
Preoperative Screening CT and PET/CT Scanning for Acral Melanoma: Is it Necessary?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Patients
2.3. Treatment and Follow-up
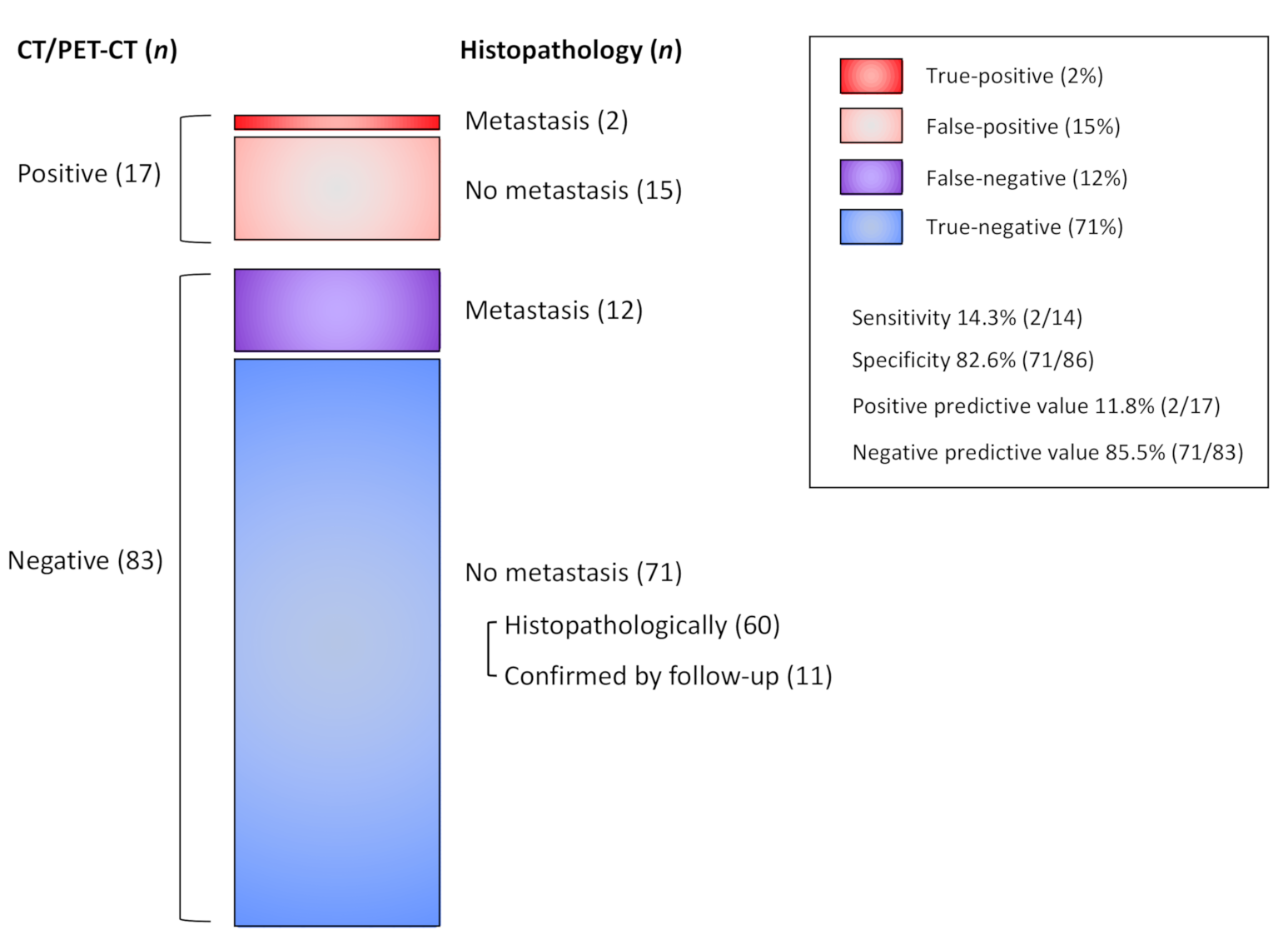
2.4. Detection of Lymph Node and Distant Metastasis by Imaging Modalities
3. Results
3.1. Patient Data
3.2. Detection of Lymph Node and Distant Metastasis
3.3. Breslow Thickness (T category) and Metastasis in Patients without Lymphadenopathy
3.4. Detection of Distant Metastasis in Patients with Lymphadenopathy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Ward, E.; Brawley, O.; Jemal, A. Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J. Clin. 2011, 61, 212–236. [Google Scholar] [CrossRef] [PubMed]
- Kohler, B.A.; Ward, E.; McCarthy, B.J.; Schymura, M.J.; Ries, L.A.G.; Eheman, C.; Jemal, A.; Anderson, R.N.; Ajani, U.A.; Edwards, B.K. Annual Report to the Nation on the Status of Cancer, 1975-2007, Featuring Tumors of the Brain and Other Nervous System. J. Natl. Cancer Inst. 2011, 103, 714–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinnes, J.; Di Ruffano, L.F.; Takwoingi, Y.; Cheung, S.T.; Nathan, P.; Matin, R.N.; Chuchu, N.; Chan, S.A.; Durack, A.; E Bayliss, S.; et al. Ultrasound, CT, MRI, or PET-CT for staging and re-staging of adults with cutaneous melanoma. Cochrane Database Syst. Rev. 2019, 2019, CD012806. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.R., Jr.; South, D.A. Acral lentiginous melanoma. Cutis. 1980, 26, 35–36. [Google Scholar] [PubMed]
- Sakaizawa, K.; Ashida, A.; Uchiyama, A.; Ito, T.; Fujisawa, Y.; Ogata, D.; Matsushita, S.; Fujii, K.; Fukushima, S.; Shibayama, Y.; et al. Clinical characteristics associated with BRAF, NRAS and KIT mutations in Japanese melanoma patients. J. Dermatol. Sci. 2015, 80, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Xu, Y.; Gabriel, E.M.; Misra, S.; Chen, Y.; Bagaria, S.P.; Asadi, A.K. Comparative Analysis of Acral Melanoma in Chinese and Caucasian Patients. J. Ski. Cancer 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Asai, J.; Igaki, H.; Inozume, T.; Namikawa, K.; Hayashi, A.; Fukushima, S.; Fujimura, T.; Ito, T.; Imafuku, K.; et al. Japanese Dermatological Association Guidelines: Outlines of guidelines for cutaneous melanoma 2019. J. Dermatol. 2019, 47, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Hafner, J.; Schmid, M.; Kempf, W.; Burg, G.; Kunzi, W.; Meuli-Simmen, C.; Neff, P.; Meyer, V.; Mihic, D.; Garzoli, E.; et al. Baseline staging in cutaneous malignant melanoma. Br. J. Dermatol. 2004, 150, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Miranda, E.P.; Gertner, M.; Wall, J.; Grace, E.; Kashani-Sabet, M.; Allen, R.; Leong, S.P.L. Routine Imaging of Asymptomatic Melanoma Patients With Metastasis to Sentinel Lymph Nodes Rarely Identifies Systemic Disease. Arch. Surg. 2004, 139, 831–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, Y.; Bronstein, Y.; Ross, M.I.; Askew, R.L.; Lee, J.E.; Gershenwald, J.E.; Royal, R.; Cormier, J.N. Contemporary Diagnostic Imaging Modalities for the Staging and Surveillance of Melanoma Patients: A Meta-analysis. J. Natl. Cancer Inst. 2010, 103, 129–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancovitz, M.; Finelt, N.; Warycha, M.A.; Christos, P.J.; Mazumdar, M.; Shapiro, R.L.; Pavlick, A.C.; Osman, I.; Polsky, D.; Berman, R.S. Role of radiologic imaging at the time of initial diagnosis of stage T1b-T3b melanoma. Cancer 2007, 110, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Pandalai, P.K.; Dominguez, F.J.; Michaelson, J.; Tanabe, K.K. Clinical Value of Radiographic Staging in Patients Diagnosed With AJCC Stage III Melanoma. Ann. Surg. Oncol. 2010, 18, 506–513. [Google Scholar] [CrossRef] [PubMed]
- NCCN Guidelines Version 3.2020 Cutaneous Melanoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf (accessed on 16 June 2020).
- Swetter, S.M.; Tsao, H.; Bichakjian, C.K.; Curiel-Lewandrowski, C.; Elder, D.E.; Gershenwald, J.E.; Guild, V.; Grant-Kels, J.M.; Halpern, A.C.; Johnson, T.M.; et al. Guidelines of care for the management of primary cutaneous melanoma. J. Am. Acad. Dermatol. 2019, 80, 208–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Bastholt, L.; Bataille, V.; Del Marmol, V.; Dréno, B.; Fargnoli, M.C.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 1: Diagnostics – Update 2019. Eur. J. Cancer 2020, 126, 141–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, Y.; Yoshikawa, S.; Minagawa, A.; Takenouchi, T.; Yokota, K.; Uchi, H.; Noma, N.; Nakamura, Y.; Asai, J.; Kato, J.; et al. Clinical and histopathological characteristics and survival analysis of 4594 Japanese patients with melanoma. Cancer Med. 2019, 8, 2146–2156. [Google Scholar] [CrossRef] [PubMed]
- Tardelli, E.; Mazzarri, S.; Rubello, D.; Gennaro, M.; Fantechi, L.; Duce, V.; Romanini, A.; Chondrogiannis, S.; Volterrani, D.; Colletti, P.M.; et al. Sentinel Lymph Node Biopsy in Cutaneous Melanoma: Standard and New Technical Procedures and Clinical Advances. A Systematic Review of the Literature. Clin. Nucl. Med. 2016, 41, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Dai, B.; Kong, Y.; Shen, X.; Kong, J. Acral Melanoma in Chinese: A Clinicopathological and Prognostic Study of 142 cases. Sci. Rep. 2016, 6, 31432. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Parameters | Number (%) |
|---|---|
| Age, years | |
| Mean (median) | 66.3 (69) |
| Range | 16–90 |
| Sex | |
| Male | 46 (42.2) |
| Female | 63 (57.8) |
| Primary site | |
| Foot | 64 (58.7) |
| Hand | 21 (19.3) |
| Toenail | 14 (12.8) |
| Fingernail | 10 (9.2) |
| Breslow thickness | |
| Tis | 22 (20.2) |
| T1 | 25 (22.9) |
| T2 | 14 (12.8) |
| T3 | 15 (13.8) |
| T4 | 33 (30.3) |
| Ulceration | |
| Present | 33 (30.3) |
| Absent | 76 (69.7) |
| Lymphadenopathy | |
| Present | 9 (8.3) |
| Absent | 100 (91.7) |
| Imaging modality | |
| CT alone | 20 (18.3) |
| CT and PET/CT | 89 (81.7) |
| Detection of Lymph Node Metastasis | ||||
| Patients | Positive in Imaging | Metastasis in Histopathology | Positive Predictive Value | |
| CT alone | 17 | 2 (11.8%) | 1 (5.9%) | 50.0% |
| CT and PET/CT | 83 | 15 (18.1%) | 1 (1.2%) | 6.7% |
| Total | 100 | 17 (17.0%) | 2 (2.0%) | 11.8% |
| Detection of Distant Metastasis | ||||
| Patients | Positive in Imaging | Metastasis Confirmed during Follow-up | Positive Predictive Value | |
| CT alone | 17 | 1 (5.9%) | 0 (0%) | 0% |
| CT and PET/CT | 83 | 3 (3.6%) | 0 (0%) | 0% |
| Total | 100 | 4 (4.0%) | 0 (0%) | 0% |
| Detection of Lymph Node Metastasis | ||||
| Patients | Positive in Imaging | Metastasis in Histopathology | Positive Predictive Value | |
| Tis | 22 | 4 (18.2%) | 0 (0%) | 0% |
| T1 | 24 | 4 (16.7%) | 0 (0%) | 0% |
| T2 | 14 | 2 (14.3%) | 0 (0%) | 0% |
| T3 | 13 | 2 (15.4%) | 0 (0%) | 0% |
| T4 | 27 | 5 (18.5%) | 2 (7.4%) | 40.0% |
| Detection of Distant Metastasis | ||||
| Patients | Positive in Imaging | Metastasis Confirmed during Follow-up | Positive Predictive Value | |
| Tis | 22 | 0 (0%) | 0 (0%) | - |
| T1 | 24 | 0 (0%) | 0 (0%) | - |
| T2 | 14 | 2 (14.3%) | 0 (0%) | 0% |
| T3 | 13 | 1 (7.7%) | 0 (0%) | 0% |
| T4 | 27 | 1 (3.7%) | 0 (0%) | 0% |
| Patients | Age | Sex | Primary site | T category | N category | Site of Distant Metastasis |
|---|---|---|---|---|---|---|
| #1 | 74 | Male | Foot | T1a | N3b | - |
| #2 | 74 | Male | Foot | T3a | N3b | Liver |
| #3 | 64 | Male | Foot | T3a | N3b | - |
| #4 | 74 | Male | Toenail | T4a | N2b | - |
| #5 | 79 | Male | Fingernail | T4a | N1c | - |
| #6 | 63 | Male | Hand | T4b | N3c | Paraaortic LN |
| #7 | 74 | Male | Foot | T4b | N3b | Paraaortic LN |
| #8 | 69 | Male | Foot | T4b | N3c | Lung |
| #9 | 76 | Female | Hand | T4b | N1b | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ide, T.; Ito, T.; Wada-Ohno, M.; Furue, M. Preoperative Screening CT and PET/CT Scanning for Acral Melanoma: Is it Necessary? J. Clin. Med. 2021, 10, 811. https://doi.org/10.3390/jcm10040811
Ide T, Ito T, Wada-Ohno M, Furue M. Preoperative Screening CT and PET/CT Scanning for Acral Melanoma: Is it Necessary? Journal of Clinical Medicine. 2021; 10(4):811. https://doi.org/10.3390/jcm10040811
Chicago/Turabian StyleIde, Taketoshi, Takamichi Ito, Maiko Wada-Ohno, and Masutaka Furue. 2021. "Preoperative Screening CT and PET/CT Scanning for Acral Melanoma: Is it Necessary?" Journal of Clinical Medicine 10, no. 4: 811. https://doi.org/10.3390/jcm10040811