
Age Differences in Motor Recruitment Patterns of the Shoulder in Dynamic and Isometric Contractions. A Cross-Sectional Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
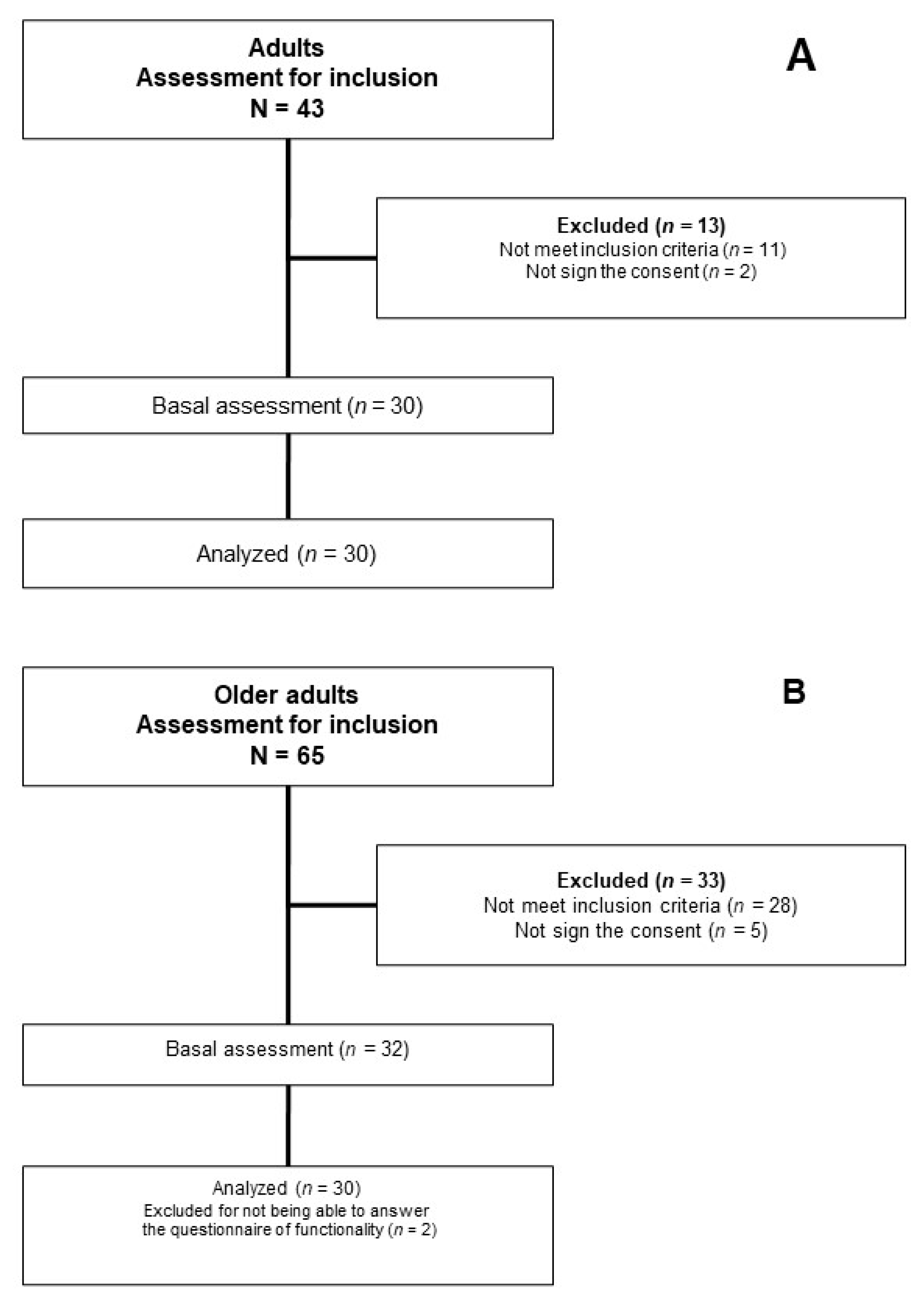
2.2. Participants
2.3. Assessments/Interventions
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. Age-Related Differences in Demographic and Clinical Data
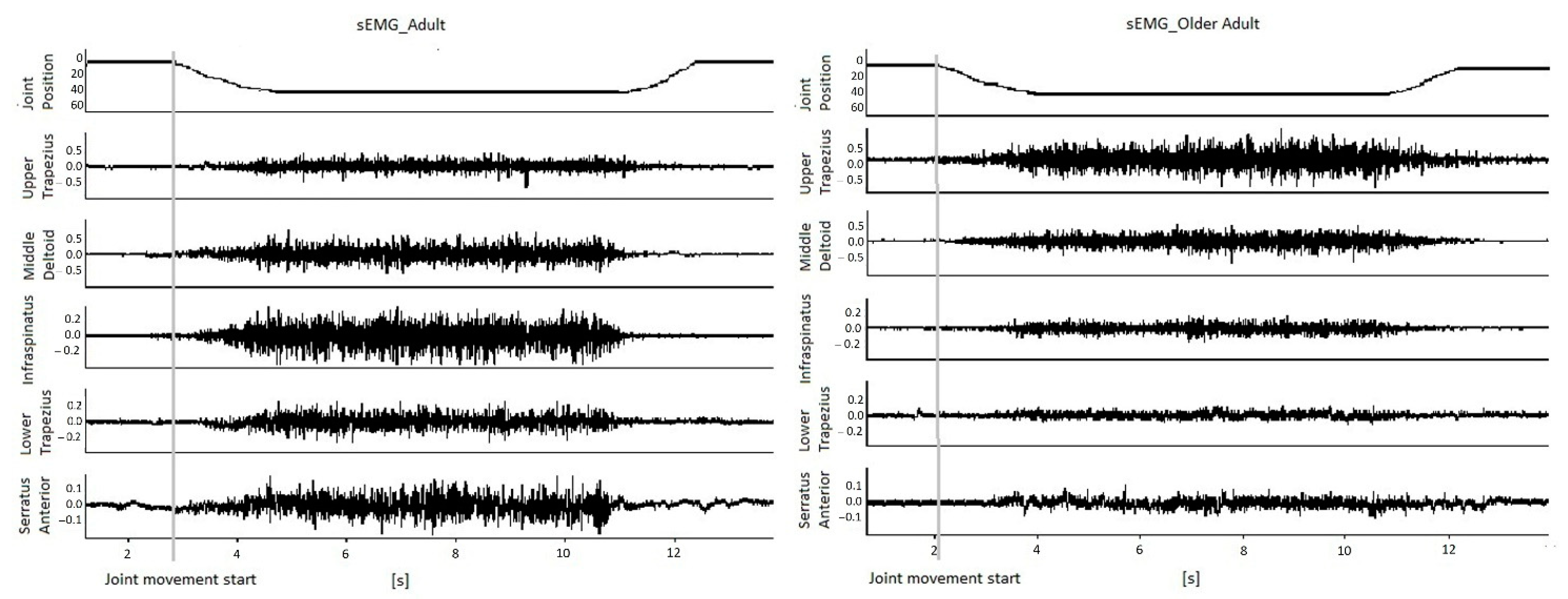
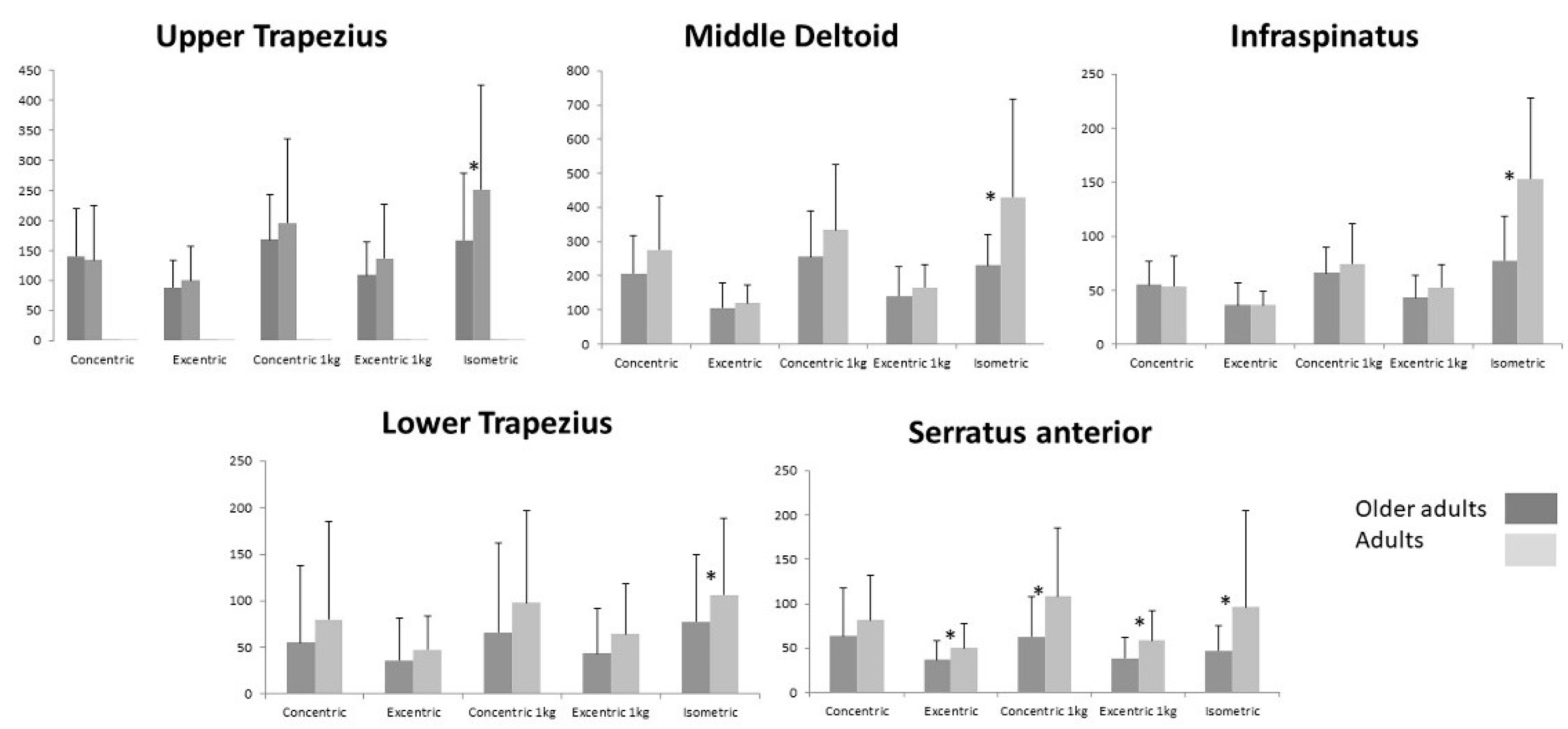
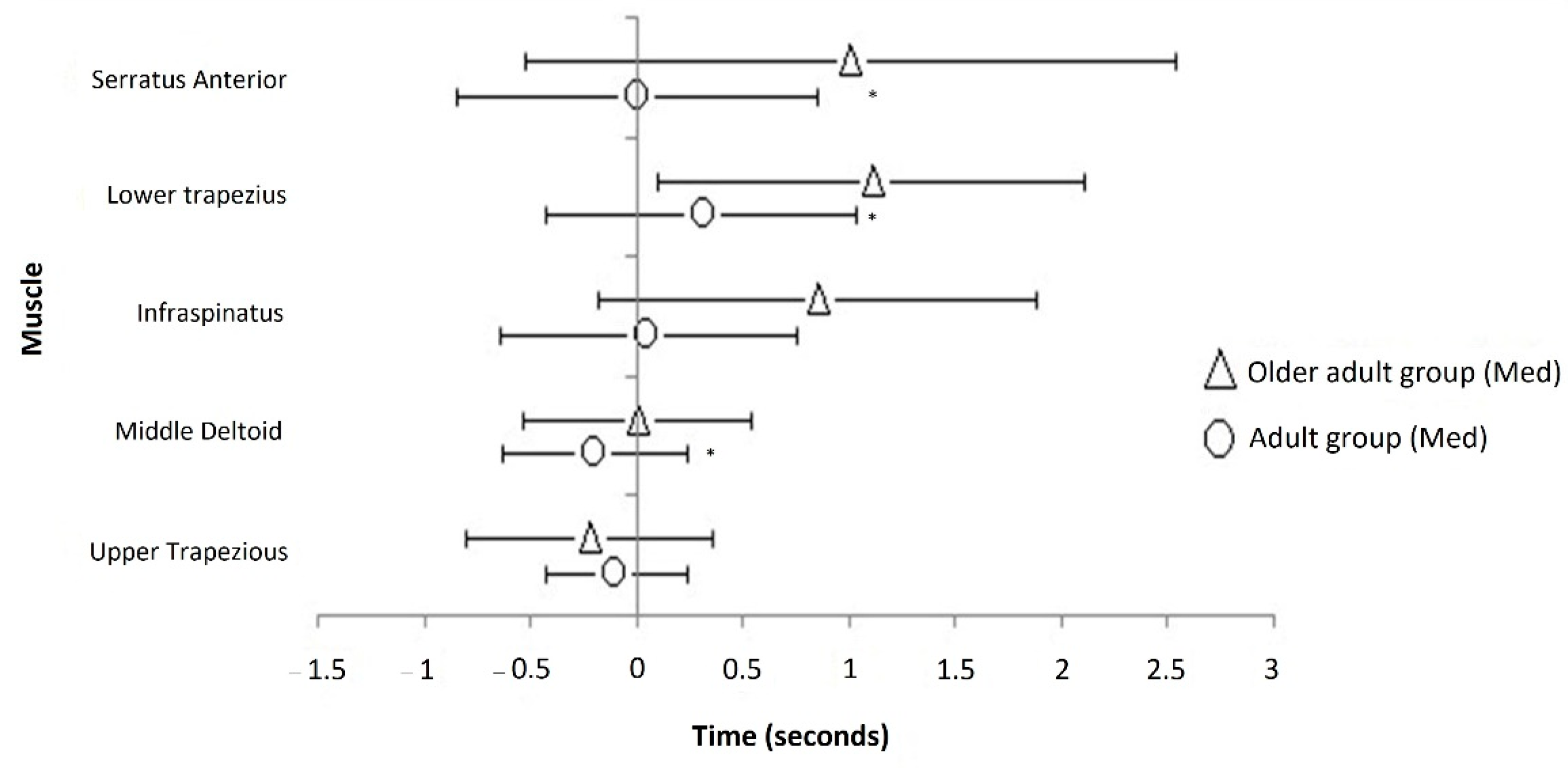
3.2. Age-Related Differences in sEMG Signal
4. Discussion
4.1. sEMG Signal
4.2. Limitations and Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dziechciaż, M.; Filip, R. Biological Psychological and Social Determinants of Old Age: Bio-Psycho-Social Aspects of Human Aging. Ann. Agric. Environ. Med. 2014, 21, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Tuna, H.D.; Edeer, A.O.; Malkoc, M.; Aksakoglu, G. Effect of Age and Physical Activity Level on Functional Fitness in Older Adults. Eur. Rev. Aging Phys. Act. 2009, 6, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, J.A.; Ramos, G.C.F.; Barbosa, A.T.F.; de Mendonça, J.M.G.; de Costa, F.M.; Caldeira, A.P. Prevalência e Fatores Associados à Fragilidade Em Idosos Não Institucionalizados. Rev. Bras. Enferm. 2016, 69, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Faurot, K. Epidemiology of Aging. In Proceedings of the APHA’s 2019 Annual Meeting and Expo, Philadelphia, PA, USA, 2–6 November 2019; American Public Health Association: Philadelphia, PA, USA, 2019. [Google Scholar]
- WHO. Ageing and Health; 2018. Available online: https://www.who.int/ageing/about/facts/es/ (accessed on 11 December 2020).
- Farr, J.N.; Almeida, M. The Spectrum of Fundamental Basic Science Discoveries Contributing to Organismal Aging. J. Bone Miner. Res. 2018, 33, 1568–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhillon, R.J.S.; Hasni, S. Pathogenesis and Management of Sarcopenia. Clin. Geriatr. Med. 2017, 33, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Ohlendiec, K. Proteomic Profiling of Fast-to-Slow Muscle Transitions during Aging. Front. Physiol. 2011, 2, 105. [Google Scholar] [CrossRef] [Green Version]
- Khosa, S.; Trikamji, B.; Khosa, G.S.; Khanli, H.M.; Mishra, S.K. An Overview of Neuromuscular Junction Aging Findings in Human and Animal Studies. Curr. Aging Sci. 2019, 12, 28–34. [Google Scholar] [CrossRef]
- Sanders, O.; Hsiao, H.Y.; Savin, D.N.; Creath, R.A.; Rogers, M.W. Aging Changes in Protective Balance and Startle Responses to Sudden Drop Perturbations. J. Neurophysiol. 2019, 122, 39–50. [Google Scholar] [CrossRef]
- Wickham, J.; Pizzari, T.; Stansfeld, K.; Burnside, A.; Watson, L. Quantifying ‘Normal’ Shoulder Muscle Activity during Abduction. J. Electromyogr. Kinesiol. 2010, 20, 212–222. [Google Scholar] [CrossRef]
- Lirio-Romero, C.; Anders, C.; de La Villa-Polo, P.; Torres-Lacomba, M. Implications on Older Women of Age- and Sex-Related Differences in Activation Patterns of Shoulder Muscles: A Cross-Sectional Study. J. Women Aging 2019, 31, 492–512. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, J.A.; Larkin, L.M.; Claflin, D.R.; Brooks, S.V. Age-related changes in the structure and function of skeletal muscles. Clin. Exp. Pharmacol. Physiol. 2007, 34, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.M.; Housh, T.J.; Hill, E.C.; Keller, J.L.; Johnson, G.O.; Schmidt, R.J. Are There Mode-Specific and Fatigue-Related Electromechanical Delay Responses for Maximal Isokinetic and Isometric Muscle Actions? J. Electromyogr. Kinesiol. 2017, 37, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.M.; Housh, T.J.; Hill, E.C.; Johnson, G.O.; Schmidt, R.J. Dynamic versus Isometric Electromechanical Delay in Non-Fatigued and Fatigued Muscle: A Combined Electromyographic, Mechanomyographic, and Force Approach. J. Electromyogr. Kinesiol. 2017, 33, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Namdari, S.; Yagnik, G.; Ebaugh, D.D.; Nagda, S.; Ramsey, M.L.; Williams, G.R.; Mehta, S. Defining Functional Shoulder Range of Motion for Activities of Daily Living. J. Shoulder Elb. Surg. 2012, 21, 1177–1183. [Google Scholar] [CrossRef]
- Veeger, H.E.J.; van der Helm, F.C.T. Shoulder Function: The Perfect Compromise between Mobility and Stability. J. Biomech. 2007, 40, 711–714. [Google Scholar] [CrossRef]
- McManus, L.; de Vito, G.; Lowery, M.M. Analysis and Biophysics of Surface EMG for Physiotherapists and Kinesiologists: Toward a Common Language with Rehabilitation Engineers. Front. Neurol. 2020, 11, 576729. [Google Scholar] [CrossRef]
- Medved, V.; Medved, S.; Kovač, I. Critical Appraisal of Surface Electromyography (SEMG) as a Taught Subject and Clinical Tool in Medicine and Kinesiology. Front. Neurol. 2020, 11, 560363. [Google Scholar] [CrossRef]
- Clinical Trials.gov. U.S. National Library of Medicine. 2021. Available online: https://clinicaltrials.gov (accessed on 12 January 2021).
- Kapanji, A. The Physiology of the Joints, Vol. 1, the Upper Limb; Churchill Livingstone: Edingburgh, UK, 2007. [Google Scholar]
- Celik, D.; Dirican, A.; Baltaci, G. Intrarater Reliability of Assessing Strength of the Shoulder and Scapular Muscles. J. Sport Rehabil. 2012, 21, 1–5. [Google Scholar] [CrossRef]
- Ashour, A.A. Relationship between Isometric Muscle Force and Surface EMG of Wrist Muscles at Different Shoulder and Elbow Angles. J. Am. Sci. 2014, 10, 26–34. [Google Scholar]
- Rolf, O.; Ochs, K.; Bohm, T.D.; Baumann, B.; Kirschner, S.; Gohlke, F. Rotator cuff tear—An occupational disease? An epidemiological analysis. Z. Orthop. Ihre Grenzgeb. 2006, 144, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Magermans, D.J.; Chadwick, E.K.J.; Veeger, H.E.J.; Van Der Helm, F.C.T. Requirements for upper extremity motions during activities of daily living. Clin. Biomech. 2005, 20, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Lucas, K.R.; Rich, P.A.; Polus, B.I. Muscle activation patterns in the scapular positioning muscles during loaded scapular plane elevation: The effects of latent myofascial trigger points. Clin. Biomech. 2010, 25, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.S.; Christensen, B.H.; Samani, A.; Madeleine, P. Between-Day Reliability of a Hand-Held Dynamometer and Surface Electromyography Recordings during Isometric Submaximal Contractions in Different Shoulder Positions. J. Electromyogr. Kinesiol. 2014, 24, 579–587. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, G.J.M.G.; Leffers, P.; Bouter, L.M. Shoulder Disability Questionnaire Design and Responsiveness of a Functional Status Measure. J. Clin. Epidemiol. 2000, 53, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Villarroya Aparicio, M.A. Electromiografía Cinesiológica. Rehabilitación 2005, 39, 255–264. [Google Scholar] [CrossRef]
- Raz, Y.; Henseler, J.F.; Kolk, A.; Tatum, Z.; Groosjohan, N.K.; Verwey, N.E.; Arindrarto, W.; Kielbasa, S.M.; Nagels, J.; ’t Hoen, P.A.C.; et al. Molecular Signatures of Age-Associated Chronic Degeneration of Shoulder Muscles. Oncotarget 2016, 7, 8513–8523. [Google Scholar] [CrossRef] [Green Version]
- Farina, D.; Merletti, R.; Enoka, R.M. The Extraction of Neural Strategies from the Surface EMG: An Update. J. Appl. Physiol. 2014, 117, 1215–1230. [Google Scholar] [CrossRef] [Green Version]
- Doherty, T.J. Invited Review: Aging and Sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef] [Green Version]
- Merletti, R.; Farina, D.; Gazzoni, M.; Schieroni, M.P. Effect of Age on Muscle Functions Investigated with Surface Electromyography. Muscle Nerve 2002, 25, 65–76. [Google Scholar] [CrossRef]
- Plow, E.B.; Varnerin, N.; Cunningham, D.A.; Janini, D.; Bonnett, C.; Wyant, A.; Hou, J.; Siemionow, V.; Wang, X.-F.; Machado, A.G.; et al. Age-Related Weakness of Proximal Muscle Studied with Motor Cortical Mapping: A TMS Study. PLoS ONE 2014, 9, e89371. [Google Scholar] [CrossRef]
- Raz, Y.; Henseler, J.F.; Kolk, A.; Riaz, M.; van der Zwaal, P.; Nagels, J.; Nelissen, R.G.H.H.; Raz, V. Patterns of Age-Associated Degeneration Differ in Shoulder Muscles. Front. Aging Neurosci. 2015, 7, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, A.-C.; Hsieh, T.-H.; Luh, J.-J.; Lin, T.-T. A Comparison of Upper-Limb Motion Pattern Recognition Using EMG Signals during Dynamic and Isometric Muscle Contractions. Biomed. Signal Process. Control 2014, 11, 17–26. [Google Scholar] [CrossRef]
- McDonald, A.C.; Savoie, S.M.; Mulla, D.M.; Keir, P.J. Dynamic and Static Shoulder Strength Relationship and Predictive Model. Appl. Ergon. 2018, 67, 162–169. [Google Scholar] [CrossRef]
- Radaelli, R.; Bottaro, M.; Weber, F.; Brown, L.E.; Pinto, R.S. Influence of Body Position on Shoulder Rotator Muscle Strength during Isokinetic Assessment. Isokinet. Exerc. Sci. 2010, 18, 119–124. [Google Scholar] [CrossRef]
- Linnamo, V. Motor Unit Activation and Force Production during Eccentric, Concentric and Isometric Actions. Stud. Sport Phys. Educ. Health 2002, 82. [Google Scholar]
- Baggen, R.J.; van Dieën, J.H.; Verschueren, S.M.; van Roie, E.; Delecluse, C. Differences in Maximum Voluntary Excitation Between Isometric and Dynamic Contractions Are Age-Dependent. J. Appl. Biomech. 2019, 35, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Lirio-Romero, C.; Torres-Lacomba, M.; Gómez-Blanco, A.; Acero-Cortés, A.; Retana-Garrido, A.; de la Villa-Polo, P.; Sánchez-Sánchez, B. Electromyographic Biofeedback Improves Upper Extremity Function: A Randomized, Single-Blinded, Controlled Trial. Physiotherapy 2020, 15, S0031-9406(20)30016-X. [Google Scholar] [CrossRef] [PubMed]
- Phadke, V.; Camargo, P.; Ludewig, P. Scapular and Rotator Cuff Muscle Activity during Arm Elevation: A Review of Normal Function and Alterations with Shoulder Impingement. Braz. J. Phys. Ther. 2009, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kibler, B.W.; McMullen, J. Scapular dyskinesis and its relation to shoulder pain. J. Am. Acad. Orthop. Surg. 2003, 11, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Comerford, M.J.; Mottram, S. Diagnosis of Uncontrolled Movement, Subgroup Classification and Motor Control Retraining of the Shoulder Girdle; KC International: Ludlow, UK, 2010. [Google Scholar]
- Hackett, L.; Reed, D.; Halaki, M.; Ginn, K.A. Assessing the validity of surface electromyography for recording muscle activation patterns from serratus anterior. J. Electromyogr. Kinesiol. 2014, 24, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Nordander, C.; Willner, J.; Hansson, G.; Larsson, B.; Unge, J.; Granquist, L.; Skerfving, S. Influence of the Subcutaneous Fat Layer, as Measured by Ultrasound, Skinfold Calipers and BMI, on the EMG Amplitude. Eur. J. Appl. Physiol. 2003, 89, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.-S.; Kim, J.-H.; Hong, J.-H.; Chun, K.-J. Electromyograph Analysis during Isokinetic Testing of Shoulder Joint in Elderly People. J. Biomech. Sci. Eng. 2012, 7, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Kwon, M.; Chen, Y.-T.; Fox, E.J.; Christou, E.A. Aging and Limb Alter the Neuromuscular Control of Goal-Directed Movements. Exp. Brain Res. 2014, 232, 1759–1771. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Chandler, T.J.; Shapiro, R.; Conuel, M. Muscle activation in coupled scapulohumeral motions in the high performance tennis serve. Br. J. Sports Med. 2007, 41, 745–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kibler, W.B.; Ellenbecker, T.; Sciascia, A. Neuromuscular adaptations in shoulder function and dysfunction. Handb. Clin. Neurol. 2018, 158, 385–400. [Google Scholar] [CrossRef]
- Chadnova, E.; St-Onge, N.; Courtemanche, R.; Kilgour, R.D. Kinematics and Muscle Activation Patterns during a Maximal Voluntary Rate Activity in Healthy Elderly and Young Adults. Aging Clin. Exp. Res. 2017, 29, 1001–1011. [Google Scholar] [CrossRef]
- Škarabot, J.; Ansdell, P.; Brownstein, C.G.; Hicks, K.M.; Howatson, G.; Goodall, S.; Durbaba, R. Reduced Corticospinal Responses in Older Compared with Younger Adults during Submaximal Isometric, Shortening, and Lengthening Contractions. J. Appl. Physiol. 2019, 126, 1015–1031. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Adults n = 30 | Older Adults n = 30 | p-Value † |
|---|---|---|---|
| Age Median (IR *) | 45.5(27.5) | 70.5(8.3) | <0.01 |
| Gender n women (%) | 15(50) | 16(53.3) | 0.80 |
| Dominant limb n right (%) | 30(100) | 28(93.3) | 0.16 |
| Previous physiotherapy treatments n yes (%) | 2(6.7) | 11(36.7) | <0.05 |
| Body mass index Mean (SD **) | 24.4(3) | 29.2(3.6) | <0.01 |
| MVIC [Newton] Mean (SD **) | 122.9(44) | 75.7(26) | <0.01 |
| SDQ Median (IR *) | 0(0) | 0(12.5) | <0.01 |
| Glenohumeral Flexion Mean (SD **) | 160.5(9.5) | 151.2(9.3) | <0.01 |
| Glenohumeral Internal Rotation Mean (SD **) | 73.8(10.6) | 70.7(22.7) | 0.49 |
| Glenohumeral External Rotation Mean (SD **) | 85.5(8.4) | 71.8(15.1) | <0.01 |
| Glenohumeral Abduction Mean (SD **) | 160.8(11.8) | 147.5(9.5) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lirio-Romero, C.; Palomo-Carrión, R.; Romay-Barrero, H.; Ferri-Morales, A.; Prieto-Gómez, V.; Torres-Lacomba, M. Age Differences in Motor Recruitment Patterns of the Shoulder in Dynamic and Isometric Contractions. A Cross-Sectional Study. J. Clin. Med. 2021, 10, 525. https://doi.org/10.3390/jcm10030525
Lirio-Romero C, Palomo-Carrión R, Romay-Barrero H, Ferri-Morales A, Prieto-Gómez V, Torres-Lacomba M. Age Differences in Motor Recruitment Patterns of the Shoulder in Dynamic and Isometric Contractions. A Cross-Sectional Study. Journal of Clinical Medicine. 2021; 10(3):525. https://doi.org/10.3390/jcm10030525
Chicago/Turabian StyleLirio-Romero, Cristina, Rocío Palomo-Carrión, Helena Romay-Barrero, Asunción Ferri-Morales, Virginia Prieto-Gómez, and María Torres-Lacomba. 2021. "Age Differences in Motor Recruitment Patterns of the Shoulder in Dynamic and Isometric Contractions. A Cross-Sectional Study" Journal of Clinical Medicine 10, no. 3: 525. https://doi.org/10.3390/jcm10030525