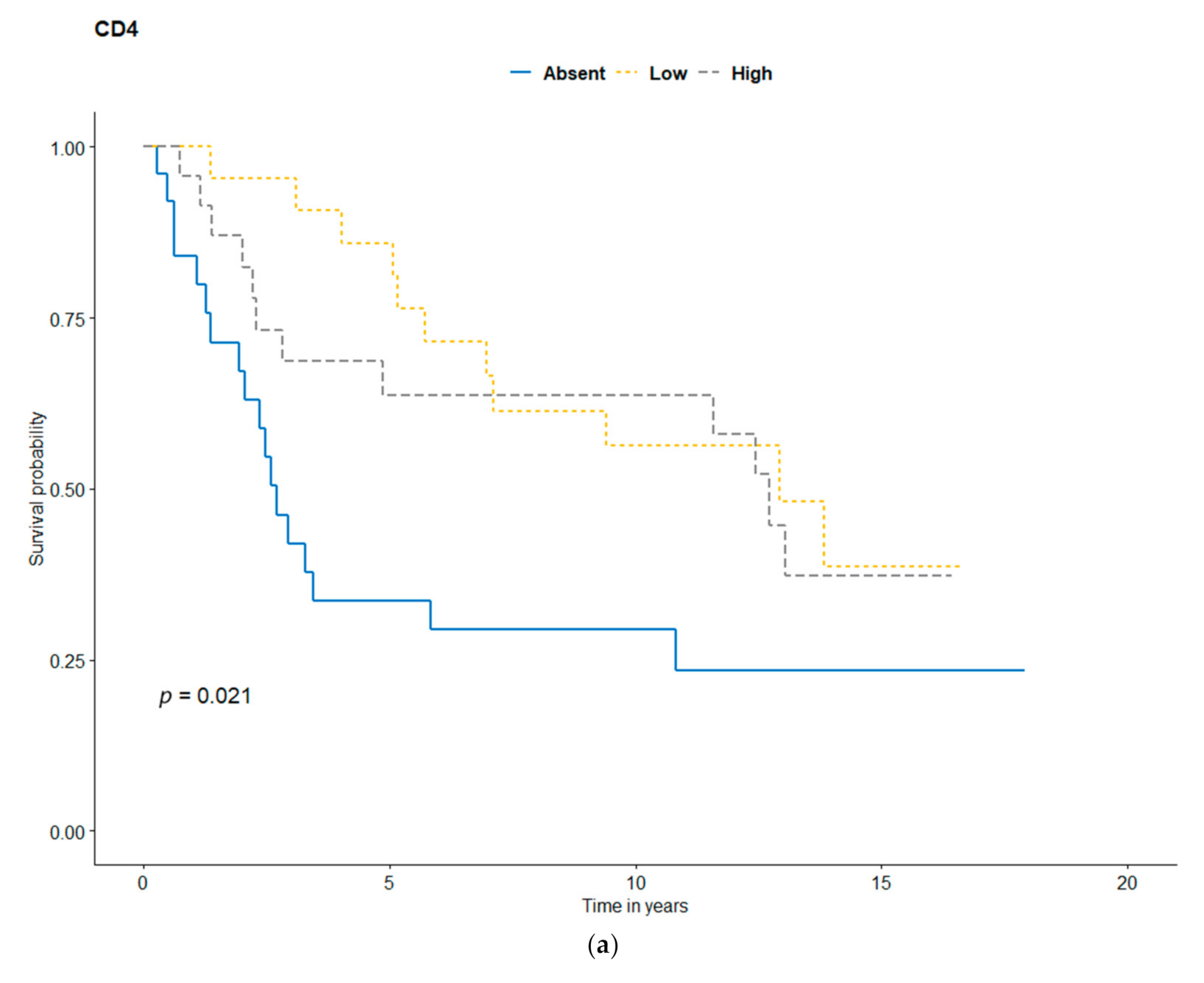
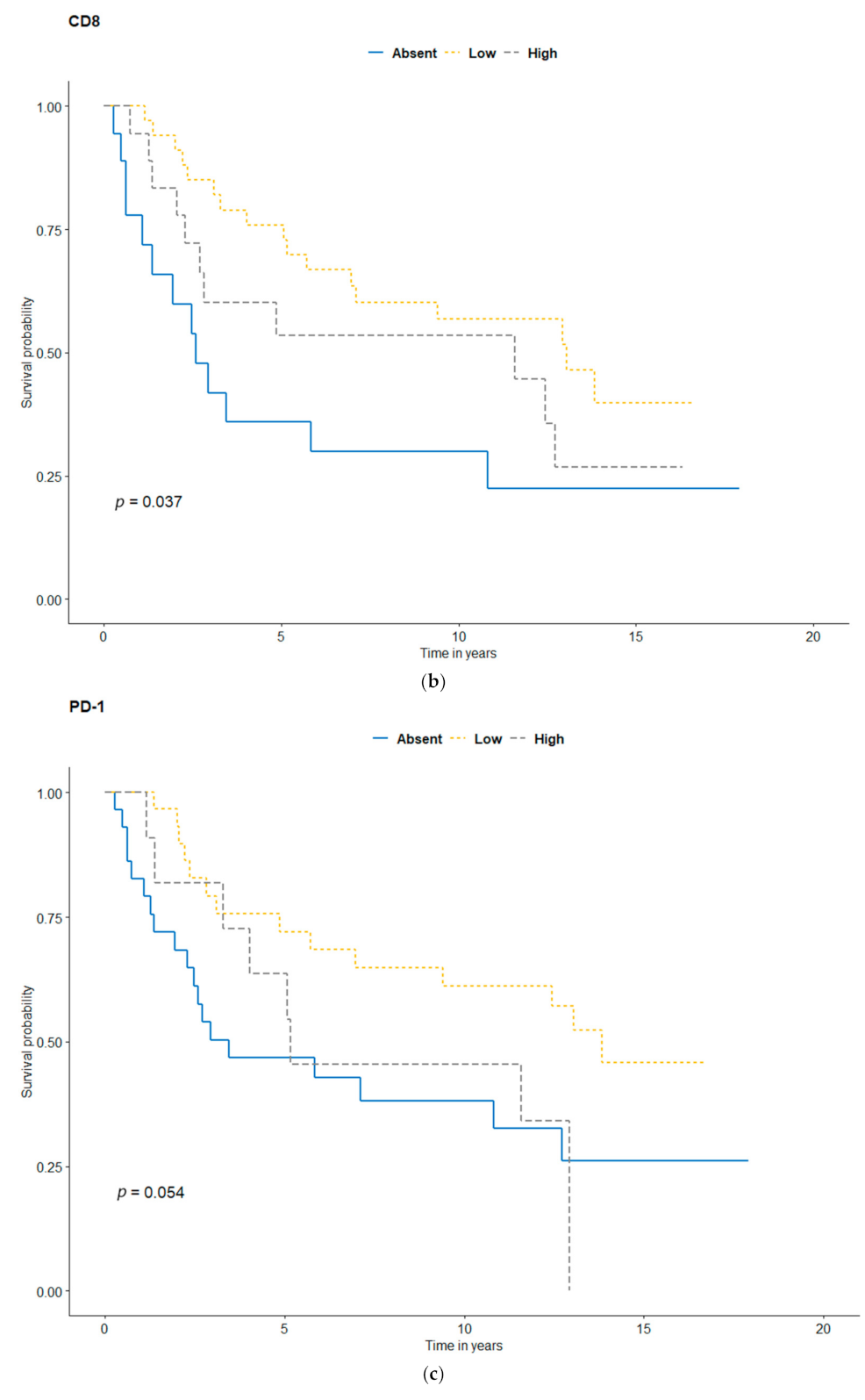
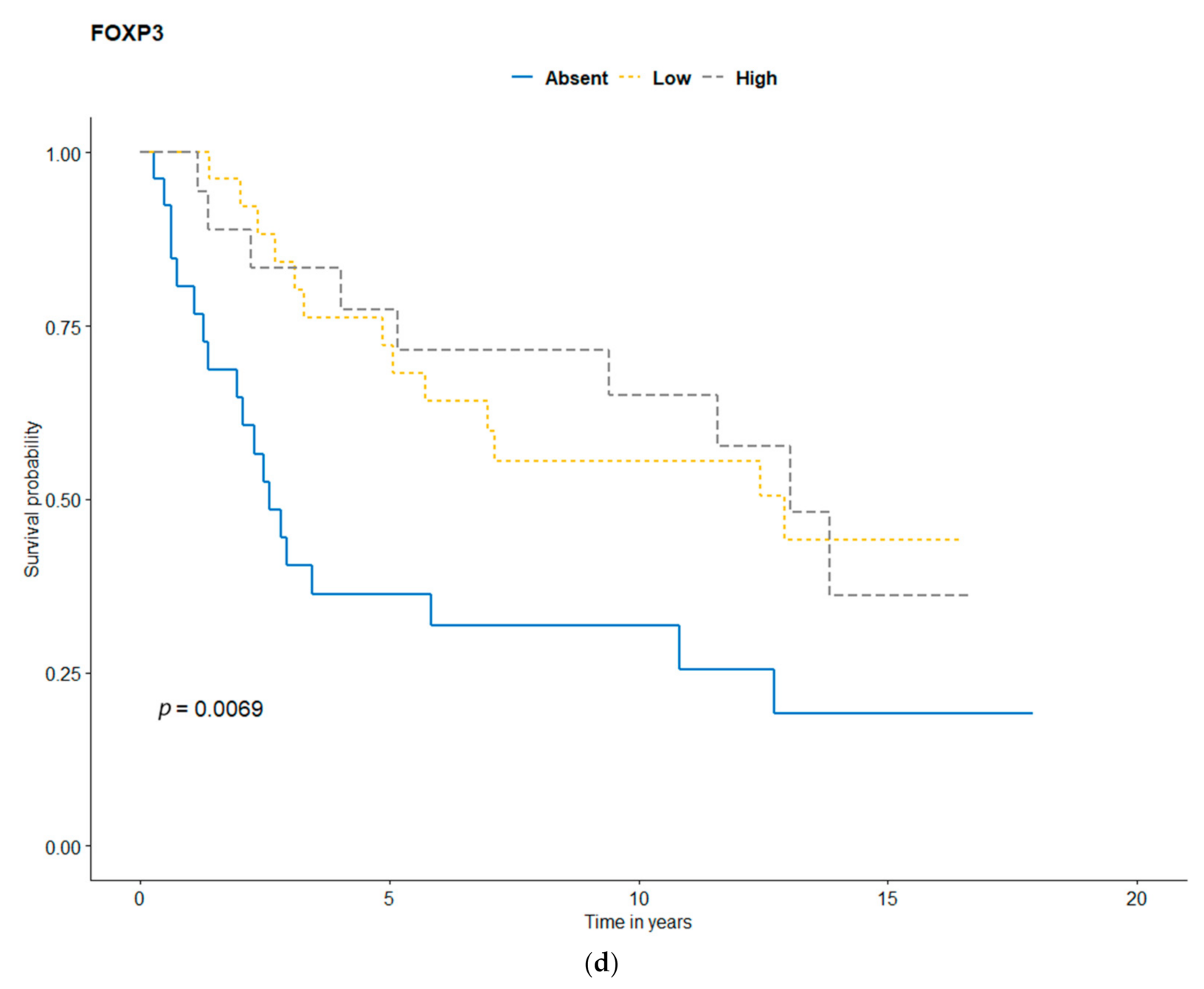
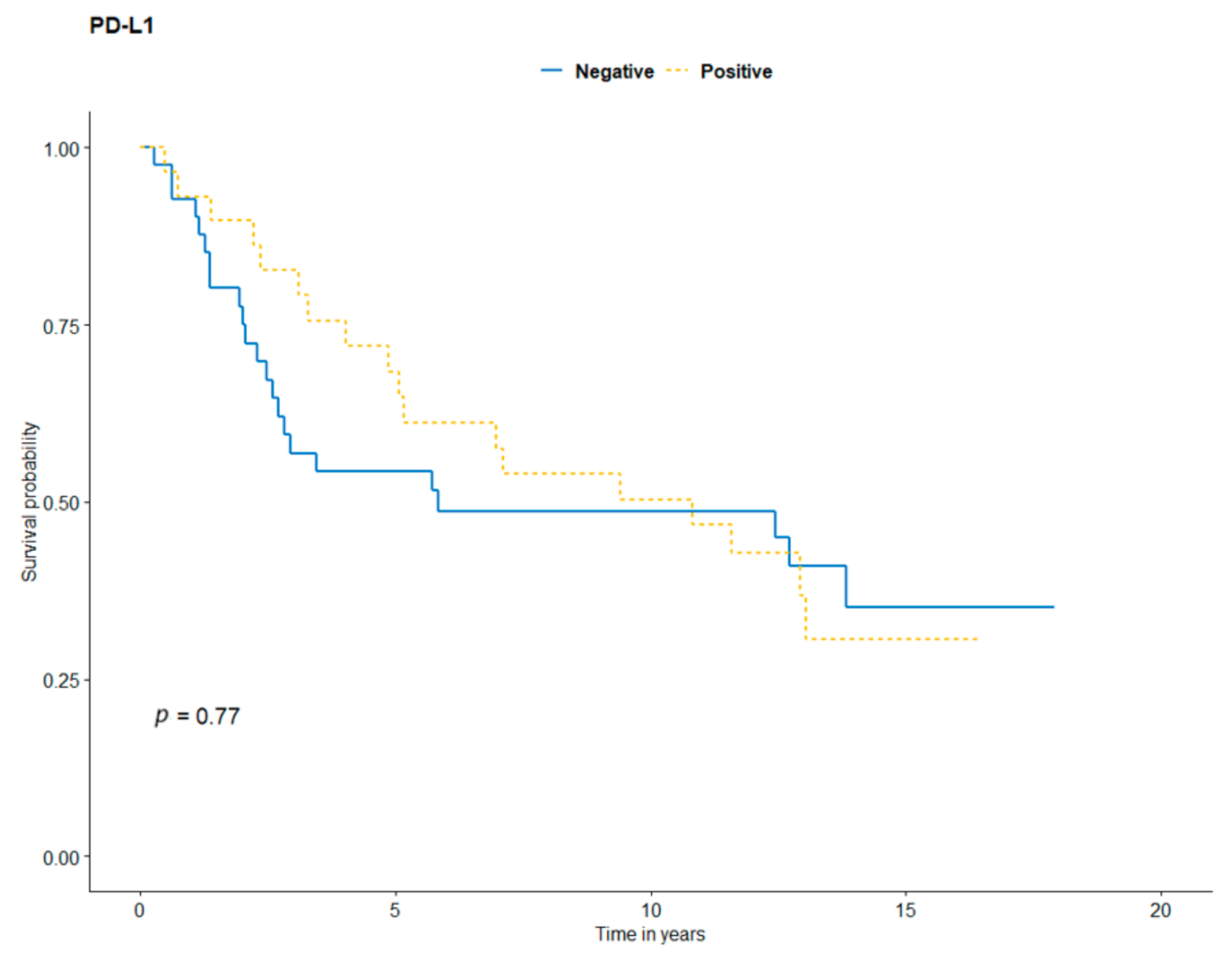
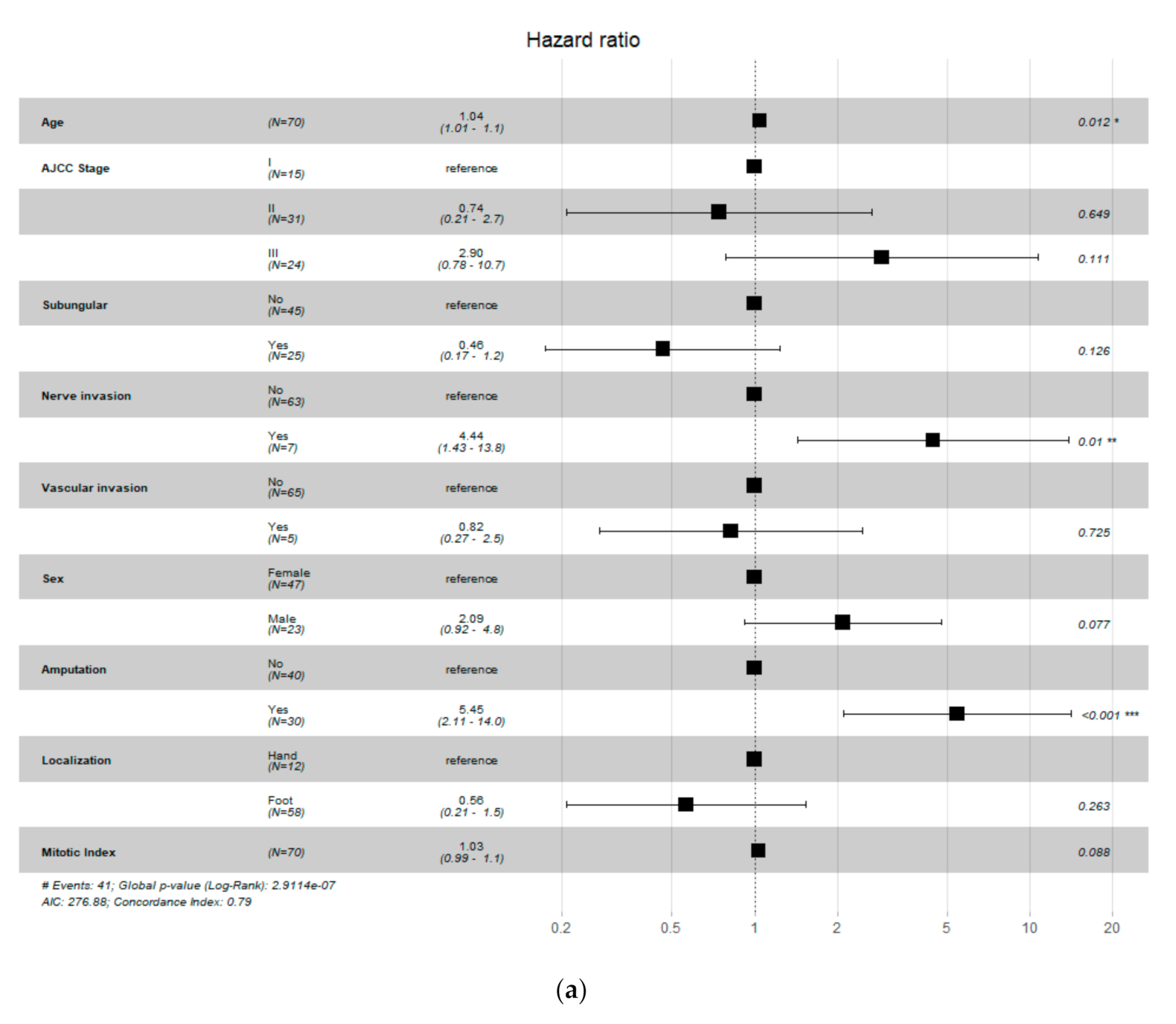
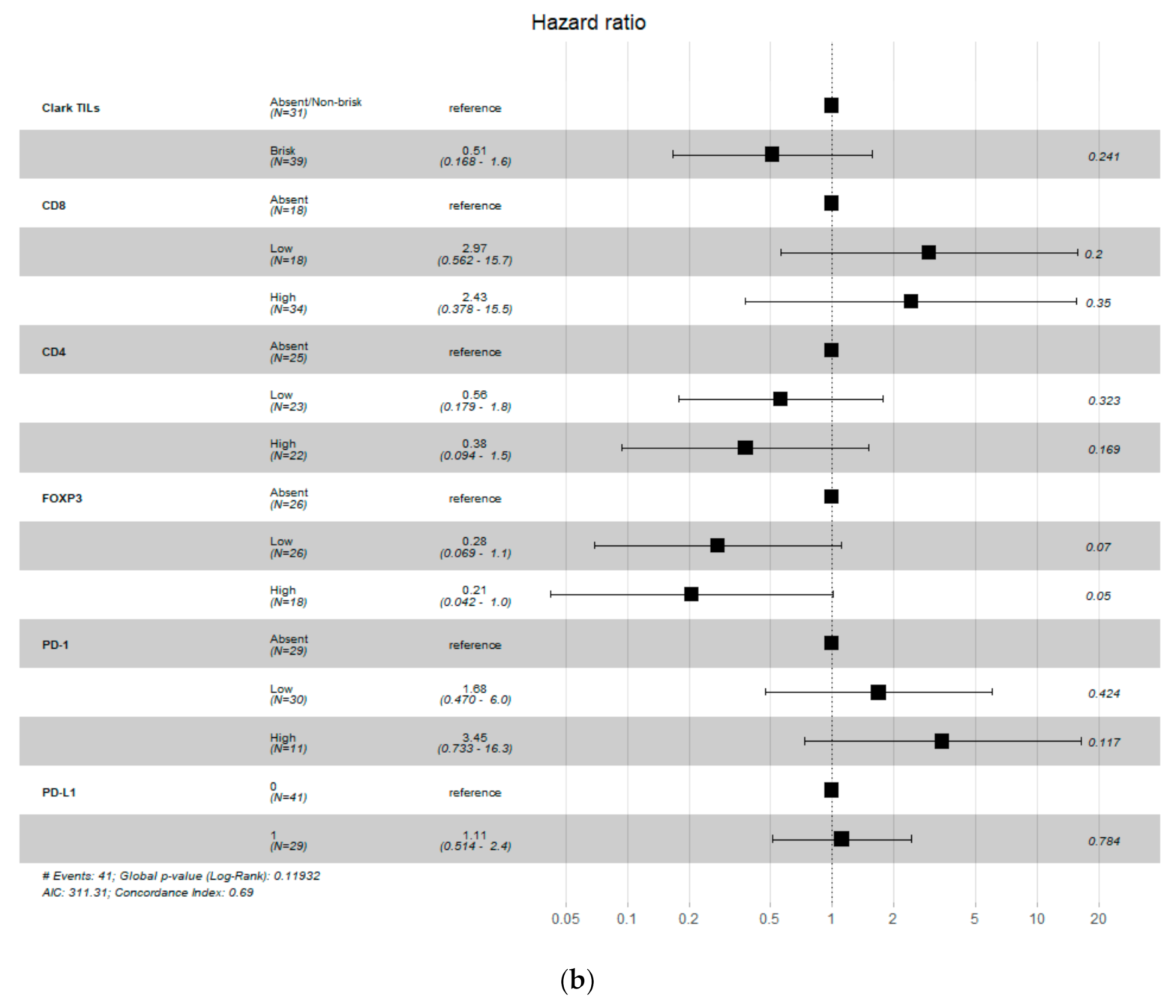
3.3. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mandalà, M.; Massi, D. Tissue prognostic biomarkers in primary cutaneous melanoma. Virchows Archiv. 2014, 464, 265–281. [Google Scholar] [CrossRef] [PubMed]
- Scolyer, R.A.; Rawson, R.V.; Gershenwald, J.E.; Ferguson, P.M.; Prieto, V.G. Melanoma pathology reporting and staging. Mod. Pathol. 2019, 33, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Durbec, F.; Martin, L.; Derancourt, C.; Grange, F. Melanoma of the hand and foot: Epidemiological, prognostic and genetic features. A systematic review. Br. J. Dermatol. 2012, 166, 727–739. [Google Scholar] [CrossRef] [PubMed]
- Fortin, P.T.; Freiberg, A.A.; Rees, R.; Sondak, V.K.; Johnson, T.M. Malignant melanoma of the foot and ankle. J. Bone Jt. Surg. 1995, 77, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Heaton, K.M.; El-Naggar, A.; Ensign, L.G.; Ross, M.I.; Balch, C.M. Surgical Management and Prognostic Factors in Patients with Subungual Melanoma. Ann. Surg. 1994, 219, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maio, M. Melanoma as a model tumour for immuno-oncology. Ann. Oncol. 2012, 23, viii10–viii14. [Google Scholar] [CrossRef]
- Taube, J.M.; Galon, J.; Sholl, L.M.; Rodig, S.J.; Cottrell, T.R.; Giraldo, N.A.; Baras, A.S.; Patel, S.S.; Anders, R.A.; Rimm, D.L.; et al. Implications of the tumor immune microenvironment for staging and therapeutics. Mod. Pathol. 2017, 31, 214–234. [Google Scholar] [CrossRef]
- Gimotty, P.A.; Van Belle, P.; Elder, D.E.; Murry, T.; Montone, K.T.; Xu, X.; Hotz, S.; Raines, S.; Ming, M.E.; Wahl, P.; et al. Biologic and Prognostic Significance of Dermal Ki67 Expression, Mitoses, and Tumorigenicity in Thin Invasive Cutaneous Melanoma. J. Clin. Oncol. 2005, 23, 8048–8056. [Google Scholar] [CrossRef]
- Badalamenti, G.; Fanale, D.; Incorvaia, L.; Barraco, N.; Listì, A.; Maragliano, R.; Vincenzi, B.; Calò, V.; Iovanna, J.L.; Bazan, V.; et al. Role of tumor-infiltrating lymphocytes in patients with solid tumors: Can a drop dig a stone? Cell. Immunol. 2019, 343, 103753. [Google Scholar] [CrossRef]
- Incorvaia, L.; Badalamenti, G.; Rinaldi, G.; Iovanna, J.L.; Olive, D.; Swayden, M.; Terruso, L.; Vincenzi, B.; Fulfaro, F.; Bazan, V.; et al. Can the plasma PD-1 levels predict the presence and efficiency of tumor-infiltrating lymphocytes in patients with metastatic melanoma? Ther. Adv. Med. Oncol. 2019, 11, 175883591984887. [Google Scholar] [CrossRef]
- Barnhill, R.L.; Fine, J.A.; Roush, G.C.; Berwick, M. Predicting five-year outcome for patients with cutaneous melanoma in a population-based study. Cancer 1996, 78, 427–432. [Google Scholar] [CrossRef]
- Taylor, R.C.; Patel, A.; Panageas, K.S.; Busam, K.J.; Brady, M.S. Tumor-Infiltrating Lymphocytes Predict Sentinel Lymph Node Positivity in Patients With Cutaneous Melanoma. J. Clin. Oncol. 2007, 25, 869–875. [Google Scholar] [CrossRef]
- Azimi, F.; Scolyer, R.A.; Rumcheva, P.; Moncrieff, M.; Murali, R.; McCarthy, S.W.; Saw, R.P.; Thompson, J.F. Tumor-Infiltrating Lymphocyte Grade Is an Independent Predictor of Sentinel Lymph Node Status and Survival in Patients with Cutaneous Melanoma. J. Clin. Oncol. 2012, 30, 2678–2683. [Google Scholar] [CrossRef]
- Ros-Martínez, S.; Navas-Carrillo, D.; Alonso-Romero, J.L.; Orenes-Piñero, E. Immunoscore: A novel prognostic tool. Association with clinical outcome, response to treatment and survival in several malignancies. Crit. Rev. Clin. Lab. Sci. 2020, 57, 432–443. [Google Scholar] [CrossRef]
- Massi, D.; Rulli, E.; Cossa, M.; Valeri, B.; Rodolfo, M.; Merelli, B.; De Logu, F.; Nassini, R.; Del Vecchio, M.; Di Guardo, L.; et al. The density and spatial tissue distribution of CD8+ and CD163+ immune cells predict response and outcome in melanoma patients receiving MAPK inhibitors. J. Immuno Ther. Cancer 2019, 7. [Google Scholar] [CrossRef]
- Simoni, Y.; Becht, E.; Fehlings, M.; Loh, C.Y.; Koo, S.-L.; Teng, K.W.W.; Yeong, J.P.S.; Nahar, R.; Zhang, T.; Kared, H.; et al. Bystander CD8 + T cells are abundant and phenotypically distinct in human tumour infiltrates. Nature 2018, 557, 575–579. [Google Scholar] [CrossRef]
- Chauvin, J.-M.; Pagliano, O.; Fourcade, J.; Sun, Z.; Wang, H.; Sander, C.; Kirkwood, J.M.; Chen, T.T.; Maurer, M.; Korman, A.J.; et al. TIGIT and PD-1 impair tumor antigen-specific CD8+ T cells in melanoma patients. J. Clin. Investig. 2015, 125, 2046–2058. [Google Scholar] [CrossRef]
- Han, S.; Toker, A.; Liu, Z.Q.; Ohashi, P.S. Turning the Tide against Regulatory T Cells. Front. Oncol. 2019, 9, 279. [Google Scholar] [CrossRef]
- Ladányi, A.; Mohos, A.; Somlai, B.; Liszkay, G.; Gilde, K.; Fejős, Z.; Gaudi, I.; Tímár, J. FOXP3+ Cell Density in Primary Tumor Has No Prognostic Impact in Patients with Cutaneous Malignant Melanoma. Pathol. Oncol. Res. 2010, 16, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Knol, A.C.; Nguyen, J.M.; Quéreux, G.; Brocard, A.; Khammari, A.; Dréno, B. Prognostic value of tumor-infiltrating Foxp3+ T-cell subpopulations in metastatic melanoma. Exp. Dermatol. 2011, 20, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Lee, Y.J.; Shin, H.J.; Won, C.H.; Chang, S.E.; Choi, J.H.; Lee, M.W. Clinicopathological significance of tumor-infiltrating lymphocytes and programmed death-1 expression in cutaneous melanoma: A comparative study on clinical subtypes. Melanoma Res. 2018, 28, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, C.A.; Castillo, M.; Torres-Cabala, C.; Bernabe, L.A.; Casavilca, S.; Villegas, V.; Sanchez, J.; de la Cruz, M.; Dunstan, J.; Cotrina, J.M.; et al. Relationship between tumor-associated immune infiltrate and p16 staining over clinicopathological features in acral lentiginous melanoma. Clin. Transl. Oncol. 2019, 21, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Lim, H.J.; Choi, Y.H.; Chang, Y.H.; Lee, W.J.; Kim, D.W.; Yoon, G.S. The Clinical Significance of Tumor-Infiltrating Lymphocytes and Microscopic Satellites in Acral Melanoma in a Korean Population. Ann. Dermatol. 2013, 25, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, W.H.; Elder, D.E.; Guerry, D.; Braitman, L.E.; Trock, B.J.; Schultz, D.; Synnestvedt, M.; Halpern, A.C. Model Predicting Survival in Stage I Melanoma Based on Tumor Progression. J. Natl. Cancer Inst. 1989, 81, 1893–1904. [Google Scholar] [CrossRef] [PubMed]
- Gartrell, R.D.; Marks, D.K.; Hart, T.D.; Li, G.; Davari, D.R.; Wu, A.; Blake, Z.; Lu, Y.; Askin, K.N.; Monod, A.; et al. Quantitative Analysis of Immune Infiltrates in Primary Melanoma. Cancer Immunol. Res. 2018, 6, 481–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massi, D.; Romano, E.; Rulli, E.; Merelli, B.; Nassini, R.; De Logu, F.; Bieche, I.; Baroni, G.; Cattaneo, L.; Xue, G.; et al. Baseline β-catenin, programmed death-ligand 1 expression and tumour-infiltrating lymphocytes predict response and poor prognosis in BRAF inhibitor-treated melanoma patients. Eur. J. Cancer 2017, 78, 70–81. [Google Scholar] [CrossRef]
- R Development Core Team. R: The R Project for Statistical Computing. Available online: http://www.r-project.org (accessed on 7 March 2020).
- Saldanha, G.; Flatman, K.; Teo, K.W.; Bamford, M. A Novel Numerical Scoring System for Melanoma Tumor-infiltrating Lymphocytes Has Better Prognostic Value than Standard Scoring. Am. J. Surg. Pathol. 2017, 41, 906–914. [Google Scholar] [CrossRef]
- Ren, M.; Dai, B.; Kong, Y.-Y.; Lv, J.-J.; Cai, X. PD-L1 expression in tumour-infiltrating lymphocytes is a poor prognostic factor for primary acral melanoma patients. Histopathology 2018, 73, 386–396. [Google Scholar] [CrossRef]
- Castaneda, C.; Catillo, M.; Torres-Cabala, C.; Bernabe, L.; Villegas, V.; Sanchez, J.; Dunstan, J.; Calderon, G.; De La Cruez, M.; Cotrina, J.; et al. Characterization of the Tumor-Associated Immune Infiltrate in Acral Lentiginous Melanoma. Austin J. Cancer Clin. Res. 2017, 19, 1478–1488. [Google Scholar]
- Sterlacci, W.; Fiegl, M.; Droeser, R.A.; Tzankov, A. Expression of PD-L1 Identifies a Subgroup of More Aggressive Non-Small Cell Carcinomas of the Lung. Pathobiology 2016, 83, 267–275. [Google Scholar] [CrossRef]
- Eto, S.; Yoshikawa, K.; Nishi, M. Programmed cell death protein 1 expression is an independent prognostic factor in gastric cancer after curative resection. Gastric Cancer 2016, 19, 466–471. [Google Scholar] [CrossRef]
- Cimino-Mathews, A.; Thompson, F.; Taube, I.M. PD-L1 (B7-H1) expression and the immune tumor microenvironment in primary and metastaticbreast carcinomas. Hum. Pathol. 2016, 47, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.R.; Ha, S.; Hong, M. PD-L1 expression on immune cells, but not on tumor cells, is a favorable prognostic factor for head and neck cancer patients. Sci. Rep. 2016, 6, 36956. [Google Scholar] [CrossRef] [Green Version]
- Webb, I.; Milne, K.; Kroeger, D.; Nelson, B. PD-L1 expression is associated with tumor-infiltrating T cells and favorable prognosis in high-grade serous ovarian cancer. Gynecol. Oncol. 2016, 141, 293–302. [Google Scholar] [CrossRef] [Green Version]
- De Logu, F.; Galli, F.; Nassini, R.; Ugolini, F.; Simi, S.; Cossa, M.; Miracco, C.; Gianatti, A.; De Giorgi, V.; Rulli, E.; et al. Digital Immunophenotyping Predicts Disease Free and Overall Survival in Early Stage Melanoma Patients. Cells 2021, 10, 422. [Google Scholar] [CrossRef]
- De Smet, F.; Antoranz Martinez, A.; Bosisio, F.M. Next-Generation Pathology by Multiplexed Immunohistochemistry. Trends Biochem. Sci. 2021, 46, 80–82. [Google Scholar] [CrossRef]
- Sinnamon, A.J.; Sharon, C.E.; Song, Y.; Neuwirth, M.G.; Elder, D.E.; Xu, X.; Chu, E.Y.; Ming, M.E.; Fraker, D.L.; Gimotty, P.A.; et al. The prognostic significance of tumor-infiltrating lymphocytes for primary melanoma varies by sex. J. Am. Acad. Dermatol. 2018, 79, 245–251. [Google Scholar] [CrossRef]
- Fortes, C.; Mastroeni, S.; Caggiati, A.; Passarelli, F.; Ricci, F.; Michelozzi, P. High level of TILs is an independent predictor of negative sentinel lymph node in women but not in men. Arch. Dermatol. Res. 2020, 313, 57–61. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristic | |
|---|---|
| Features | Number (%) |
| Age (median = 64.5; range = 21–79) | |
| Breslow thickness (median = 5; range = 0.1–25) | |
| Mitotic index (median = 8.5 mitoses per 1 mm2; range = 1–41) | |
| Gender | |
| Female | 47 (67) |
| Male | 23 (33) |
| Localization | |
| Hand | 12 (17) |
| Foot | 58 (83) |
| Subungual localization | |
| No | 45 (64) |
| Yes | 25 (36) |
| Amputation | |
| No | 40 (57) |
| Yes | 30 (43) |
| SLN biopsy | |
| Negative | 46 (65) |
| Positive | 24 (35) |
| AJCC Pathologic Stage | |
| I | 15 (21) |
| II | 31 (44) |
| III | 24 (35) |
| Ulceration | |
| No | 18 (26) |
| Yes | 52 (74) |
| pT | |
| pT1 | |
| a | 7 (10) |
| b | 2 (3) |
| pT2 | |
| a | 7 (10) |
| b | 2 (3) |
| pT3 | |
| a | 3 (4) |
| b | 7 (10) |
| pT4 | |
| a | 1 (1) |
| b | 41 (59) |
| Clark scale | |
| 1 | 4 (6) |
| 2 | 5 (7) |
| 3 | 6 (8) |
| 4 | 28 (40) |
| 5 | 27 (39) |
| Vascular Invasion | |
| No | 65 (93) |
| Yes | 5 (7) |
| Nerve Invasion | |
| No | 63 (90) |
| Yes | 7 (10) |
| Tumor-Infiltrating Lymphocytes Characteristics | |
|---|---|
| Feature | Number (%) |
| TILs Clark | |
| Absent | 18 (26) |
| Non-brisk | 39 (56) |
| Brisk | 13 (18) |
| TILs MIA Grade | |
| 0 | 18 (26) |
| 1 | 23 (33) |
| 2 | 17 (24) |
| 3 | 12 (17) |
| TILs MIA Density | |
| Absent | 18 (26) |
| Mild | 30 (43) |
| Moderate | 14 (20) |
| Marked | 8 (11) |
| TILs MIA Distribution | |
| Absent | 18 (26) |
| Focal | 13 (18) |
| Multifocal | 19 (27) |
| Diffuse | 20 (29) |
| CD4 | |
| Absent | 25 (36) |
| Low | 23 (33) |
| High | 22 (31) |
| CD8 | |
| Absent | 18 (26) |
| Low | 18 (26) |
| High | 34 (48) |
| FOXP3 | |
| Absent | 26 (37) |
| Low | 26 (37) |
| High | 18 (26) |
| PD-1 | |
| Absent | 29 (41) |
| Low | 30 (43) |
| High | 11 (16) |
| PD-L1 on melanoma cells | |
| Positive | 41 (59) |
| Negative | 29 (41) |
| TILs Clark | TILs MIA Grade | TILs MIA Density | TILs MIA Distribution | CD8 | CD4 | FOXP3 | PD-1 | PD-L1 | |
|---|---|---|---|---|---|---|---|---|---|
| Ulceration | 0.20 | 0.36 | 0.34 | 0.44 | 0.22 | 0.08 | 0.05 * | 0.50 | 1.00 |
| AJCC Stage | 0.20 | 0.29 | 0.11 | 0.45 | 0.03 * | <0.01 * | 0.62 | 0.33 | 0.21 |
| Gender | 0.98 | 0.40 | 0.77 | 0.83 | 0.77 | 0.46 | 0.33 | 0.45 | 0.62 |
| Localization | 0.22 | 0.14 | 0.38 | 0.55 | 0.08 | 0.12 | 0.15 | 0.83 | 0.34 |
| SLN Status | 0.02 * | 0.01 * | 0.03 * | 0.08 | <0.01 * | 0.03 * | <0.01 * | 0.02 * | 0.73 |
| Subungual | 0.27 | 0.10 | 0.40 | 0.23 | 0.01 * | 0.18 | 0.33 | 0.74 | 0.94 |
| Nerve invasion | 0.55 | 0.61 | 0.70 | 0.50 | 0.30 | 0.30 | 0.30 | 0.96 | 0.63 |
| Vascular Invasion | 0.95 | 0.97 | 0.93 | 0.34 | 0.88 | 0.92 | 0.50 | 0.02 * | 0.18 |
| Feature | Value | Hazard Ratio | CI.95 | p-Value |
|---|---|---|---|---|
| Clark TILs | Absent/Non-brisk | - | ||
| Brisk | 0.58 | 0.31–1.10 | 0.084 | |
| TILs MIA Grade | 0 | - | ||
| 1 | 0.45 | 020–0.99 | 0.046 * | |
| 2 | 0.37 | 0.15–0.92 | 0.033 * | |
| 3 | 0.62 | 0.26–1.45 | 0.271 | |
| TILs MIA Density | Absent | - | ||
| Mild | 0.45 | 0.21–0.95 | 0.036 * | |
| Moderate | 0.32 | 0.12–0.84 | 0.021 * | |
| Marked | 0.83 | 0.33–2.08 | 0.687 | |
| TILs MIA Distribution | Absent | - | ||
| Focal | 0.52 | 0.21–1.31 | 0.167 | |
| Multifocal | 0.33 | 0.14–0.79 | 0.013 * | |
| Diffuse | 0.58 | 0.27–1.25 | 0.161 | |
| CD8 | Absent | - | ||
| Low | 0.62 | 0.28–1.40 | 0.251 | |
| High | 0.4 | 0.19–0.82 | 0.013 * | |
| CD4 | Absent | - | ||
| Low | 0.48 | 0.23–1.00 | 0.048 * | |
| High | 0.39 | 0.18–0.82 | 0.013 * | |
| FOXP3 | Absent | - | ||
| Low | 0.39 | 0.19–0.79 | 0.009 * | |
| High | 0.38 | 0.17–0.83 | 0.016 * | |
| PD-1 | Absent | - | ||
| Low | 0.44 | 0.22–0.89 | 0.022 * | |
| High | 0.89 | 0.39–2.04 | 0.785 | |
| PD-L1 | Absent | - | ||
| Positive | 0.91 | 0.49–1.69 | 0.771 |
| Feature | Value | Hazard Radio | Cl.95 | p-Value |
|---|---|---|---|---|
| Age | Mean (SD) | 1.06 | 1.02–1.09 | 0.001 * |
| AJCC Stage | I | - | ||
| II | 2.76 | 0.91–8.34 | 0.073 | |
| III | 7.98 | 2.70–23.56 | <0.001 * | |
| Ulceration | no | - | ||
| yes | 5.52 | 1.96–15.59 | 0.001 * | |
| Breslow thickness | Mean (SD) | 1.13 | 1.06–1.19 | <0.001 * |
| Subungular | no | - | ||
| yes | 1.64 | 0.87–3.09 | 0.125 | |
| Nerve invasion | no | - | ||
| yes | 3.87 | 1.60–9.36 | 0.003 * | |
| Vascular invasion | no | - | ||
| yes | 1.50 | 0.54–4.30 | 0.43 | |
| Sex | female | |||
| male | 2.29 | 1.22–4.30 | 0.010 * | |
| Amputation | no | |||
| yes | 1.85 | 1.00–3.44 | 0.051 | |
| Localization | hand | |||
| foot | 0.48 | 0.23–1.02 | 0.058 | |
| Mitotic Index | Mean (SD) | 1.05 | 1.02–1.8 | <0.001 * |
| Number of Cases | Clinical Characteristics | Histopathological Characteristics | TILs Characteristics | Prognostic Value of TILs on OS | Reference Number/Year | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (Median) | Population | F:M | Localization | AJCC Stage | Breslow (mm, Median) | Ulceration Present | Positive SLN | TILs Evaluation | Methods | IHC Profile | |||
| 148 | 66 | Peru ** | 1.21 | NA | 0–III | 6.0 | 69% | 54.2% | TILs grade | IHC | CD3, CD8, p16 | p16 p = 0.001 * | Castaneda et al. [23]/2019 |
| 78 | 61.5 | Chinese | 0.63 | Hand (6%) Foot (94%) | I–IV | NA | 45% | 35% | TILs distribution Extent of TILs infiltration (<5% vs. ≥5%) | PDL-1 | PD-L1 expression in TILs p = 0.008 * | Ren et al. [30]/2018 | |
| 90 | 61.3 | Korean | 1.09 | NA | NA | NA | NA | NA | TILs absent, non-brisk, brisk | HE | TILs absent p = 0.037 * | Lee et al. [24]/2013 | |
| 43 | 66.7 | Peru ** | 0.45 | NA | I–III | 5.0 | 74% | 44.2% | TILs density TILs distribution TILs grade | CD3, CD4, CD8, CD20, CD68, CD163 | CD4 p = 0.005 * | Castaneda et al. [31]/2017 | |
| 70 | 64.5 | Caucasian | 2.04 | Hand (17%) Foot (83%) | I–III | 5.0 | 74% | 34% | TILs Clark; TILs MIA Grade; TILs Absent vs. Low/High | HE IHC | CD4, CD8, FOXP3, PD-1, | TILs Clark p = 0.08; TILs MIA Grade p = 0.094; TILs MIA Distribution p = 0.077; TILs MIA Density p = 0.043 *; CD8 p = 0.03 *; CD4 p = 0.02 *; FOXP3 p = 0.006 *; PD-1 p = 0.05 * | Presented study/2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borkowska, A.M.; Szumera-Ciećkiewicz, A.; Chraszczewska, M.; Sokół, K.; Goryń, T.; Rutkowski, P.Ł. Clinical Significance of Tumor Microenvironment in Acral Melanoma: A Large Single-Institution Study of Caucasians. J. Clin. Med. 2021, 10, 1452. https://doi.org/10.3390/jcm10071452
Borkowska AM, Szumera-Ciećkiewicz A, Chraszczewska M, Sokół K, Goryń T, Rutkowski PŁ. Clinical Significance of Tumor Microenvironment in Acral Melanoma: A Large Single-Institution Study of Caucasians. Journal of Clinical Medicine. 2021; 10(7):1452. https://doi.org/10.3390/jcm10071452
Chicago/Turabian StyleBorkowska, Aneta Maria, Anna Szumera-Ciećkiewicz, Maria Chraszczewska, Kamil Sokół, Tomasz Goryń, and Piotr Łukasz Rutkowski. 2021. "Clinical Significance of Tumor Microenvironment in Acral Melanoma: A Large Single-Institution Study of Caucasians" Journal of Clinical Medicine 10, no. 7: 1452. https://doi.org/10.3390/jcm10071452