
Proportion of Thick versus Thin Melanomas as a Benchmarking Tool


Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Osborne, J.E.; Chave, T.A.; Hutchinson, P.E. Comparison of diagnostic accuracy for cutaneous malignant melanoma between general dermatology, plastic surgery and pigmented lesion clinics. Br. J. Dermatol. 2003, 148, 252–258. [Google Scholar] [CrossRef] [PubMed]
- English, D.R.; Del Mar, C.; Burton, R.C. Factors influencing the number needed to excise: Excision rates of pigmented lesions by general practitioners. Med. J. Aust. 2004, 180, 16–19. [Google Scholar] [CrossRef]
- Wilkinson, D.; Askew, D.A.; Dixon, A. Skin cancer clinics in Australia: Workload profile and performance indicators from an analysis of billing data. Med. J. Aust. 2006, 184, 162–164. [Google Scholar] [CrossRef]
- Hansen, C.; Wilkinson, D.; Hansen, M.; Argenziano, G. How good are skin cancer clinics at melanoma detection? Number needed to treat variability across a national clinic group in Australia. J. Am. Acad. Dermatol. 2009, 61, 599–604. [Google Scholar] [CrossRef]
- Sidhu, S.; Bodger, O.; Williams, N.; Roberts, D.L. The number of benign moles excised for each malignant melanoma: The number needed to treat. Clin. Exp. Dermatol. 2012, 37, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl, C.; Williams, G.; Eley, D.; Wilson, T.; Canning, G.; Keir, J.; McColl, I.; Wilkinson, D. The impact of subspecialization and dermatoscopy use on accuracy of melanoma diagnosis among primary care doctors in Australia. J. Am. Acad. Dermatol. 2012, 67, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Argenziano, G.; Cerroni, L.; Zalaudek, I.; Staibano, S.; Hofmann-Wellenhof, R.; Arpaia, N.; Bakos, R.M.; Balme, B.; Bandic, J.; Bandelloni, R.; et al. Accuracy in melanoma detection: A 10-year multicenter survey. J. Am. Acad. Dermatol. 2012, 67, 54–59. [Google Scholar] [CrossRef]
- Carli, P.; De Giorgi, V.; Crocetti, E.; Mannone, F.; Massi, D.; Chiarugi, A.; Giannotti, B. Improvement of malignant/benign ratio in excised melanocytic lesions in the ‘dermoscopy era’: A retrospective study 1997–2001. Br. J. Dermatol. 2004, 150, 687–692. [Google Scholar] [CrossRef]
- Tromme, I.; Sacré, L.; Hammouch, F.; Legrand, C.; Marot, L.; Vereecken, P.; Theate, I.; van Eeckhout, P.; Richez, P.; Baurain, J.; et al. Availability of digital dermoscopy in daily practice dramatically reduces the number of excised melanocytic lesions: Results from an observational study. Br. J. Dermatol. 2012, 167, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Ahnlide, I.; Nielsen, K.; Bjellerup, M. Diagnosis of pigmented skin tumours in a dermatological setting: Different aspects of the number needed to excise as a measure of efficiency. Acta Derm. Venereol. 2014, 94, 683–686. [Google Scholar] [CrossRef] [Green Version]
- Alarcon, I.; Carrera, C.; Palou, J.; Alos, L.; Malvehy, J.; Puig, S. Impact of in vivo reflectance confocal microscopy on the number needed to treat melanoma in doubtful lesions. Br. J. Dermatol. 2014, 170, 802–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellacani, G.; Pepe, P.; Casari, A.; Longo, C. Reflectance confocal microscopy as a second-level examination in skin oncology improves diagnostic accuracy and saves unnecessary excisions: A longitudinal prospective study. Br. J. Dermatol. 2014, 171, 1044–1051. [Google Scholar] [CrossRef]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final Version of 2009 AJCC Melanoma Staging and Classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Menchón, T.; Sánchez-Pedreño, P.; Martínez-Escribano, J.; Corbalán-Vélez, R.; Martínez-Barba, E. Cost analysis of sentinel lymph node biopsy in melanoma. Actas Dermosifiliogr. 2015, 106, 201–207. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology: Melanoma. 2013. Available online: http://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf (accessed on 5 June 2017).
- Dummer, R.; Guggenheim, M.; Arnold, A.W.; Braun, R.; von Moos, R. Task Force Skin Cancer. Updated Swiss guidelines for the treatment and follow-up of cutaneous melanoma. Swiss. Med. Wkly. 2011, 141, w13320. [Google Scholar]
- Garbe, C.; Hauschild, A.; Volkenandt, M.; Schadendorf, D.; Stolz, W.; Reinhold, U.; Kortmann, R.-D.; Kettelhack, C.; Frerich, B.; Keilholz, U.; et al. Evidence and interdisciplinary consense-based German guidelines: Diagnosis and surveillance of melanoma. Melanoma Res. 2007, 17, 393–399. [Google Scholar] [CrossRef]
- Pehamberger, H.; Binder, M.; Knollmayer, S.; Wolff, K. Immediate effects of a public education campaign on prognostic features of melanoma. J. Am. Acad. Dermatol 1993, 29, 106–109. [Google Scholar] [CrossRef]
- Beam, C.A.; Conant, E.F.; Sickles, E.A. Correlation of radiologist rank as a measure of skill in screening and diagnostic interpretation of mammograms. Radiology 2006, 238, 446–453. [Google Scholar] [CrossRef]
- Esdaile, B.; Mahmud, I.; Palmer, A.; Bowling, J. Diagnosing melanoma: How do we assess how good we are? Clin. Exp. Dermatol. 2014, 39, 129–134. [Google Scholar] [CrossRef]
- Betti, R.; Moneghini, L.; Vergani, R.; Cerri, A. Diagnostic performance parameters for melanocytic lesions before and during the dermoscopy era. Eur. J. Dermatol. 2017, 27, 174–175. [Google Scholar] [CrossRef]
- Aires, D.J.; Wick, J.; Shaath, T.S.; Rajpara, A.N.; Patel, V.; Badawi, A.H.; Li, C.; Fraga, G.R.; Doolittle, G.; Liu, D.Y. Economic costs avoided by diagnosing melanoma six months earlier justify >100 benign biopsies. J. Drugs Dermatol. 2016, 15, 527–532. [Google Scholar] [PubMed]
- Pagliarello, C.; Stanganelli, I.; Fabrizi, G.; Feliciani, C.; Nuzzo, S. Digital dermoscopy monitoring: Is it time to define a quality standard? Acta Derm. Venereol. 2017, 97, 864–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buist, D.S.; Anderson, M.L.; Smith, R.A.; Carney, P.A.; Miglioretti, D.L.; Monsees, B.S.; Sickles, E.A.; Taplin, S.H.; Geller, B.M.; Yankaskas, B.C.; et al. Effect of radiologists’ diagnostic work-up volume on interpretive performance. Radiology 2014, 273, 351–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| IRST | Parma | p | |
|---|---|---|---|
| OVERALL EXCISED LESION | 1604 | 15,134 | |
| EXCISED NEVI | 1308 | 13,828 | |
| Age (mean ± SD) | 38.57 ± 13.77 | 36.97 ± 15.6 | <0.001 |
| Gender (%) | |||
| Male | 553 (42%) | 5633 (41%) | NS |
| Female | 755 (58%) | 8195 (59%) | |
| Location (%) | |||
| Head and neck | 110 (8.5%) | 2080 (16.5%) | <0.001 |
| Trunk | 846 (65.5%) | 7029 (55%) | |
| Arms | 90 (7%) | 1177 (9.5%) | |
| Legs | 212 (16.5%) | 1400 (11%) | |
| Acral | 34 (2.5%) | 1033 (8%) | |
| EXCISED MELANOMA | 296 | 1306 | |
| Gender (%) | |||
| Male | 139 (47%) | 592 (45%) | NS |
| Female | 157 (53%) | 714 (55%) | |
| Mean age ± SD | 53.8 ± 18 | 56.3 ± 18 | <0.05 |
| Mean Breslow ± SD | 0.56 ± 0.89 | 1.07 ± 2.2 | NS |
| Median Breslow (range) | 0.4 (9) | 0.4 (30) | NS |
| Melanoma type (%) | <0.001 | ||
| In situ | 94 (31.8%) | 510 (39.1%) | |
| Breslow ≤ 1 mm | 166 (56.1%) | 482 (36.9%) | |
| Breslow >1 mm | 36 (12.2%) | 314 (24%) | |
| Thin melanoma (%) | 260 (87.8%) | 992 (76%) | <0.001 |
| Thick melanoma (%) | 36 (12.2%) | 314 (24%) | |
| Gender (%) | |||
| Male | |||
| Thin melanoma | 124 (89.2%) | 421 (71.1%) * | |
| Thick melanoma | 15 (10.8%) | 171 (28.9%) * | |
| Female | |||
| Thin melanoma | 136 (86.6%) | 571 (80%) * | |
| Thick melanoma | 21 (13.4%) | 143 (20%) * | |
| Location (%) | <0.001 | ||
| Head and neck | 29 (10%) | 220 (18%) | |
| Trunk | 156 (53%) | 458 (38%) | |
| Arms | 41 (14%) | 171 (14%) | |
| Legs | 64 (22%) | 280 (23%) | |
| Acral | 3 (1%) | 90 (7%) | |
| Head and neck (%) | NS | ||
| Thin melanoma | 26 (89.7%) | 178 (80.9%) | |
| Thick melanoma | 3 (10.3%) | 42 (19.1%) | |
| Trunk (%) | NS | ||
| Thin melanoma | 136 (87.2%) | 368 (80.3%) | |
| Thick melanoma | 20 (12.8%) | 90 (19.7%) | |
| Arms (%) | <0.01 | ||
| Thin melanoma | 38 (92.7%) | 125 (73.1%) | |
| Thick melanoma | 3 (7.3%) | 46 (26.9%) | |
| Legs (%) | NS | ||
| Thin melanoma | 55 (85.9%) | 218 (77.9%) | |
| Thick melanoma | 9 (14.1%) | 62 (22.1%) | |
| Acral (%) | NS | ||
| Thin melanoma | 3 (100%) | 43 (47.8%) | |
| Thick melanoma | 0 (0%) | 47 (52.2%) | |
| OVERALL NNE | 4.42 | 10.6 | |
| Male NNE | 3.98 | 9.52 | |
| Female NNE | 4.81 | 11.48 | |
| Head and neck NNE | 3.79 | 9.45 | |
| Trunk NNE | 5.42 | 15.35 | |
| Arms NNE | 2.19 | 6.88 | |
| Legs NNE | 3.31 | 5 | |
| Acral NNE | 11.33 | 11.47 |
| Thick vs. Thin | Thick vs. Thin | |||||
|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | |||||
| OR | 95% CI | p | OR | 95% CI | p | |
| Centre | ||||||
| IRST | 1 | – | <0.001 | 1 | – | <0.01 |
| Parma | 2.3 | 1.6–3.3 | 1.8 | 1.2–2.7 | ||
| Gender | ||||||
| Female | 1 | – | <0.001 | 1 | – | <0.01 |
| Male | 1.5 | 1.1–1.9 | 1.5 | 1.2–2 | ||
| Location | ||||||
| Head and neck | 1 | – | <0.001 | 1 | – | <0.001 |
| Trunk | 0.9 | 0.7–1.4 | 1.5 | 0.9–2.2 | ||
| Arms | 1.4 | 0.9–2.1 | 1.8 | 1.1–2.9 | ||
| Legs | 1.2 | 0.8–18 | 2 | 1.2–3 | ||
| Acral | 4.6 | 2.7–7.8 | 5.6 | 3.3–9.6 | ||
| Age (for each ten-year increase) | 1.2 | 1.2-1.3 | <0.001 | 1.2 | 1.1–1.3 | <0.001 |
| RCM | <0.01 | NS | ||||
| No | 3.4 | 1.3–8.5 | 1.9 | 0.7–5.2 | ||
| Yes | – | – | – | – | ||
| 0–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80–89 | 90–99 | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| EXCISED NEVI | |||||||||||
| IRST (%) | 14 (1.1) | 82 (6.3) | 213 (16.3) | 438 (33.6) | 319 (24.5) | 125 (9.6) | 72 (5.5) | 34 (2.6) | 7 (0.5) | 0 (0) | <0.001 |
| Parma (%) | 218 (1.6) | 1622 (11.8) | 2679 (19.4) | 3916 (28.4) | 2647 (19.2) | 1361 (9.9) | 890 (6.5) | 355 (2.6) | 84 (0.6) | 10 (0.1) | |
| EXCISED MELANOMA | |||||||||||
| Overall | |||||||||||
| IRST (%) | 0 (0) | 1 (0.3) | 27 (9.2) | 54 (18.3) | 56 (19) | 41 (13.9) | 37 (12.5) | 57 (19.3) | 21 (7.1) | 1 (0.3) | <0.05 |
| Parma (%) | 0 (0) | 11 (0.8) | 71 (5.4) | 207 (15.8) | 218 (16.7) | 210 (16.1) | 217 (16.6) | 222 (17) | 132 (10.1) | 18 (1.4) | |
| Thin | |||||||||||
| IRST (%) | 0 (0) | 1 (0.4) | 25 (9.7) | 46 (17.8) | 51 (19.7) | 36 (13.9) | 34 (13.1) | 49 (18.9) | 16 (6.2) | 1 (0.4) | NS |
| Parma (%) | 0 (0) | 8 (0.8) | 63 (6.4) | 182 (18.3) | 169 (17) | 160 (16.1) | 166 (16.7) | 152 (15.3) | 88 (8.9) | 4 (0.4) | |
| Thick | |||||||||||
| IRST (%) | 0 (0) | 0 (0) | 2 (5.6) | 8 (22.2) | 5 (13.9) | 5 (13.9) | 3 (8.3) | 8 (22.2) | 5 (13.9) | 0 (0) | NS |
| Parma (%) | 0 (0) | 3 (1) | 8 (2.5) | 25 (8) | 49 (15.6) | 50 (15.9) | 51 (16.2) | 70 (22.3) | 44 (14) | 14 (4.5) | |
| NNE IRST | NA | 82 | 7.9 | 8.1 | 5.7 | 3 | 1.9 | 0.6 | 0.3 | NA | <0.001 |
| Thick/thin (TTR) IRST | n/a | n/a | 0.08 | 0.17 | 0.10 | 0.14 | 0.09 | 0.16 | 0.31 | n/a | NS |
| NNE Parma | NA | 147 | 37.7 | 18.9 | 12.1 | 6.5 | 4.1 | 0.6 | 0.6 | 0.55 | <0.001 |
| Thick/Thin (TTR) Parma | n/a | 0.37 | 0.13 | 0.14 | 0.29 | 0.31 | 0.30 | 0.45 | 0.50 | 3.33 | <0.001 |
| Excised melanoma IRST | |||||||||||
| Thin (%) | 0 (0) | 1 (0.4) | 25 (9.7) | 46 (17.8) | 51 (19.7) | 36 (13.9) | 34 (13.1) | 49 (18.9) | 16 (6.2) | 1 (0.4) | NS |
| Thick (%) | 0 (0) | 0 (0) | 2 (5.6) | 8 (22.2) | 5 (13.9) | 5 (13.9) | 3 (8.3) | 8 (22.2) | 5 (13.9) | 0 (0) | |
| Excised melanoma Parma | |||||||||||
| Thin (%) | 0 | 8 (0.8) | 63 (6.4) | 182 (18.3) | 169 (17) | 160 (16.1) | 166 (16.7) | 152 (15.3) | 88 (8.9) | 4 (0.4) | <0.001 |
| Thick (%) | 0 | 3 (1) | 8 (2.5) | 25 (8) | 49 (15.6) | 50 (15.9) | 51 (16.2) | 70 (22.3) | 44 (14) | 14 (4.5) |
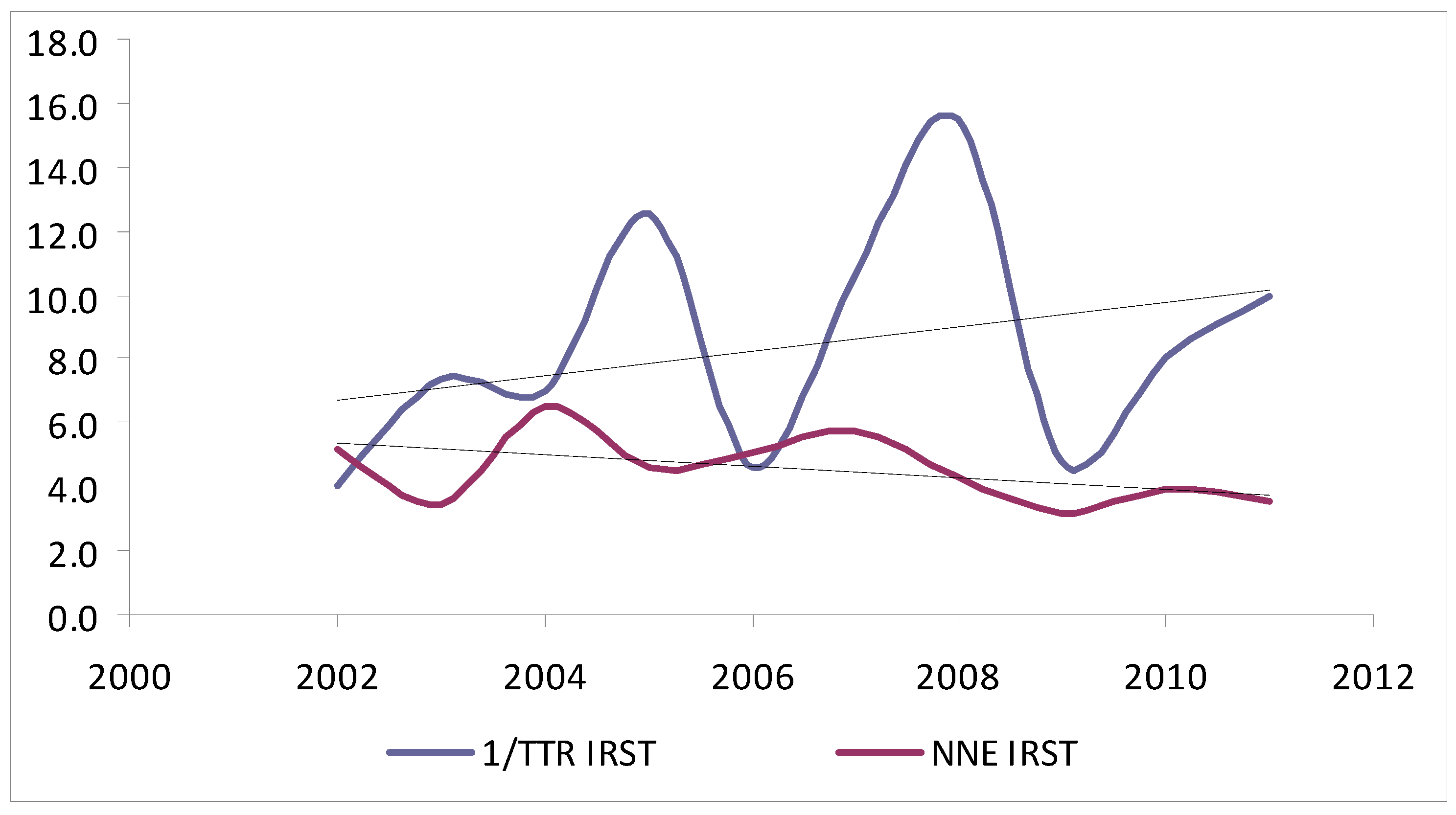
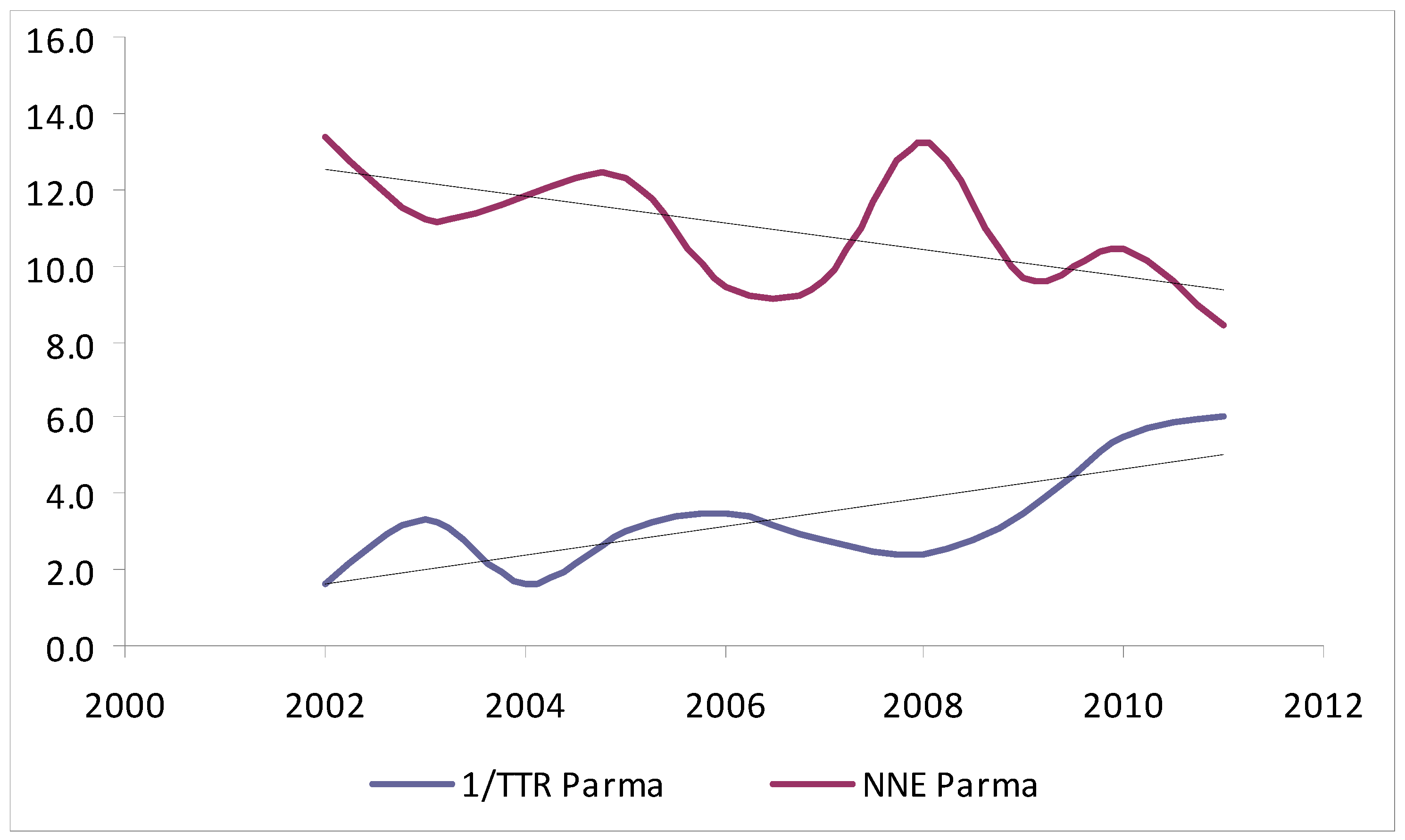
| 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| EXCISED NEVI | |||||||||||
| IRST (%) | 157 (12) | 142 (10.9) | 157 (12) | 124 (9.5) | 144 (11) | 131 (10) | 141 (10.8) | 92 (7) | 105 (8) | 115 (8.8) | <0.001 |
| Parma (%) | 765 (5.5) | 1018 (7.4) | 1235 (8.9) | 1637 (11.8) | 1415 (10.2) | 1482 (10.7) | 1589 (11.5) | 1537 (11.1) | 1553 (11.2) | 1597 (11.5) | |
| EXCISED MELANOMA | |||||||||||
| Overall | |||||||||||
| IRST (%) | 30 (0) | 42 (0.3) | 24 (9.2) | 27 (18.3) | 28 (19) | 23 (13.9) | 33 (12.5) | 29 (19.3) | 27 (7.1) | 33 (0.3) | <0.001 |
| Parma (%) | 57 (4.4) | 91 (7) | 105 (8) | 133 (10.2) | 150 (11.5) | 154 (11.8) | 120 (9.2) | 158 (12.1) | 149 (11.4) | 189 (14.5) | |
| Thin | |||||||||||
| IRST (%) | 24 (9.2) | 37 (14.2) | 21 (8.1) | 25 (9.6) | 23 (8.8) | 21 (8.1) | 31 (11.9) | 24 (9.2) | 24 (9.2) | 30 (11.5) | <0.001 |
| Parma (%) | 35 (3.5) | 70 (7.1) | 64 (6.5) | 100 (10.1) | 117 (11.8) | 113 (11.4) | 85 (8.6) | 120 (12.1) | 126 (12.7) | 162 (16.3) | |
| Thick | |||||||||||
| IRST (%) | 6 (16.7) | 5 (13.9) | 3 (8.3) | 2 (5.6) | 5 (13.9) | 2 (5.6) | 2 (5.6) | 5 (13.9) | 3 (8.3) | 3 (8.3) | NS |
| Parma (%) | 22 (7) | 21 (6.7) | 41 (13.1) | 33 (10.5) | 33 (10.5) | 41 (13.1) | 35 (11.1) | 38 (12.1) | 23 (7.3) | 27 (8.6) | |
| NNE IRST | 5.2 | 3.4 | 6.5 | 4.6 | 5.1 | 5.7 | 4.3 | 3.2 | 3.9 | 3.5 | NS |
| TTR IRST | 0.25 | 0.14 | 0.14 | 0.08 | 0.22 | 0.09 | 0.06 | 0.21 | 0.12 | 0.10 | NS |
| NNE Parma | 13.4 | 11.2 | 11.8 | 12.3 | 9.4 | 9.6 | 13.2 | 9.7 | 10.4 | 8.4 | <0.01 |
| TTR Parma | 0.62 | 0.30 | 0.62 | 0.33 | 0.29 | 0.36 | 0.42 | 0.31 | 0.18 | 0.17 | <0.01 |
| Excised melanoma IRST | |||||||||||
| Thin | 24 (9.2) | 37 (14.2) | 21 (8.1) | 25 (9.6) | 23 (8.8) | 21 (8.1) | 31 (11.9) | 24 (9.2) | 24 (9.2) | 30 (11.5) | NS |
| Thick | 6 (16.7) | 5 (13.9) | 3 (8.3) | 2 (5.6) | 5 (13.9) | 2 (5.6) | 2 (5.6) | 5 (13.9) | 3 (8.3) | 3 (8.3) | |
| Excised melanoma Parma | |||||||||||
| Thin | 35 (3.5) | 70 (7.1) | 64 (6.5) | 100 (10.1) | 117 (11.8) | 113 (11.4) | 85 (8.6) | 120 (12.1) | 126 (12.7) | 162 (16.3) | <0.001 |
| Thick | 22 (7) | 21 (6.7) | 41 (13.1) | 33 (10.5) | 33 (10.5) | 41 (13.1) | 35 (11.1) | 38 (12.1) | 23 (7.3) | 27 (8.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagliarello, C.; Magi, S.; Mazzoni, L.; Stanganelli, I. Proportion of Thick versus Thin Melanomas as a Benchmarking Tool. J. Clin. Med. 2021, 10, 5545. https://doi.org/10.3390/jcm10235545
Pagliarello C, Magi S, Mazzoni L, Stanganelli I. Proportion of Thick versus Thin Melanomas as a Benchmarking Tool. Journal of Clinical Medicine. 2021; 10(23):5545. https://doi.org/10.3390/jcm10235545
Chicago/Turabian StylePagliarello, Calogero, Serena Magi, Laura Mazzoni, and Ignazio Stanganelli. 2021. "Proportion of Thick versus Thin Melanomas as a Benchmarking Tool" Journal of Clinical Medicine 10, no. 23: 5545. https://doi.org/10.3390/jcm10235545