
Interaction between Subjective Memory Decline and Depression Symptom Intensity in Older People. Results of the Second Wave of Cognition of Older People, Education, Recreational Activities, Nutrition, Comorbidities, and Functional Capacity Studies (COPERNICUS)

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
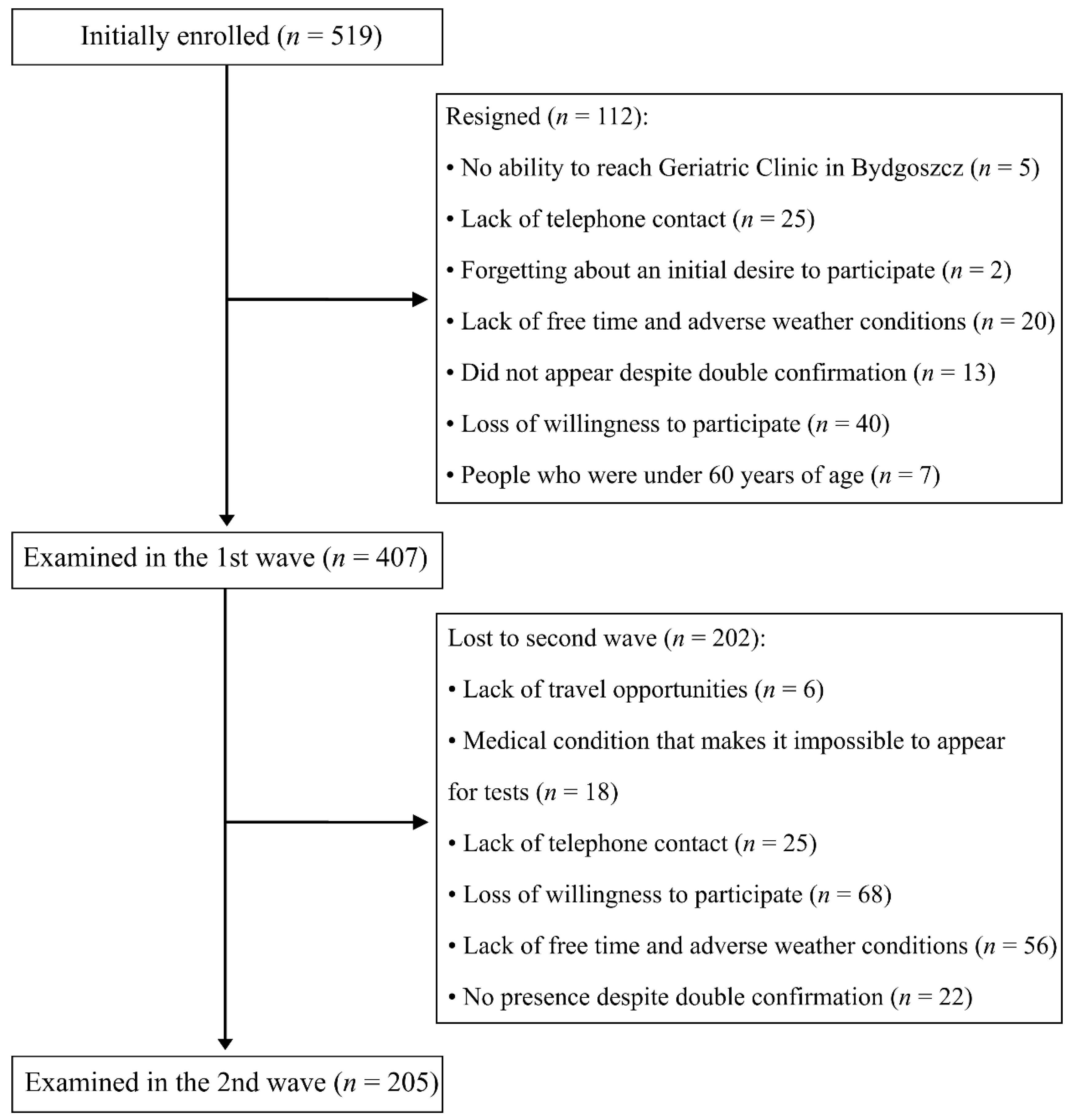
2.1. Enrolment
2.2. Measurement
2.2.1. Subjective Questionnaire
2.2.2. Cognitive Tests
2.2.3. Emotional State Assessment
2.2.4. Functional Performance Assessment
2.2.5. Activity Level Assessment
2.3. Statistical Analysis
3. Results
3.1. Baseline Data from Those Participating in the Follow-Up Compared to Those Not Participating
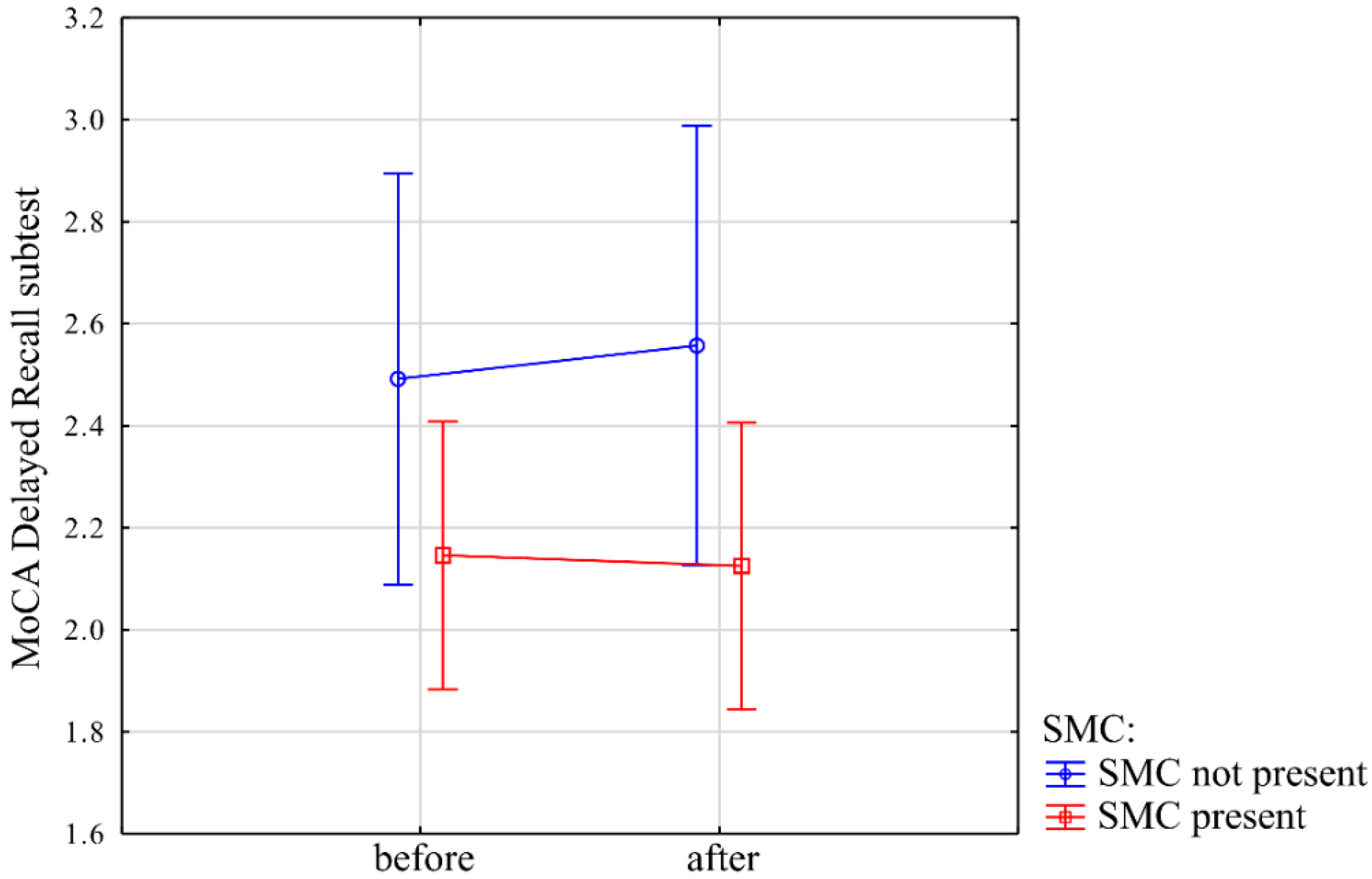
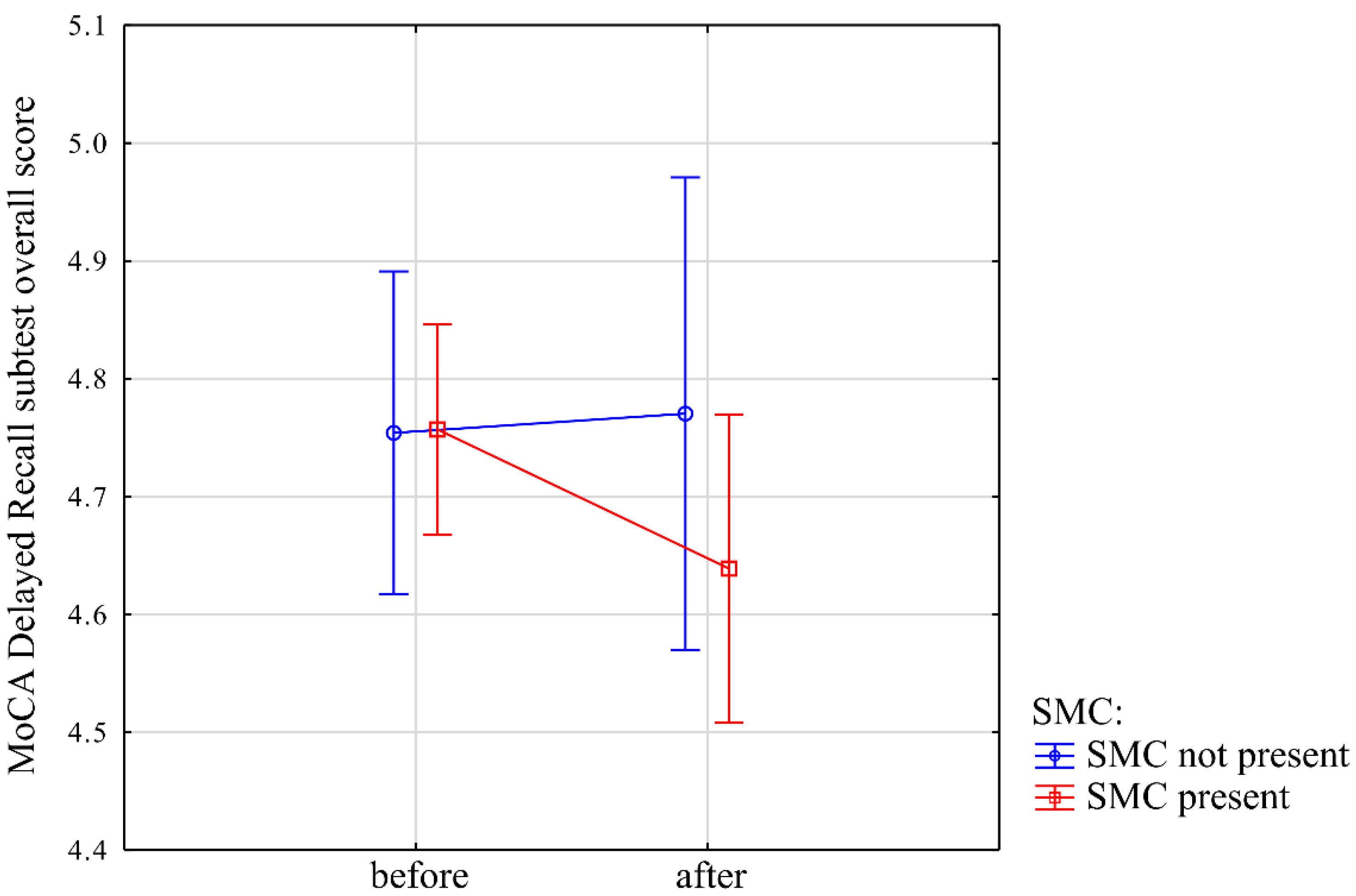
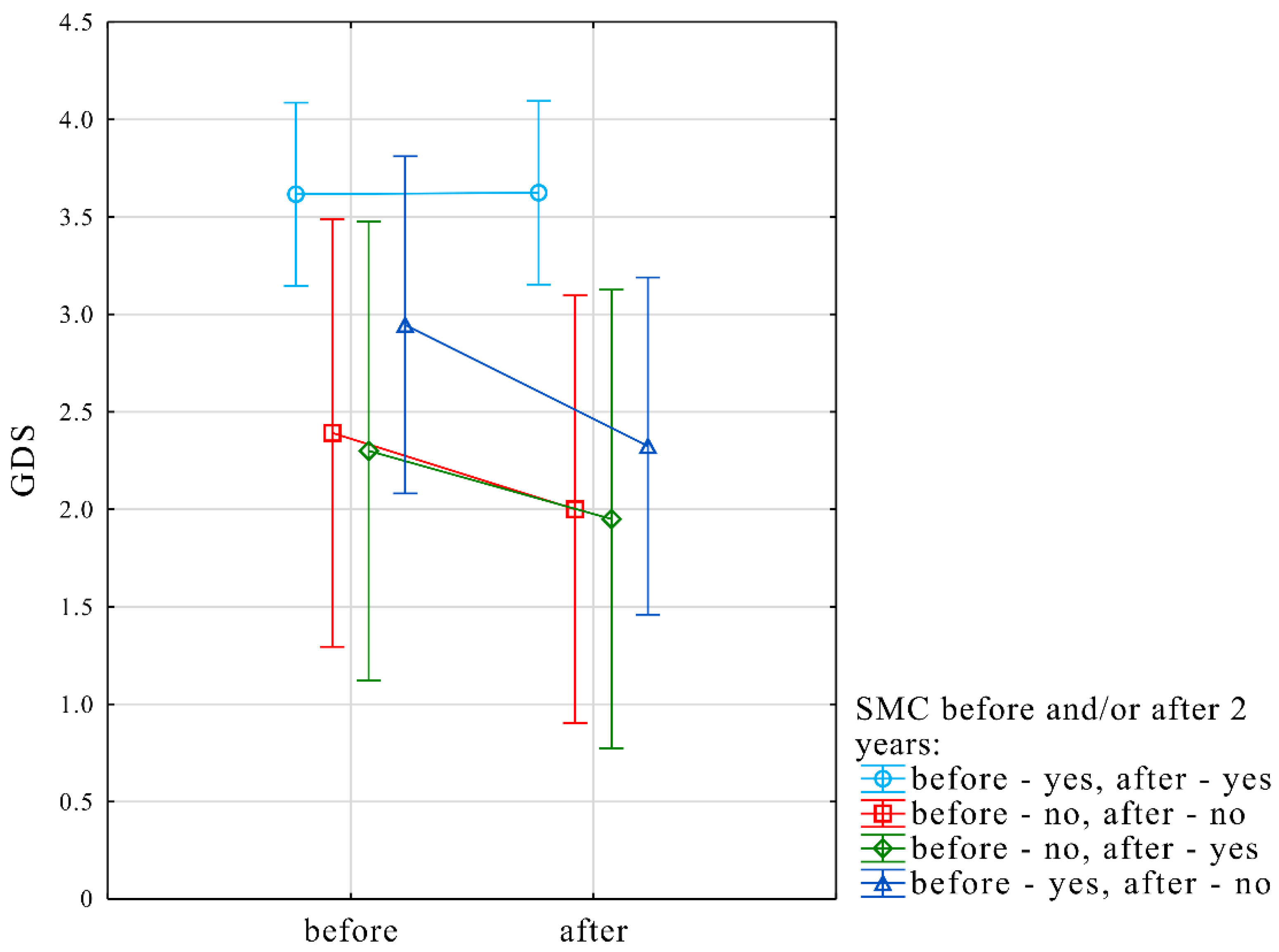
3.2. Comparison of Measures in the Cohort with Baseline and Follow-Up Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment–beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Portet, F.; Ousset, P.J.; Visser, P.J.; Frisoni, G.B.; Nobili, F.; Scheltens, P.; Vellas, B.; Touchon, J. MCI Working Group of the European Consortium on Alzheimer’s Disease (EADC). Mild cognitive impairment (MCI) in medical practice: A critical review of the concept and new diagnostic procedure. Report of the MCI Working Group of the European Consortium on Alzheimer’s Disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 714–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crumley, J.J.; Stetler, C.A.; Horhota, M. Examining the relationship between subjective and objective memory performance in older adults: A meta-analysis. Psychol. Aging 2014, 29, 250. [Google Scholar] [CrossRef] [PubMed]
- Mogle, J.; Hill, N.L.; Bhargava, S.; Bell, T.R.; Bhang, I. Memory complaints and depressive symptoms over time: A construct-level replication analysis. BMC Geriatr. 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heun, R.; Hein, S. Risk factors of major depression in the elderly. Eur. Psychiatry 2005, 20, 199–204. [Google Scholar] [CrossRef]
- Potvin, O.; Bergua, V.; Swendsen, J.; Meillon, C.; Tzourio, C.; Ritchie, K.; Dartigues, J.F.; Amieva, H. Anxiety and 10-year risk of incident and recurrent depressive symptomatology in older adults. Depress. Anxiety 2013, 30, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Dugravot, A.; Ankri, J.; Nabi, H.; Berr, C.; Goldberg, M.; Zins, M.; Kivimaki, M.; Elbaz, A. Subjective cognitive complaints and mortality: Does the type of complaint matter? J. Psychiatr. Res. 2014, 48, 73–78. [Google Scholar] [CrossRef]
- Brailean, A.; Steptoe, A.; Batty, G.D.; Zaninotto, P.; Llewellyn, D.J. Are subjective memory complaints indicative of objective cognitive decline or depressive symptoms? Findings from the English Longitudinal Study of Ageing. J. Psychiatr. Res. 2019, 110, 143–151. [Google Scholar] [CrossRef]
- Lehrner, J.; Moser, D.; Klug, S.; Gleiß, A.; Auff, E.; Dal-Bianco, P.; Pusswald, G. Subjective memory complaints, depressive symptoms and cognition in patients attending a memory outpatient clinic. Int. Psychogeriatr. 2014, 26, 463–473. [Google Scholar] [CrossRef] [Green Version]
- Brigola, A.G.; Manzini, C.S.S.; Oliveira, G.B.S.; Ottaviani, A.C.; Sako, M.P.; Vale, F.A.C. Subjective memory complaints associated with depression and cognitive impairment in the elderly: A systematic review. Dement. Neuropsychol. 2015, 9, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Kujawski, S.; Kujawska, A.; Gajos, M.; Topka, W.; Perkowski, R.; Androsiuk-Perkowska, J.; Newton, J.L.; Zalewski, P.; Kędziora-Kornatowska, K. Cognitive functioning in older people. Results of the first wave of cognition of older people, education, recreational activities, nutrition, comorbidities, functional capacity studies (COPERNICUS). Front. Aging Neurosci. 2018, 10, 421. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.F.; Colcombe, S. Fitness effects on the cognitive function of older adults: A meta-analytic study—Revisited. Perspect. Psychol. Sci. 2018, 13, 213–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weuve, J.; Kang, J.H.; Manson, J.E.; Breteler, M.M.; Ware, J.H.; Grodstein, F. Physical activity, including walking, and cognitive function in older women. JAMA 2004, 292, 1454–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquine, M.J.; Segawa, E.; Wilson, R.S.; Bennett, D.A.; Barnes, L.L. Association between cognitive activity and cognitive function in older Hispanics. J. Int. Neuropsychol. Soc. 2012, 18, 1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, Y.; Barnes, C.A.; Grady, C.; Jones, R.N.; Raz, N. Brain reserve, cognitive reserve, compensation, and maintenance: Operationalization, validity, and mechanisms of cognitive resilience. Neurobiol. Aging 2019, 83, 124–129. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1983, 12, 189–198. [Google Scholar] [CrossRef]
- Mitchell, A.J. The Mini-Mental State Examination (MMSE): Update on its diagnostic accuracy and clinical utility for cognitive disorders. In Cognitive Screening Instruments; Springer: Cham, Switzerland, 2017; pp. 37–48. [Google Scholar]
- Uchmanowicz, I.; Jankowska-Polańska, B.; Mazur, G.; Froelicher, E.S. Cognitive deficits and self-care behaviors in elderly adults with heart failure. Clin. Interv. Aging 2017, 12, 1565–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarlane, O.; Kozakiewicz, M.; Kędziora-Kornatowska, K.; Gębka, D.; Szybalska, A.; Szwed, M.; Klich-Rączka, A. Blood Lipids and Cognitive Performance of Aging Polish Adults: A Case-Control Study Based on the PolSenior Project. Front. Aging Neurosci. 2020, 12, 590546. [Google Scholar] [CrossRef]
- Kapusta, J.; Kidawa, T.M.; Rynkowska-Kidawa, M.; Irzmański, T.R.; Kowalski, T.J. Evaluation of frequency of occurrence of cognitive impairment in the course of arterial hypertension in an elderly population. Psychogeriatrics 2020, 20, 406–411. [Google Scholar] [CrossRef]
- Freitas, S.; Simoes, M.R.; Marôco, J.; Alves, L.; Santana, I. Construct validity of the montreal cognitive assessment (MoCA). J. Int. Neuropsychol. Soc. 2012, 18, 242–250. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Magierska, J.; Magierski, R.; Fendler, W.; Kłoszewska, I.; Sobów, T.M. Clinical application of the Polish adaptation of the Montreal Cognitive Assessment (MoCA) test in screening for cognitive impairment. Neurol. Neurochir. Pol. 2012, 46, 130–139. [Google Scholar] [CrossRef] [Green Version]
- Reitan, R.M. Validity of the Trail Making Test as an indicator of organic brain damage. Percept. Mot. Skills 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Almeida, O.P.; Almeida, S.A. Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- Conradsson, M.; Rosendahl, E.; Littbrand, H.; Gustafson, Y.; Olofsson, B.; Lövheim, H. Usefulness of the Geriatric Depression Scale 15-item version among very old people with and without cognitive impairment. Aging Ment. Health 2013, 17, 638–645. [Google Scholar] [CrossRef]
- Albiński, R.; Kleszczewska-Albińska, A.; Bedyńska, S. Geriatryczna Skala Depresji (GDS). Trafność i rzetelność różnych wersji tego narzędzia–przegląd badań. Psychiatry Pol. 2011, 45, 555–562. [Google Scholar]
- Roomi, J.; Johnson, M.M.; Waters, K.; Yohannes, A.; Helm, A.C.M.J.; Connolly, M.J. Respiratory rehabilitation, exercise capacity and quality of life in chronic airways disease in old age. Age Ageing 1996, 25, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community-residing older adults. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. arXiv 2014, arXiv:1406.5823. [Google Scholar]
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous inference in general parametric models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cargin, W.J.; Collie, A.; Masters, C.; Maruff, P. The nature of cognitive complaints in healthy older adults with and without objective memory decline. J. Clin. Exp. Neuropsychol. 2008, 30, 245–257. [Google Scholar] [CrossRef]
- Farrin, L.; Hull, L.; Unwin, C.; Wykes, T.; David, A. Effects of depressed mood on objective and subjective measures of attention. J. Neuropsychiatry Clin. Neurosci. 2003, 15, 98–104. [Google Scholar] [CrossRef]
- Donaldson, C.; Lam, D.; Mathews, A. Rumination and attention in major depression. Behav. Res. 2007, 45, 2664–2678. [Google Scholar] [CrossRef] [PubMed]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balash, Y.; Mordechovich, M.; Shabtai, H.; Giladi, N.; Gurevich, T.; Korczyn, A.D. Subjective memory complaints in elders: Depression, anxiety, or cognitive decline? Acta Neurol. Scand. 2013, 127, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Charlesworth, G.M.; Brooker, H.J.; Potts, H.W.; Corbett, A.; Aarsland, D.; Ballard, C.G. Temporal Relationship Between Depressive Symptoms and Cognition in Mid and Late Life: A Longitudinal Cohort Study. Am. Med. Dir. Assoc. 2020, 21, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Schmand, B.E.N.; Jonker, C.; Geerlings, M.I.; Lindeboom, J. Subjective memory complaints in the elderly: Depressive symptoms and future dementia. Br. J. Psychiatry 1997, 171, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schütz, H.; Caspers, S.; Moebus, S.; Lux, S. Prevalence and psychosocial correlates of subjectively perceived decline in five cognitive domains. Results from a population-based cohort study in Germany. Int. J. Geriatr. Psychiatry 2020, 35, 1219–1227. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.N.; Wang, S.J.; Fuh, J.L.; Teng, E.L.; Liu, C.Y.; Lin, C.H.; Shyu, H.Y.; Lu, S.R.; Chen, C.C.; Liu, H.C. Subjective memory complaint in relation to cognitive performance and depression: A longitudinal study of a rural Chinese population. J. Am. Geriatr. Soc. 2000, 48, 295–299. [Google Scholar] [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Yates, J.A.; Clare, L.; Woods, R.T.; MRC CFAS. Subjective memory complaints, mood and MCI: A follow-up study. Aging Ment. Health 2017, 21, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenehan, M.E.; Klekociuk, S.Z.; Summers, M.J. Absence of a relationship between subjective memory complaint and objective memory impairment in mild cognitive impairment (MCI): Is it time to abandon subjective memory complaint as an MCI diagnostic criterion? Int. Psychogeriatr. 2012, 24, 1505–1514. [Google Scholar] [CrossRef]
- Molinuevo, J.L.; Rabin, L.A.; Amariglio, R.; Buckley, R.; Dubois, B.; Ellis, K.A.; Subjective Cognitive Decline Initiative (SCD-I) Working Group. Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement. 2017, 13, 296–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertzog, C.; Hülür, G.; Gerstorf, D.; Pearman, A.M. Is subjective memory change in old age based on accurate monitoring of age-related memory change? Evidence from two longitudinal studies. Psychol. Aging 2018, 33, 273. [Google Scholar] [CrossRef]
- Hill, N.L.; Mogle, J.; Whitaker, E.B.; Gilmore-Bykovskyi, A.; Bhargava, S.; Bhang, I.Y.; Sweeder, L.; Tiwari, P.A.; Van Haitsma, K. Sources of response bias in cognitive self-report items: “Which memory are you talking about?”. Gerontologist 2019, 59, 912–924. [Google Scholar] [CrossRef] [PubMed]
- Mogle, J.; Hill, N.; Bhang, I.; Bhargava, S.; Whitaker, E.; Kitt-Lewis, E. Time frame, problem specificity, and framing: The implicit structures of questions about memory in older adults. Aging Ment. Health 2020, 24, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Papenberg, G.; Bäckman, L.; Fratiglioni, L.; Laukka, E.J.; Fastbom, J.; Johnell, K. Anticholinergic drug use is associated with episodic memory decline in older adults without dementia. Neurobiol. Aging 2017, 55, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Couto, M.I.; Monteiro, A.; Oliveira, A.; Lunet, N.; Massano, J. Depression and anxiety following deep brain stimulation in Parkinson’s disease: Systematic review and meta-analysis. Acta Med. Port. 2014, 27, 372–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Not Examined in the Second Wave (n = 202) Mean ± SD | Re-Examined (n = 205) Mean ± SD | z or t | p-Value |
|---|---|---|---|---|
| Age (years) | 69.84 ± 6.3 | 69.66 ± 6.0 | 0.01 | 0.99 |
| Age of memory impairment (years) | 64.75 ± 7.3 | 65.12 ± 7.7 | −0.96 | 0.34 |
| MMSE (points) | 27.33 ± 2.4 | 27.80 ± 2.1 | −2.24 | 0.03 |
| MoCA (points) | 22.74 ± 3.7 | 23.63 ± 3.5 | −2.46 | 0.01 |
| MoCA Delayed Recall (words) | 2.26 ± 1.7 | 2.25 ± 1.6 | 0.10 | 0.92 |
| MoCA DR in overall (words) | 4.62 ± 0.8 | 4.76 ± 0.5 | −1.31 | 0.19 |
| MoCA Verbal Fluency (words) | 12.02 ± 4.4 | 12.73 ± 4.5 | −1.59 | 0.11 |
| TMT B (seconds) | 162.74 ± 99.4 | 136.90 ± 88.5 | 3.33 | <0.01 |
| GDS (points) | 3.37 ± 2.8 | 3.23 ± 2.8 | 0.71 | 0.48 |
| Health self-assessment-currently (points) | 6.73 ± 1.6 | 7.05 ± 1.5 | −1.75 | 0.08 |
| Health self-assessment-10 years ago (points) | 8.09 ± 1.7 | 8.00 ± 2.0 | 0.03 | 0.97 |
| Years of education (years) | 13.55 ± 3.1 | 14.37 ± 3.4 | −2.24 | 0.02 |
| Mental and social activity lvl (points) | 40.06 ± 8.5 | 42.72 ± 8.2 | −3.05 | <0.01 |
| Physical activity lvl (points) | 19.48 ± 7.9 | 20.06 ± 7.2 | −0.74 | 0.46 |
| Touristic activity lvl (points) | 6.42 ± 3.6 | 6.44 ± 3.4 | −0.21 | 0.83 |
| Sum of rich in antioxidants food intake (points) | 22.91 ± 6.2 | 24.11 ± 5.7 | −1.23 | 0.22 |
| Ethanol intake (points) | 4.27 ± 3.6 | 4.76 ± 3.5 | −1.41 | 0.16 |
| Total cognitive + physical + touristic activity lvl (points) | 65.95 ± 14.9 | 69.22 ± 14.2 | −2.24 | 0.02 |
| Financial status (points) | 10.95 ± 5.3 | 13.12 ± 5.3 | −3.96 | <0.01 |
| SMC Baseline | SMC after 2 Years | Count (n) | Frequency (%) |
|---|---|---|---|
| yes | yes | 125 | 61 |
| no | yes | 20 | 9.8 |
| yes | no | 37 | 18 |
| no | no | 23 | 11.2 |
| Variable | Subjective Memory Complaint Present | z | p-Value | |||
|---|---|---|---|---|---|---|
| Present (n = 162) | Not Present (n = 43) | |||||
| Mean | Std. Dev. | Mean | Std. Dev. | |||
| Age (years) | 70.25 | 6.1 | 67.44 | 5.2 | 2.67 | 0.01 |
| Years of education (years) | 14.23 | 3.5 | 14.91 | 3.2 | −1.56 | 0.12 |
| MMSE (points) | 27.69 | 2.2 | 28.21 | 1.7 | −1.35 | 0.18 |
| MoCA (points) | 23.67 | 3.6 | 23.51 | 3.1 | 0.63 | 0.53 |
| MoCA Verbal Fluency (words) | 12.67 | 4.5 | 12.95 | 4.7 | t = −0.36 | 0.72 |
| MoCA Delayed Recall (words) | 2.28 | 1.6 | 2.12 | 1.5 | 0.63 | 0.53 |
| TMT B (seconds) | 142.66 | 89.3 | 115.33 | 82.7 | 2.33 | 0.02 |
| GDS (points) | 3.46 | 2.8 | 2.35 | 2.7 | 2.69 | 0.01 |
| 8 ft test (seconds) | 6.14 | 2 | 5.58 | 2 | 2.19 | 0.03 |
| 6MWT (meters) | 496.95 | 97.9 | 535.33 | 105.8 | −2.54 | 0.01 |
| Variable | Subjective and Objective Memory Impairment | z | p-Value | |||
|---|---|---|---|---|---|---|
| Present (n = 60) | Not Present (n = 145) | |||||
| Mean | Std. Dev. | Mean | Std. Dev. | |||
| Age (years) | 70.38 | 6 | 69.37 | 6 | −1.20 | 0.23 |
| Years of education (years) | 13.55 | 3.3 | 14.71 | 3.4 | 2.54 | 0.01 |
| MMSE (points) | 27.78 | 2.2 | 27.81 | 2.1 | −0.28 | 0.78 |
| MoCA (points) | 24.68 | 3.2 | 23.20 | 3.6 | −2.74 | 0.01 |
| MoCA Verbal Fluency (words) | 12.53 | 4.4 | 12.81 | 4.6 | t = 0.4 | 0.69 |
| MoCA Delayed Recall (words) | 3.22 | 1.2 | 1.85 | 1.6 | −5.55 | <0.0001 |
| TMT B (seconds) | 158.78 | 101.1 | 127.78 | 81.3 | −2.02 | 0.04 |
| GDS (points) | 3.72 | 2.9 | 3.03 | 2.8 | −1.71 | 0.09 |
| 8 ft test (seconds) | 6.15 | 2.1 | 5.97 | 2 | −0.74 | 0.46 |
| 6MWT (meters) | 495.68 | 93.8 | 508.42 | 103.2 | 0.53 | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kujawski, S.; Kujawska, A.; Perkowski, R.; Androsiuk-Perkowska, J.; Hajec, W.; Kwiatkowska, M.; Skierkowska, N.; Husejko, J.; Bieniek, D.; Newton, J.L.; et al. Interaction between Subjective Memory Decline and Depression Symptom Intensity in Older People. Results of the Second Wave of Cognition of Older People, Education, Recreational Activities, Nutrition, Comorbidities, and Functional Capacity Studies (COPERNICUS). J. Clin. Med. 2021, 10, 1334. https://doi.org/10.3390/jcm10071334
Kujawski S, Kujawska A, Perkowski R, Androsiuk-Perkowska J, Hajec W, Kwiatkowska M, Skierkowska N, Husejko J, Bieniek D, Newton JL, et al. Interaction between Subjective Memory Decline and Depression Symptom Intensity in Older People. Results of the Second Wave of Cognition of Older People, Education, Recreational Activities, Nutrition, Comorbidities, and Functional Capacity Studies (COPERNICUS). Journal of Clinical Medicine. 2021; 10(7):1334. https://doi.org/10.3390/jcm10071334
Chicago/Turabian StyleKujawski, Sławomir, Agnieszka Kujawska, Radosław Perkowski, Joanna Androsiuk-Perkowska, Weronika Hajec, Małgorzata Kwiatkowska, Natalia Skierkowska, Jakub Husejko, Daria Bieniek, Julia L. Newton, and et al. 2021. "Interaction between Subjective Memory Decline and Depression Symptom Intensity in Older People. Results of the Second Wave of Cognition of Older People, Education, Recreational Activities, Nutrition, Comorbidities, and Functional Capacity Studies (COPERNICUS)" Journal of Clinical Medicine 10, no. 7: 1334. https://doi.org/10.3390/jcm10071334