
Polymorphisms in the Gene Encoding Caspase 8 May Predict the Response to First-Line Platinum-Based Chemotherapy in Locally Advanced or Advanced Non-Small-Cell Lung Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Distribution of CASP-8 Genotypes and Their Influence on the Risk of Early Progression
3.2. Univariate Survival Analysis
3.3. Multivariate Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fennell, D.A. Caspase Regulation in Non–Small Cell Lung Cancer and its Potential for Therapeutic Exploitation. Clin. Cancer Res. 2005, 11, 2097–2105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, C.G.; Span, S.W.; Peters, G.J.; Kruyt, F.A.; Giaccone, G. Chemotherapy triggers apoptosis in a caspase-8-dependent and mitochon-dria-controlled manner in the non-small cell lung cancer cell line NCI-H460. Cancer Res. 2000, 60, 7133–7141. [Google Scholar]
- Paul, I.; Chacko, A.D.; Stasik, I.; Busacca, S.; Crawford, N.; McCoy, F.; McTavish, N.; Wilson, B.; Barr, M.; O’Byrne, K.J.; et al. Acquired differential regulation of caspase-8 in cisplatin-resistant non-small-cell lung cancer. Cell Death Dis. 2012, 3, e449. [Google Scholar] [CrossRef] [Green Version]
- Panov, S.Z. Molecular biology of the lung cancer. Radiol. Oncol. 2005, 39, 197–210. [Google Scholar]
- Massion, P.P.; Carbone, D.P. The molecular basis of lung cancer: Molecular abnormalities and therapeutic implications. Respir. Res. 2003, 4, 12. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [Green Version]
- McIlwain, D.R.; Berger, T.; Mak, T.W. Caspase functions in cell death and disease. Cold Spring Harb. Perspec. Biol. 2013, 5, a008656. [Google Scholar] [CrossRef]
- Chang, D.W.; Xing, Z.; Capacio, V.L.; Peter, M.E.; Yang, X. Interdimer processing mechanism of procaspase-8 activation. EMBO J. 2003, 22, 4132–4142. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.S.; Dixit, V.; Ashkenazi, A. Death receptor signal transducers: Nodes of coordination in immune signaling networks. Nat. Immunol. 2009, 10, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Gurung, P.; Anand, P.K.; Malireddi, R.K.S.; Walle, L.V.; Van Opdenbosch, N.; Dillon, C.P.; Weinlich, R.; Green, D.R.; Lamkanfi, M.; Kanneganti, T.-D. FADD and Caspase-8 Mediate Priming and Activation of the Canonical and Noncanonical Nlrp3 Inflammasomes. J. Immunol. 2014, 192, 1835–1846. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, W.J.; Upton, J.W.; Long, A.B.; Livingston-Rosanoff, D.; Daley-Bauer, L.P.; Hakem, R.; Caspary, T.; Mocarski, E.S. RIP3 mediates the embryonic lethality of caspase-8-deficient mice. Nat. Cell Biol. 2011, 471, 368–372. [Google Scholar] [CrossRef] [Green Version]
- Oberst, A.; Dillon, C.P.; Weinlich, R.; McCormick, L.L.; Fitzgerald, P.; Pop, C.; Hakem, R.; Salvesen, G.S.; Green, D.R. Catalytic activity of the caspase-8-FLIP(L) complex inhibits RIPK3-dependent ne-crosis. Nature 2011, 471, 363–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawadler, H.; Gantz, M.A.; Riley, J.L.; Yang, X. The Paracaspase MALT1 Controls Caspase-8 Activation during Lymphocyte Proliferation. Mol. Cell 2008, 31, 415–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terlizzi, M.; Di Crescenzo, V.G.; Perillo, G.; Galderisi, A.; Pinto, A.; Sorrentino, R. Pharmacological inhibition of caspase-8 limits lung tumour outgrowth. Br. J. Pharmacol. 2015, 172, 3917–3928. [Google Scholar] [CrossRef] [Green Version]
- Herrera, L.A.; Benítez-Bribiesca, L.; Mohar, A.; Ostrosky-Wegman, P. Role of infectious diseases in human carcinogenesis. Environ. Mol. Mutagen. 2005, 45, 284–303. [Google Scholar] [CrossRef]
- Soung, Y.H.; Lee, J.W.; Kim, S.Y.; Jang, J.; Park, Y.G.; Park, W.S.; Nam, S.W.; Lee, J.Y.; Yoo, N.J.; Lee, S.H. CASPASE-8 gene is inactivated by somatic mutations in gastric carcinomas. Cancer Res. 2005, 65, 815–821. [Google Scholar]
- Fulda, S. Caspase-8 in cancer biology and therapy. Cancer Lett. 2009, 281, 128–133. [Google Scholar] [CrossRef]
- Kim, H.S.; Lee, J.W.; Soung, Y.H.; Park, W.S.; Kim, S.Y.; Lee, J.H.; Park, J.Y.; Cho, Y.G.; Kim, C.J.; Jeong, S.W.; et al. Inactivating mutations of caspase-8 gene in colorectal carcinomas. Gastroenterology 2003, 125, 708–715. [Google Scholar] [CrossRef]
- Duiker, E.W.; Meijer, A.; Van Der Bilt, A.R.M.; Meersma, G.J.; Kooi, N.; Van Der Zee, A.G.J.; De Vries, E.G.; De Jong, S. Drug-induced caspase 8 upregulation sensitises cisplatin-resistant ovarian carcinoma cells to rhTRAIL-induced apoptosis. Br. J. Cancer 2011, 104, 1278–1287. [Google Scholar] [CrossRef]
- Van Geelen, C.M.; Pennarun, B.; Ek, W.B.; Le, P.T.K.; Spierings, D.C.J.; De Vries, E.G.E.; De Jong, S. Downregulation of active caspase 8 as a mechanism of acquired TRAIL re-sistance in mismatch repair-proficient colon carcinoma cell lines. Int. J. Oncol. 2010, 37, 1031–1041. [Google Scholar]
- Shivapurkar, N.; Reddy, J.; Matta, H.; Sathyanarayana, U.G.; Huang, C.X.; Toyooka, S.; Minna, J.D.; Chaudhary, P.M.; Gazdar, A.F. Loss of expression of death-inducing signaling complex (DISC) components in lung cancer cell lines and the influence of MYC amplification. Oncogene 2002, 21, 8510–8514. [Google Scholar] [CrossRef] [Green Version]
- Riley, J.S.; Hutchinson, R.W.; McArt, D.G.; Crawford, N.P.S.; Holohan, C.; Paul, A.I.; Van Schaeybroeck, S.; Saltotellez, M.; Johnston, P.G.; Fennell, A.D.; et al. Prognostic and therapeutic relevance of FLIP and procaspase-8 overexpression in non-small cell lung cancer. Cell Death Dis. 2013, 4, e951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grenet, J.; Teitz, T.; Wei, T.; Valentine, V.; Kidd, V.J. Structure and chromosome localization of the human CASP8 gene. Gene 1999, 226, 225–232. [Google Scholar] [CrossRef]
- Son, J.-W.; Kang, H.-K.; Chae, M.H.; Choi, J.E.; Park, J.M.; Lee, W.K.; Kim, C.H.; Kim, D.S.; Kam, S.; Kang, Y.M.; et al. Polymorphisms in the caspase-8 gene and the risk of lung cancer. Cancer Genet. Cytogenet. 2006, 169, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Hart, K.; Landvik, N.E.; Lind, H.; Skaug, V.; Haugen, A.; Zienolddiny, S. A combination of functional polymorphisms in the CASP8, MMP1, IL10 and SEPS1 genes affects risk of non-small cell lung cancer. Lung Cancer 2011, 71, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Ulybina, Y.M.; Kuligina, E.S.; Mitiushkina, N.V.; Rozanov, M.E.; Ivantsov, A.O.; Ponomariova, D.N.; Togo, A.V.; Levchenko, E.V.; Shutkin, V.A.; Brenister, S.I.; et al. Coding polymorphisms in Casp5, Casp8 and DR4 genes may play a role in predisposition to lung cancer. Cancer Lett. 2009, 278, 183–191. [Google Scholar] [CrossRef]
- Zhang, R.; Chu, M.; Zhao, Y.; Wu, C.; Guo, H.; Shi, Y.; Dai, J.; Wei, Y.; Jin, G.; Ma, H.; et al. A genome-wide gene-environment interaction analysis for tobacco smoke and lung cancer susceptibility. Carcinogenesis 2014, 35, 1528–1535. [Google Scholar] [CrossRef] [Green Version]
- Thorgeirsson, T.E.; Stefansson, K. Commentary: Gene-environment interactions and smoking-related cancers. Int. J. Epidemiology 2010, 39, 577–579. [Google Scholar] [CrossRef] [Green Version]
- VanderWeele, T.J.; Asomaning, K.; Tchetgen, E.J.T.; Han, Y.; Spitz, M.R.; Shete, S.; Wu, X.; Gaborieau, V.; Wang, Y.; McLaughlin, J.; et al. Genetic Variants on 15q25.1, Smoking, and Lung Cancer: An Assessment of Mediation and Interaction. Am. J. Epidemiol. 2012, 175, 1013–1020. [Google Scholar] [CrossRef]
- Maher, B. Personal genomes: The case of the missing heritability. Nat. Cell Biol. 2008, 456, 18–21. [Google Scholar] [CrossRef]
- Buttitta, F.; Barassi, F.; Fresu, G.; Felicioni, L.; Chella, A.; Paolizzi, D.; Lattanzio, G.; Salvatore, S.; Camplese, P.P.; Rosini, S.; et al. Mutational analysis of theHER2 gene in lung tumors from Caucasian patients: Mutations are mainly present in adenocarcinomas with bronchioloalveolar features. Int. J. Cancer 2006, 119, 2586–2591. [Google Scholar] [CrossRef]
- Amos, I.C.; Wu, X.; Broderick, P.; Gorlov, I.P.; Gu, J.; Eisen, T.; Dong, Q.; Zhang, Q.; Gu, X.; Vijayakrishnan, J.; et al. Genome-wide association scan of tag SNPs identifies a susceptibility locus for lung cancer at 15q25.1. Nat. Genet. 2008, 40, 616–622. [Google Scholar] [CrossRef] [Green Version]
- Le Marchand, L.; Derby, K.S.; Murphy, S.E.; Hecht, S.S.; Hatsukami, D.; Carmella, S.G.; Tiirikainen, M.; Wang, H. Smokers with the CHRNA Lung Cancer–Associated Variants Are Exposed to Higher Levels of Nicotine Equivalents and a Carcinogenic Tobacco-Specific Nitrosamine. Cancer Res. 2008, 68, 9137–9140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, J.D.; Hung, R.J.; Gaborieau, V.; Boffetta, P.; Chabrier, A.; Byrnes, G.; Zaridze, D.; Mukeria, A.; Szeszenia-Dabrowska, N.; Lissowska, J. Lung cancer susceptibility locus at 5p15.33. Nat. Genet. 2008, 40, 1404–1406. [Google Scholar] [CrossRef] [PubMed]
- Landi, M.T.; Chatterjee, N.; Yu, K.; Goldin, L.R.; Goldstein, A.M.; Rotunno, M.; Mirabello, L.; Jacobs, K.; Wheeler, W.; Yeager, M.; et al. A Genome-wide Association Study of Lung Cancer Identifies a Region of Chromosome 5p15 Associated with Risk for Adenocarcinoma. Am. J. Hum. Genet. 2009, 85, 679–691. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Broderick, P.; Webb, E.; Wu, X.; Vijayakrishnan, J.; Matakidou, A.; Qureshi, M.; Dong, Q.; Gu, X.; Chen, W.V.; et al. Common 5p15.33 and 6p21.33 variants influence lung cancer risk. Nat. Genet. 2008, 40, 1407–1409. [Google Scholar] [CrossRef]
- Truong, T.; Hung, R.J.; Amos, C.I.; Wu, X.; Bickeböller, H.; Rosenberger, A.; Sauter, W.; Illig, T.; Wichmann, H.-E.; Risch, A.; et al. Replication of Lung Cancer Susceptibility Loci at Chromosomes 15q25, 5p15, and 6p21: A Pooled Analysis From the International Lung Cancer Consortium. J. Natl. Cancer Inst. 2010, 102, 959–971. [Google Scholar] [CrossRef] [Green Version]
- Miki, D.; Kubo, M.; Takahashi, A.; Yoon, K.-A.; Kim, J.; Lee, G.K.; Zo, J.I.; Lee, J.S.; Hosono, N.; Morizono, T.; et al. Variation in TP63 is associated with lung adenocarcinoma susceptibility in Japanese and Korean populations. Nat. Genet. 2010, 42, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xiao, X.; Han, Y.; Gorlova, O.; Qian, D.; Leighl, N.; Johansen, J.S.; Barnett, M.; Chen, C.; Goodman, G.; et al. Genome-wide interaction study of smoking behavior and non-small cell lung cancer risk in Caucasian population. Carcinogenesis 2017, 39, 336–346. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Q.; Yuan, S.; Xie, W.; Liu, Y.; Xiang, Y.; Wu, N.; Wu, L.; Ma, X.; Cai, T.; et al. Genetic predisposition to lung cancer: Comprehensive literature integration, meta-analysis, and multiple evidence assessment of candidate-gene association studies. Sci. Rep. 2017, 7, 1–13. [Google Scholar] [CrossRef]
- Liao, Y.; Yang, F.; Li, X.; Chen, K.; Zhou, L.; Wang, Y.; Wang, J. The impact of Caspase-8 on non-small cell lung cancer brain metastasis in II/III stage patient. Neoplasma 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Camp, N.J.; Lin, W.; Bigelow, A.; Burghel, G.; Mosbruger, T.L.; Parry, M.A.; Waller, R.G.; Rigas, S.H.; Tai, P.-Y.; Berrett, K. Discordant Haplotype Sequencing Identifies Functional Variants at the 2q33 Breast Cancer Risk Locus. Cancer Res. 2016, 76, 1916–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivapurkar, N.; Toyooka, S.; Eby, M.T.; Huang, C.X.; Sathyanarayana, U.G.; Cunningham, H.T.; Reddy, J.L.; Brambilla, E.; Takahashi, T.; Minna, J.D.; et al. Differential inactivation of caspase-8 in lung cancers. Cancer Biol. Ther. 2002, 1, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Xu, W.; Ding, X.; Yang, Y.; Lu, Y.; Fei, K.; Su, B. Caspase 8 polymorphisms contribute to the prognosis of advanced lung adenocarcinoma patients after platinum-based chemotherapy. Cancer Biol. Ther. 2017, 18, 948–957. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Factor | Study Group (n = 99) | |
|---|---|---|
| Gender | Male | 76 (76.77%) |
| Female | 23 (23.23%) | |
| Age, median (range) | 66.5 (44–83) | |
| ≥66.5 | 49 (49.50%) | |
| <66.5 | 50 (50.50%) | |
| Disease stage | III | 35(35.35%) |
| IV | 64 (64.65%) | |
| Distant metastases | No | 43 (43.43%) |
| Yes | 56 (56.57%) | |
| Histopathology | AC | 40 (40.40%) |
| SCC | 52 (52.53%) | |
| NOS | 7 (7.07%) | |
| Performance status (ECOG score) | 0 | 17(17.17%) |
| 1 | 58 (58.59%) | |
| 2 | 24 (24.24%) | |
| Smoking status | Smoker | 92 (92.93%) |
| Non-smoker | 7 (7.07%) | |
| Pack-years, median (range) | 45.00 (1–100) | |
| ≥45 | 45 (45.45%) | |
| <45 | 54 (54.55%) | |
| Weight, median (range) | 74 (46–117) | |
| ≥74 | 49 (49.49%) | |
| <74 | 50 (50.51%) | |
| BMI, median (range) | 24.91 (15.02–40.88) | |
| ≥24.91 | 49 (49.49%) | |
| <24.91 | 50 (50.51%) | |
| Body loss (%), median (range) | 9.84(0–40) | |
| ≥9.84 | 32 (32.32%) | |
| <9.84 | 67 (67.68%) | |
| Time from diagnosis to treatment (days) | 17.00 (3–217) | |
| ≥17 | 48 (48.48%) | |
| <17 | 51 (51.52%) | |
| First-line chemotherapy (I) | Cis + PEM | 23 (23.23%) |
| PN | 60 (60.60%) | |
| PG | 16 (16.16%) | |
| Number of CTH cycles | 1–3 | 38 (38.38%) |
| 4–8 | 61 (61.62%) | |
| First evaluation after first-line chemotherapy | PR | 36 (48.65%) |
| SD | 29 (39.19%) | |
| PD | 9 (12.16%) | |
| Second evaluation after first-line chemotherapy | PR | 10 (20.00%) |
| SD | 32 (64.00%) | |
| PD | 8 (16.00%) | |
| Occupational exposure | No | 55 (79.71%) |
| Yes | 14 (20.29%) | |
| Family history of malignancy (any) | No | 46 (46.46%) |
| Yes | 53 (53.54%) | |
| Family history of malignancy (lung) | No | 75 (75.76%) |
| Yes | 24 (24.24%) | |
| Variable | CASP-8 (rs3769818) | ||||
|---|---|---|---|---|---|
| AA (n = 8) | AG (n = 38) | GG (n = 53) | p-Value χ2 | ||
| Gender | Male | 5 (6.58%) | 32 (42.11%) | 39 (51.31%) | 0.3020 2.39 |
| Female | 3 (13.04%) | 6 (26.09%) | 14 (60.87%) | ||
| Age | ≥66.5 | 4 (81.16%) | 21 (42.86%) | 24 (48.98%) | 0.6432 0.88 |
| <66.5 | 4 (8.00%) | 17 (34.00%) | 29 (58.00%) | ||
| Disease stage | III | 3 (8.58%) | 16 (45.71%) | 16 (45.71%) | 0.4984 1.39 |
| IV | 5 (7.81%) | 22 (34.38%) | 37 (57.81%) | ||
| Distant metastases | No | 1 (2.56%) | 21 (53.85%) | 17 (43.59%) | 0.0221 7.62 * |
| Yes | 7 (11.67%) | 17 (28.33%) | 36 (60.00%) | ||
| Histopathology | AC | 5 (12.50%) | 18 (45.00%) | 17 (42.50%) | 0.2165 5.78 |
| SCC | 3 (5.77%) | 16 (30.78%) | 33 (63.46%) | ||
| NOS | - | 4 (57.14%) | 3 (42.86%) | ||
| Performance status (ECOG score) | 0 | 1 (5.88%) | 11 (64.71%) | 5 (29.41%) | 0.1178 7.36 |
| 1 | 4 (6.90%) | 18 (31.03%) | 36 (62.07%) | ||
| 2 | 3 (12.50%) | 9 (37.50%) | 12 (50.00%) | ||
| Smoking status | Smoker | 5 (5.43%) | 37 (40.22%) | 52 (56.52%) | <0.0001 19.14 * |
| Non-smoker | 3 (42.86%) | 1 (28.57%) | 1 (28.57%) | ||
| Body loss (%) | ≥9.84 | 1 (3.13%) | 9 (28.12%) | 22 (68.75%) | 0.0917 4.78 |
| <9.84 | 7 (10.45%) | 29 (43.28%) | 31 (46.27%) | ||
| Family history of malignancy (any) | No | - | 27 (57.45%) | 20 (42.55%) | 0.0003 16.00 * |
| Yes | 8 (15.69%) | 12 (23.53%) | 31 (60.78%) | ||
| Family history of malignancy (lung) | No | 3 (6.38%) | 25 (53.19%) | 19 (40.46%) | 0.0157 8.30 * |
| Yes | 5 (9.62%) | 13 (25.00%) | 34 (65.38%) | ||
| Variable | Objective Response # | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|
| PD (n = 9) | PR and SD (n = 65) | ||||
| Gender | Male | 6 (10.00%) | 54 (90.00%) | 0.41 (0.091.88) | 0.2500 |
| Female | 3 (21.43%) | 11 (78.57%) | |||
| Age | ≥66.5 | 3 (9.37%) | 29 (90.63%) | 1.24 (0.23–6.62) | 0.8001 |
| <66.5 | 6 (14.28%) | 36 (85.72%) | |||
| Disease stage | III | 1 (3.57%) | 27 (96.43%) | 5.68 (0.67–48.15) | 0.1109 |
| IVA | 8 (17.39%) | 38 (82.61%) | |||
| Performance status (ECOG score) | 0 | 2 (18.18%) | 9 (81.82%) | 1.78 (0.32–9.95) | 0.5125 |
| 1 and 2 | 7 (11.11%) | 56 (88.89%) | |||
| Smoking status | Smoker | 8 (11.59%) | 61 (88.41%) | 0.52 (0.05–5.29) | 0.5844 |
| Non-smoker | 1 (20.00%) | 4 (80.00%) | |||
| Pack-years | ≥45 | 4 (11.11%) | 32 (88.89%) | 0.82 (0.20–3.35) | 0.7880 |
| <45 | 5 (13.16%) | 33 (86.84%) | |||
| First-line chemotherapy (I) | Cis + PEM | 3 (17.65%) | 14 (82.35%) | 1.82 (0.40–8.22) | 0.4354 |
| Other | 6 (10.53%) | 51 (89.47%) | |||
| First-line chemotherapy (II) | PN | 5 (10.42%) | 43 (89.58%) | 0.64 (0.15–2.62) | 0.5348 |
| Other | 4 (15.38%) | 22 (84.62%) | |||
| First-line chemotherapy (III) | PG | 1 (14.29%) | 6 (85.71%) | 1.23 (0.13–11.57) | 0.8028 |
| Other | 8 (11.94%) | 59 (88.06%) | |||
| Distant metastases | No | 1 (4.35%) | 22 (95.65%) | 0.24 (0.03–2.08) | 0.1971 |
| Yes | 8 (15.69%) | 43 (84.31%) | |||
| Weight | ≥74 | 1 (2.94%) | 33 (97.06%) | 0.12 (0.01–1.02) | 0.0527 |
| <74 | 8 (20.00%) | 32 (80.00%) | |||
| BMI | ≥24.91 | 1 (3.03%) | 32 (96.97%) | 0.13 (0.01–1.09) | 0.0600 |
| <24.91 | 8 (19.51%) | 33 (80.49%) | |||
| Body loss (%) | ≥9.84 | 6 (24.00%) | 19 (76.00%) | 4.84 (1.09–21.39) | 0.0374 * |
| <9.84 | 3 (6.52%) | 46 (93.48%) | |||
| Time from diagnosis to treatment (days) | ≥17 | 5 (14.28%) | 30 (85.72%) | 1.4583 (0.36–5.93) | 0.5980 |
| <17 | 4 (10.27%) | 35 (89.73%) | |||
| Occupational exposure | No | 7 (12.73%) | 48 (87.27%) | 1.90 (0.21–16.82) | 0.5658 |
| Yes | 1 (7.14%) | 13 (92.86%) | |||
| Family history of malignancy (any) | No | 2 (5.56%) | 34 (94.44%) | 0.26 (0.05–1.35) | 0.1090 |
| Yes | 7 (18.42%) | 31 (81.58%) | |||
| Family history of malignancy (lung) | No | 6 (11.11%) | 48 (88.89%) | 0.71 (0.16–3.15) | 0.6506 |
| Yes | 3 (15.00%) | 17 (85.00%) | |||
| Histopathology (I) | AC | 4 (13.79%) | 25 (86.21%) | 1.28 (0.31–5.22) | 0.7309 |
| SCC and NOS | 5 (11.11%) | 40 (88.89%) | |||
| Histopathology (II) | SCC | 5 (12.50%) | 35 (87.50%) | 1.07 (0.26–4.35) | 0.9232 |
| AC and NOS | 4 (11.76%) | 30 (88.24%) | |||
| CASP-8 (rs3769818) | AA | 1 (16.67%) | 6 (83.33%) | 1.23 (0.13–11.57) | 0.8569 |
| AG and GG | 8 (11.94%) | 59 (88.06%) | |||
| CASP-8 (rs3769818) | AG | - | 28 (100.00%) | 0.07 (0.01–1.24) | 0.0697 |
| AA and GG | 9 (19.57%) | 37 (80.43%) | |||
| CASP-8 (rs3769818) | GG | 8 (20.51%) | 31 (79.49%) | 8.77 (1.04–74.21) | 0.0462 * |
| AG and AA | 1 (2.86%) | 34 (97.14%) | |||
| Variable | PD (n = 8) | PR and SD (n = 42) | OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Gender | Male | 5(12.20%) | 37 (87.80%) | 0.22 (0.04–1.24) | 0.0874 |
| Female | 3(37.50%) | 5(62.50%) | |||
| Age | ≥66.5 | 4(21.05%) | 15 (78.95%) | 1.80 (0.39–8.25) | 0.4494 |
| <66.5 | 4(12.90%) | 27 (87.10%) | |||
| Disease stage | III | 1(4.76%) | 20 (95.24%) | 0.16 (0.02–1.39) | 0.0963 |
| IV | 7 (24.18%) | 22 (78.86%) | |||
| Performance status (ECOG score) | 0 | 0(0.00%) | 9(100.00%) | 0.21 (0.01–3.93) | 0.2946 |
| 1 and 2 | 8 (19.51%) | 33 (80.49%) | |||
| Smoking status | Smoker | 8 (17.02%) | 39(82.98%) | 1.59 (0.07–31.95 | 0.7926 |
| Non-smoker | 0(0.00%) | 3(100.00%) | |||
| Pack-years | ≥45 | 4(17.39%) | 19(82.61%) | 1.21 (0.27–5.50) | 0.8046 |
| <45 | 4(14.81%) | 23(85.19%) | |||
| First-line chemotherapy (I) | Cis + PEM | 3(23.08%) | 10(76.92%) | 1.26 (0.25–6.35) | 0.7794 |
| Other | 5(19.23%) | 21(80.77%) | |||
| First-line chemotherapy (II) | PN | 4(12.50%) | 28(87.50%) | 0.50 (0.11–2.30) | 0.3737 |
| Other | 4 (22.22%) | 14(77.78%) | |||
| First-line chemotherapy (III) | PG | 1(33.33%) | 2(66.67%) | 2.86 (0.23–35.91) | 0.4163 |
| Other | 7 (14.89%) | 40 (85.11%) | |||
| Number of cycles | 1–3 | 2 (28.57%) | 5 (71.43%) | 2.46 (0.39–15.73) | 0.3395 |
| 4–8 | 6 (13.95%) | 37(86.05%) | |||
| Metastases | No | 1(5.88%) | 16 (94.11%) | 0.23 (0.03–2.07) | 0.1904 |
| Yes | 7 (21.21%) | 26 (78.79%) | |||
| Weight | ≥74 | 5 (18.52%) | 22 (81.48%) | 1.51 (0.32–7.17) | 0.6003 |
| <74 | 3 (13.04%) | 20 (86.96%) | |||
| BMI | ≥24.91 | 6 (22.22%) | 21 (77.78%) | 3.00 (0.54–16.60) | 0.2082 |
| <24.91 | 2(8.70%) | 21 (91.30%) | |||
| Body weight loss (%) | ≥9.84 | 7(46.67%) | 8(53.33%) | 29.75 (3.19–277.33) | 0.0029 * |
| <9.84 | 1(2.86%) | 34(97.14%) | |||
| Time from diagnosis to treatment (days) | ≥17 | 7 (28.00%) | 18 (72.00%) | 9.33 (1.05–82.78) | 0.0449 * |
| <17 | 1(4.00%) | 24 (96.00%) | |||
| Occupational exposure | No | 6 (15.79%) | 32 (84.21%) | 0.94 (0.16–5.40) | 0.9424 |
| Yes | 2 (16.67%) | 10 (83.33%) | |||
| Family history of malignancy (any) | No | 4 (17.39%) | 19 (82.61%) | 1.21 (0.27–5.50) | 0.8046 |
| Yes | 4 (10.81%) | 23 (89.19%) | |||
| Family history of malignancy (lung) | No | 1(7.14%) | 13 (92.86%) | 0.26 (0.02–2.85) | 0.2681 |
| Yes | 3 (23.08%) | 10 (76.92%) | |||
| Histopathology (I) | AC | 4 (22.22%) | 14 (77.78%) | 2.00 (0.43–9.21) | 0.3737 |
| SCC and NOS | 4 (12.50%) | 28 (87.50%) | |||
| Histopathology (II) | SCC | 4 (14.81%) | 23 (85.19%) | 0.83 (0.18–3.75) | 0.8046 |
| AC and NOS | 4 (17.39%) | 19 (82.61%) | |||
| CASP-8 (rs3769818) | AA | 0(0.00%) | 3 (100.00%) | 0.66 (0.03–14.08) | 0.7926 |
| AG and GG | 8 (17.02%) | 39 (82.98%) | |||
| CASP-8 (rs3769818) | AG | 1(5.26%) | 18 (94.74%) | 0.19 (0.02–1.69) | 0.1365 |
| AA and GG | 7 (22.58%) | 24 (77.42%) | |||
| CASP-8 (rs3769818) | GG | 7 (29.17%) | 17(70.83%) | 10.29 (1.16–91.43) | 0.0364 * |
| AG and AA | 1(3.85%) | 25(96.15%) | |||
| Variable | Survival Analysis # (n = 89) | ||||||
|---|---|---|---|---|---|---|---|
| Progression-Free Survival | Time to Progression | Overall Survival | |||||
| Median (Days) | p-Value HR (95% CI) | Median (Days) | p-Value HR (95% CI) | Median (Days) | p-Value HR (95% CI) | ||
| Gender | Male Female | 41.00 131.00 | 0.3903 1.26 (0.71–2.23) 0.80 (0.45–1.41) | 54.00 164.00 | 0.2553 1.34 (0.77–2.34) 0.75 (0.43–1.30) | 282.00 332.00 | 0.9624 1.01 (0.59–1.73) 0.99 (0.58–1.69) |
| Age | ≥66.5 <66.5 | 84.00 122.00 | 0.1941 1.33 (0.85–2.07) 0.75(0.48–1.17) | 117.00 167.00 | 0.2033 1.31 (0.86–2.02) 0.76 (0.49–1.17) | 249.00 389.00 | 0.1539 1.37 (0.88–2.11) 0.73 (0.47–1.13) |
| Disease stage | III IV | 198.00 68.00 | <0.0001 * 0.40 (0.26–0.62) 2.50 (1.61–3.89) | 222.00 92.00 | <0.0001 * 0.39 (0.25–0.60) 2.56 (1.67–3.92) | 502.00 228.00 | 0.0021 * 0.50 (0.32–0.77) 2.01 (1.30–3.09) |
| Performance status (ECOG score) | 0 1 and 2 | 182.00 95.00 | 0.4665 0.74 (0.35–1.54) 1.35 (0.65–2.82) | 190.00 134.00 | 0.5332 0.77 (0.36–1.62) 1.30 (0.62–2.74) | 389.00 233.00 | 0.1058 0.51 (0.27–0.97) 1.96 (1.03–3.71) |
| Smoking status | Smoker Non-smoker | 36.00 107.00 | 0.6478 1.23(0.46–3.30) 0.81 (0.30–2.19) | 51.00 145.00 | 0.73201.17 (0.44–3.08) 0.86 (0.32–2.25) | 321.00 412.00 | 0.3434 1.54 (0.72–3.27) 0.65 (0.31–1.38) |
| Pack-years | <45 ≥45 | 122.00 89.00 | 0.0513 0.67 (0.43–1.03) 1.50 (0.97–2.30) | 167.00 114.00 | 0.0408 * 0.65 (0.42–1.00) 1.54 (1.00–2.36) | 337.00 321.00 | 0.3978 0.83 (0.54–1.28) 1.20 (0.78–1.86) |
| First-line chemotherapy (I) | Cis + Pem Other | 61.00 122.00 | 0.0356 * 1.64 (0.94–2.88) 0.61 (0.35–1.06) | 70.00 149.00 | 0.0240 * 1.72(0.97–3.03) 0.58 (0.33–1.03) | 233.00 337.00 | 0.0638 1.58 (0.90–2.78) 0.63 (0.36–1.11) |
| First-line chemotherapy (II) | PN Other | 122.00 76.00 | 0.,0198 * 0.61 (0.38–0.97) 1.64 (1.03–2.62) | 167.00 115.00 | 0.0380 * 0.64 (0.40–1.02) 1.56 (0.98–2.49) | 332.00 237.00 | 0.6685 0.91 (0.58–1.42) 1.10 (0.70–1.72) |
| First-line chemotherapy (III) | PG Other | 68.00 122.00 | 0.3377 1.35 (0.66–2.76) 0.74 (0.36–1.51) | 115.00 162.00 | 0.7066 1.13 (0.58–2.20) 0.89 (0.45–1.72) | 355.00 337.00 | 0.9503 0.98 (0.50–1.89) 1.02 (0.53–1.98) |
| Number of cycles | 1–3 4–8 | 40.00 213.00 | <0.0001 * 4.24 (2.07–8.72) 0.23 (0.11–0.48) | 58.00 237.00 | <0.0001 * 3.80 (1.90–7.59) 0.26 (0.13–0.53) | 137.00 472.00 | 0.0005 * 2.39 (1.31–4.36) 0.42 (0.23–0.76) |
| Metastases | No Yes | 213.00 61.00 | 0.0016 * 0.43 (0.27–0.70) 2.30 (1.42–3.72) | 237.00 78.00 | 0.0013 * 0. 42 (0.26–0.69) 2.36 (1.46–3.82) | 502.00 224.00 | 0.0026 * 0.44 (0.27–0.72) 2.28 (1.40–3.73) |
| Weight | ≥74 <74 | 122.00 89.00 | 0.7208 0.93 (0.60–1.42) 1.08 (0.70–1.65) | 145.00 139.00 | 0.7114 0.92 (0.60–1.41) 1.08 (0.71–1.66) | 337.00 274.00 | 0.4882 0.86 (0.56–1.32) 1.16 (0.75–1.80) |
| BMI | ≥24.91 <24.91 | 122.00 82.00 | 0.9569 1.01(0.66–1.55) 0.99 (0.64–1.51) | 131.00 151.00 | 0.8788 1.03 (0.68–1.58) 0.97 (0.63–1.48) | 337.00 250.00 | 0.7648 0.94 (0.61–1.44) 1.07 (0.69–1.65) |
| Body weight loss (%) | <9.84 ≥9.84 | 122.00 47.00 | 0.2319 0.76 (0.47–1.23) 1.31 (0.81–2.12) | 167.00 78.00 | 0.2424 0.76 (0.47–1.24) 1.31 (0.81–2.12) | 438.00 168.00 | 0.0428 * 0.62 (0.37–1.05) 1.60 (0.95–2.69) |
| Time from diagnosis to treatment (days) | ≥17 <17 | 92.00 122.00 | 0.0504 1.50 (0.97–2.31) 0.67 (0.43–1.03) | 149.00 134.00 | 0.2929 1.25 (0.81–1.91) 0.80 (0.52–1.23) | 337.00 282.00 | 0.6745 0.91 (0.59–1.41) 1.10 (0.71–1.69) |
| Occupational exposure | No Yes | 95.00 105.00 | 0.5610 1.20 (0.66–2.18) 0.83 (0.46–1.52) | 139.00 164.00 | 0.6304 1.16 (0.64–2.13) 0.86 (0.47–1.57) | 282.00 350.00 | 0.8392 1.07 (0.57–1.99) 0.94 (0.50–1.74) |
| Family history of malignancy (any) | No Yes | 137.00 91.00 | 0.5386 0.88 (0.57–1.35) 1.14 (0.74–1.75) | 177.00 132.00 | 0.5338 0.87 (0.57–1.34) 1.14 (0.75–1.75) | 273.00 321.00 | 0.7529 1.07 (0.69–1.66) 0.93 (0.60–1.44) |
| Family history of malignancy (lung) | No Yes | 107.00 83.00 | 0.7111 0.89 (0.47–1.67) 1.12 (0.60–2.10) | 135.00 115.00 | 0.7796 0.92 (0.49–1.71) 1.09 (0.58–2.05) | 438.00 168.00 | 0.3720 0.75 (0.40–1.42) 1.33 (0.70–2.52) |
| Histopathology (I) | SCC AC and NOS | 84.00 137.00 | 0.7849 1.07 (0.64–1.81) 0.93 (0.55–1.57) | 117.00 167.00 | 0.9363 1.02 (0.60–1.73) 0.98 (0.58–1.65) | 355.00 337.00 | 0.9455 1.02 (0.58–1.77) 0.98 (0.56–1.71) |
| Histopathology (II) | AC SCC and NOS | 137.00 84.00 | 0.4433 0.82 (0.49–1.37) 1.22 (0.73–2.04) | 167.00 117.00 | 0.5556 0.85 (0.51–1.43) 1.17 (0.70–1.96) | 337.00 355.00 | 0.9228 1.03 (0.59–1.79) 0.97 (0.56–1.69) |
| CASP-8 (rs3769818) | AA AG and GG | 365.00 95.00 | 0.0035 * 0.36 (0.21–0.61) 2.78 (1.65–4.76) | 135.00 458.00 | 0.0029 * 0.35 (0.20–0.59) 2.88(1.70–4.88) | 631.00 273.00 | 0.1757 0.61 (0.33–1.12) 1.64 (0.89–3.00) |
| CASP-8 (rs3769818) | AG AA and GG | 152.00 84.00 | 0.0105 * 0.56 (0.36–0.86) 1.79 (1.16–2.75) | 222.00 114.00 | 0.0117 * 0.56 (0.36–0.86) 1.79 (1.17–2.76) | 332.00 321.00 | 0.3665 1.26 (0.76–2.08) 0.79 (0.48–1.31) |
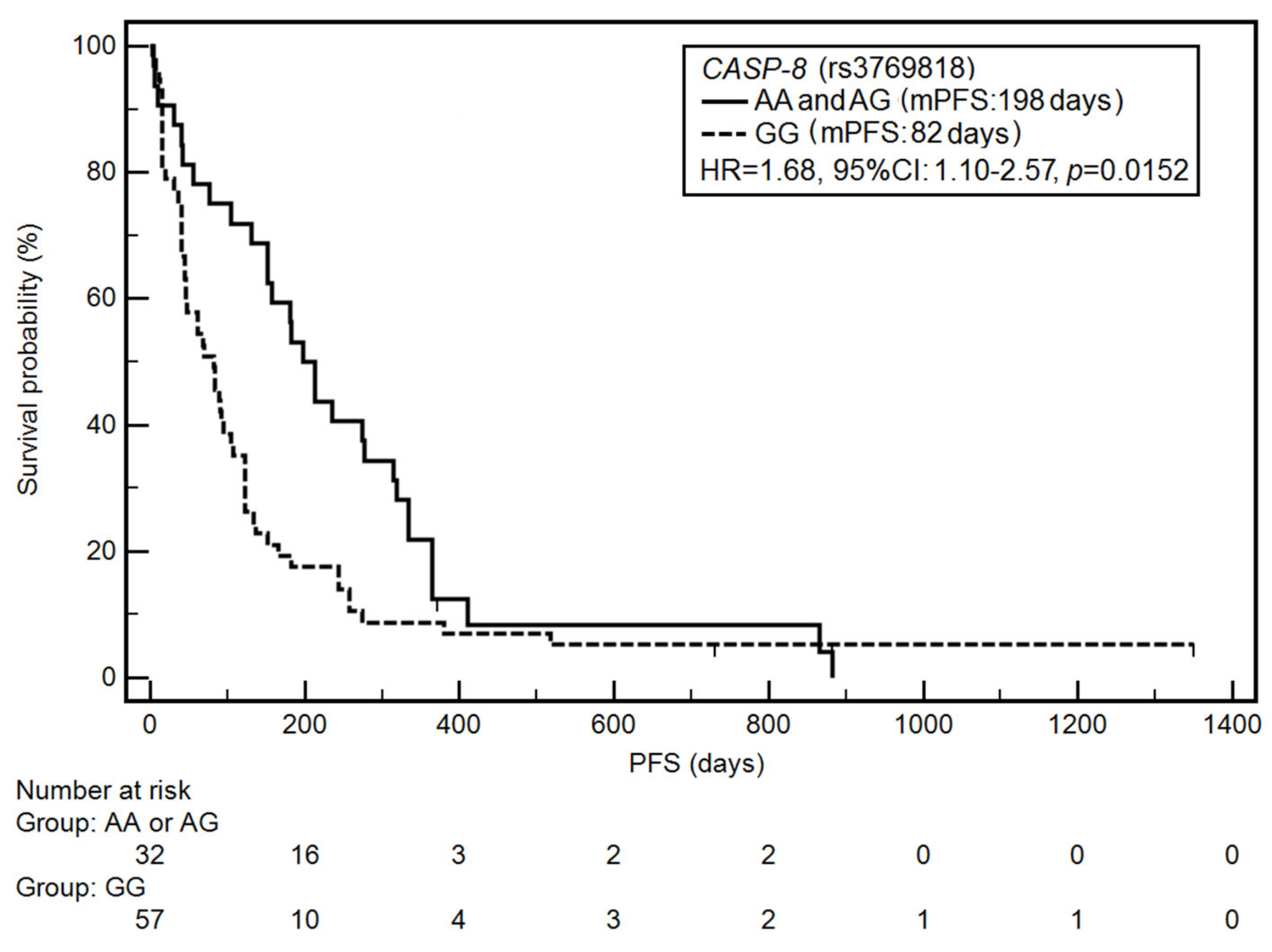
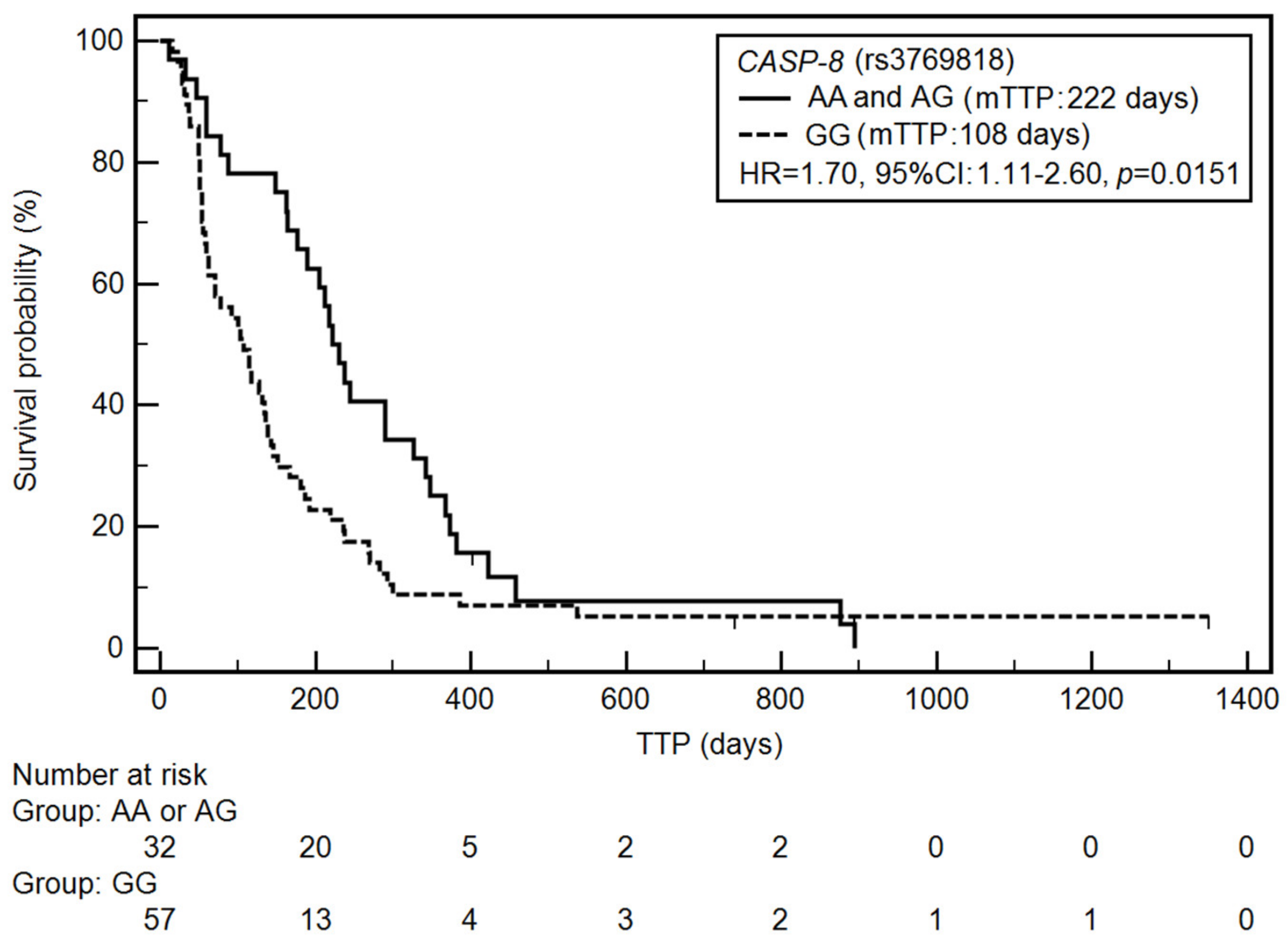
| CASP-8 (rs3769818) | GG AG and AA | 82.00 198.00 | 0.0152 * 1.68 (1.10–2.57) 0.59 (0.39–0.91) | 108.00 222.00 | 0.0151 * 1.70 (1.11–2.60) 0.59 (0.38–0.91) | 237.00 502.00 | 0.0601 1.52 (0.98–2.34) 0.66 (0.43–1.02) |
| Variable | Survival Analysis # (n = 89) | |||
|---|---|---|---|---|
| Progression-Free Survival | Time to Progression | Overall Survival | ||
| p-Value HR (95% CI) | p-Value HR (95% CI) | p-Value HR (95% CI) | ||
| Gender | Female | 0.0689 0.47 (0.21–1.06) | 0.9032 0.95 (0.42–2.14) | 0.9976 0.99 (0.50–2.00) |
| Age | <66.5 | 0.1160 0.64 (0.37–1.11) | 0.0952 0.61 (0.34–1.09) | 0.1312 0.66 (0.38–1.13) |
| Disease stage | IV | 0.0016 * 2.56 (1.43–7.76) | 0.0028 * 2.44 (1.35–4.35) | 0.0002 * 2.94 (1.64–5.26) |
| Performance status (ECOG score) | 1 and 2 | 0.5521 0.71 (0.23–2.19) | 0.6948 0.79 (0.24–2.57) | 0.0917 2.54 (0.86–7.49) |
| Smoking status | Smoker | 0.3681 0.63 (0.23–1.71) | 0.9254 1.05 (0.39–2.79) | 0.3583 1.56 (0.60–4.01) |
| Pack-years | ≥45 (years) | 0.4021 1.24 (0.75–2.05) | 0.3709 1.25 (0.77–2.04) | 0.7364 0.92 (0.55–1.53) |
| First-line chemotherapy (I) | Cis + PEM | 0.8361 0.92 (0.41–2.04) | 0.3604 0.69 (0.31–1.54) | 0.4484 0.80 (0.45–1.42) |
| First-line chemotherapy (II) | PN | 0.4374 1.22 (0.74–2.00) | 0.6315 1.13 (0.68–1.87) | 0.1687 0.69 (0.41–1.17) |
| First-line chemotherapy (III) | PG | 0.8369 1.09 (0.49–2.42) | 0.3636 1.46 (0.65–3.27) | 0.1728 1.69 (0.79–3.57) |
| Number of chemotherapy cycles | 4–8 | 0.5711 0.74 (0.26–2.08) | 0.4788 0.68 (0.24–1.97) | 0.7475 1.19 (0.41–3.41) |
| Distant metastases | Yes | 0.0353 * 3.16 (1.09–9.15) | 0.0514 2.95 (0.99–8.75) | 0.1656 2.09 (0.74–5.91) |
| Weight | ≥74 (kg) | 0.1160 0.64 (0.37–1.11) | 0.4989 1.19 (0.72–1.96) | 0.1433 1.49 (0.87–2.54) |
| BMI | <24.91 | 0.4987 0.99 (0.94–1.03) | 0.4333 1.23 (0.73–2.05) | 0.0474 * 1.72 (1.01–2.95) |
| Body loss (%) | ≥9.84 (%) | 0.5747 1.16 (0.69–1.94) | 0.1384 1.56 (0.87–2.81) | 0.0202 * 1.95 (1.11–3.44) |
| Time from diagnosis to treatment (days) | ≥17 (days) | 0.7208 0.91 (0.55–1.51) | 0.3378 1.29 (0.76–2.19) | 0.3286 1.32 (0.76–2.28) |
| Occupational exposure | Yes | 0.5177 1.31 (0.58–2.93) | 0.2608 1.61 (0.70–3.72) | 0.5984 1.25 (0.55–2.86) |
| Family history of malignancy (any) | Yes | 0.4368 1.14 (0.74–1.75) | 0.1450 1.49 (0.87–2.53) | 0.4585 0.81 (0.46–1.42) |
| Family history of malignancy (lung) | Yes | 0.8379 1.11 (0.40–3.10) | 0.5220 0.75 (0.32–6.75) | 0.5430 0.76 (0.31–1.85) |
| Histopathology | SCC | 0.2543 1.81 (0.65–5.02) | 0.0167 * 3.87 (1.28–11.70) | 0.1252 1.73 (0.86–3.50) |
| CASP-8 (rs3769818) | AA | 0.1084 0.44 (0.16–1.19) | 0.0506 0.36 (0.13–1.00) | 0.8303 1.11 (0.42–2.90) |
| CASP-8 (rs3769818) | AG | 0.2769 0.69 (0.35–1.35) | 0.7188 0.89 (0.46–1.72) | 0.4396 0.78 (0.42–1.46) |
| CASP-8 (rs3769818) | GG | 0.0317 * 1.80 (1.06–3.05) | 0.5372 1.19 (0.69–2.06) | 0.9805 1.01 (0.58–1.75) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szczyrek, M.; Mlak, R.; Szudy-Szczyrek, A.; Kędziora, K.; Małecka-Massalska, T.; Krawczyk, P.; Milanowski, J. Polymorphisms in the Gene Encoding Caspase 8 May Predict the Response to First-Line Platinum-Based Chemotherapy in Locally Advanced or Advanced Non-Small-Cell Lung Cancer. J. Clin. Med. 2021, 10, 1126. https://doi.org/10.3390/jcm10051126
Szczyrek M, Mlak R, Szudy-Szczyrek A, Kędziora K, Małecka-Massalska T, Krawczyk P, Milanowski J. Polymorphisms in the Gene Encoding Caspase 8 May Predict the Response to First-Line Platinum-Based Chemotherapy in Locally Advanced or Advanced Non-Small-Cell Lung Cancer. Journal of Clinical Medicine. 2021; 10(5):1126. https://doi.org/10.3390/jcm10051126
Chicago/Turabian StyleSzczyrek, Michał, Radosław Mlak, Aneta Szudy-Szczyrek, Karolina Kędziora, Teresa Małecka-Massalska, Paweł Krawczyk, and Janusz Milanowski. 2021. "Polymorphisms in the Gene Encoding Caspase 8 May Predict the Response to First-Line Platinum-Based Chemotherapy in Locally Advanced or Advanced Non-Small-Cell Lung Cancer" Journal of Clinical Medicine 10, no. 5: 1126. https://doi.org/10.3390/jcm10051126