
Deep Learning to Distinguish ABCA4-Related Stargardt Disease from PRPH2-Related Pseudo-Stargardt Pattern Dystrophy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Database
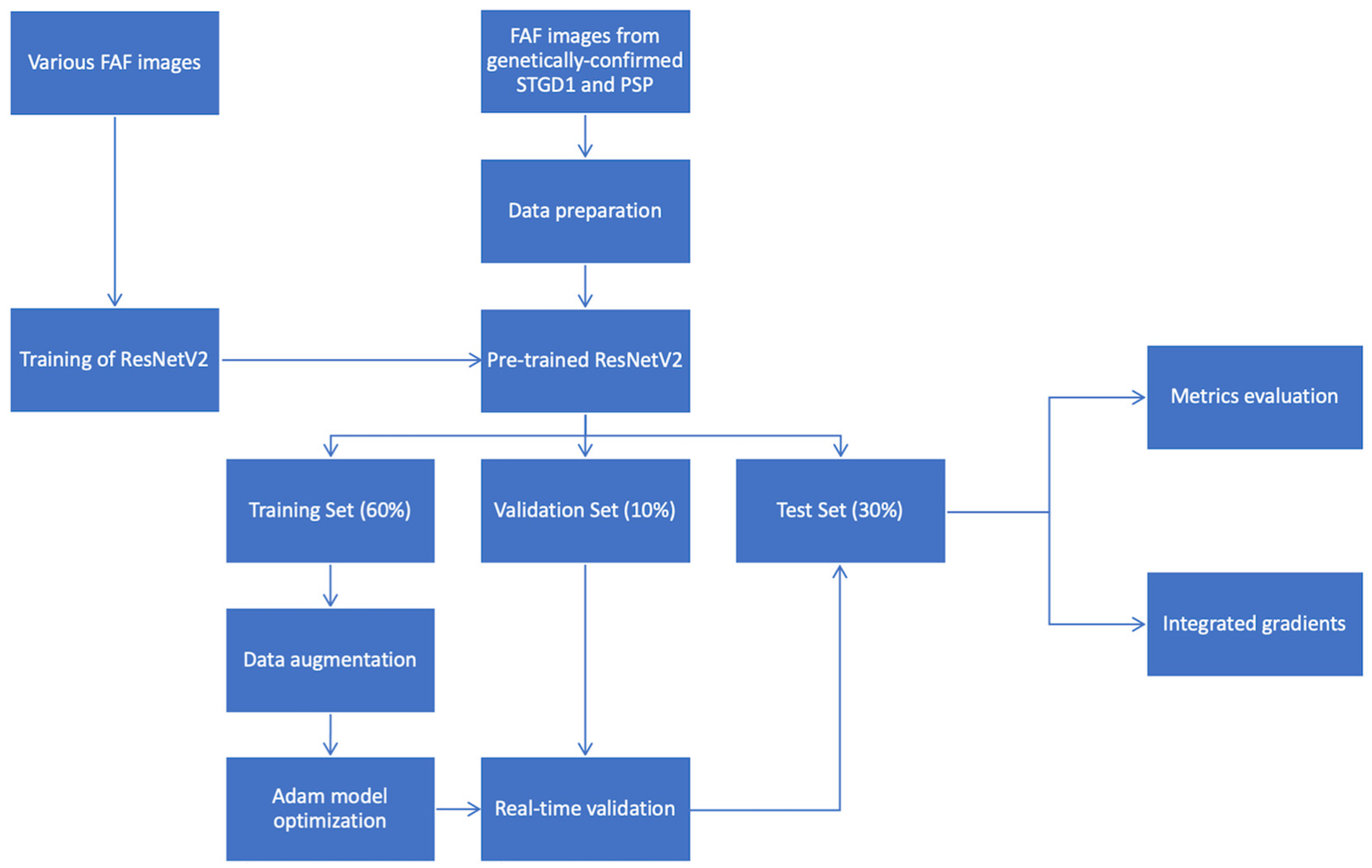
2.2. Development of a Deep Learning Classifier
2.3. Evaluation of Retina Specialists’ Performance
3. Results
3.1. Deep Learning Classifier
3.2. Evaluation of Retina Specialists’ Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Molday, L.L.; Rabin, A.R.; Molday, R.S. ABCR expression in foveal cone photoreceptors and its role in Stargardt macular dystrophy. Nat. Genet. 2000, 25, 257–258. [Google Scholar] [CrossRef]
- Allikmets, R.; Singh, N.; Sun, H.; Shroyer, N.; Hutchinson, A.; Chidambaram, A.; Gerrard, B.; Baird, L.; Stauffer, D.; Peiffer, A.; et al. A photoreceptor cell-specific ATP-binding transporter gene (ABCR) is mutated in recessive Starqardt macular dystrophy. Nat. Genet. 1997, 15, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Haaften, S.C.W.-V.; Boon, C.J.; Cremers, F.P.; Hoefsloot, L.H.; Hollander, A.I.D.; Hoyng, C.B. Clinical and Genetic Characteristics of Late-onset Stargardt’s Disease. Ophthalmology 2012, 119, 1199–1210. [Google Scholar] [CrossRef]
- Zernant, J.; Lee, W.; Collison, F.T.; Fishman, G.A.; Sergeev, Y.V.; Schuerch, K.; Sparrow, J.R.; Tsang, S.H.; Allikmets, R. Frequent hypomorphic alleles account for a significant fraction of ABCA4 disease and distinguish it from age-related macular degeneration. J. Med. Genet. 2017, 54, 404–412. [Google Scholar] [CrossRef]
- Cideciyan, A.V.; Aleman, T.S.; Swider, M.; Schwartz, S.B.; Steinberg, J.D.; Brucker, A.J.; Maguire, A.M.; Bennett, J.; Stone, E.M.; Jacobson, S. Mutations in ABCA4 result in accumulation of lipofuscin before slowing of the retinoid cycle: A reappraisal of the human disease sequence. Hum. Mol. Genet. 2004, 13, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Cideciyan, A.V.; Swider, M.; Aleman, T.S.; Sumaroka, A.; Schwartz, S.B.; Roman, M.I.; Milam, A.H.; Bennett, J.; Stone, E.M.; Jacobson, S. ABCA4-Associated Retinal Degenerations Spare Structure and Function of the Human Parapapillary Retina. Investig. Opthalmol. Vis. Sci. 2005, 46, 4739–4746. [Google Scholar] [CrossRef] [Green Version]
- Boon, C.J.F. Retinal Dystrophies Associated with the PRPH2 Gene. In Inherited Chorioretinal Dystrophies; Puech, B., De Laey, J.-J., Holder, G.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; Volume 2014, pp. 213–233. [Google Scholar]
- Holz, F.; Spaide, R.; Bird, A.C.; Schmitz-Valckenberg, S. (Eds.) Atlas of Fundus Autofluorscence Imaging; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Pichi, F.; Abboud, E.B.; Ghazi, N.G.; Khan, A.O. Fundus autofluorescence imaging in hereditary retinal diseases. Acta Ophthalmol. 2017, 96, e549–e561. [Google Scholar] [CrossRef]
- Delori, F.C.; Dorey, C.K.; Staurenghi, G.; Arend, O.; Goger, D.G.; Weiter, J.J. In vivo fluorescence of the ocular fundus exhibits retinal pigment epithelium lipofuscin characteristics. Investig. Ophthalmol. Vis. Sci. 1995, 36, 718–729. [Google Scholar]
- Birnbach, C.D.; Järveläínen, M.; Possin, D.E.; Milam, A.H. Histopathology and Immunocytochemistry of the Neurosensory Retina in Fundus Flavimaculatus. Ophthalmology 1994, 101, 1211–1219. [Google Scholar] [CrossRef]
- Burke, T.R.; Duncker, T.; Woods, R.L.; Greenberg, J.P.; Zernant, J.; Tsang, S.H.; Smith, R.T.; Allikmets, R.; Sparrow, J.R.; Delori, F.C. Quantitative Fundus Autofluorescence in Recessive Stargardt Disease. Investig. Opthalmol. Vis. Sci. 2014, 55, 2841–2852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncker, T.; Tsang, S.H.; Woods, R.; Lee, W.; Zernant, J.; Allikmets, R.; Delori, F.C.; Sparrow, J.R. Quantitative Fundus Autofluorescence and Optical Coherence Tomography inPRPH2/RDS- andABCA4-Associated Disease Exhibiting Phenotypic Overlap. Investig. Opthalmol. Vis. Sci. 2015, 56, 3159–3170. [Google Scholar] [CrossRef] [Green Version]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Sundararajan, M.; Taly, A.; Yan, Q. Axiomatic Attribution for Deep Networks. International Conference on Machine Learing. March 2017. Available online: http://arxiv.org/abs/1703.01365 (accessed on 4 September 2020).
- Schmitz-Valckenberg, S.; Pfau, M.; Fleckenstein, M.; Staurenghi, G.; Sparrow, J.R.; Bindewald-Wittich, A.; Spaide, R.F.; Wolf, S.; Sadda, S.R.; Holz, F.G. Fundus autofluorescence imaging. Prog. Retin. Eye Res. 2021, 81, 100893. [Google Scholar] [CrossRef] [PubMed]
- Le, D.; Alam, M.; Yao, C.K.; Lim, J.I.; Hsieh, Y.-T.; Chan, R.V.P.; Toslak, D.; Yao, X. Transfer Learning for Automated OCTA Detection of Diabetic Retinopathy. Transl. Vis. Sci. Technol. 2020, 9, 35. [Google Scholar] [CrossRef]
- Miere, A.; Le Meur, T.; Bitton, K.; Pallone, C.; Semoun, O.; Capuano, V.; Colantuono, D.; Taibouni, K.; Chenoune, Y.; Astroz, P.; et al. Deep Learning-Based Classification of Inherited Retinal Diseases Using Fundus Autofluorescence. J. Clin. Med. 2020, 9, 3303. [Google Scholar] [CrossRef]
- Miere, A.; Capuano, V.; Kessler, A.; Zambrowski, O.; Jung, C.; Colantuono, D.; Pallone, C.; Semoun, O.; Petit, E.; Souied, E. Deep learning-based classification of retinal atrophy using fundus autofluorescence imaging. Comput. Biol. Med. 2021, 130, 104198. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Ledo, A.R.; Rittscher, J. Automated classification of normal and Stargardt disease optical coherence tomography images using deep learning. Acta Ophthalmol. 2020, 98, e715–e721. [Google Scholar] [CrossRef] [PubMed]
- Fujinami-Yokokawa, Y.; Ninomiya, H.; Liu, X.; Yang, L.; Pontikos, N.; Yoshitake, K.; Iwata, T.; Sato, Y.; Hashimoto, T.; Tsunoda, K.; et al. Prediction of causative genes in inherited retinal disorder from fundus photography and autofluorescence imaging using deep learning techniques. Br. J. Ophthalmol. 2021, 105, 1272–1279. [Google Scholar] [CrossRef]
- Fujinami-Yokokawa, Y.; Pontikos, N.; Yang, L.; Tsunoda, K.; Yoshitake, K.; Iwata, T.; Miyata, H.; Fujinami, K.; Japan Eye Genetics Consortium. Prediction of Causative Genes in Inherited Retinal Disorders from Spec-tral-Domain Optical Coherence Tomography Utilizing Deep Learning Techniques. J. Ophthalmol. 2019, 2019, 1691064. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Training Set | Validation Set | Test Set | Total | |
|---|---|---|---|---|
| Stargardt disease (n) | 183 | 30 | 91 | 304 |
| Pseudo-Stargardt Pattern Dystrophy (n) | 40 | 6 | 20 | 66 |
| Total (n) | 223 | 36 | 111 | 370 |
| Patient | Age | Sex | Mutation | |
|---|---|---|---|---|
| RDS/PRPH2 mutation | #1 | 49 | M | c.639c > G (p.Cys213Trp) RHO: c.185C > A (Thr62Asn) |
| #2 | 50 | F | c.639c > G (p.Cys213Trp) | |
| #3 | 51 | F | c623G > A (p.Gly208Asp) | |
| #4 | 83 | M | c.461del (p.Lys154Argfs*102) | |
| #5 | 54 | M | c.461del (p.Lys154Argfs*102) | |
| #6 | 49 | M | c.628C > G (p.Pro210Ala) | |
| #7 | 43 | M | NA | |
| #8 | 39 | F | NA | |
| #9 | 43 | F | NA | |
| ABCA4 mutation | #1 | 50 | M | c.3259G > A (p.Glu1087Lys) c.5882G > A (p.Gly1961Glu) |
| #2 | 36 | M | c.1749G > C (p.Lys583Asn) c.3916delinsGT (p.Pro1306Valfs*116) | |
| #3 | 36 | F | c.1222C > T (p.Arg408*) c.6320G > A(p.Arg2107His) | |
| #4 | 30 | M | c.2966T > C (p.Val989Ala) c.5318C > T (p.Ala1773Val) | |
| #5 | 71 | M | c.1648G > A (p.Gly550Arg) c.5603A > T (p.Asn1868Ile) | |
| #6 | 14 | M | c.4918C > T (p.Arg1640Trp) c.5087G > A (p.Ser1696Asn) | |
| #7 | 39 | F | c.2123T > C (p.Met708Thr) c.3058dup (p.Val1020Glyfs*3) | |
| #8 | 41 | F | c.3322C > T (p.Arg1108Cys) c.5885G > A (p.Gly1961Glu) | |
| #9 | 68 | F | c.1015T > G (p.Trp339Gly) c.5603A > T (p.Asn1868Ile) | |
| #10 | 56 | M | c.2966T > C (p.Val989Ala) c.3289A > G (p.Arg1097Gly) | |
| #11 | 25 | F | c.1018T > C (p.Tyr340His) c.5315G > A (p.Trp1772*) ‡ | |
| #12 | 25 | F | c.5018 + 2T > C(IVS35 + 2T > C) c.5196 + 1137G > A ‡ | |
| #13 | 66 | F | c.4685T > C (p.Ile1562Thr) c.5113C > T (p.Arg1705Trp) | |
| #14 | 44 | M | c.452T > C(p.Ile151Thr) ‡ c.3352C > T(p.His1118Tyr) ‡ | |
| #15 | 71 | M | c.1671T > A (p.Tyr557*) c.4139C > T (p.Pro1380Leu) | |
| #16 | 17 | M | c.3813G > C (p.Glu1271Asp) ‡ c.455G > A (p.Arg152Gln) ‡ c.3322C > T (p.Arg1108Cys) ‡ c.6320G > A (p.Arg2107His) ‡ | |
| #17 | 37 | M | c.5363C > T (p.Pro1788Leu) c.1054G > A (p.Asp352asn) ‡, c.5882G > A (p.Gly1961Glu) ‡ | |
| #18 | 45 | F | c.5885G > A (p.Gly1961Glu) c.1648G > A (p.Gly550Arg) ‡, c.5603A > T (p.Asn1868Ile) ‡ | |
| #19 | 17 | M | c.1015T > G (p.Trp339Gly) c.2588G > C (p.Gly863Ala) c.1715G > A (p.Arg572Gln) ‡ | |
| #20 | 63 | F | c.5603A > T (p.Asn1868Ile) c.614G > A (p.Cys205Tyr) ‡ | |
| #21 | 50 | M | c.3113C > T (p.Ala1038Val) c.455G > A (p.Arg152Gln) ‡, c.3322C > T (p.Arg1108Cys) ‡, c.6320G > A (p.Arg2107His) ‡ | |
| #22 | 75 | F | c.455G > A (p.Arg152Gln) ‡, c.3322C > T (p.Arg1108Cys) ‡, c.6320G > A (p.Arg2107His) ‡ | |
| #23 | 43 | M | c.514G > A (p.Gly172Ser) ‡, c.4875T > A (p.His1625Gln) ‡, c.6094C > T (p.His2032Tyr) ‡ | |
| #24 | 64 | F | c.1749G > (p.Lys583Asn) | |
| #25 | 73 | M | c.3916delinsGT (p.Pro1306Valfs*116) | |
| #26 | 25 | M | c.1749G > C (p.Lys583Asn) | |
| #27 | 43 | M | c.1749G > C (p.Lys583Asn) | |
| #28 | 87 | F | c.735T > G (p.Tyr245*) | |
| #29 | 38 | F | c.3813G > C (p.Glu1271Asp) | |
| #30 | 70 | F | c.5363C > T (p.Pro1788Leu) | |
| #31 | 37 | M | c.1749G > C (p.Lys583Asn) | |
| #32 | 67 | M | c.5885G > A (p.Gly1961Glu) | |
| #33 | 68 | F | c.769–784C > T (p.Leu257Aspfs*3) ‡ | |
| #34 | 43 | M | c.4070C > T (p.Ala1357Val) | |
| #35 | 51 | F | c.1804C > T (p.Arg602Trp) | |
| #36 | 49 | F | c.1804C > T (p.Arg602Trp) | |
| #37 | 25 | F | c.634C > T (p.Arg212Cys) | |
| #38 | 55 | M | c.5315G > A (p.Trp1772*) | |
| #39 | 20 | F | c.1018T > C (p.Tyr340His) | |
| #40 | 54 | M | c.1018T > C (p.Tyr340His) |
| Loss | Accuracy | AUROC | ||
|---|---|---|---|---|
| ResNet50V2 | Training set | 0.342 | 0.869 | 0.925 |
| Validation set | 0.6383 | 0.769 | 0.837 | |
| Test set | 0.413 | 0.882 | 0.892 | |
| Accuracy | Sensitivity (Recall) | Specificity | |
|---|---|---|---|
| Retina expert | 0.816 | 0.790 | 0.801 |
| Retina fellow | 0.724 | 0.595 | 0.590 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miere, A.; Zambrowski, O.; Kessler, A.; Mehanna, C.-J.; Pallone, C.; Seknazi, D.; Denys, P.; Amoroso, F.; Petit, E.; Souied, E.H. Deep Learning to Distinguish ABCA4-Related Stargardt Disease from PRPH2-Related Pseudo-Stargardt Pattern Dystrophy. J. Clin. Med. 2021, 10, 5742. https://doi.org/10.3390/jcm10245742
Miere A, Zambrowski O, Kessler A, Mehanna C-J, Pallone C, Seknazi D, Denys P, Amoroso F, Petit E, Souied EH. Deep Learning to Distinguish ABCA4-Related Stargardt Disease from PRPH2-Related Pseudo-Stargardt Pattern Dystrophy. Journal of Clinical Medicine. 2021; 10(24):5742. https://doi.org/10.3390/jcm10245742
Chicago/Turabian StyleMiere, Alexandra, Olivia Zambrowski, Arthur Kessler, Carl-Joe Mehanna, Carlotta Pallone, Daniel Seknazi, Paul Denys, Francesca Amoroso, Eric Petit, and Eric H. Souied. 2021. "Deep Learning to Distinguish ABCA4-Related Stargardt Disease from PRPH2-Related Pseudo-Stargardt Pattern Dystrophy" Journal of Clinical Medicine 10, no. 24: 5742. https://doi.org/10.3390/jcm10245742