
Does Humeral Component Version Affect Range of Motion and Clinical Outcomes in Reverse Total Shoulder Arthroplasty? A Systematic Review


Abstract
:1. Introduction
- Which humeral stem version gives the best functional outcomes and ROM in RTSA?
- Which type of humeral design (onlay vs. inlay) within this setting gives the best functional outcomes and ROM?
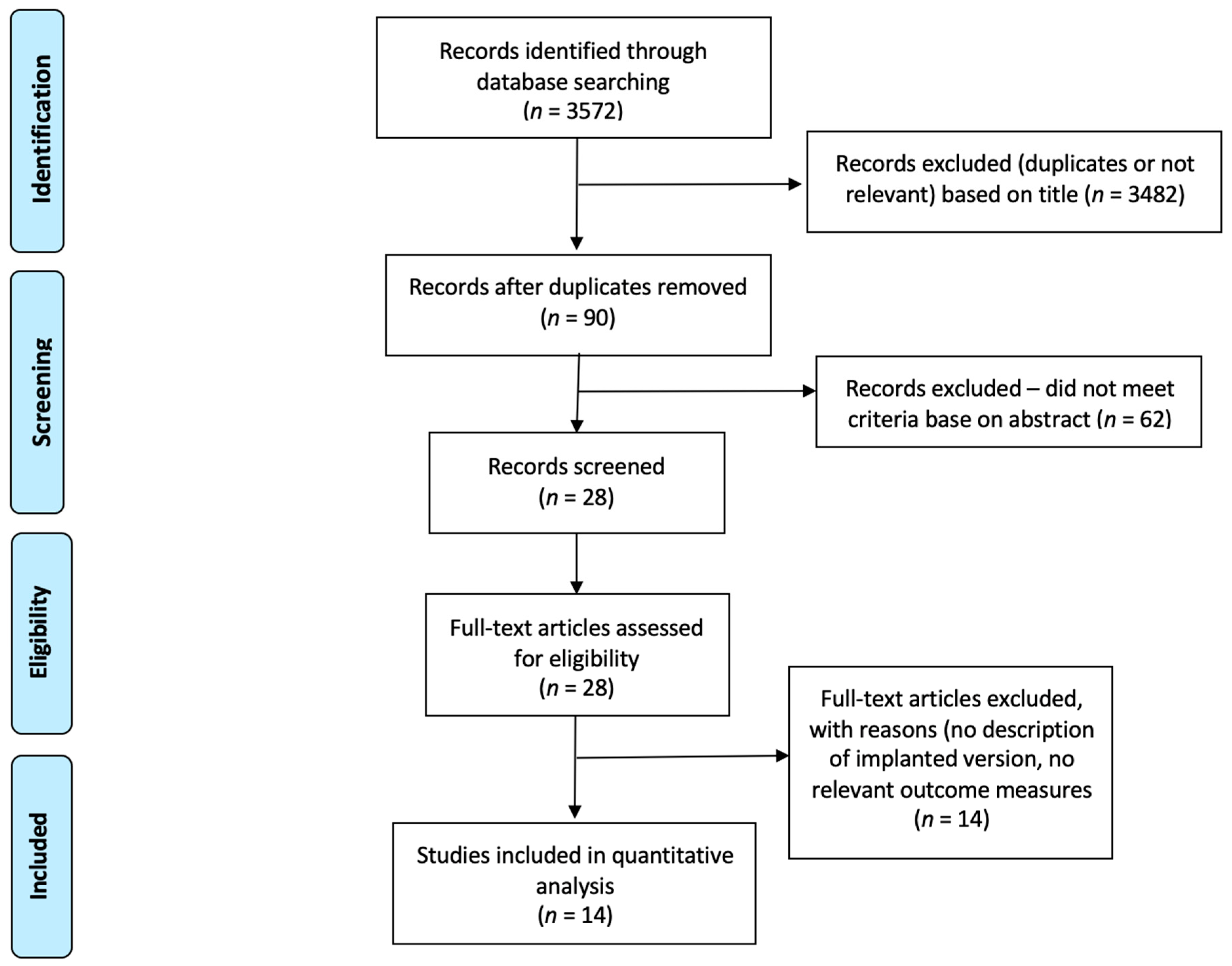
2. Methods
2.1. Search Strategy and Criteria
2.2. Data Collection
- Group 1: RTSA with the humeral stem implanted in less than 20° of retroversion;
- Group 2: RTSA with the humeral stem implanted in 20° retroversion;
- Group 3: RTSA with the humeral stem implanted in greater than 20° retroversion.
2.3. Statistical Analysis
3. Results
3.1. Study Characteristics
3.1.1. Group 1: Humeral Version at Less than 20° Retroversion
3.1.2. Group 2: Humeral Version at 20° Retroversion
3.1.3. Group 3: Humeral Version at Greater than 20° Retroversion
3.2. Comparison between Groups—Humeral Retroversion
3.3. Comparison between Groups—Humeral Stem Designs (Onlay vs. Inlay)
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Australian Orthopaedic Association National Joint Replacment Registry. 2019. Available online: https://aoanjrr.sahmri.com/ (accessed on 26 October 2021).
- Ek, E.T.H.; Neukom, L.; Catanzaro, S.; Gerber, C. Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old: Results after five to fifteen years. J. Shoulder Elb. Surg. 2013, 22, 1199–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerber, C.; Canonica, S.; Catanzaro, S.; Ernstbrunner, L. Longitudinal observational study of reverse total shoulder arthroplasty for irreparable rotator cuff dysfunction: Results after 15 years. J. Shoulder Elb. Surg. 2018, 27, 831–838. [Google Scholar] [CrossRef]
- Werner, C.M.L.; Steinmann, P.A.; Gilbart, M.; Gerber, C. Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J. Bone Jt. Surg. Am. 2005, 87, 1476–1486. [Google Scholar] [CrossRef]
- Ernstbrunner, L.; Rahm, S.; Suter, A.; Imam, M.A.; Catanzaro, S.; Grubhofer, F.; Gerber, C. Salvage reverse total shoulder arthroplasty for failed operative treatment of proximal humeral fractures in patients younger than 60 years: Long-term results. J. Shoulder Elb. Surg. 2020, 29, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Ernstbrunner, L.; Andronic, O.; Grubhofer, F.; Camenzind, R.S.; Wieser, K.; Gerber, C. Long-term results of reverse total shoulder arthroplasty for rotator cuff dysfunction: A systematic review of longitudinal outcomes. J. Shoulder Elb. Surg. 2019, 28, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Ernstbrunner, L.; Suter, A.; Catanzaro, S.; Rahm, S.; Gerber, C. Reverse Total Shoulder Arthroplasty for Massive, Irreparable Rotator Cuff Tears Before the Age of 60 Years: Long-Term Results. J. Bone Jt. Surg. Am. 2017, 99, 1721–1729. [Google Scholar] [CrossRef] [Green Version]
- Ernstbrunner, L.; Werthel, J.-D.; Wagner, E.; Hatta, T.; Sperling, J.W.; Cofield, R.H. Glenoid bone grafting in primary reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2017, 26, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Baulot, E.; Sirveaux, F.; Boileau, P. Grammont’s idea: The story of Paul Grammont’s functional surgery concept and the development of the reverse principle. Clin. Orthop. Relat. Res. 2011, 469, 2425–2431. [Google Scholar] [CrossRef] [Green Version]
- Sheth, U.; Saltzman, M. Reverse Total Shoulder Arthroplasty: Implant Design Considerations. Curr. Rev. Musculoskelet. Med. 2019, 12, 554–561. [Google Scholar] [CrossRef]
- Merolla, G.; Walch, G.; Ascione, F.; Paladini, P.; Fabbri, E.; Padolino, A.; Porcellini, G. Grammont humeral design versus onlay curved-stem reverse shoulder arthroplasty: Comparison of clinical and radiographic outcomes with minimum 2-year follow-up. J. Shoulder Elb. Surg. 2018, 27, 701–710. [Google Scholar] [CrossRef]
- Kontaxis, A.; Chen, X.; Berhouet, J.; Choi, D.; Wright, T.; Dines, D.M.; Warren, R.F.; Gulotta, L.V. Humeral version in reverse shoulder arthroplasty affects impingement in activities of daily living. J. Shoulder Elb. Surg. 2017, 26, 1073–1082. [Google Scholar] [CrossRef]
- Nalbone, L.; Adelfio, R.; D’Arienzo, M.; Ingrassia, T.; Nigrelli, V.; Zabbara, F.; Paladini, P.; Campi, F.; Pellegrini, A.; Porcellini, G. Optimal positioning of the humeral component in the reverse shoulder prosthesis. Musculoskelet. Surg. 2014, 98, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Aleem, A.W.; Feeley, B.T.; Austin, L.S.; Ma, C.B.; Krupp, R.J.; Ramsey, M.L.; Getz, C.L. Effect of Humeral Component Version on Outcomes in Reverse Shoulder Arthroplasty. Orthopedics 2017, 40, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.H.; Sharma, N.; Rhee, S.M.; Park, J.H. Do individualized humeral retroversion and subscapularis repair affect the clinical outcomes of reverse total shoulder arthroplasty? J. Shoulder Elb. Surg. 2019, 29, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Rhee, Y.G.; Cho, N.S.; Moon, S.C. Effects of humeral component retroversion on functional outcomes in reverse total shoulder arthroplasty for cuff tear arthropathy. J. Shoulder Elb. Surg. 2015, 24, 1574–1581. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Richards, R.R.; An, K.N.; Bigliani, L.U.; Friedman, R.J.; Gartsman, G.M.; Gristina, A.G.; Iannotti, J.P.; Mow, V.C.; Sidles, J.A.; Zuckerman, J.D. A standardized method for the assessment of shoulder function. J. Shoulder Elb. Surg. 1994, 3, 347–352. [Google Scholar] [CrossRef]
- Boileau, P.; Alta, T.D.; Decroocq, L.; Sirveaux, F.; Clavert, P.; Favard, L.; Chelli, M. Reverse shoulder arthroplasty for acute fractures in the elderly: Is it worth reattaching the tuberosities? J. Shoulder Elb. Surg. 2019, 28, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Frankle, M.; Siegal, S.; Pupello, D.; Saleem, A.; Mighell, M.; Vasey, M. The Reverse Shoulder Prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency. A minimum two-year follow-up study of sixty patients. J. Bone Jt. Surg. Am. 2005, 87, 1697–1705. [Google Scholar] [CrossRef]
- Harmsen, S.M.; Norris, T.R. Radiographic changes and clinical outcomes associated with an adjustable diaphyseal press-fit humeral stem in primary reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2017, 26, 1589–1597. [Google Scholar] [CrossRef]
- Kim, M.S.; Jeong, H.Y.; Kim, J.D.; Ro, K.H.; Rhee, S.-M.; Rhee, Y.G. Difficulty in performing activities of daily living associated with internal rotation after reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2020, 29, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Leathers, M.P.; Ialenti, M.N.; Feeley, B.T.; Zhang, A.L.; Ma, C.B. Do younger patients have better results after reverse total shoulder arthroplasty? J. Shoulder Elb. Surg. 2018, 27, S24–S28. [Google Scholar] [CrossRef]
- Samuelsen, B.T.; Wagner, E.R.; Houdek, M.T.; Elhassan, B.T.; Sanchez-Sotelo, J.; Cofield, R.; Sperling, J.W. Primary reverse shoulder arthroplasty in patients aged 65 years or younger. J. Shoulder Elb. Surg. 2017, 26, e13–e17. [Google Scholar] [CrossRef] [PubMed]
- Statz, J.M.; Wagner, E.R.; Houdek, M.T.; Cofield, R.H.; Sanchez-Sotelo, J.; Elhassan, B.T.; Sperling, J.W. Outcomes of primary reverse shoulder arthroplasty in patients with morbid obesity. J. Shoulder Elb. Surg. 2016, 25, e191–e198. [Google Scholar] [CrossRef]
- Theivendran, K.; Varghese, M.; Large, R.; Bateman, M.; Morgan, M.; Tambe, A.; Espag, M.; Cresswell, T.; Clark, D.I. Reverse total shoulder arthroplasty using a trabecular metal glenoid base plate: Functional and radiological outcomes at two to five years. Bone Jt. J. 2016, 98-B, 969–975. [Google Scholar] [CrossRef]
- Valenti, P.; Sauzieres, P.; Katz, D.; Kalouche, I.; Kilinc, A.S. Do less medialized reverse shoulder prostheses increase motion and reduce notching? Clin. Orthop. Relat. Res. 2011, 469, 2550–2557. [Google Scholar] [CrossRef] [Green Version]
- Vourazeris, J.D.; Wright, T.W.; Struk, A.M.; King, J.J.; Farmer, K.W. Primary reverse total shoulder arthroplasty outcomes in patients with subscapularis repair versus tenotomy. J. Shoulder Elb. Surg. 2017, 26, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Young, A.A.; Smith, M.M.; Bacle, G.; Moraga, C.; Walch, G. Early results of reverse shoulder arthroplasty in patients with rheumatoid arthritis. J. Bone Jt. Surg. Am. 2011, 93, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Gerber, C.; Pennington, S.D.; Nyffeler, R.W. Reverse total shoulder arthroplasty. J. Am. Acad. Orthop. Surg. 2009, 17, 284–295. [Google Scholar] [CrossRef]
- Gulotta, L.V.; Choi, D.; Marinello, P.; Knutson, Z.; Lipman, J.; Wright, T.; Cordasco, F.A.; Craig, E.V.; Warren, R.F. Humeral component retroversion in reverse total shoulder arthroplasty: A biomechanical study. J. Shoulder Elb. Surg. 2012, 21, 1121–1127. [Google Scholar] [CrossRef]
- Stephenson, D.R.; Oh, J.H.; McGarry, M.H.; Rick Hatch, G.F., 3rd; Lee, T.Q. Effect of humeral component version on impingement in reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2011, 20, 652–658. [Google Scholar] [CrossRef]
- Favre, P.; Sussmann, P.S.; Gerber, C. The effect of component positioning on intrinsic stability of the reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2010, 19, 550–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lädermann, A.; Denard, P.J.; Boileau, P.; Farron, A.; Deransart, P.; Terrier, A.; Ston, J.; Walch, G. Effect of humeral stem design on humeral position and range of motion in reverse shoulder arthroplasty. Int. Orthop. 2015, 39, 2205–2213. [Google Scholar] [CrossRef] [Green Version]
- Caceres, A.P.; Permeswaran, V.N.; Goetz, J.E.; Hettrich, C.M.; Anderson, D.D. The Influence of Different Rotator Cuff Deficiencies on Shoulder Stability Following Reverse Shoulder Arthroplasty. Iowa Orthop. J. 2019, 39, 63–68. [Google Scholar]
- Boileau, P.; Watkinson, D.; Hatzidakis, A.M.; Hovorka, I. Neer Award 2005: The Grammont reverse shoulder prosthesis: Results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J. Shoulder Elb. Surg. 2006, 15, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Werner, B.S.; Chaoui, J.; Walch, G. The influence of humeral neck shaft angle and glenoid lateralization on range of motion in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2017, 26, 1726–1731. [Google Scholar] [CrossRef]
- Nabergoj, M.; Onishi, S.; Lädermann, A.; Kalache, H.; Trebše, R.; Bothorel, H.; Collin, P. Can Lateralization of Reverse Shoulder Arthroplasty Improve Active External Rotation in Patients with Preoperative Fatty Infiltration of the Infraspinatus and Teres Minor? J. Clin. Med. 2021, 10, 4130. [Google Scholar] [CrossRef] [PubMed]
- Virani, N.A.; Cabezas, A.; Gutiérrez, S.; Santoni, B.G.; Otto, R.; Frankle, M. Reverse shoulder arthroplasty components and surgical techniques that restore glenohumeral motion. J. Shoulder Elb. Surg. 2013, 22, 179–187. [Google Scholar] [CrossRef]
- Goetti, P.; Denard, P.J.; Collin, P.; Ibrahim, M.; Mazzolari, A.; Lädermann, A. Biomechanics of anatomic and reverse shoulder arthroplasty. EFORT Open Rev. 2021, 6, 918–931. [Google Scholar] [CrossRef] [PubMed]
- Giles, J.W.; Langohr, G.D.G.; Johnson, J.A.; Athwal, G.S. The rotator cuff muscles are antagonists after reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2016, 25, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, S.; Comiskey, C.A., 4th; Luo, Z.-P.; Pupello, D.R.; Frankle, M.A. Range of impingement-free abduction and adduction deficit after reverse shoulder arthroplasty. Hierarchy of surgical and implant-design-related factors. J. Bone Jt. Surg. Am. 2008, 90, 2606–2615. [Google Scholar] [CrossRef] [PubMed]
- Wall, B.; Nove-Josserand, L.; O’Connor, D.P.; Edwards, T.B.; Walch, G. Reverse total shoulder arthroplasty: A review of results according to etiology. J. Bone Jt. Surg. Am. 2007, 89, 1476–1485. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Patients | Mean Follow-Up (Months) | Type of Implant | Implanted Stem Version (° Retroversion) | Outcome Measures | Study Details |
|---|---|---|---|---|---|---|---|
| Aleem et al. [14] | 2017 | 64 | 24 | Inlay | <10°R/>20°R | ASES, ROM | Retrospective study comparing outcomes in two groups of primary RTSR patients based on having their humeral stem implanted in either <10° or >20° of retroversion. |
| Boileau et al. [20] | 2018 | 38 | 36 | Inlay | 20°R | Constant, SSV, ROM | Retrospective study assessing outcomes of patients undergoing primary RTSR for proximal humerus fracture with reattachment of the tuberosities. |
| Frankle et al. [21] | 2005 | 60 | 33 | Inlay | 30°R | ASES, ROM | Retrospective study assessing outcomes of patients undergoing primary RTSR for glenohumeral arthritis associated with severe rotator cuff deficiencies. |
| Harmsen et al. [22] | 2017 | 232 | 26.4 | Inlay | 30°R | ASES, SANE, ROM | Retrospective study assessing outcomes of patients undergoing primary RTSR with a diaphyseal press-fit humeral stem. |
| Kim et al. [23] | 2019 | 77 | 70.6 | Inlay | 20°R | Constant, UCLA, ROM | Retrospective study assessing outcomes of patients undergoing primary RTSR for cuff tear arthropathy and/or a massive irreparable cuff tear. |
| Leathers et al. [24] | 2018 | 82 | 40.8/37.2 | Inlay | 10°R | ASES, ROM | Retrospective study comparing outcomes in two groups of primary RTSR patients, either aged 70 years and older or 65 years and younger. |
| Oh et al. [15] | 2019 | 80 | 31.4 | Onlay | <20°R/20°R/>20°R | ASES, SST, ROM | Retrospective study comparing outcomes in two groups of primary RTSR patients based on having their humeral stem implanted in either 20° of retroversion or with an individualised native version. Secondary outcomes assessed the effect of subscapularis tendon repair. |
| Rhee et al. [16] | 2015 | 62 | 43.3/38.4 | Inlay | 0°/20°R | Constant, UCLA, ROM, VAS | Retrospective study comparing outcomes in two groups of primary RTSR patients based on having their humeral stem implanted in either 0° or 20° of retroversion. |
| Samuelsen et al. [25] | 2016 | 67 | 36 | Mixed | 27°R | ASES, SST, ROM | Retrospective study assessing outcomes of patients aged 65 years and under, undergoing primary RTSR. |
| Statz et al. [26] | 2016 | 41 | 38.4 | Mixed | >20°R | ASES, ROM | Retrospective study assessing outcomes of morbidly obese patients undergoing primary RTSR. |
| Theivendran et al. [27] | 2016 | 124 | 32 | Inlay | <20°R | Constant, OSS, ROM | Retrospective study assessing outcomes of patients undergoing primary RTSR with a trabecular metal glenoid base plate. |
| Valenti et al. [28] | 2011 | 76 | 44 | Onlay | <20°R | Constant, ROM | Retrospective study assessing outcomes of patients undergoing primary RTSR with a lateralised glenosphere. |
| Vourazeris et al. [29] | 2017 | 202 | 39.6/37.2 | Onlay | 20°R | ASES, Constant, UCLA, SST, ROM | Retrospective study comparing outcomes in two groups of primary RTSR patients based on having either a subscapularis repair or tenotomy. |
| Young et al. [30] | 2011 | 16 | 45.6 | Inlay | <10°R | Constant, ROM | Retrospective study assessing outcomes of patients with rheumatoid arthritis undergoing primary RTSR. |
| Group 1 (<20°R) | Group 2 (20°R) | Group 3 (>20°R) | |
|---|---|---|---|
| Number of studies | 7 | 5 | 6 |
| Number of patients | 380 | 375 | 466 |
| Mean follow-up (months) | 35.9 | 44.8 | 31.5 |
| <20°R | 20°R | p Value | |
|---|---|---|---|
| Number of patients | 380 | 375 | |
| ASES (Mean (Standard Deviation)) | 76.0 (3.47) | 75.8 (3.96) | 0.956 |
| Constant Score (Mean (Standard Deviation)) | 62.5 (5.71) | 68.1 (3.73) | 0.153 |
| Dislocations (n) | 5 | 3 | 0.725 |
| Forward elevation (°) (Mean (Standard Deviation)) | 127.9 (12.66) | 129.7 (6.10) | 0.777 |
| External Rotation (ER1) (°) (Mean (Standard Deviation)) | 33.6 (10.34) | 36.4 (11.41) | 0.659 |
| External Rotation (ER2) (°) (Mean (Standard Deviation)) | 59.3 (13.15) | 73.4 (1.27) | 0.228 |
| Internal Rotation (0° shoulder abduction) (Points) (Mean (Standard Deviation)) | 7.99 (1.41) | 7.78 (3.14) | 0.893 |
| <20°R | >20°R | p Value | |
|---|---|---|---|
| Number of patients | 380 | 466 | |
| ASES (Mean (Standard Deviation)) | 76.0 (3.47) | 73.3 (7.55) | 0.586 |
| Constant Score (Mean (Standard Deviation)) | 62.5 (5.71) | N/A | - |
| Dislocations (n) | 5 | 6 | 0.601 |
| Forward elevation (°) (Mean (Standard Deviation)) | 127.9 (12.66) | 129.1 (15.81) | 0.881 |
| External Rotation (ER1) (°) (Mean (Standard Deviation)) | 33.6 (10.34) | 41.3 (9.46) | 0.192 |
| External Rotation (ER2) (°) (Mean (Standard Deviation)) | 59.3 (13.15) | 61.0 (4.24) | 0.877 |
| Internal Rotation (0° shoulder abduction) (Points) (Mean (Standard Deviation)) | 7.99 (1.41) | 7.68 (4.27) | 0.877 |
| 20°R | >20°R | p Value | |
|---|---|---|---|
| Number of patients | 375 | 466 | |
| ASES (Mean (Standard Deviation)) | 75.8 (3.96) | 73.3 (7.55) | 0.682 |
| Constant Score (Mean (Standard Deviation)) | 68.1 (3.73) | N/A | - |
| Dislocations (n) | 3 | 6 | 0.738 |
| Forward elevation (°) (Mean (Standard Deviation)) | 129.7 (6.10) | 129.1 (15.81) | 0.945 |
| External Rotation (ER1) (°) (Mean (Standard Deviation)) | 36.4 (11.41) | 41.3 (9.46) | 0.462 |
| External Rotation (ER2) (°) (Mean (Standard Deviation)) | 73.4 (1.27) | 61.0 (4.24) | 0.058 |
| Internal Rotation (0° shoulder abduction) (Points) (Mean (Standard Deviation)) | 7.78 (3.14) | 7.68 (4.27) | 0.976 |
| Inlay Design | Onlay Design | p Value | |
|---|---|---|---|
| Number of patients | 755 | 358 | |
| ASES (Mean (Standard Deviation)) | 74.9 (4.66) | 77.9 (3.68) | 0.332 |
| Constant Score (Mean (Standard Deviation)) | 65.0 (4.53) | 66.0 (9.90) | 0.842 |
| Forward elevation (°) (Mean (Standard Deviation)) | 127.0 (12.88) | 132.0 (9.58) | 0.459 |
| External Rotation (ER1) (°) (Mean (Standard Deviation)) | 34.4 (9.54) | 39.5 (12.41) | 0.382 |
| External Rotation (ER2) (°) (Mean (Standard Deviation)) | 65.2 (10.11) | 50 (8.24) | 0.210 |
| Internal Rotation (0° shoulder abduction) (Points) (Mean (Standard Deviation)) | 7.1 (1.44) | 9.8 (2.33) | 0.048 |
| Inlay Design | Onlay Design | |||||
|---|---|---|---|---|---|---|
| <20°R | 20°R | >20°R | <20°R | 20°R | >20°R | |
| Number of patients (studies) | 283 (5) | 145 (3) | 327 (3) | 97 (2) | 230 (2) | 31 (1) |
| ASES (Mean (Standard Deviation)) | 73.5 (2.56) | N/A | 76 (3.73) | 78.2 (17.7) | 77.9 (1.83) | 81.9 (4) |
| Constant Score (Mean (Standard Deviation)) | 59.8 (5.13) | 66.5 (1.54) | N/A | 59 (1.58) | 73 (N/A) | N/A |
| Forward elevation (°) (Mean (Standard Deviation)) | 118 (11.42) | 134 (3.35) | 122 (10.26) | 129.6 (6.79) | 122 (2.59) | 141.6 (3.86) |
| External Rotation (ER1) (°) (Mean (Standard Deviation)) | 29.7 (6.82) | 41.1 (10.21) | 33.6 (3.59) | 31.9 (3.68) | 26.7 (4.55) | 54.5 (3.87) |
| External Rotation (ER2) (°) (Mean (Standard Deviation)) | 65.3 (10.02) | 73 (0.81) | 58.8 (2.03) | 50 (2.24) | N/A | N/A |
| Internal Rotation (0° shoulder abduction) (Points) (Mean (Standard Deviation)) | 8.86 (2) | 6.8 (2.60) | N/A | 7.31 (1.32) | 12.1 (2.7) | 10.7 (2.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jassim, S.S.; Ernstbrunner, L.; Ek, E.T. Does Humeral Component Version Affect Range of Motion and Clinical Outcomes in Reverse Total Shoulder Arthroplasty? A Systematic Review. J. Clin. Med. 2021, 10, 5745. https://doi.org/10.3390/jcm10245745
Jassim SS, Ernstbrunner L, Ek ET. Does Humeral Component Version Affect Range of Motion and Clinical Outcomes in Reverse Total Shoulder Arthroplasty? A Systematic Review. Journal of Clinical Medicine. 2021; 10(24):5745. https://doi.org/10.3390/jcm10245745
Chicago/Turabian StyleJassim, Shivan S., Lukas Ernstbrunner, and Eugene T. Ek. 2021. "Does Humeral Component Version Affect Range of Motion and Clinical Outcomes in Reverse Total Shoulder Arthroplasty? A Systematic Review" Journal of Clinical Medicine 10, no. 24: 5745. https://doi.org/10.3390/jcm10245745