
Cutaneous and Mucosal Melanomas of Uncommon Sites: Where Do We Stand Now?

 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Cutaneous Melanomas at Uncommon Sites
2.1. Acral Melanomas
2.2. Scalp Melanomas
3. Mucosal Melanomas at Uncommon Sites
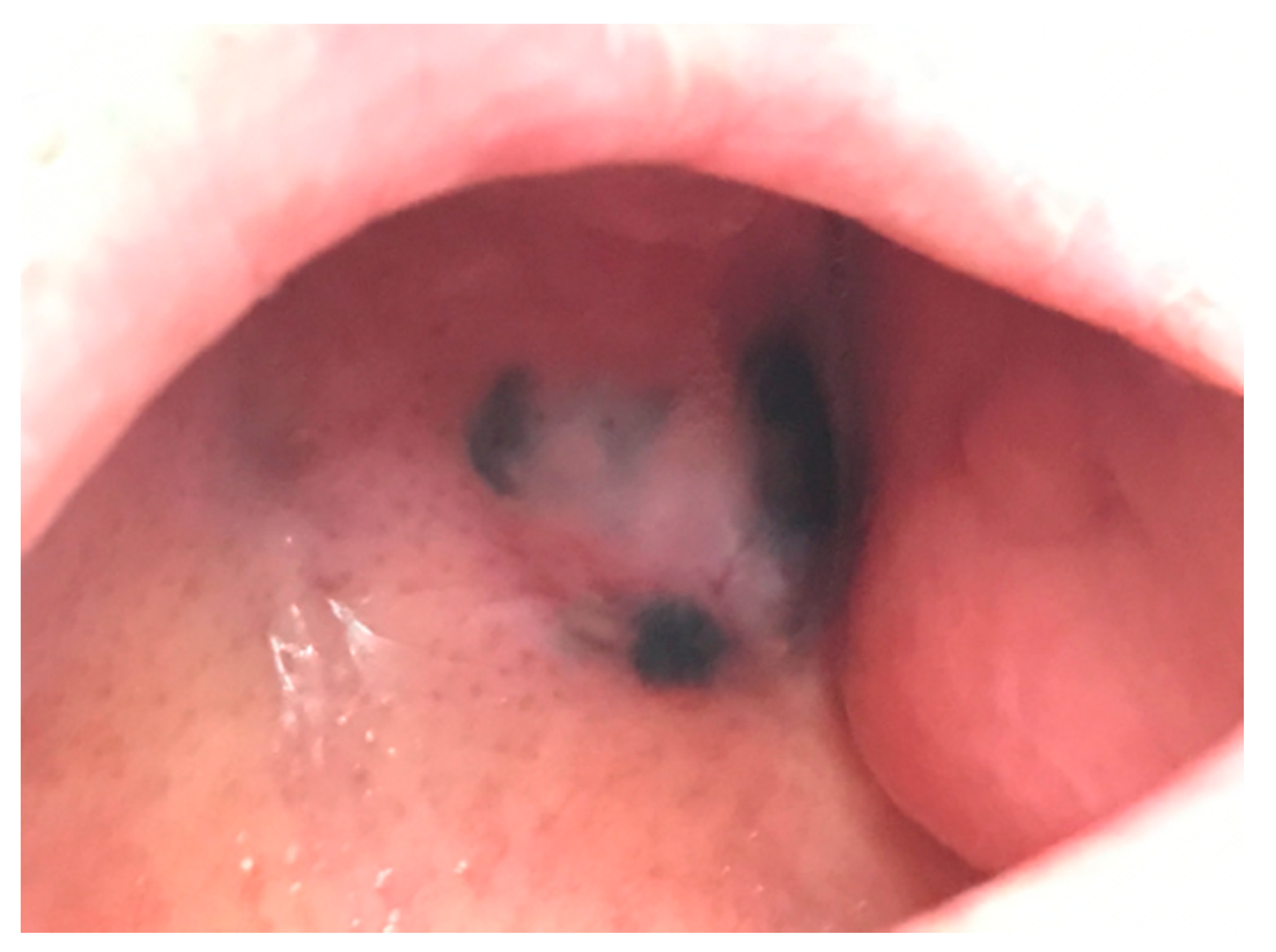
3.1. Oral Melanomas
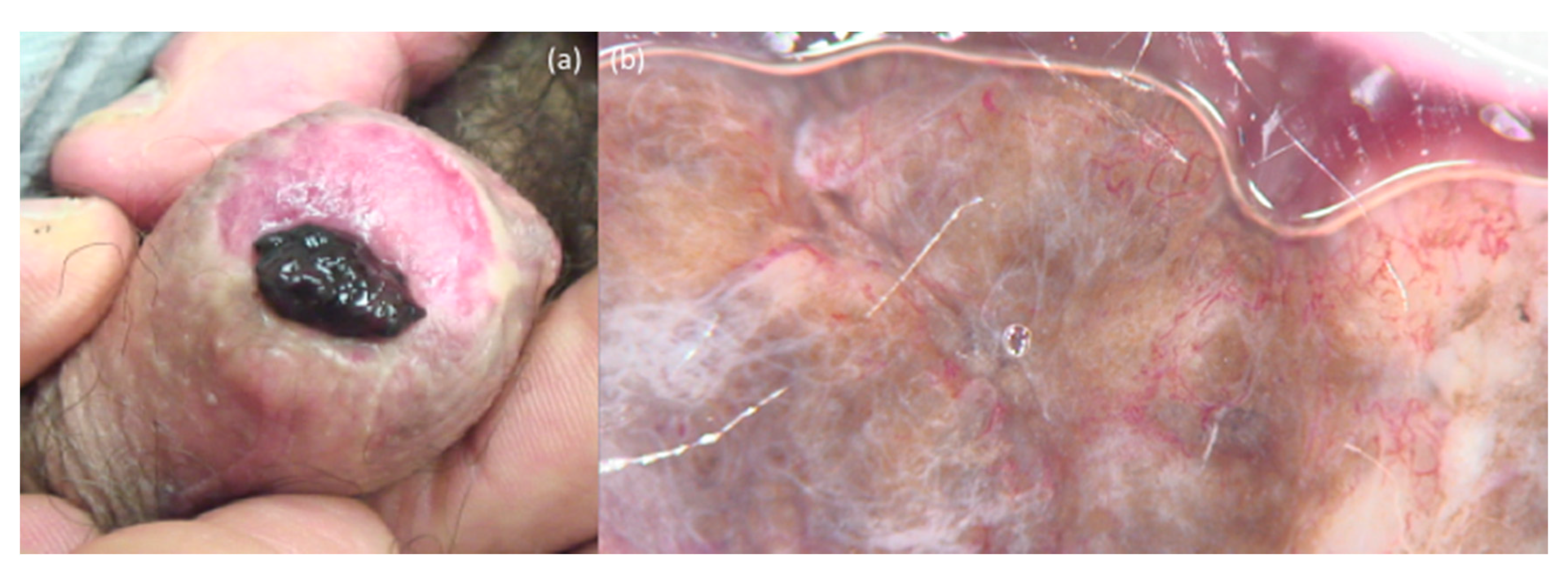
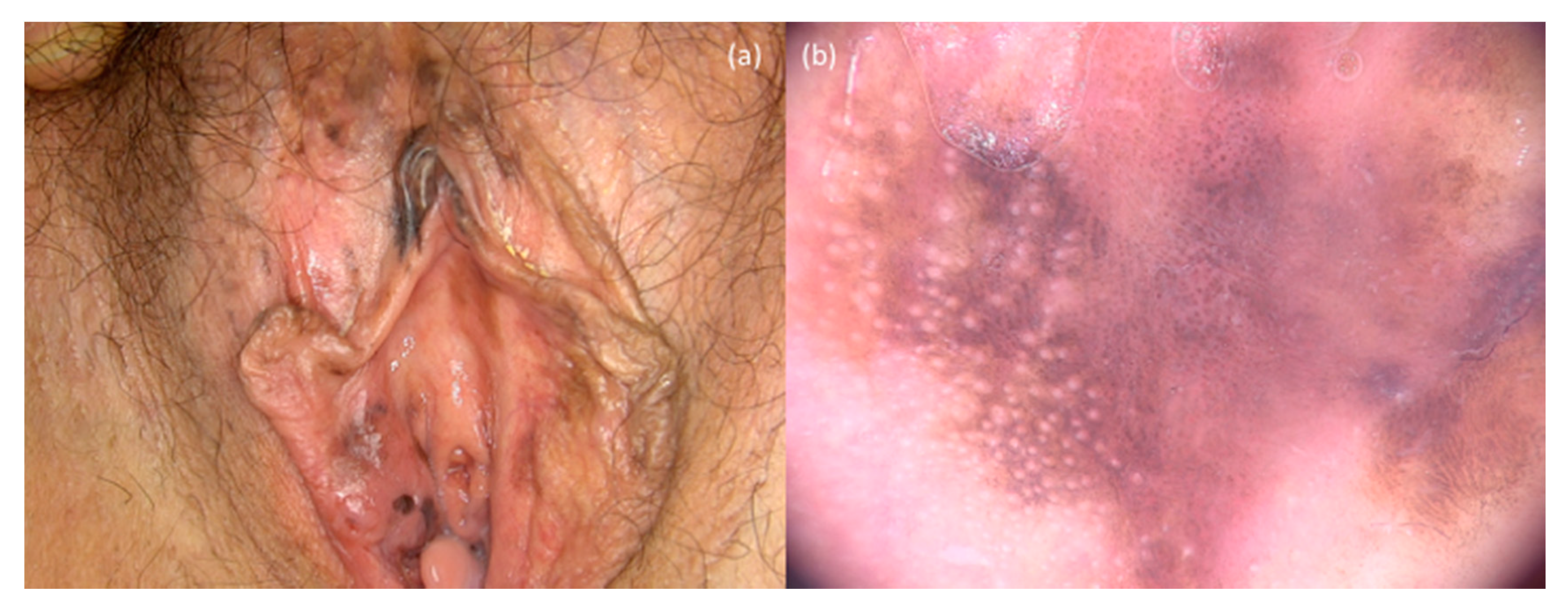
3.2. Genital Melanomas
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Shi, K.; Zhang, B.; Kong, B.Y.; Zhang, Y.; Igartua, C.; Mohan, L.S.; Quan, V.L.; Panah, E.; Isales, M.C.; Beaubier, N.; et al. Distinct Genomic Features in a Retrospective Cohort of Mucosal, Acral and Vulvovaginal Melanomas. J. Am. Acad. Dermatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, G.M.; Dika, E.; Lambertini, M.; Chessa, M.A.; Fanti, P.; Patrizi, A. Acral melanoma: Correlating the clinical presentation to the mutational status. G. Ital. Dermatol. Venereol. 2018, 154, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Costello, C.M.; Pittelkow, M.R.; Mangold, A.R. Acral Melanoma and Mechanical Stress on the Plantar Surface of the Foot. N. Engl. J. Med. 2017, 377, 395–396. [Google Scholar] [CrossRef] [PubMed]
- Fanti, P.A.; Dika, E.; Misciali, C.; Vaccari, S.; Barisani, A.; Piraccini, B.M.; Cavrin, G.; Maibach, H.I.; Patrizi, A. Nail apparatus melanoma: Is trauma a coincidence? Is this peculiar tumor a real acral melanoma? Cutan. Ocul. Toxicol. 2013, 32, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Rawson, R.V.; Johansson, P.A.; Hayward, N.K.; Waddell, N.; Patch, A.-M.; Lo, S.; Pearson, J.V.; Thompson, J.F.; Mann, G.J.; Scolyer, R.A.; et al. Unexpected UVR and non-UVR mutation burden in some acral and cutaneous melanomas. Lab. Investig. 2017, 97, 130–145. [Google Scholar] [CrossRef] [Green Version]
- Brash, D.E. UV Signature Mutations. Photochem. Photobiol. 2015, 91, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Baran, R.; Juhlin, L. Drug-induced photo-onycholysis: Three sub-types revealed in a study of 15 cases. Br. J. Dermatol. 1987, 117, 26–27. [Google Scholar] [CrossRef]
- Dika, E.; Starace, M.; Lambertini, M.; Patrizi, A.; Veronesi, G.; Alessandrini, A.; Piraccini, B.M. Oral and nail pigmentations: A useful parallelism for the clinician. JDDG 2020, 18, 7–14. [Google Scholar] [CrossRef]
- Lee, D.J.R.; Arbache, S.T.; Quaresma, M.V.; Nico, M.M.S.; Gabbi, T.V.B. Nail Apparatus Melanoma: Experience of 10 Years in a Single Institution. Skin Appendage Disord. 2019, 5, 20–26. [Google Scholar] [CrossRef]
- Lambertini, M.; Filippi, F.; Traniello Gradassi, A.; Magni, L.; Dika, E. Multiple Digit Melanonychia: Examine the Scalp. J. Am. Acad. Dermatol. 2017, 78, e97–e98. [Google Scholar] [CrossRef]
- Benati, E.; Ribero, S.; Longo, C.; Piana, S.; Puig, S.; Carrera, C.; Cicero, F.; Kittler, H.; Deinlein, T.; Zalaudek, I.; et al. Clinical and dermoscopic clues to differentiate pigmented nail bands: An International Dermoscopy Society study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Piraccini, B.M.; Dika, E.; Fanti, P.A. Tips for diagnosis and treatment of nail pigmentation with practical algorithm. Dermatol. Clin. 2015, 33, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Starace, M.; Dika, E.; Fanti, P.A.; Patrizi, A.; Misciali, C.; Alessandrini, A.; Bruni, F.; Piraccini, B.M. Nail apparatus melanoma: Dermoscopic and histopathologic correlations on a series of 23 patients from a single centre. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Dika, E.; Patrizi, A.; Fanti, P.A.; Christman, H.; Misciali, C.; Piraccini, B.M. An asymptomatic subungual nodule. J. Am. Acad. Dermatol. 2016, 74, e27–e28. [Google Scholar] [CrossRef]
- Desai, A.; Ugorji, R.; Khachemoune, A. Acral melanoma foot lesions. Part 2: Clinical presentation, diagnosis, and management. Clin. Exp. Dermatol. 2018, 43, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Koga, H.; Saida, T. Revised 3-Step Dermoscopic Algorithm for the Management of Acral Melanocytic Lesions. Arch. Dermatol. 2011, 147, 741. [Google Scholar] [CrossRef] [Green Version]
- Dika, E.; Veronesi, G.; Altimari, A.; Riefolo, M.; Ravaioli, G.M.; Piraccini, B.M.; Lambertini, M.; Campione, E.; Gruppioni, E.; Fiorentino, M.; et al. BRAF, KIT, and NRAS Mutations of Acral Melanoma in White Patients. Am. J. Clin. Pathol. 2020, 153, 664–671. [Google Scholar] [CrossRef]
- Lambertini, M.; Piraccini, B.M.; Fanti, P.A.; Dika, E. Mohs micrographic surgery for nail unit tumours: An update and a critical review of the literature. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1638–1644. [Google Scholar] [CrossRef]
- Brodland, D.G. The treatment of nail apparatus melanoma with Mohs micrographic surgery. Dermatol. Surg. 2001, 27, 269–273. [Google Scholar]
- Lieberherr, S.; Cazzaniga, S.; Haneke, E.; Hunger, R.E.; Seyed Jafari, S.M. Melanoma of the nail apparatus: A systematic review and meta-analysis of current challenges and prognosis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 967–976. [Google Scholar] [CrossRef]
- Dika, E.; Patrizi, A.; Fanti, P.A.; Chessa, M.A.; Reggiani, C.; Barisani, A.; Piraccini, B.M. The Prognosis of Nail Apparatus Melanoma: 20 Years of Experience from a Single Institute. Dermatology (Basel) 2016, 232, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Hayward, N.K.; Wilmott, J.S.; Waddell, N.; Johansson, P.A.; Field, M.A.; Nones, K.; Patch, A.; Kakavand, H.; Alexandrov, L.B.; Burke, H.; et al. Whole-genome landscapes of major melanoma subtypes. Nature 2017, 545, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Darmawan, C.C.; Jo, G.; Montenegro, S.E.; Kwak, Y.; Cheol, L.; Cho, K.H.; Mun, J. Early detection of acral melanoma: A review of clinical, dermoscopic, histopathologic, and molecular characteristics. J. Am. Acad. Dermatol. 2019, 81, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.S.; Hendricks, W.; Kiefer, J.; Schmidt, J.; Sekar, S.; Carpten, J.; Craig, D.W.; Adkins, J.; Cuyugan, L.; Manojlovic, Z.; et al. Integrated genomic analyses reveal frequent TERT aberrations in acral melanoma. Genome Res. 2017, 27, 524–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaremba, A.; Murali, R.; Jansen, P.; Möller, I.; Sucker, A.; Paschen, A.; Livingstone, E.; Brinker, T.J.; Hadaschik, E.; Franklin, C.; et al. Clinical and genetic analysis of melanomas arising in acral sites. Eur. J. Cancer 2019, 119, 66–76. [Google Scholar] [CrossRef]
- Yeh, I.; Jorgenson, E.; Shen, L.; Xu, M.; North, J.P.; Shain, A.H.; Reuss, D.; Wu, H.; Robinson, W.A.; Olshen, A.; et al. Targeted Genomic Profiling of Acral Melanoma. J. Natl. Cancer Inst. 2019, 111, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Tate, J.G.; Bamford, S.; Jubb, H.C.; Sondka, Z.; Beare, D.M.; Bindal, N.; Flanagan, A.; Teague, J.; Futreal, P.A.; Stratton, M.R.; et al. COSMIC: The Catalogue Of Somatic Mutations In Cancer. Nucleic Acids Res. 2019, 47, D941–D947. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Yoon, J.; Chung, Y.-J.; Lee, S.Y.; Choi, J.Y.; Shin, O.R.; Park, H.Y.; Bahk, W.J.; Yu, D.S.; Lee, Y.B. Whole-exome sequencing reveals differences between nail apparatus melanoma and acral melanoma. J. Am. Acad. Dermatol. 2018, 79, 559–561.e1. [Google Scholar] [CrossRef] [Green Version]
- Hodi, F.S.; Corless, C.L.; Giobbie-Hurder, A.; Fletcher, J.A.; Zhu, M.; Marino-Enriquez, A.; Friedlander, P.; Gonzalez, R.; Weber, J.S.; Gajewski, T.F.; et al. Imatinib for Melanomas Harboring Mutationally Activated or Amplified KIT Arising on Mucosal, Acral, and Chronically Sun-Damaged Skin. J. Clin. Oncol. 2013, 31, 3182–3190. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Si, L.; Kong, Y.; Flaherty, K.T.; Xu, X.; Zhu, Y.; Corless, C.L.; Li, L.; Li, H.; Sheng, X.; et al. Phase II, Open-Label, Single-Arm Trial of Imatinib Mesylate in Patients With Metastatic Melanoma Harboring c-Kit Mutation or Amplification. J. Clin. Oncol. 2011, 29, 2904–2909. [Google Scholar] [CrossRef]
- Shoushtari, A.N.; Munhoz, R.R.; Kuk, D.; Ott, P.A.; Johnson, D.B.; Tsai, K.K.; Rapisuwon, S.; Eroglu, Z.; Sullivan, R.J.; Luke, J.J.; et al. The efficacy of anti-PD-1 agents in acral and mucosal melanoma: PD-1 in Acral or Mucosal Melanoma. Cancer 2016, 122, 3354–3362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namin, A.W.; Cornell, G.E.; Thombs, L.A.; Zitsch, R.P. Patterns of recurrence and retreatment outcomes among clinical stage I and II head and neck melanoma patients. Head Neck 2019, 41, 1304–1311. [Google Scholar] [CrossRef] [PubMed]
- Unsal, A.A.; Patel, V.R.; Chung, S.Y.; Zhou, A.H.; Baredes, S.; Eloy, J.A. Head and neck sweat gland adenocarcinoma: A population-based perspective of a rare entity: Head and Neck Sweat Gland Adenocarcinoma. Laryngoscope 2017, 127, 2757–2762. [Google Scholar] [CrossRef] [PubMed]
- Conley, J.J. Management of malignant tumors of the scalp. Ann. N. Y. Acad. Sci. 1964, 114, 976–984. [Google Scholar] [CrossRef]
- Xie, C.; Pan, Y.; McLean, C.; Mar, V.; Wolfe, R.; Kelly, J.W. Scalp melanoma: Distinctive high risk clinical and histological features. Australas. J. Dermatol. 2017, 58, 181–188. [Google Scholar] [CrossRef]
- Pillemer, B.B.L.; Pugliano-Mauro, M.A.; Ferris, L.K.; Patton, T.J. Three cases of scalp melanomas discovered by hairdressers. J. Clin. Aesthet. Dermatol. 2013, 6, 32–34. [Google Scholar]
- Torres, F.; Fabbrocini, G.; Hirata, S.H.; Yamada, S.; De Vita, V.; Annunziata, M.C.; Tosti, A. Dermoscopy of Scalp Melanoma: Report of Three Cases. Cancers 2010, 2, 1597–1601. [Google Scholar] [CrossRef]
- Tiodorovic-Zivkovic, D.; Zalaudek, I.; Lallas, A.; Stratigos, A.; Piana, S.; Argenziano, G. The importance of gray color as a dermoscopic clue in facial pigmented lesion evaluation: A case report. Dermatol. Pract. Concept. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Tschandl, P.; Rosendahl, C.; Kittler, H. Dermatoscopy of flat pigmented facial lesions. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 120–127. [Google Scholar] [CrossRef]
- Howard, M.D.; Wee, E.; Wolfe, R.; McLean, C.A.; Kelly, J.W.; Pan, Y. Anatomic location of primary melanoma: Survival differences and sun exposure. J. Am. Acad. Dermatol. 2019, 81, 500–509. [Google Scholar] [CrossRef]
- Pozdnyakova, O.; Grossman, J.; Barbagallo, B.; Lyle, S. The hair follicle barrier to involvement by malignant melanoma. Cancer 2009, 115, 1267–1275. [Google Scholar] [CrossRef]
- Dika, E.; Veronesi, G.; Misciali, C.; Corti, B.; Dika, I.; Riefolo, M.; Scarfì, F.; Lambertini, M.; Patrizi, A. Malignant Melanoma Cells and Hair Follicles. Am. J. Clin. Pathol. 2019, 152, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Tjarks, B.J.; Somani, N.; Piliang, M.; Bergfeld, W.F. A proposed classification for follicular involvement by melanoma: Patterns of follicular involvement by melanoma. J. Cutan. Pathol. 2017, 44, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Connolly, K.L.; Giordano, C.; Dusza, S.; Busam, K.J.; Nehal, K. Follicular involvement is frequent in lentigo maligna: Implications for treatment. J. Am. Acad. Dermatol. 2019, 80, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.G.; Spatz, A.; Bröcker, E.-B.; Ruiter, D.J. Identification of histological features associated with metastatic potential in thin (<1.0 mm) cutaneous melanoma with metastases. A study on behalf of the EORTC Melanoma Group: Histological features as-sociated with metastatic potential in thin (<1.0 mm) cutaneous melanoma with metastases. J. Pathol. 2002, 197, 188–193. [Google Scholar] [CrossRef]
- Scolyer, R.A.; Judge, M.J.; Evans, A.; Frishberg, D.P.; Prieto, V.G.; Thompson, J.F.; Trotter, M.J.; Walsh, M.Y.; Walsh, N.M.; Ellis, D.W.; et al. Data Set for Pathology Reporting of Cutaneous Invasive Melanoma: Recommendations From the International Collaboration on Cancer Reporting (ICCR). Am. J. Surg. Pathol. 2013, 37, 1797–1814. [Google Scholar] [CrossRef]
- Dika, E.; Lambertini, M.; Patrizi, A.; Misciali, C.; Altimari, A.; Fiorentino, M.; Melotti, B.; Corti, B.; Riefolo, M.; Veronesi, G. Frequency of somatic mutations in head and neck melanoma: A single institution experience. Pigment Cell Melanoma Res. 2020, 33, 515–517. [Google Scholar] [CrossRef]
- Tas, F.; Erturk, K. Scalp melanoma is associated with high mitotic rate and is a poor prognostic factor for recurrence and outcome. Melanoma Res. 2017, 27, 387–390. [Google Scholar] [CrossRef]
- Su, A.; Low, L.; Li, X.; Zhou, S.; Mascarenhas, L.; Barnhill, R.L. De Novo Congenital Melanoma: Analysis of 2 Cases With Array Comparative Genomic Hybridization. Am. J. Dermatopathol. 2014, 36, 915–919. [Google Scholar] [CrossRef]
- Hocker, T.L.; Singh, M.K.; Tsao, H. Melanoma Genetics and Therapeutic Approaches in the 21st Century: Moving from the Benchside to the Bedside. J. Investig. Dermatol. 2008, 128, 2575–2595. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.D. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Mucosal Melanomas. Head Neck Pathol. 2017, 11, 110–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, R.J.; Fenske, N.A.; Messina, J.L. Primary mucosal melanoma. J. Am. Acad. Dermatol. 2007, 56, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Accorona, R.; Botti, G.; Farina, D.; Fossati, P.; Gatta, G.; Gogas, H.; Lombardi, D.; Maroldi, R.; Nicolai, P.; et al. Mucosal melanoma of the head and neck. Crit. Rev. Oncol. Hematol. 2017, 112, 136–152. [Google Scholar] [CrossRef] [PubMed]
- Hicks, M.J.; Flaitz, C.M. Oral mucosal melanoma: Epidemiology and pathobiology. Oral Oncol. 2000, 36, 152–169. [Google Scholar] [CrossRef]
- Warszawik-Hendzel, O.; Słowińska, M.; Olszewska, M.; Rudnicka, L. Melanoma of the oral cavity: Pathogenesis, dermoscopy, clinical features, staging and management. J. Dermatol. Case Rep. 2014, 8, 60. [Google Scholar] [CrossRef] [Green Version]
- Olszewska, M.; Banka, A.; Gorska, R.; Warszawik, O. Dermoscopy of pigmented oral lesions. J. Dermatol. Case Rep. 2008, 2, 43. [Google Scholar] [CrossRef]
- McLean, N.; Tighiouart, M.; Muller, S. Primary mucosal melanoma of the head and neck. Comparison of clinical presentation and histopathologic features of oral and sinonasal melanoma. Oral Oncol. 2008, 44, 1039–1046. [Google Scholar] [CrossRef]
- Lambertini, M.; Patrizi, A.; Fanti, P.A.; Melotti, B.; Caliceti, U.; Magnoni, C.; Misciali, C.; Baraldi, C.; Ravaioli, G.M.; Dika, E. Oral melanoma and other pigmentations: When to biopsy? J. Eur. Acad. Dermatol. Venereol. 2018, 32, 209–214. [Google Scholar] [CrossRef]
- Kahn, M.A.; Weathers, D.R.; Hoffman, J.G. Transformation of a benign oral pigmentation to primary oral melanoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 454–459. [Google Scholar] [CrossRef]
- Ballester Sánchez, R.; de Unamuno Bustos, B.; Navarro Mira, M.; Botella Estrada, R. Actualización en melanoma mucoso. Actas Dermo-Sifiliográficas 2015, 106, 96–103. [Google Scholar] [CrossRef]
- De Piano, E.; Cinotti, E.; Tognetti, L.; Rubegni, P. Commentary on ‘Oral melanoma and other pigmentations: When to biopsy’? J. Eur. Acad. Dermatol. Venereol. 2018, 32, e398–e399. [Google Scholar] [CrossRef] [PubMed]
- Dika, E.; Lambertini, M. Reply to the commentary on ‘Oral melanoma and other pigmentations: When to biopsy’? J. Eur. Acad. Dermatol. Venereol. 2018, 32, e399. [Google Scholar] [CrossRef] [PubMed]
- Hajar-Serviansky, T.; Gutierrez-Mendoza, D.; Galvan, I.L.; Lammoglia-Ordiales, L.; Mosqueda-Taylor, A.; Hernandez-Cázares, M.L.; Toussaint-Caire, S. A case of oral mucosal melanoma. Clinical and dermoscopic correlation. J. Dermatol. Case Rep. 2012, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambertini, M.; Patrizi, A.; Ravaioli, G.M.; Dika, E. Oral pigmentation in physiologic conditions, post-inflammatory affections and systemic diseases. G. Ital. Dermatol. Venereol. 2018, 153, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Feller, L.; Khammissa, R.A.G.; Lemmer, J. A Review of the Aetiopathogenesis and Clinical and Histopathological Features of Oral Mucosal Melanoma. Sci. World J. 2017, 2017, 9189812. [Google Scholar] [CrossRef]
- Wu, Y.; Zhong, Y.; Li, C.; Song, H.; Guo, W.; Ren, G. Neck dissection for oral mucosal melanoma: Caution of nodular lesion. Oral Oncol. 2014, 50, 319–324. [Google Scholar] [CrossRef]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Exp. Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef]
- Krengli, M.; Masini, L.; Kaanders, J.H.A.M.; Maingon, P.; Oei, S.B.; Zouhair, A.; Ozyar, E.; Roelandts, M.; Amichetti, M.; Bosset, M.; et al. Radiotherapy in the treatment of mucosal melanoma of the upper aerodigestive tract: Analysis of 74 cases. A Rare Cancer Network study. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 751–759. [Google Scholar] [CrossRef]
- Medina, J.E.; Ferlito, A.; Pellitteri, P.K.; Shaha, A.R.; Khafif, A.; Devaney, K.O.; Fisher, S.R.; O’Brien, C.J.; Byers, R.M.; Robbins, K.T.; et al. Current management of mucosal melanoma of the head and neck. J. Surg. Oncol. 2003, 83, 116–122. [Google Scholar] [CrossRef]
- Song, H.; Wang, L.; Lyu, J.; Wu, Y.; Guo, W.; Ren, G. Loss of nuclear BAP1 expression is associated with poor prognosis in oral mucosal melanoma. Oncotarget 2017, 8, 29080–29090. [Google Scholar] [CrossRef] [Green Version]
- Zhou, R.; Shi, C.; Tao, W.; Li, J.; Wu, J.; Han, Y.; Yang, G.; Gu, Z.; Xu, S.; Wang, Y.; et al. Analysis of Mucosal Melanoma Whole-Genome Landscapes Reveals Clinically Relevant Genomic Aberrations. Clin. Cancer Res. 2019, 25, 3548–3560. [Google Scholar] [CrossRef] [Green Version]
- Lyu, J.; Song, Z.; Chen, J.; Shepard, M.J.; Song, H.; Ren, G.; Li, Z.; Guo, W.; Zhuang, Z.; Shi, Y. Whole-exome sequencing of oral mucosal melanoma reveals mutational profile and therapeutic targets: WES of OMM reveals genomic alterations. J. Pathol. 2018, 244, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Mignard, C.; Deschamps Huvier, A.; Gillibert, A.; Duval Modeste, A.B.; Dutriaux, C.; Khammari, A.; Kramkimel, N.; Mortier, L.; Marcant, P.; Lesimple, T.; et al. Efficacy of Immunotherapy in Patients with Metastatic Mucosal or Uveal Melanoma. J. Oncol. 2018, 2018, 1908065. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, Y.; Sadahira, T.; Mitsui, Y.; Wada, K.; Tanimoto, R.; Kobayashi, Y.; Araki, M.; Watanabe, M.; Watanabe, T.; Nasu, Y. Red nodular melanoma of the penile foreskin: A case report and literature review. Mol. Clin. Oncol. 2018, 9, 449–452. [Google Scholar] [CrossRef] [Green Version]
- Saglam, O.; Naqvi, S.M.H.; Zhang, Y.; Mesa, T.; Teer, J.K.; Yoder, S.; Lee, J.; Messina, J. Female genitourinary tract melanoma: Mutation analysis with clinicopathologic correlation. Melanoma Res. 2018, 28, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Lorusso, D.; Raspagliesi, F.; Del Vecchio, M. Investigating the role of immunotherapy in advanced/recurrent female genital tract melanoma: A preliminary experience. J. Gynecol. Oncol. 2019, 30. [Google Scholar] [CrossRef]
- Vaccari, S.; Barisani, A.; Dika, E.; Fanti, P.A.; Iaco, P.D.; Gurioli, C.; Tosti, G. Management and treatment of mucosal melanoma of the genital tract. G. Ital. Dermatol. Venereol. 2017, 152, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Wohlmuth, C.; Wohlmuth-Wieser, I.; May, T.; Vicus, D.; Gien, L.T.; Laframboise, S. Malignant Melanoma of the Vulva and Vagina: A US Population-Based Study of 1863 Patients. Am. J. Clin. Dermatol. 2020, 21, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Scalvenzi, M.; Palmisano, F.; Russo, D.; Mascolo, M.; Costa, C. Melanoma of the glans penis successfully treated with topical imiquimod: Dermoscopy usefulness in clinical monitoring and review of the literature. G. Ital. Dermatol. Venereol. 2017, 152, 663–668. [Google Scholar] [CrossRef]
- Tan, A.; Bieber, A.K.; Stein, J.A.; Pomeranz, M.K. Diagnosis and management of vulvar cancer: A review. J. Am. Acad. Dermatol. 2019, 81, 1387–1396. [Google Scholar] [CrossRef]
- Vaccari, S.; Barisani, A.; Dika, E.; Fanti, P.A.; D’antuono, A.; Gaspari, V.; Tosti, G.; Patrizi, A. Genital bowenoid papulosis: The variegated dermoscopic features. G. Ital. Dermatol. Venereol. 2018, 153, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Carinelli, S.; Guerrieri, M.E.; Aletti, G.D. Melanoma of the lower genital tract: Prognostic factors and treatment modalities. Gynecol. Oncol. 2018, 150, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Bittar, J.M.; Bittar, P.G.; Wan, M.T.; Kovell, R.C.; Guzzo, T.J.; Shin, T.M.; Etzkorn, J.R.; Sobanko, J.F.; Miller, C.J. Systematic Review of Surgical Treatment and Outcomes After Local Surgery of Primary Cutaneous Melanomas of the Penis and Scrotum. Dermatol. Surg. 2018, 44, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Dika, E.; Fanti, P.A.; Patrizi, A.; Christman, H.; Baraldi, C.; Lambertini, M. Unsuccessful treatment of penile intraepithelial neoplasia with Mohs micrographic surgery. G. Ital. Dermatol. Venereol. 2019. [Google Scholar] [CrossRef]
- van Geel, A.N.; den Bakker, M.A.; Kirkels, W.; Horenblas, S.; Kroon, B.B.R.; de Wilt, J.H.W.; Eggermont, A.M.; Mooi, W.J.; van der Aa, M.N. Prognosis of Primary Mucosal Penile Melanoma: A Series of 19 Dutch Patients and 47 Patients from the Literature. Urology 2007, 70, 143–147. [Google Scholar] [CrossRef]
- Furney, S.J.; Turajlic, S.; Stamp, G.; Nohadani, M.; Carlisle, A.; Thomas, J.M.; Hayes, A.; Strauss, D.; Gore, M.; van den Oord, J.; et al. Genome sequencing of mucosal melanomas reveals that they are driven by distinct mechanisms from cutaneous melanoma: Whole genome sequencing of mucosal melanoma. J. Pathol. 2013, 230, 261–269. [Google Scholar] [CrossRef]
- Omholt, K.; Grafstrom, E.; Kanter-Lewensohn, L.; Hansson, J.; Ragnarsson-Olding, B.K. KIT Pathway Alterations in Mucosal Melanomas of the Vulva and Other Sites. Clin. Cancer Res. 2011, 17, 3933–3942. [Google Scholar] [CrossRef] [Green Version]
- Heinzelmann-Schwarz, V.A.; Nixdorf, S.; Valadan, M.; Diczbalis, M.; Olivier, J.; Otton, G.; Fedier, A.; Hacker, N.F.; Scurry, J.P. A clinicopathological review of 33 patients with vulvar melanoma identifies c-KIT as a prognostic marker. Int. J. Mol. Med. 2014, 33, 784–794. [Google Scholar] [CrossRef] [Green Version]
- Tseng, D.; Kim, J.; Warrick, A.; Nelson, D.; Pukay, M.; Beadling, C.; Heinrich, M.; Selim, M.A.; Corless, C.L.; Nelson, K. Oncogenic mutations in melanomas and benign melanocytic nevi of the female genital tract. J. Am. Acad. Dermatol. 2014, 71, 229–236. [Google Scholar] [CrossRef] [Green Version]
- van Engen-van Grunsven, A.C.H.; Küsters-Vandevelde, H.V.N.; De Hullu, J.; van Duijn, L.M.; Rijntjes, J.; Bovée, J.V.M.G.; Groenen, P.J.T.A.; Blokxa, W.A.M. NRAS mutations are more prevalent than KIT mutations in melanoma of the female urogenital tract—A study of 24 cases from the Netherlands. Gynecol. Oncol. 2014, 134, 10–14. [Google Scholar] [CrossRef]
- Rouzbahman, M.; Kamel-Reid, S.; Al Habeeb, A.; Butler, M.; Dodge, J.; Laframboise, S.; Murphy, J.; Rasty, G.; Ghazarian, D. Malignant Melanoma of Vulva and Vagina: A Histomorphological Review and Mutation Analysis—A Single-Center Study. J. Lower Genit. Tract Dis. 2015, 19, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Udager, A.M.; Frisch, N.K.; Hong, L.J.; Stasenko, M.; Johnston, C.M.; Liu, J.R.; Chan, M.P.; Harms, P.W.; Fullen, D.R.; Orsini, A.; et al. Gynecologic melanomas: A clinicopathologic and molecular analysis. Gynecol. Oncol. 2017, 147, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Wylomanski, S.; Denis, M.G.; Théoleyre, S.; Bouquin, R.; Vallée, A.; Knol, A.-C.; Saint-Jean, M.; Peuvrel, L.; Dréno, B.; Quéreux, G. BRAF mutations might be more common than supposed in vulvar melanomas. Exp. Dermatol. 2018, 27, 210–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarei, S.; Voss, J.S.; Jin, L.; Jenkins, S.M.; Bryce, A.H.; Erickson, L.A.; Bell, D.A.; Kipp, B.R.; Flotte, T.J. Mutational Profile in Vulvar, Vaginal, and Urethral Melanomas: Review of 37 Cases with Focus on Primary Tumor Site. Int. J. Gynecol. Pathol. 2020, 39, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Oiso, N.; Sakai, K.; Yanagihara, S.; Nishio, K.; Kawada, A. Genital mucosal melanoma with somatic SF3B1 R625C mutation. Eur. J. Dermatol. 2018, 28, 414–415. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Annessi, G.; Didona, D.; Didona, B. Multifocal melanoma in situ of the penis treated with topical Imiquimod. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Baraziol, R.; Schiavon, M.; Fraccalanza, E.; De Giorgi, G. Melanoma in situ of penis: A very rare entity. Medicine 2017, 96, e7652. [Google Scholar] [CrossRef]
- Riefolo, M.; Porcellini, E.; Dika, E.; Broseghini, E.; Ferracin, M. Interplay between small and long non-coding RNAs in cutaneous melanoma: A complex jigsaw puzzle with missing pieces. Mol. Oncol. 2019, 13, 74–98. [Google Scholar] [CrossRef]
- Dika, E.; Riefolo, M.; Porcellini, E.; Broseghini, E.; Ribero, S.; Senetta, R.; Osella-Abate, S.; Scarfì, F.; Lambertini, M.; Veronesi, G.; et al. Defining the prognostic role of microRNAs in cutaneous melanoma. J. Investig. Dermatol. 2020, 140, 2260–2267. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dika, E.; Lambertini, M.; Pellegrini, C.; Veronesi, G.; Melotti, B.; Riefolo, M.; Sperandi, F.; Patrizi, A.; Ricci, C.; Mussi, M.; et al. Cutaneous and Mucosal Melanomas of Uncommon Sites: Where Do We Stand Now? J. Clin. Med. 2021, 10, 478. https://doi.org/10.3390/jcm10030478
Dika E, Lambertini M, Pellegrini C, Veronesi G, Melotti B, Riefolo M, Sperandi F, Patrizi A, Ricci C, Mussi M, et al. Cutaneous and Mucosal Melanomas of Uncommon Sites: Where Do We Stand Now? Journal of Clinical Medicine. 2021; 10(3):478. https://doi.org/10.3390/jcm10030478
Chicago/Turabian StyleDika, Emi, Martina Lambertini, Cristina Pellegrini, Giulia Veronesi, Barbara Melotti, Mattia Riefolo, Francesca Sperandi, Annalisa Patrizi, Costantino Ricci, Martina Mussi, and et al. 2021. "Cutaneous and Mucosal Melanomas of Uncommon Sites: Where Do We Stand Now?" Journal of Clinical Medicine 10, no. 3: 478. https://doi.org/10.3390/jcm10030478