Usefulness of Staging Chest CT in Breast Cancer: Evaluating Diagnostic Yield of Chest CT According to the Molecular Subtype and Clinical Stage


Abstract
:1. Introduction
2. Materials and Methods
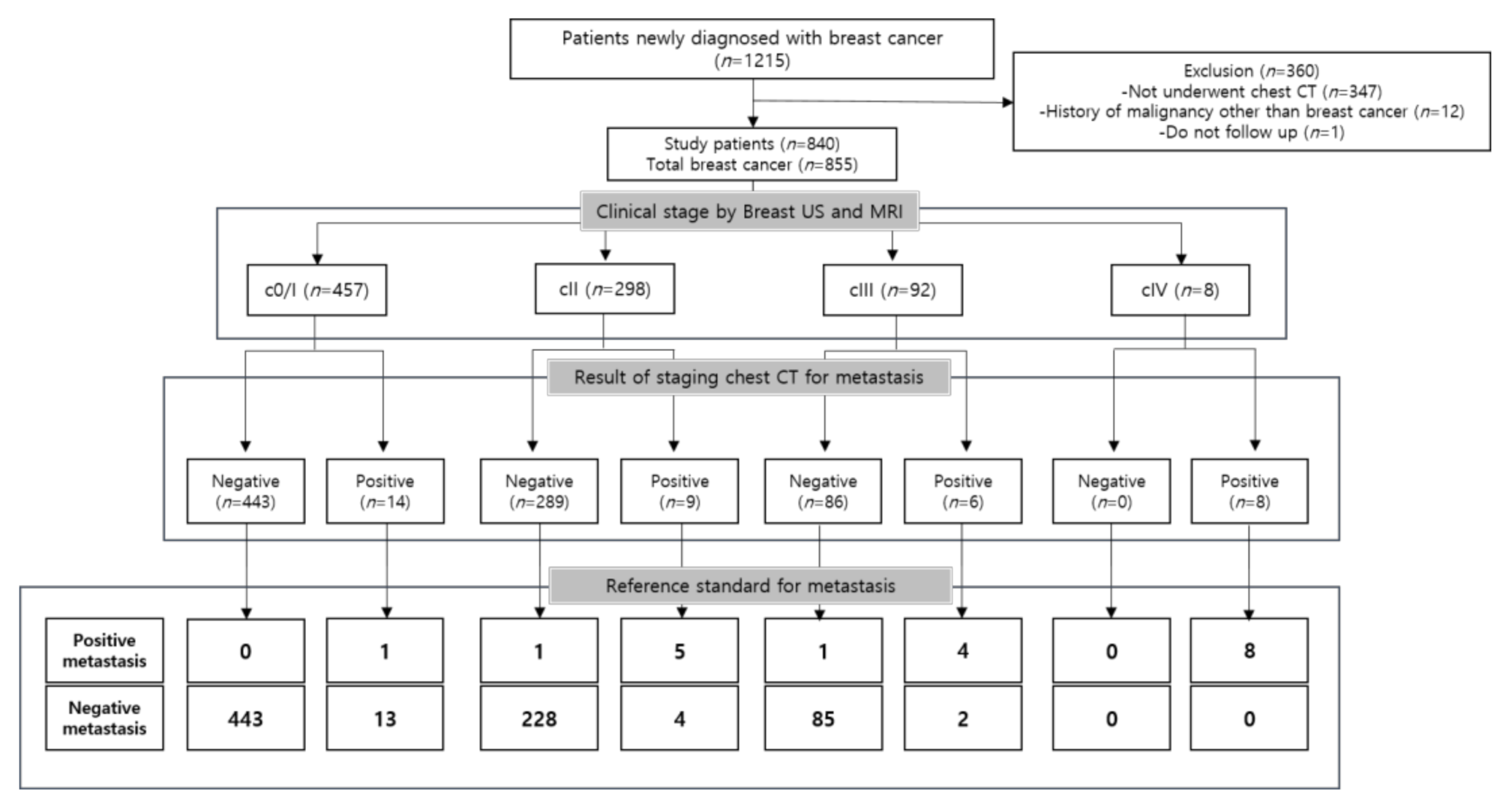
2.1. Study Design and Patients
2.2. Image Acquisition
2.3. Clinical and Image Analysis
2.3.1. Analysis of Breast Imaging
2.3.2. Analysis of Chest Imaging
2.4. Reference Standard
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Mahner, S.; Schirrmacher, S.; Brenner, W.; Jenicke, L.; Habermann, C.R.; Avril, N.; Dose-Schwarz, J. Comparison between positron emission tomography using 2-[fluorine-18]fluoro-2-deoxy-D-glucose, conventional imaging and computed tomography for staging of breast cancer. Ann. Oncol. 2008, 19, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Kreisman, H.; Wolkove, N.; Finkelstein, H.S.; Cohen, C.; Margolese, R.; Frank, H. Breast cancer and thoracic metastases: Review of 119 patients. Thorax 1983, 38, 175–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, M.E.; Houssami, N. Evaluation of the evidence on staging imaging for detection of asymptomatic distant metastases in newly diagnosed breast cancer. Breast 2012, 21, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Han, W.; Moon, H.G.; Min, J.; Ahn, S.K.; Kim, T.Y.; Im, S.A.; Oh, D.Y.; Han, S.W.; Chie, E.K.; et al. The value of preoperative staging chest computed tomography to detect asymptomatic lung and liver metastasis in patients with primary breast carcinoma. Breast Cancer Res. Treat. 2011, 126, 637–641. [Google Scholar] [CrossRef]
- Schnipper, L.E.; Smith, T.J.; Raghavan, D.; Blayney, D.W.; Ganz, P.A.; Mulvey, T.M.; Wollins, D.S. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: The top five list for oncology. J. Clin. Oncol. 2012, 30, 1715–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradishar, W.J.; Anderson, B.O. NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 18 March 2020).
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol 2019, 30, 1674. [Google Scholar] [CrossRef] [Green Version]
- Dull, B.; Linkugel, A.; Margenthaler, J.A.; Cyr, A.E. Overuse of Chest CT in Patients with Stage I and II Breast Cancer: An Opportunity to Increase Guidelines Compliance at an NCCN Member Institution. J. Nat. Compr. Cancer Netw. 2017, 15, 783–789. [Google Scholar] [CrossRef]
- Telli, M.L.; Gradishar, W.J.; Ward, J.H. NCCN Guidelines Updates: Breast Cancer. J. Nat. Compr. Cancer Netw. 2019, 17, 552–555. [Google Scholar]
- Simos, D.; Hutton, B.; Graham, I.D.; Arnaout, A.; Caudrelier, J.M.; Clemons, M. Imaging for metastatic disease in patients with newly diagnosed breast cancer: Are doctor's perceptions in keeping with the guidelines? J. Eval. Clin. Pract. 2015, 21, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Trop, I.; LeBlanc, S.M.; David, J.; Lalonde, L.; Tran-Thanh, D.; Labelle, M.; El Khoury, M.M. Molecular classification of infiltrating breast cancer: Toward personalized therapy. Radiographics 2014, 34, 1178–1195. [Google Scholar] [CrossRef] [Green Version]
- Sorlie, T.; Tibshirani, R.; Parker, J.; Hastie, T.; Marron, J.S.; Nobel, A.; Deng, S.; Johnsen, H.; Pesich, R.; Geisler, S.; et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 2003, 100, 8418–8423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, C.; Oh, D.S.; Wessels, L.; Weigelt, B.; Nuyten, D.S.; Nobel, A.B.; van't Veer, L.J.; Perou, C.M. Concordance among gene-expression-based predictors for breast cancer. N. Engl. J. Med. 2006, 355, 560–569. [Google Scholar] [CrossRef] [Green Version]
- Voduc, K.D.; Cheang, M.C.; Tyldesley, S.; Gelmon, K.; Nielsen, T.O.; Kennecke, H. Breast cancer subtypes and the risk of local and regional relapse. J. Clin. Oncol. 2010, 28, 1684–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobbezoo, D.J.; van Kampen, R.J.; Voogd, A.C.; Dercksen, M.W.; van den Berkmortel, F.; Smilde, T.J.; van de Wouw, A.J.; Peters, F.P.; van Riel, J.M.; Peters, N.A.; et al. Prognosis of metastatic breast cancer subtypes: The hormone receptor/HER2-positive subtype is associated with the most favorable outcome. Breast Cancer Res. Treat. 2013, 141, 507–514. [Google Scholar] [CrossRef]
- Kennecke, H.; Yerushalmi, R.; Woods, R.; Cheang, M.C.; Voduc, D.; Speers, C.H.; Nielsen, T.O.; Gelmon, K. Metastatic behavior of breast cancer subtypes. J. Clin. Oncol. 2010, 28, 3271–3277. [Google Scholar] [CrossRef]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth edition of the AJCC cancer staging manual: Breast cancer. Ann. Surg Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- Park, C.M.; Goo, J.M.; Kim, T.J.; Lee, H.J.; Lee, K.W.; Lee, C.H.; Kim, Y.T.; Kim, K.G.; Lee, H.Y.; Park, E.A.; et al. Pulmonary nodular ground-glass opacities in patients with extrapulmonary cancers: What is their clinical significance and how can we determine whether they are malignant or benign lesions? Chest 2008, 133, 1402–1409. [Google Scholar] [CrossRef]
- Tsushima, Y.; Suzuki, K.; Watanabe, S.; Kusumoto, M.; Tsuta, K.; Matsuno, Y.; Asamura, H. Multiple lung adenocarcinomas showing ground-glass opacities on thoracic computed tomography. Ann. Thorac. Surg. 2006, 82, 1508–1510. [Google Scholar] [CrossRef]
- van Overhagen, H.; Brakel, K.; Heijenbrok, M.W.; van Kasteren, J.H.; van de Moosdijk, C.N.; Roldaan, A.C.; van Gils, A.P.; Hansen, B.E. Metastases in supraclavicular lymph nodes in lung cancer: Assessment with palpation, US, and CT. Radiology 2004, 232, 75–80. [Google Scholar] [CrossRef]
- Fultz, P.J.; Harrow, A.R.; Elvey, S.P.; Feins, R.H.; Strang, J.G.; Wandtke, J.C.; Johnstone, D.W.; Watson, T.J.; Gottlieb, R.H.; Voci, S.L.; et al. Sonographically guided biopsy of supraclavicular lymph nodes: A simple alternative to lung biopsy and other more invasive procedures. Am. J. Roentgenol. 2003, 180, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Udoji, T.N.; Phillips, G.S.; Berkowitz, E.A.; Berkowitz, D.; Ross, C.; Bechara, R.I. Mediastinal and Hilar Lymph Node Measurements. Comparison of Multidetector-Row Computed Tomography and Endobronchial Ultrasound. Ann. Am. Thorac. Soc. 2015, 12, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Lincke, T.; Zech, C.J. Liver metastases: Detection and staging. Eur. J. Radiol. 2017, 97, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, C.M.; Rohren, E.M.; Madewell, J.E.; Hamaoka, T.; Theriault, R.L.; Yu, T.K.; Lewis, V.O.; Ma, J.; Stafford, R.J.; Tari, A.M.; et al. Imaging bone metastases in breast cancer: Techniques and recommendations for diagnosis. Lancet Oncol. 2009, 10, 606–614. [Google Scholar] [CrossRef]
- Hamaoka, T.; Madewell, J.E.; Podoloff, D.A.; Hortobagyi, G.N.; Ueno, N.T. Bone imaging in metastatic breast cancer. J. Clin. Oncol. 2004, 22, 2942–2953. [Google Scholar] [CrossRef]
- Pepe, M.S.; Alonzo, T.A. Comparing disease screening tests when true disease status is ascertained only for screen positives. Biostatistics 2001, 2, 249–260. [Google Scholar] [CrossRef]
- Lee, K.H.; Park, J.H.; Kim, Y.H.; Lee, K.W.; Kim, J.W.; Oh, H.K.; Jeon, J.J.; Yoon, H.; Kim, J.; Lee, K.H. Diagnostic Yield and False-Referral Rate of Staging Chest CT in Patients with Colon Cancer. Radiology 2018, 289, 535–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerber, B.; Seitz, E.; Muller, H.; Krause, A.; Reimer, T.; Kundt, G.; Friese, K. Perioperative screening for metastatic disease is not indicated in patients with primary breast cancer and no clinical signs of tumor spread. Breast Cancer Res. Treat. 2003, 82, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Linkugel, A.; Margenthaler, J.; Dull, B.; Cyr, A. Staging studies have limited utility for newly diagnosed stage I-II breast cancer. J. Surg Res. 2015, 196, 33–38. [Google Scholar] [CrossRef]
- Simos, D.; Hutton, B.; Clemons, M. Are Physicians Choosing Wisely When Imaging for Distant Metastases in Women With Operable Breast Cancer? J. Oncol. Pract. 2015, 11, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Vona-Davis, L.; Rose, D.P.; Gadiyaram, V.; Ducatman, B.; Hobbs, G.; Hazard, H.; Kurian, S.; Abraham, J. Breast cancer pathology, receptor status, and patterns of metastasis in a rural appalachian population. J. Cancer Epidemiol. 2014, 2014, 170634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.C.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M.; et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017, 284, 228–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brothers, J.M.; Kidwell, K.M.; Brown, R.K.; Henry, N.L. Incidental radiologic findings at breast cancer diagnosis and likelihood of disease recurrence. Breast Cancer Res. Treat. 2016, 155, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Cancer (%) |
|---|---|
| Age (years) | 840 patients |
| ≤35 | 35 |
| 36–50 | 430 |
| ≥51 | 375 |
| Clinical stage | 855 cases |
| 0 | 28 (3.3) |
| I | 429 (50.2) |
| II | 298 (34.9) |
| III | 92 (10.8) |
| IV | 8 (0.9) |
| ER status | 855 cases |
| Positive | 679 (79.4) |
| Negative | 162 (18.9) |
| Unknown | 14 (1.6) |
| PgR status | 855 cases |
| Positive | 632 (73.9) |
| Negative | 206 (24.1) |
| Unknown | 17 (2.0) |
| HER2 amplification | 855 cases |
| Positive | 169 (19.8) |
| Negative | 665 (77.8) |
| Unknown | 21 (2.5) |
| Molecular type | 855 cases |
| Luminal | 709 (82.9) |
| HER2-enriched | 55 (6.4) |
| Triple negative | 77 (9.0) |
| Unknown | 14 (1.6) |
| Histologic grade | |
| High | 246 (28.8) |
| Low | 505 (59.1) |
| Unknown | 104 (12.2) |
| Nuclear grade | |
| High | 301 (35.2) |
| Low | 450 (52.6) |
| Unknown | 104 (12.2) |
| Histology | Number of Cancer (n = 855) |
|---|---|
| Invasive ductal carcinoma | 759 |
| Invasive lobular carcinoma | 49 |
| Mucinous carcinoma | 19 |
| Metaplastic carcinoma | 7 |
| Tubular carcinoma | 6 |
| Micropapillary carcinoma | 5 |
| Others | 10 |
| Clinical Stage by US and MRI | ||||||
|---|---|---|---|---|---|---|
| 0/I | II | III | IV | Total | ||
| Molecular subtype | Luminal | 400 (56.4%) | 242 (34.1%) | 63 (8.9%) | 4 (0.6%) | 709 |
| HER2-enriched | 20 (36.4%) | 23 (41.8%) | 11 (20.0%) | 1 (1.8%) | 55 | |
| Triple negative | 30 (39.0%) | 29 (37.7%) | 16 (20.8%) | 2 (2.6%) | 77 | |
| Total | 450 | 294 | 90 | 7 | 841 | |
| Clinical Stage (n = 855) | Diagnostic Yield | False-Referral Rate |
| 0/1 | 0.2% [1/457] | 2.8% [13/457] |
| II | 1.7% [5/298] | 1.3% [4/298] |
| III | 4.3% [4/92] | 2.2% [2/92] |
| IV | 100.0% [8/8] | 0.0% [0/8] |
| Molecular Subtype (n = 841) | Diagnostic Yield | False-Referral Rate |
| Luminal | 1.7% [12/709] | 2.1% [15/709] |
| HER2-enriched | 3.6% [2/55] | 1.8% [1/55] |
| Triple negative | 2.6% [2/77] | 3.9% [3/77] |
| Unknown | [2/14] | [0/14] |
| Clinical Stage | ||||
|---|---|---|---|---|
| Molecular Subtype | 0/I | II | III | IV |
| Luminal | 0% | 1.65% | 6.30% | 100% |
| (0/400) | (4/242) | (4/63) | (4/4) | |
| HER2-enriched | 0% | 4.30% | 0% | 100% |
| (0/20) | (1/23) | (0/11) | (1/1) | |
| Triple negative | 0% | 0% | 0% | 100% |
| (0/30) | (0/29) | (0/16) | (2/2) | |
| Diagnostic Yield | False-Referral Rate | |||||
|---|---|---|---|---|---|---|
| Factors | Negative Metastasis | Positive Metastasis | p-Value | Negative Finding | False Positive | p-Value |
| Clinical stage | 0.000 * | 0.526 | ||||
| 0/I | 456 | 1 | 444 | 13 | ||
| II | 293 | 5 | 294 | 4 | ||
| III | 88 | 4 | 90 | 2 | ||
| IV | 0 | 8 | 8 | 0 | ||
| Age | 0.063 | 0.808 | ||||
| ≤35 | 35 | 0 | 34 | 1 | ||
| 36–50 | 430 | 5 | 427 | 8 | ||
| ≥51 | 372 | 13 | 375 | 10 | ||
| Molecular subtype | 0.343 | 0.481 | ||||
| Luminal | 697 | 12 | 694 | 15 | ||
| HER2-enriched | 53 | 2 | 54 | 1 | ||
| TN | 75 | 2 | 74 | 3 | ||
| Histologic grade | 0.399 | 0.130 | ||||
| High | 243 | 3 | 237 | 9 | ||
| Low | 502 | 3 | 496 | 9 | ||
| Nuclear grade | 0.225 | 0.027 * | ||||
| High | 297 | 4 | 289 | 12 | ||
| Low | 448 | 2 | 444 | 6 | ||
| Total (n = 840) | c0/I (n = 445) | cII (n = 295) | cIII (n = 92) | cIV (n = 8) | |
| Lung cancer | 6 (0.7%) | 3 (0.7%) | 2 (0.7%) | 1 (1.1%) | 0 (0%) |
| Cancer * | 3 (0.4%) | 1 (0.2%) | 1 (0.3%) | 1 (1.1%) | 0 (0%) |
| Subsolid nodule ** | 19 (2.3%) | 12 (2.7%) | 4 (1.4%) | 3 (3.3%) | 0 (0%) |
| Tuberculosis/Non- tuberculous mycobacterium | 4 (0.5%) | 3 (0.7%) | 0 (0%) | 1 (1.1%) | 0 (0%) |
| Pneumonia | 4 (0.5%) | 0 (0%) | 2 (0.7%) | 2 (2.2%) | 0 (0%) |
| Others *** | 12 (1.4%) | 8 (1.8%) | 4 (1.4%) | 0 (0%) | 0 (0%) |
| Total | 48 (5.7%) | 27 (6.1%) | 13 (4.4%) | 8 (8.7%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
You, S.; Kim, T.H.; Kang, D.K.; Park, K.J.; An, Y.-S.; Sun, J.S. Usefulness of Staging Chest CT in Breast Cancer: Evaluating Diagnostic Yield of Chest CT According to the Molecular Subtype and Clinical Stage. J. Clin. Med. 2021, 10, 906. https://doi.org/10.3390/jcm10050906
You S, Kim TH, Kang DK, Park KJ, An Y-S, Sun JS. Usefulness of Staging Chest CT in Breast Cancer: Evaluating Diagnostic Yield of Chest CT According to the Molecular Subtype and Clinical Stage. Journal of Clinical Medicine. 2021; 10(5):906. https://doi.org/10.3390/jcm10050906
Chicago/Turabian StyleYou, Seulgi, Tae Hee Kim, Doo Kyoung Kang, Kyung Joo Park, Young-Sil An, and Joo Sung Sun. 2021. "Usefulness of Staging Chest CT in Breast Cancer: Evaluating Diagnostic Yield of Chest CT According to the Molecular Subtype and Clinical Stage" Journal of Clinical Medicine 10, no. 5: 906. https://doi.org/10.3390/jcm10050906