
Relapse Patterns and Tailored Treatment Strategies for Malignant Pleural Mesothelioma Recurrence after Multimodality Therapy

Abstract
:1. Introduction
2. Material and Methods
2.1. Multimodality Treatment
2.2. Post-Operative Follow-Up, Diagnosis and Treatment of Recurrence
2.3. Statistical Analysis
3. Results
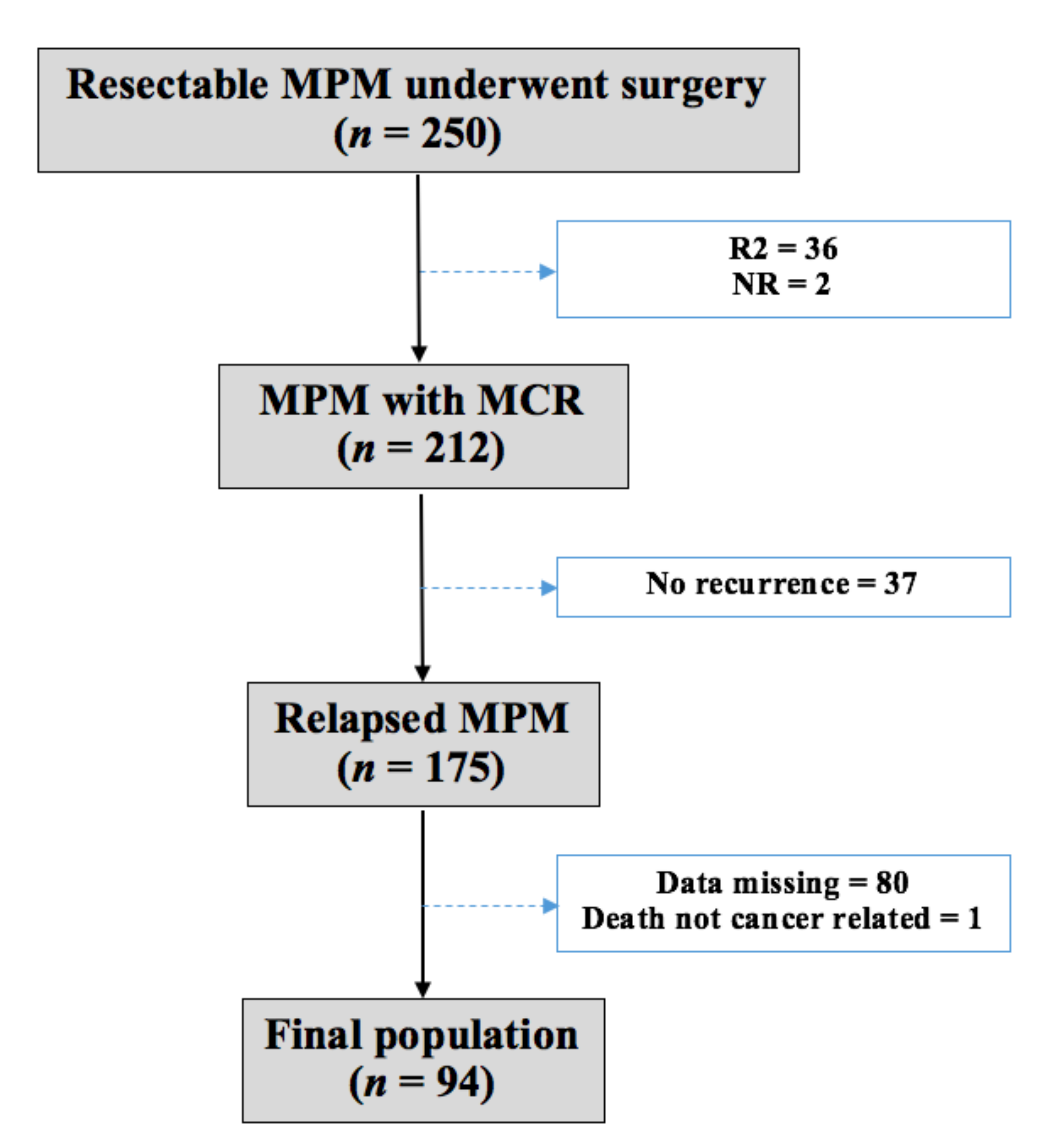
3.1. Patient Characteristics
3.2. Pattern and Treatment of Relapse
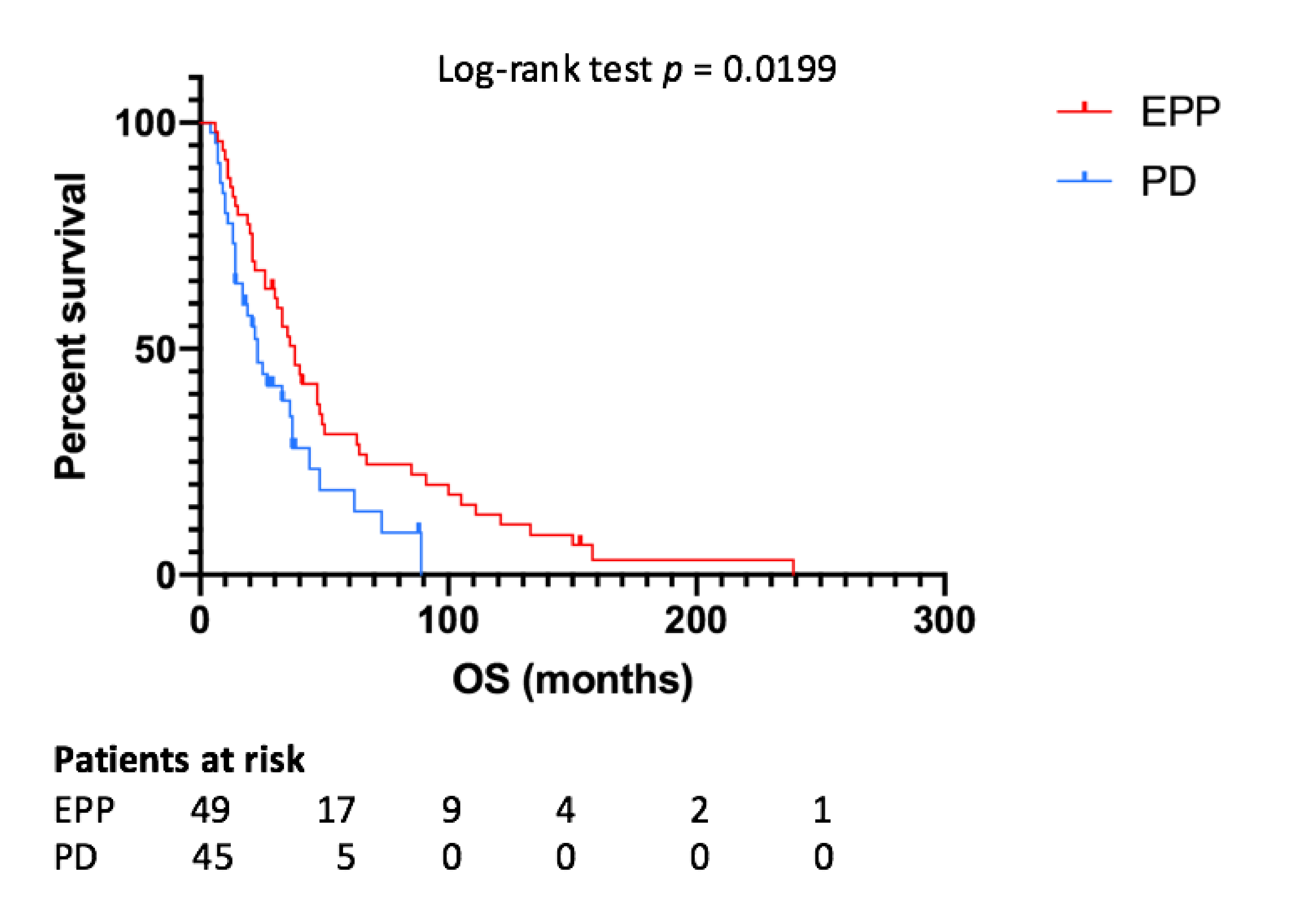
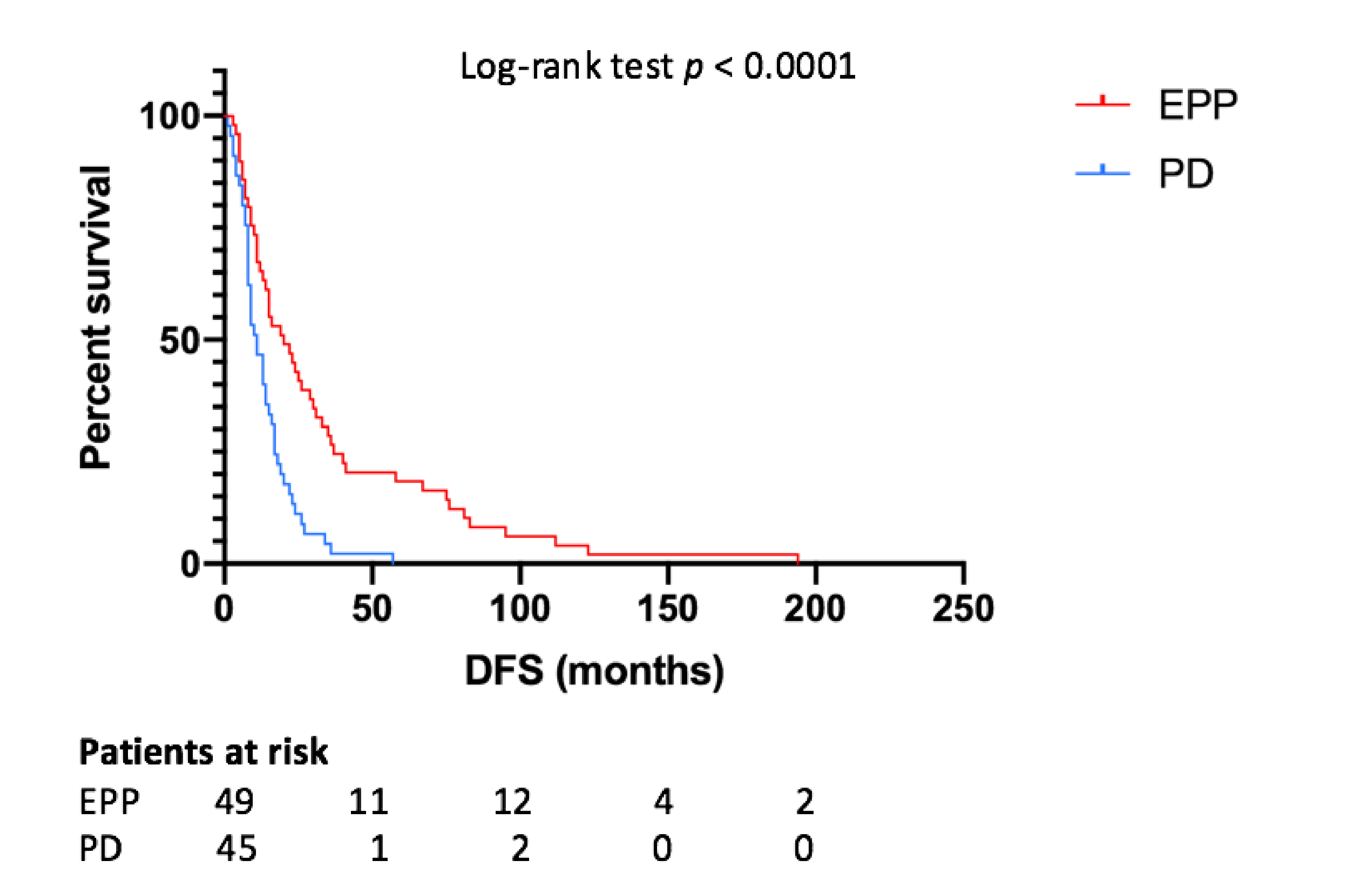
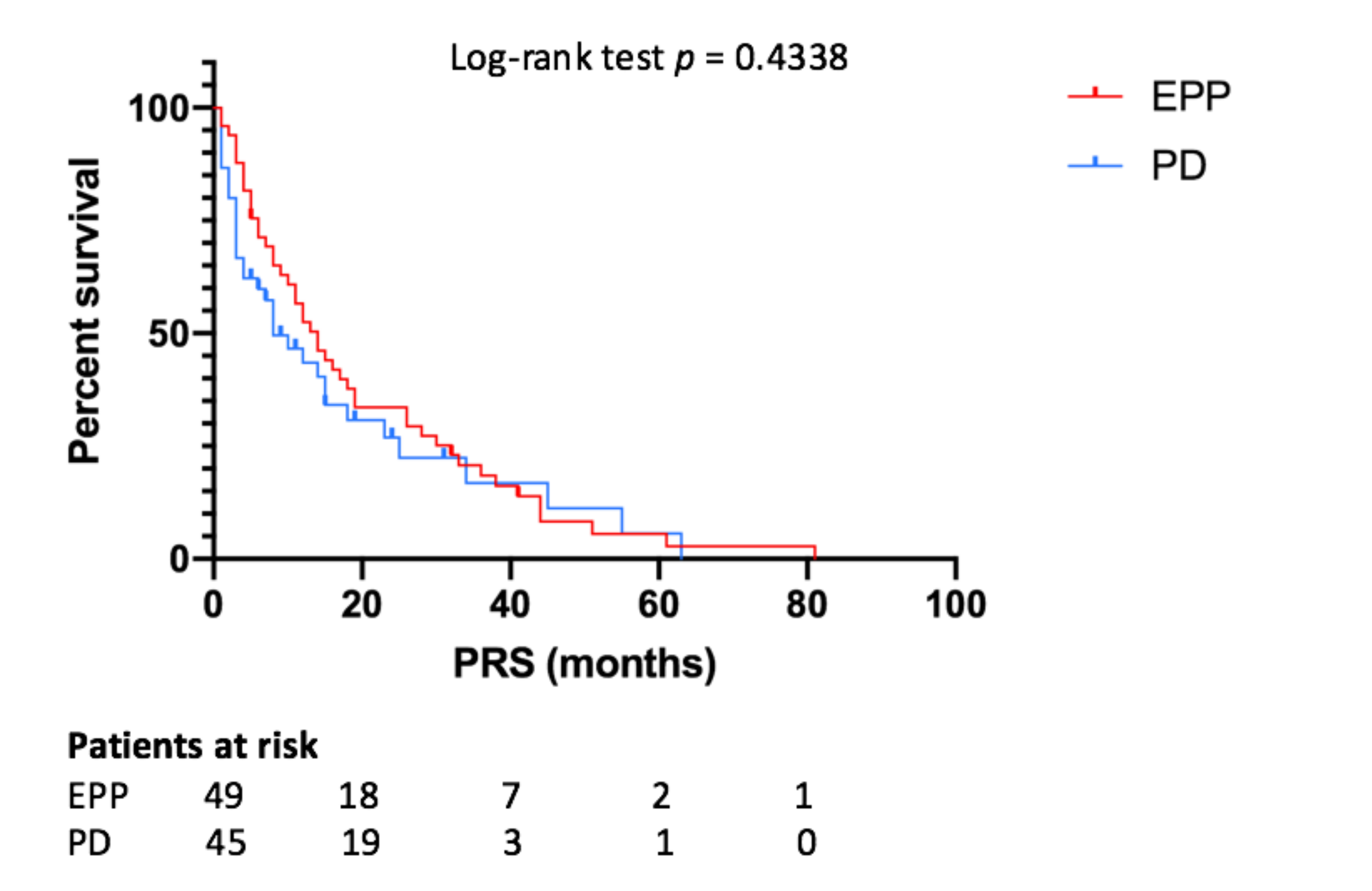
3.3. Survival Outcomes and Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Comprehensive Cancer Network. Malignant Pleural Mesothelioma (Version 1.2021). 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/mpm_blocks.pdf (accessed on 4 December 2020).
- Rusch, V.; Baldini, E.H.; Bueno, R.; De Perrot, M.; Flores, R.; Hasegawa, S.; Klepetko, W.; Krug, L.; Lang-Lazdunski, L.; Pass, H.; et al. The role of surgical cytoreduction in the treatment of malignant pleural mesothelioma: Meeting summary of the International Mesothelioma Interest Group Congress, September 11–14, 2012, Boston, Mass. J. Thorac. Cardiovasc. Surg. 2013, 145, 909–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldini, E.H.; Recht, A.; Strauss, G.M.; DeCamp, M.M.; Swanson, S.J.; Liptay, M.J.; Mentzer, S.J.; Sugarbaker, D.J. Patterns of failure after trimodality therapy for malignant pleural mesothelioma. Ann. Thorac. Surg. 1997, 63, 334–338. [Google Scholar] [CrossRef]
- Kostron, A.; Friess, M.; Crameri, O.; Inci, I.; Schneiter, D.; Hillinger, S.; Stahel, R.; Weder, W.; Opitz, I. Relapse pattern and second-line treatment following multimodality treatment for malignant pleural mesothelioma. Eur. J. Cardiothorac. Surg. 2016, 49, 1516–1523. [Google Scholar] [CrossRef] [PubMed]
- Takuwa, T.; Hashimoto, M.; Matsumoto, S.; Kondo, N.; Kuribayash, K.; Nakano, T.; Hasegawa, S. Post-recurrence chemotherapy for mesothelioma patients undergoing extrapleural pneumonectomy. Int. J. Clin. Oncol. 2017, 22, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Soldera, S.V.; Kavanagh, J.; Pintilie, M.; Leighl, N.B.; De Perrot, M.; Cho, J.; Hope, A.; Feld, R.; Bradbury, P.A. Systemic therapy use and outcomes after relapse from preoperative radiation and extrapleural pneumonectomy for malignant pleural mesothelioma. Oncologist 2019, 24, e510–e517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, A.; Takuwa, T.; Hashimoto, M.; Kuroda, A.; Nakamichi, T.; Matsumoto, S.; Kondo, N.; Kijima, T.; Yamakado, K.; Hasegawa, S. Clinical outcomes with recurrence after pleurectomy/decortications for malignant pleural mesothelioma. Ann. Thorac. Surg. 2020, 109, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Kai, Y.; Tsutani, Y.; Tsubokawa, N.; Ito, M.; Mimura, T.; Miyata, Y.; Okada, M. Prolonged post-recurrence survival following pleurectomy/decortications for malignant pleural mesothelioma. Oncol. Lett. 2019, 17, 3607–3614. [Google Scholar] [CrossRef] [PubMed]
- Bezenji, L.; Van Schil, P.E.; Carp, L. The eight TNM classification for malignant pleural mesothelioma. Transl. Lung Cancer Res. 2018, 7, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, S. Extrapleural pneumonectomy or pleurectomy/decortications for malignant pleural mesothelioma. Gen. Thorac. Cardiovasc. Surg. 2014, 62, 516–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores, R.M. Surgical options in malignant pleural mesothelioma: Extrapleural pneumonectomy or pleurectomy/decortication. Semin. Thorac. Cardiovasc. Surg. 2009, 21, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Marulli, G.; Faccioli, E.; Bellini, A.; Mammana, M.; Rea, F. Induction chemotherapy vs post-operative adjuvant therapy for malignant pleural mesothelioma. Exp. Rev. Respir. Med. 2017, 11, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, E.; Bellini, A.; Mammana, M.; Monaci, N.; Schiavon, M.; Rea, F. Extrapleural pneumonectomies for pleural mesothelioma. Exp. Rev. Respir. Med. 2020, 14, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Flores, R.M.; Pass, H.I.; Seshan, V.E.; Dycoco, J.; Zakowski, M.; Carbone, M.; Bains, M.S.; Rusch, V.W. Extrapleural pneumonectomy versus pleurectomy/decortications in the surgical management of malignant pleural mesothelioma: Results in 663 patients. J. Thorac. Cardiovasc. Surg. 2008, 135, 620–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichiki, Y.; Goto, H.; Fukuyama, T.; Nakanishi, K. Should lung-sparing surgery be the standard procedure for malignant pleural mesothelioma? J. Clin. Med. 2020, 9, 2153. [Google Scholar] [CrossRef] [PubMed]
- Politi, L.; Borzellino, G. Second surgery for recurrence of malignant pleural mesothelioma after extrapleural pneumonectomy. Ann. Thorac. Surg. 2010, 89, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Yano, T.; Haro, A.; Yoshida, T.; Kohno, M.; Maehara, Y. Treatment for recurrence after extrapleural pneumonectomy for malignant pleural mesothelioma: A single institution experience. Thorac. Cancer 2013, 4, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Burt, B.M.; Ali, S.O.; DaSilva, M.C.; Yeap, B.Y.; Richards, W.G.; Baldini, E.H.; Sugarbaker, D.J. Clinical indications and results after chest wall resection for recurrent mesothelioma. J. Thorac. Cardiovasc. Surg. 2013, 146, 1373–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baud, M.; Bobbio, A.; Lococo, F.; Regnard, J.F.; Alifano, M. Should we continue to offer extrapleural pneumonectomy to selected mesothelioma patients? A single center experience comparing surgical and non-surgical management. Jpn. J. Clin. Oncol. 2014, 44, 1127–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients n = 94 | EPP Group n = 49 | PD Group n = 45 | p-Value |
|---|---|---|---|---|
| Sex (male: female), n (%) | 69:25 (73.4:26.6) | 38:11 (77.5:22.5) | 31:14 (68.9:31.1) | 0.3612 |
| Age at surgery (years), median (IQR) | 64.7 (58–70) | 63 (58–68) | 69 (62.5–72) | 0.0026 |
| Histology, n (%) | 0.5571 | |||
| Epithelial | 81 (86.2) | 41 (83.7) | 40 (88.9) | |
| Sarcomatous | 1 (1.1) | 1 (2) | 0 (0) | |
| Biphasic | 10 (10.6) | 6 (12.3) | 4 (8.9) | |
| Desmoplastic | 2 (2.1) | 1 (2) | 1 (2.2) | |
| Side, n (%) | 0.3989 | |||
| Right | 58 (61.7) | 28 (57.1) | 30 (66.7) | |
| Left | 36 (38.3) | 21 (42.9) | 15 (33.3) | |
| CCI, n (IQR) | 4 (3–7) | 4 (3–7) | 4 (4–7) | 0.0745 |
| ECOG-PS | >0.9999 | |||
| 0 | 57 | 29 | 28 | |
| 1 | 29 | 14 | 15 | |
| FEV1%, n (IQR) | 77 (69–89) | 80 (69–88.5) | 76.5 (68.75–91.25) | 0.7624 |
| FVC%, n (IQR) | 77 (64–88) | 76 (62–81.5) | 79 (66.25–89.75) | 0.2386 |
| VC%, n (IQR) | 79 (67–87) | 79 (62.5–87) | 79.5 (69.75–92.25) | 0.4865 |
| TLC%, n (IQR) | 79 (72–89) | 79 (72–88.5) | 79.5 (70.75–90.5) | 0.6916 |
| DLCO%, n (IQR) | 68 (57.5–77) | 64 (52–75) | 69 (61–80) | 0.1386 |
| VO2 max (ml/kg/min), n (IQR) | 17.3 (15.88–21.1) | 17.15 (15.83–21.38) | 17.3 (15.88–21.1) | 0.933 |
| Pathological lung scintigraphy perfusion%, n (IQR) | 33.68 (26.82–39.38) | 29 (25.69–37) | 37.38 (29–43.64) | 0.024 |
| Pathological lung scintigraphy ventilation%, n (IQR) | 30.4 (20.5–38) | 28.94 (16.92–34.07) | 34.7 (22.95–44.39) | 0.0675 |
| Surgical intervention, n (%) | <0.0001 | |||
| Before 2012 | 45 (47.9) | 38 (77.6) | 7 (15.6) | |
| After 2012 | 49 (52.1) | 11 (22.5) | 38 (84.4) | |
| Pericardium resection, n (%) | <0.0001 | |||
| No | 20 (21.3) | 2 (4.1) | 18 (40) | |
| Yes | 3 (3.2) | 1 (2) | 2 (4.4) | |
| Yes, reconstruction with patch | 71 (75.5) | 46 (93.9) | 25 (55.6) | |
| Diaphragm resection, n (%) | 0.4733 | |||
| No | 8 (8.5) | 3 (6.1) | 5 (11.1) | |
| Yes, direct suture | 5 (5.3) | 0 (0) | 5 (11.1) | |
| Yes, reconstruction with patch | 81 (86.2) | 46 (93.9) | 35 (77.8) | |
| pT (TNM VIII edition), n (%) | 0.1921 | |||
| Complete remission | 2 (2.1) | 1 (2) | 1 (2.2) | |
| 1 | 5 (5.3) | 1 (2) | 4 (8.9) | |
| 2 | 24 (25.5) | 11 (22.5) | 13 (28.9) | |
| 3 | 45 (47.9) | 28 (57.1) | 17 (37.8) | |
| 4 | 18 (19.1) | 8 (16.3) | 10 (22.2) | |
| pN (TNM VIII edition), n (%) | >0.9999 | |||
| 0 | 71 (75.5) | 37 (75.5) | 34 (75.5) | |
| 1 | 23 (24.5) | 12 (24.5) | 11 (24.5) | |
| Pathological stage (TNM VIII edition), n (%) | 0.8244 | |||
| Complete remission | 2 (2.1) | 1 (2) | 1 (2.2) | |
| I | 57 (60.6) | 32 (65.3) | 25 (55.6) | |
| II | 7 (7.4) | 2 (4.1) | 5 (11.1) | |
| III | 13 (13.8) | 8 (16.3) | 5 (11.1) | |
| IV | 15 (16) | 6 (12.3) | 9 (20) | |
| Induction chemotherapy, n (%) | 0.2433 | |||
| No | 3 (3.2) | 3 | 0 (0) | |
| Yes | 91 (96.8) | 46 | 45 (100) | |
| Adjuvant chemotherapy, n (%) | 0.2537 | |||
| No | 87 (92.5) | 47 (95.9) | 40 (88.9) | |
| Yes | 7 (7.5) | 2 (4.1) | 5 (11.1) | |
| Adjuvant radiotherapy, n (%) | 0.1592 | |||
| No | 15 (16) | 5 (10.2) | 10 (22.2) | |
| Yes | 79 (84) | 44 (89.8) | 35 (77.8) | |
| Multimodality treatment, n (%) | 0.6012 | |||
| Bimodal | 18 (19.1) | 8 (16.3) | 10 (22.2) | |
| Trimodal | 76 (80.9) | 41 (83.7) | 35 (77.8) | |
| DFS, n (%) | 0.036 | |||
| <12 months | 39 (41.5) | 15 (30.6) | 24 (53.3) | |
| ≥12 months | 55 (58.5) | 34 (69.4) | 21 (46.7) | |
| Local failure only, n (%) | 0.0067 | |||
| No | 67 (71.3) | 41 (83.7) | 26 (57.8) | |
| Yes | 27 (28.7) | 8 (16.3) | 19 (42.2) | |
| Post-recurrence treatment, n (%) | 0.1361 | |||
| No | 13 (13.8) | 4 (8.2) | 9 (20) | |
| Yes | 81 (86.2) | 45 (91.8) | 36 (80) |
| n (%) | |
|---|---|
| Recurrence pattern | |
| Local | 27 (28.7) |
| Distant | 27 (28.7) |
| Local + distant | 40 (42.6) |
| Recurrence site | |
| Ipsilateral hemithorax | 27 (28.7) |
| Contralateral hemithorax | 18 (19.1) |
| Abdomen | 11 (11.7) |
| Thorax + abdomen | 26 (27.7) |
| Others | 12 (12.8) |
| Recurrence treatment | |
| None | 13 (13.8) |
| CT | 48 (51.1) |
| RT | 1 (1.1) |
| Surgery | 3 (3.2) |
| CT + Surgery | 6 (6.4) |
| CT + RT | 9 (9.6) |
| CT + RT + Surgery | 3 (3.2) |
| CT + Other | 7 (7.4) |
| CT + RT + Other | 1 (1.1) |
| Other | 3 (3.2) |
| p-Value | HR | IC95% | |
|---|---|---|---|
| OS | |||
| EPP | 0.011 | 0.524 | 0.318–0.863 |
| Epithelial histology | 0.001 | 0.341 | 0.182–0.639 |
| Trimodality treatment | 0.012 | 0.419 | 0.212–0.826 |
| Induction chemotherapy | 0.017 | 0.151 | 0.032–0.711 |
| DFS | |||
| EPP | 0.001 | 0.446 | 0.281–0.708 |
| Epithelial histology | 0.02 | 0.489 | 0.268–0.893 |
| Trimodality treatment | 0.001 | 0.35 | 0.189–0.649 |
| Pathological stage I | 0.015 | 0.727 | 0.563–0.939 |
| Induction chemotherapy | 0.012 | 0.165 | 0.040–0.672 |
| Adjuvant chemotherapy | 0.007 | 0.302 | 0.126–0.726 |
| Adjuvant radiotherapy | 0.004 | 0.424 | 0.238–0.755 |
| PRS | |||
| Epithelial histology | 0.026 | 0.491 | 0.263–0.916 |
| Local failure | 0.027 | 0.707 | 0.521–0.961 |
| DFS ≥ 12 months | 0.006 | 0.298 | 0.137–0.812 |
| Post-recurrence medical treatment | 0.046 | 0.101 | 0.897–0.936 |
| Author | Surgery, n | Multimodality, n | Relapse, n (%) | Pattern of Recurrence, % | Median DFS (m) | Relapse Treatment, n (%) | Median PRS (m) | Median OS (m) |
|---|---|---|---|---|---|---|---|---|
| Kostron, 2015 [4] | EPP, 136 | Bimodal, 47 Trimodal, 59 | 106 (77.9) | L 24.3 D 19.9 L + D 33.8 | 9 | None, 28 (26.4) Surgery, 16 (15.1) Medical treatment, 73 (68.9) | 7 | 22 b |
| Takuwa, 2017 [5] | EPP, 59 | Bimodal, 27 Trimodal, 12 | 39 (66.1) | NR | 11.6 | None, 12 (30.7) Medical treatment, 27 (69.2) | 6.5 | 22 |
| Kai, 2018 [8] | EPP, 29 PD, 15 | Bimodal, 26 Trimodal, 18 | 32 (72.7) | L 18.2 D 27.3 L + D 27.3 | Overall, 14 c EPP, 13 c PD, 21 c | Medical treatment, 17 (53.1) | Overall, 5 EPP, 3 PD, 20 | Overall, 22 c EPP, 17 c PD, 34 c |
| Soldera, 2019 [6] | EPP, 93 | Bimodal 43 Trimodal 10 | 53 (57.0) | L 5.4 D 38.7 L + D 12.9 | NR | None, 27 (50.9) Medical treatment, 15 (28.3) NR, 11 (20.8) | 4.8 | NR |
| Nakamura, 2020 [7] | PD, 90 | Bimodal, 90 | 57 (63.3) | L 43 D 6.7 L + D 13.3 | 19 | Surgery, 3 (5.3) Medical treatment, 40 (70.2) Best supportive care, 14 (24.5) | 14.4 | 57 |
| Politi, 2010 [16] | EPP, 8 | NR | 8 (100) | L 50 D 50 | NR | Surgery, 8 (100) | 14.5 | NR |
| Okamoto, 2013 [17] | EPP, 10 | NR | 8 (80) | L 40 D 40 | 15.4 | Surgery, 2 (25) Medical treatment, 6 (75) | 17.8 | 49.6 a |
| Burt, 2012 [18] | EPP, 32 PD, 15 | NR | 47 (100) | L 100 | 16.1 | Surgery, 47 (100) | Epithelial, 20.4 Biphasic, 7.0 | 44.9 |
| Present series | EPP, 49 PD, 45 | Bimodal, 18 Trimodal, 76 | 94 (100) | L, 28.7 D, 28.7 L + D, 42.6 | Overall, 14 EPP, 20 PD, 11 | None, 13 (13.8) Surgery, 13 (13.8) Medical treatment, 68 (72.3) | Overall, 12 EPP, 14 PD, 8 | Overall, 33 EPP, 38 PD, 23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, A.; Dell’Amore, A.; Terzi, S.; Zambello, G.; Zuin, A.; Pasello, G.; Calabrese, F.; Schiavon, M.; Rea, F. Relapse Patterns and Tailored Treatment Strategies for Malignant Pleural Mesothelioma Recurrence after Multimodality Therapy. J. Clin. Med. 2021, 10, 1134. https://doi.org/10.3390/jcm10051134
Bellini A, Dell’Amore A, Terzi S, Zambello G, Zuin A, Pasello G, Calabrese F, Schiavon M, Rea F. Relapse Patterns and Tailored Treatment Strategies for Malignant Pleural Mesothelioma Recurrence after Multimodality Therapy. Journal of Clinical Medicine. 2021; 10(5):1134. https://doi.org/10.3390/jcm10051134
Chicago/Turabian StyleBellini, Alice, Andrea Dell’Amore, Stefano Terzi, Giovanni Zambello, Andrea Zuin, Giulia Pasello, Fiorella Calabrese, Marco Schiavon, and Federico Rea. 2021. "Relapse Patterns and Tailored Treatment Strategies for Malignant Pleural Mesothelioma Recurrence after Multimodality Therapy" Journal of Clinical Medicine 10, no. 5: 1134. https://doi.org/10.3390/jcm10051134