
Integrating Muscle Health in Predicting the Risk of Asymptomatic Vertebral Fracture in Older Adults

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects
2.2. Anthropometric Measurements
2.3. Bone Fragility Evaluation
Imaging Protocols
2.4. Fracture Evaluations
Imaging Protocol
2.5. Muscle Health Evaluation
2.5.1. Imaging Protocols
2.5.2. Handgrip Strength Assessment
2.5.3. Definition of Sarcopenia
2.6. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Associations between Muscle Health and Bone Quantity and Quality
3.2.1. Male Participants
3.2.2. Female Participants
3.3. Comparison of Participants with and without Asymptomatic Vertebral Fractures
3.3.1. Male Participants
3.3.2. Female Participants
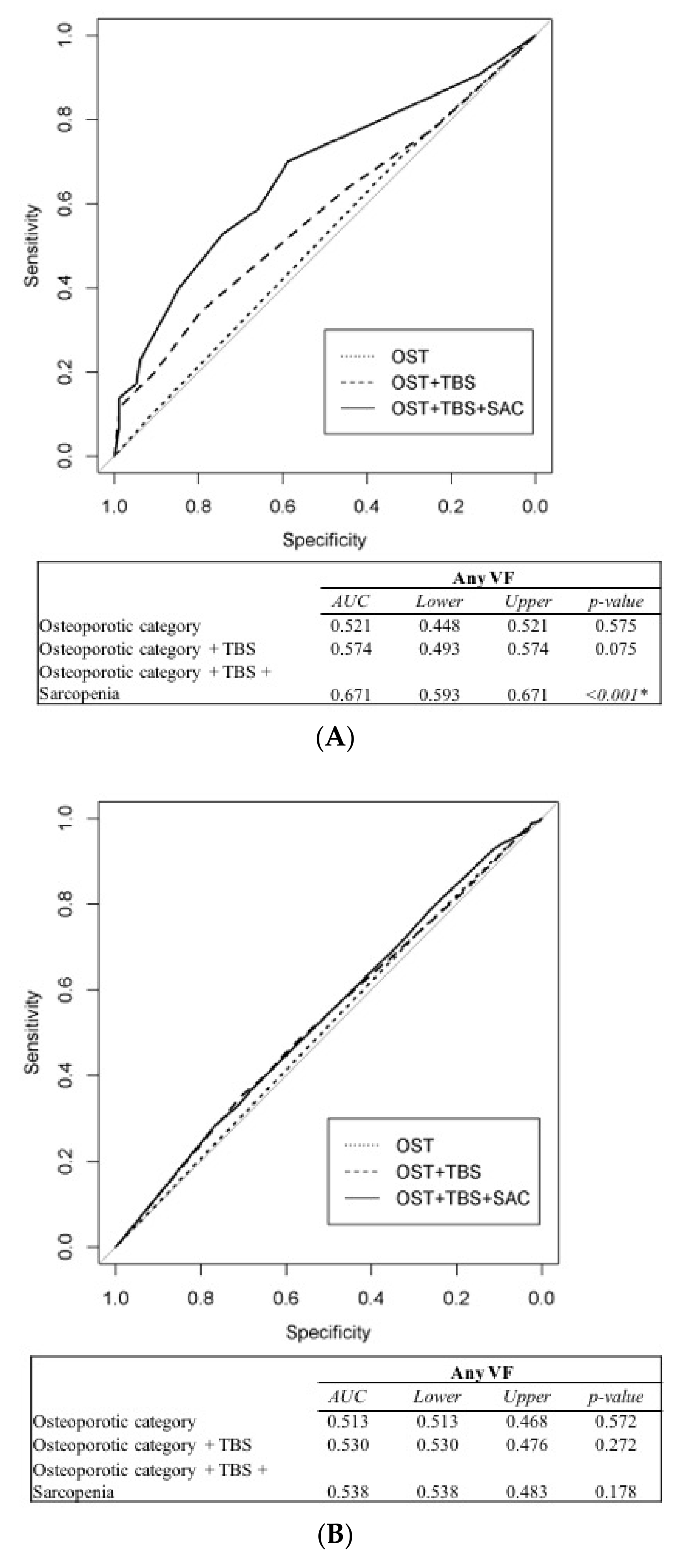
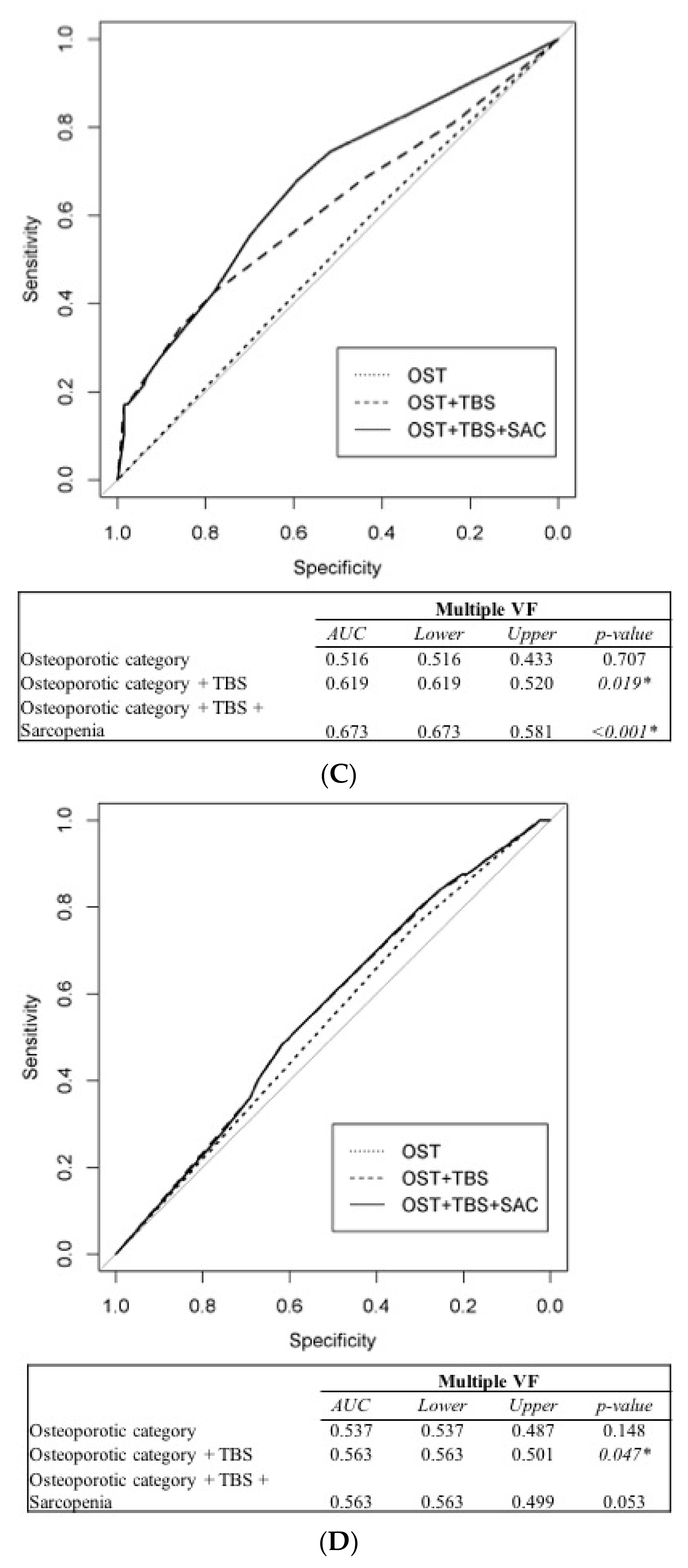
3.4. Prediction of Vertebral Fracture Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef]
- Cauley, J.A.; Palermo, L.; Vogt, M.; Ensrud, K.E.; Ewing, S.; Hochberg, M.; Nevitt, M.C.; Black, D.M. Prevalent Vertebral Fractures in Black Women and White Women. J. Bone Miner. Res. 2008, 23, 1458–1467. [Google Scholar] [CrossRef]
- Guglielmi, G.; Diacinti, D.; Van Kuijk, C.; Aparisi, F.; Krestan, C.; Adams, J.E.; Link, T.M. Vertebral morphometry: Current methods and recent advances. Eur. Radiol. 2008, 18, 1484–1496. [Google Scholar] [CrossRef]
- Lindsay, R.; Pack, S.; Li, Z. Longitudinal progression of fracture prevalence through a population of postmenopausal women with osteoporosis. Osteoporos. Int. 2004, 16, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Diacinti, D.; Guglielmi, G.; Pisani, D.; Argirò, R.; Serafini, C.; Romagnoli, E.; Minisola, S.; Catalano, C.; David, V. Vertebral morphometry by dual-energy X-ray absorptiometry (DXA) for osteoporotic vertebral fractures assessment (VFA). Radiol. Med. 2012, 117, 1374–1385. [Google Scholar] [CrossRef]
- Bhat, K.A.; Kakaji, M.; Awasthi, A.; Shukla, M.; Dubey, M.; Srivastava, R.; Singh, U.; Gupta, S.K. High Prevalence of Osteoporosis and Morphometric Vertebral Fractures in Indian Males Aged 60 Years and Above: Should Age for Screening Be Lowered? J. Clin. Densitom. 2018, 21, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Ho-Pham, L.T.; Mai, L.D.; Pham, H.N.; Nguyen, N.D.; Nguyen, T.V. Reference ranges for vertebral heights and prevalence of asymptomatic (undiagnosed) vertebral fracture in Vietnamese men and women. Arch. Osteoporos. 2012, 7, 257–266. [Google Scholar] [CrossRef]
- Imai, N.; Endo, N.; Hoshino, T.; Suda, K.; Miyasaka, D.; Ito, T. Mortality after hip fracture with vertebral compression fracture is poor. J. Bone Miner. Metab. 2014, 34, 51–54. [Google Scholar] [CrossRef]
- National Institute of Health. Consensus Development Panel on Osteoporosis Prevention D, Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001, 285, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-C.; Wu, J.; Kuo, S.-F.; Cheung, Y.-C.; Sung, C.-M.; Fan, C.-M.; Chen, F.-P.; Mhuircheartaigh, J.N. Vertebral Fractures in Type 2 Diabetes Patients: Utility of Trabecular Bone Score and Relationship With Serum Bone Turnover Biomarkers. J. Clin. Densitom. 2020, 23, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Dhaliwal, R.; Cibula, D.; Ghosh, C.; Weinstock, R.S.; Moses, A.M. Bone quality assessment in type 2 diabetes mellitus. Osteoporos. Int. 2014, 25, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Aubry-Rozier, B.; Lamy, O.; Hans, D.; Program, F.T.M.B.D. TBS (Trabecular Bone Score) and Diabetes-Related Fracture Risk. J. Clin. Endocrinol. Metab. 2013, 98, 602–609. [Google Scholar] [CrossRef] [Green Version]
- Verschueren, S.; Gielen, E.; O’Neill, T.W.; Pye, S.R.; Adams, J.E.; Ward, K.A.; Wu, F.C.; Szulc, P.; Laurent, M.; Claessens, F.; et al. Sarcopenia and its relationship with bone mineral density in middle-aged and elderly European men. Osteoporos. Int. 2013, 24, 87–98. [Google Scholar] [CrossRef]
- Miyakoshi, N.; Hongo, M.; Mizutani, Y.; Shimada, Y. Prevalence of sarcopenia in Japanese women with osteopenia and osteoporosis. J. Bone Miner. Metab. 2013, 31, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Chalhoub, D.; Cawthon, P.M.; Ensrud, K.E.; Stefanick, M.L.; Kado, D.M.; Boudreau, R.M.; Greenspan, S.L.; Newman, A.B.; Zmuda, J.M.; Orwoll, E.S.; et al. Risk of Nonspine Fractures in Older Adults with Sarcopenia, Low Bone Mass, or Both. J. Am. Geriatr. Soc. 2015, 63, 1733–1740. [Google Scholar] [CrossRef] [Green Version]
- Binkley, N.; Buehring, B. Beyond FRAX: It’s time to consider “sarco-osteopenia”. J. Clin. Densitom. 2009, 12, 413–416. [Google Scholar] [CrossRef]
- Wang, W.-F.; Lin, C.-W.; Xie, C.-N.; Liu, H.-T.; Zhu, M.-Y.; Huang, K.-L.; Teng, H.-L. The association between sarcopenia and osteoporotic vertebral compression refractures. Osteoporos. Int. 2019, 30, 2459–2467. [Google Scholar] [CrossRef]
- Langsetmo, L.; Vo, T.N.; Ensrud, K.E.; Taylor, B.C.; Cawthon, P.M.; Schwartz, A.V.; Bauer, D.C.; Orwoll, E.S.; Lane, N.E.; Barrett-Connor, E.; et al. The Association Between Trabecular Bone Score and Lumbar Spine Volumetric BMD Is Attenuated Among Older Men With High Body Mass Index. J. Bone Miner. Res. 2016, 31, 1820–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. Osteoporos. Int. 1994, 4, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Rubin, M.R.; Patsch, J.M. Assessment of bone turnover and bone quality in type 2 diabetic bone disease: Current concepts and future directions. Bone Res. 2016, 4, 16001. [Google Scholar] [CrossRef]
- Schousboe, J.T.; Vo, T.N.; Langsetmo, L.; Taylor, B.C.; Cawthon, P.M.; Schwartz, A.V.; Bauer, D.C.; Orwoll, E.S.; Lane, N.E.; Barrett-Connor, E.; et al. Association of Trabecular Bone Score (TBS) With Incident Clinical and Radiographic Vertebral Fractures Adjusted for Lumbar Spine BMD in Older Men: A Prospective Cohort Study. J. Bone Miner. Res. 2017, 32, 1554–1558. [Google Scholar] [CrossRef]
- Genant, H.K.; Wu, C.Y.; Van Kuijk, C.; Nevitt, M.C. Vertebral fracture assessment using a semiquantitative technique. J. Bone Miner. Res. 2009, 8, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Hangartner, T.N.; Warner, S.; Braillon, P.; Jankowski, L.; Shepherd, J. The Official Positions of the International Society for Clinical Densitometry: Acquisition of Dual-Energy X-Ray Absorptiometry Body Composition and Considerations Regarding Analysis and Repeatability of Measures. J. Clin. Densitom. 2013, 16, 520–536. [Google Scholar] [CrossRef]
- Chen, L.-K.; Lee, W.-J.; Peng, L.-N.; Liu, L.-K.; Arai, H.; Akishita, M. Recent Advances in Sarcopenia Research in Asia: 2016 Update From the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2016, 17, 767.e1–767.e7. [Google Scholar] [CrossRef]
- Locquet, M.; Beaudart, C.; Reginster, J.-Y.; Bruyère, O. Association Between the Decline in Muscle Health and the Decline in Bone Health in Older Individuals from the SarcoPhAge Cohort. Calcif. Tissue Int. 2019, 104, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Sheng, Y.; Chen, S.; Wang, S.; Zhang, A.; Cai, J.; Lai, B.; Ding, G. Bone mineral density and trabecular bone score in Chinese subjects with sarcopenia. Aging Clin. Exp. Res. 2019, 31, 1549–1556. [Google Scholar] [CrossRef] [Green Version]
- Bijlsma, A.Y.; Meskers, M.C.G.; Molendijk, M.; Westendorp, R.G.J.; Sipilä, S.; Stenroth, L.; Sillanpää, E.; McPhee, J.S.; Jones, D.A.; Narici, M.; et al. Diagnostic measures for sarcopenia and bone mineral density. Osteoporos. Int. 2013, 24, 2681–2691. [Google Scholar] [CrossRef]
- He, H.; Liu, Y.; Tian, Q.; Papasian, C.J.; Hu, T.; Deng, H.-W. Relationship of sarcopenia and body composition with osteoporosis. Osteoporos. Int. 2016, 27, 473–482. [Google Scholar] [CrossRef]
- Wagner, P.; Chapurlat, R.; Ecochard, R.; Szulc, P. Low Muscle Strength and Mass Is Associated With the Accelerated Decline of Bone Microarchitecture at the Distal Radius in Older Men: The Prospective STRAMBO Study. J. Bone Miner. Res. 2018, 33, 1630–1640. [Google Scholar] [CrossRef] [Green Version]
- Yuki, A.; Ando, F.; Otsuka, R.; Shimokata, H. Sarcopenia based on the Asian Working Group for Sarcopenia criteria and all-cause mortality risk in older Japanese adults. Geriatr. Gerontol. Int. 2017, 17, 1642–1647. [Google Scholar] [CrossRef]
- Anand, A.; Shetty, A.P.; Renjith, K.R.; Kanna, R.M.; Rajasekaran, S. Does Sarcopenia Increase the Risk for Fresh Vertebral Fragility Fractures?: A Case-Control Study. Asian Spine J. 2020, 14, 17–24. [Google Scholar] [CrossRef]
- Hida, T.; Shimokata, H.; Sakai, Y.; Yoshihito, S.; Matsui, Y.; Takemura, M.; Kasai, T.; Ishiguro, N.; Harada, A. Sarcopenia and sarcopenic leg as potential risk factors for acute osteoporotic vertebral fracture among older women. Eur. Spine J. 2016, 25, 3424–3431. [Google Scholar] [CrossRef] [PubMed]
- Trajanoska, K.; Schoufour, J.D.; Darweesh, S.K.; Benz, E.; Medina-Gomez, C.; Alferink, L.J.; LaHousse, L.; Brusselle, G.; Stricker, B.; Murad, S.D.; et al. Sarcopenia and Its Clinical Correlates in the General Population: The Rotterdam Study. J. Bone Miner. Res. 2018, 33, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Kubo, A.; Ishimura, K.; Fukui, T.; Tamura, T. Correlation among sarcopenia, malnutrition and activities of daily living in patients with vertebral compression fractures: A comparison based on admission and discharge parameters evaluating these conditions. J. Phys. Ther. Sci. 2018, 30, 1401–1407. [Google Scholar] [CrossRef] [Green Version]
- Ignasiak, D.; Valenzuela, W.; Reyes, M.; Ferguson, S.J. The effect of muscle ageing and sarcopenia on spinal segmental loads. Eur. Spine J. 2018, 27, 2650–2659. [Google Scholar] [CrossRef]
- Harris, R.; Chang, Y.; Beavers, K.; Laddu-Patel, D.; Bea, J.; Johnson, K.; LeBoff, M.; Womack, C.; Wallace, R.; Li, W.; et al. Risk of Fracture in Women with Sarcopenia, Low Bone Mass, or Both. J. Am. Geriatr. Soc. 2017, 65, 2673–2678. [Google Scholar] [CrossRef] [PubMed]
- Hong, N.; Kim, C.O.; Youm, Y.; Choi, J.-Y.; Kim, H.C.; Rhee, Y. Dysmobility syndrome is associated with prevalent morphometric vertebral fracture in older adults: The Korean Urban-Rural Elderly (KURE) study. Arch. Osteoporos. 2018, 13, 86. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Male (n = 186) | Female (n = 414) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Num. of Patients | % | Mean | SD | Num. of Patients | % | Mean | SD | p-Value | |
| Age (years) | 74.30 | 7.14 | 72.82 | 7.37 | 0.02 | ||||
| Weight (kg) | 63.00 | 10.26 | 55.20 | 8.89 | <0.001 * | ||||
| Height (cm) | 161.92 | 6.59 | 151.90 | 5.83 | <0.001 * | ||||
| BMI (kg/m2) | 24.00 | 3.44 | 23.90 | 3.50 | 0.75 | ||||
| TFM (kg) | 18.33 | 5.69 | 21.07 | 9.72 | <0.001 * | ||||
| TLM (kg) | 41.85 | 5.89 | 32.12 | 4.75 | <0.001 * | ||||
| TBMC (kg) | 2.30 | 0.39 | 1.66 | 0.26 | <0.001 * | ||||
| ASMI (kg/m2) | 6.93 | 0.98 | 5.88 | 0.79 | <0.001 * | ||||
| Risk of fall | 9 | 4.8 | 37 | 9.0 | 0.11 | ||||
| Vertebral fractures | |||||||||
| Any VF | 87 | 47.0 | 170 | 41.4 | 0.23 | ||||
| w sarcopenia | 43 | 49.4 | 22 | 12.9 | <0.001 * | ||||
| w/o sarcopenia | 44 | 50.6 | 148 | 87.1 | |||||
| Multiple VFs | 47 | 25.4 | 89 | 21.7 | 0.37 | ||||
| w sarcopenia | 23 | 48.9 | 13 | 14.6 | <0.001 * | ||||
| w/o sarcopenia | 24 | 51.1 | 76 | 85.4 | |||||
| Bone quantity (osteoporotic category) | <0.001 * | ||||||||
| Normal | 16 | 8.6 | 8 | 1.9 | |||||
| Osteopenia | 60 | 32.3 | 111 | 27.0 | |||||
| Osteoporosis | 110 | 59.1 | 292 | 71.0 | |||||
| Bone quality (trabecular bone score) | <0.001 * | ||||||||
| Normal | 92 | 49.7 | 39 | 9.5 | |||||
| Partially degraded | 83 | 44.9 | 217 | 52.8 | |||||
| Fully Degraded | 10 | 5.4 | 155 | 37.7 | |||||
| Muscle health | |||||||||
| Low ASMI | 101 | 54.3 | 117 | 28.3 | <0.001 * | ||||
| Low HS | 105 | 56.5 | 197 | 47.9 | 0.07 | ||||
| Sarcopenia | 68 | 36.6 | 58 | 14.1 | <0.001 * | ||||
| Osteoporotic Category | Normal | Osteopenia | Osteoporosis | p-Value | |||
|---|---|---|---|---|---|---|---|
| Males | Mean | Mean | Mean | ||||
| Age (years), SD | 74.56 | 6.60 | 74.45 | 6.84 | 74.18 | 7.44 | 0.962 |
| Weight (kg), SD | 73.63 ^ | 11.04 | 66.59 ^^ | 9.06 | 59.49 ^^^ | 9.03 | <0.001 * |
| Height (cm), SD | 163.85 | 5.94 | 163.61 ^^ | 6.25 | 160.72 | 6.64 | 0.01 * |
| BMI (kg/m2), SD | 27.41 ^ | 3.67 | 24.86 ^^ | 2.99 | 23.04 ^^^ | 3.22 | <0.001 * |
| TFM (kg), SD | 23.33 ^ | 5.64 | 19.52 ^^ | 4.97 | 16.95 ^^^ | 5.55 | <0.001 * |
| TLM (kg), SD | 46.95 | 6.64 | 43.93 ^^ | 5.37 | 39.97 ^^^ | 5.24 | <0.001 * |
| Risk of fall (n), % | 2 ^ | 13% | 0 | 0% | 7 | 6% | 0.022 * |
| Muscle health | |||||||
| Low ASMI (n), % | 4 | 25% | 27 | 45% ^^ | 70 | 64% ^^^ | 0.003 * |
| Low HS (n), % | 9 | 56% | 27 | 45% | 69 | 63% | 0.085 |
| Sarcopenia (n), % | 3 | 19% | 13 | 22% ^^ | 52 | 47% | 0.001 * |
| Females | Mean | Mean | Mean | ||||
| Age (years), SD | 69.50 | 6.91 | 71.25 ^^ | 6.10 | 73.50 | 7.72 | 0.01 * |
| Weight (kg), SD | 62.73 ^ | 5.98 | 58.57 ^^ | 9.26 | 53.72 ^^^ | 8.36 | <0.001 * |
| Height (cm), SD | 157.31 ^ | 6.66 | 153.42 ^^ | 5.51 | 151.17 ^^^ | 5.76 | <0.001 * |
| BMI (kg/m2), SD | 25.38 | 2.42 | 24.9 ^^ | 3.81 | 23.49 | 3.32 | 0.001 * |
| TFM (kg), SD | 23.35 | 3.84 | 22.48 | 6.20 | 20.47 | 10.82 | 0.145 |
| TLM (kg), SD | 36.23 | 4.81 | 33.39 ^^ | 4.86 | 31.53 ^^^ | 4.57 | <0.001 * |
| Risk of fall (n), % | 0 | 0% | 8 | 7% | 29 | 10% | 0.628 |
| Muscle health | |||||||
| Low ASMI (n), % | 2 | 25% | 29 | 26% | 86 | 29% | 0.859 |
| Low HS (n), % | 5 | 63% | 38 | 34% ^^ | 154 | 53% | 0.002 * |
| Sarcopenia (n), % | 0 | 0% | 11 | 10% | 47 | 16% | 0.209 |
| Trabecular Bone Score | Normal | Partially Degraded | Fully Degraded | p-Value | |||
| Males | Mean | Mean | Mean | ||||
| Age (years), SD | 73.80 | 7.28 | 74.86 | 7.08 | 75.20 | 6.36 | 0.580 |
| Weight (kg), SD | 65.05 ^ | 10.75 | 61.33 | 9.48 | 57.27 | 8.20 | 0.011 * |
| Height (cm), SD | 162.36 | 6.02 | 161.70 | 7.06 | 158.45 | 6.34 | 0.193 |
| BMI (kg/m2), SD | 24.64 | 3.62 | 23.45 | 3.20 | 22.82 | 3.01 | 0.039 * |
| TFM (kg), SD | 18.46 | 5.78 | 18.42 | 5.67 | 15.96 | 4.98 | 0.409 |
| TLM (kg), SD | 43.29 ^ | 6.02 | 40.72 | 5.39 | 38.08 ^^^ | 5.89 | 0.002 * |
| Risk of fall (n), % | 4 | 4% | 5 | 6% | 0 | 0% | 0.843 |
| Muscle health | |||||||
| Low ASMI (n), % | 44 | 48% | 48 | 58% | 8 | 80% | 0.113 |
| Low HS (n), % | 50 | 54% | 47 | 57% | 8 | 80% | 0.334 |
| Sarcopenia (n), % | 29 | 32% | 32 | 39% | 7 | 70% | 0.053 |
| Females | Mean | Mean | Mean | ||||
| Age (years), SD | 70.36 | 5.67 | 72.56 | 7.49 | 73.80 ^^^ | 7.44 | 0.025 * |
| Weight (kg), SD | 59.85 ^ | 8.70 | 55.53 | 8.35 | 53.58 ^^^ | 9.25 | <0.001 * |
| Height (cm), SD | 152.97 | 7.36 | 152.04 | 5.67 | 151.43 | 5.62 | 0.297 |
| BMI (kg/m2), SD | 25.60 ^ | 3.48 | 24.01 | 3.35 | 23.33 ^^^ | 3.59 | 0.001 * |
| TFM (kg), SD | 22.73 | 5.49 | 21.67 | 11.88 | 19.80 | 6.58 | 0.099 |
| TLM (kg), SD | 33.11 | 6.30 | 32.53 ^^ | 4.08 | 31.31 | 5.08 | 0.02 * |
| Risk of fall (n), % | 3 | 8% | 15 | 7% | 19 | 12% | 0.203 |
| Muscle health | |||||||
| Low ASMI (n), % | 7 | 18% | 57 | 26% | 53 | 34% | 0.077 |
| Low HS (n), % | 16 | 41% | 93 | 43% ^^ | 88 | 57% | 0.020 * |
| Sarcopenia (n), % | 3 | 8% | 25 | 12% ^^ | 30 | 19% | 0.049 * |
| Any VF | No VF | p-Value | Multiple VFs | No Multiple VFs | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Males | ||||||||||
| Age (years), SD | 75.47 | 7.99 | 73.23 | 6.19 | 0.034 * | 76.23 | 8.37 | 73.62 | 6.60 | 0.03 * |
| Weight (kg), SD | 62.07 | 9.82 | 63.73 | 10.65 | 0.271 | 62.02 | 10.00 | 63.27 | 10.38 | 0.467 |
| Height (cm), SD | 161.30 | 6.34 | 162.39 | 6.78 | 0.260 | 160.39 | 6.91 | 162.38 | 6.41 | 0.086 |
| BMI (kg/m2), SD | 23.84 | 3.23 | 24.14 | 3.65 | 0.547 | 24.08 | 3.28 | 23.97 | 3.52 | 0.839 |
| TFM (kg), SD | 18,227.28 | 5787.95 | 18,409.71 | 5651.66 | 0.829 | 18,399.63 | 5727.10 | 18,298.13 | 5713.17 | 0.917 |
| TLM (kg), SD | 41,008.78 | 5745.54 | 42,528.63 | 5950.84 | 0.079 | 40,795.42 | 6072.50 | 42,160.76 | 5806.37 | 0.182 |
| Risk of fall (n), % | 7 | 8% | 2 | 2% | 0.086 | 3 | 6% | 6 | 4% | 0.695 |
| Bone quantity | ||||||||||
| Bone mineral density (g/cm2) | 0.77 | 0.11 | 0.77 | 0.13 | 0.882 | 0.79 | 0.11 | 0.76 | 0.12 | 0.372 |
| Bone quality | ||||||||||
| Trabecular bone score | 1.33 | 0.10 | 1.36 | 0.08 | 0.032 * | 1.32 | 0.11 | 1.36 | 0.08 | 0.009 * |
| Muscle health | ||||||||||
| Low ASMI (n), % | 57 | 66% | 44 | 45% | 0.008 * | 30 | 64% | 71 | 51% | 0.193 |
| Low HS (n), % | 62 | 71% | 42 | 43% | <0.001 * | 31 | 66% | 73 | 53% | 0.165 |
| Sarcopenia (n), % | 43 | 49% | 25 | 26% | 0.001 * | 23 | 49% | 45 | 33% | 0.067 |
| Females | ||||||||||
| Age (years), SD | 74.82 | 7.72 | 71.41 | 6.78 | <0.001 * | 76.88 | 7.99 | 71.70 | 6.78 | <0.001 * |
| Weight (kg), SD | 55.29 | 8.67 | 55.14 | 9.05 | 0.863 | 54.35 | 8.09 | 55.44 | 9.09 | 0.278 |
| Height (cm), SD | 151.60 | 5.83 | 152.11 | 5.84 | 0.388 | 150.73 | 6.04 | 152.22 | 5.74 | 0.039 * |
| BMI (kg/m2), SD | 24.03 | 3.35 | 23.82 | 3.61 | 0.546 | 23.92 | 3.24 | 23.90 | 3.58 | 0.967 |
| TFM (kg), SD | 21,619.22 | 13,324.25 | 20,681.37 | 6003.69 | 0.336 | 19,894.98 | 6084.48 | 21,393.87 | 10,490.67 | 0.198 |
| TLM (kg), SD | 32,111.69 | 5307.66 | 32,134.30 | 4330.71 | 0.962 | 31,929.38 | 4850.85 | 32,179.00 | 4731.80 | 0.666 |
| Risk of fall (n), % | 19 | 11% | 18 | 7% | 0.263 | 11 | 12% | 26 | 8% | 0.298 |
| Bone quantity | ||||||||||
| Bone mineral density (g/cm2) | 0.66 | 0.13 | 0.68 | 0.11 | 0.144 | 0.66 | 0.11 | 0.67 | 0.12 | 0.649 |
| Bone quality | ||||||||||
| Trabecular bone score | 1.22 | 0.09 | 1.23 | 0.08 | 0.340 | 1.21 | 0.09 | 1.23 | 0.09 | 0.047 * |
| Muscle health | ||||||||||
| Low ASMI (n), % | 43 | 25% | 74 | 31% | 0.277 | 21 | 24% | 96 | 30% | 0.880 |
| Low HS (n), % | 94 | 55% | 103 | 43% | 0.016 * | 58 | 65% | 139 | 43% | <0.001 * |
| Sarcopenia (n), % | 22 | 13% | 36 | 15% | 0.668 | 13 | 15% | 45 | 14% | 1.000 |
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | Lower | Upper | p-Value | OR | Lower | Upper | p-Value | |
| Any VF | ||||||||
| Osteoporotic category | ||||||||
| Normal | 1.000 | 1.000 | ||||||
| Osteopenia | 0.712 | 0.220 | 2.292 | 0.565 | 2.058 | 0.426 | 15.019 | 0.404 |
| Osteoporosis | 0.517 | 0.159 | 1.651 | 0.263 | 2.141 | 0.439 | 15.736 | 0.382 |
| Trabecular bone score | ||||||||
| Normal | 1.000 | 1.000 | ||||||
| Partially degraded | 1.264 | 0.661 | 2.433 | 0.480 | 0.947 | 0.450 | 2.035 | 0.887 |
| Fully Degraded | 11.302 | 1.847 | 219.505 | 0.028 * | 1.164 | 0.531 | 2.597 | 0.707 |
| Sarcopenia | ||||||||
| w | 1.000 | 1.000 | ||||||
| w/o | 2.820 | 1.469 | 5.533 | 0.002 * | 0.805 | 0.446 | 1.423 | 0.461 |
| Multiple VFs | ||||||||
| Osteoporotic category | ||||||||
| Normal | 1.000 | - | - | - | - | |||
| Osteopenia | 0.933 | 0.273 | 3.748 | 0.916 | 1.000 | |||
| Osteoporosis | 1.074 | 0.343 | 4.079 | 0.908 | 1.301 | 0.763 | 2.290 | 0.346 |
| Trabecular bone score | ||||||||
| Normal | 1.000 | 1.000 | ||||||
| Partially degraded | 1.203 | 0.588 | 2.468 | 0.611 | 1.130 | 0.490 | 2.941 | 0.787 |
| Degraded | 15.158 | 3.462 | 106.173 | 0.001 * | 1.537 | 0.659 | 4.039 | 0.346 |
| Sarcopenia | ||||||||
| w | 1.000 | 1.000 | ||||||
| w/o | 1.981 | 1.008 | 3.899 | 0.047 * | 1.053 | 0.522 | 2.002 | 0.880 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-C.; Juan, Y.-H.; Chan, W.P.; Yeh, K.-Y.; Wong, A.M.K.; Sung, C.-M.; Lin, Y.-J.; Chang, S.-C.; Chen, F.-P. Integrating Muscle Health in Predicting the Risk of Asymptomatic Vertebral Fracture in Older Adults. J. Clin. Med. 2021, 10, 1129. https://doi.org/10.3390/jcm10051129
Lin Y-C, Juan Y-H, Chan WP, Yeh K-Y, Wong AMK, Sung C-M, Lin Y-J, Chang S-C, Chen F-P. Integrating Muscle Health in Predicting the Risk of Asymptomatic Vertebral Fracture in Older Adults. Journal of Clinical Medicine. 2021; 10(5):1129. https://doi.org/10.3390/jcm10051129
Chicago/Turabian StyleLin, Yu-Ching, Yu-Hsiang Juan, Wing P. Chan, Kun-Yun Yeh, Alice M. K. Wong, Chen-Ming Sung, Yu-Jr Lin, Shu-Chen Chang, and Fang-Ping Chen. 2021. "Integrating Muscle Health in Predicting the Risk of Asymptomatic Vertebral Fracture in Older Adults" Journal of Clinical Medicine 10, no. 5: 1129. https://doi.org/10.3390/jcm10051129