
The Relationship between Alcohol Hangover Severity, Sleep and Cognitive Performance; a Naturalistic Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Breath Alcohol Content (BrAC)
2.3.2. Alcohol Consumption
2.3.3. Alcohol Hangover Severity Scale (AHSS)
2.3.4. Core Consensus Sleep Diary (CSD)
2.3.5. Online Trail-Making Task (TMT-B)
2.4. Procedure
2.5. Analysis
3. Results
3.1. Participant Characteristics
3.2. Sleep Quality
3.3. Correlations
3.3.1. Drinking Characteristics
3.3.2. AH Severity and Sleep Characteristics
3.3.3. AH Severity, Sleep and TMT-B Performance
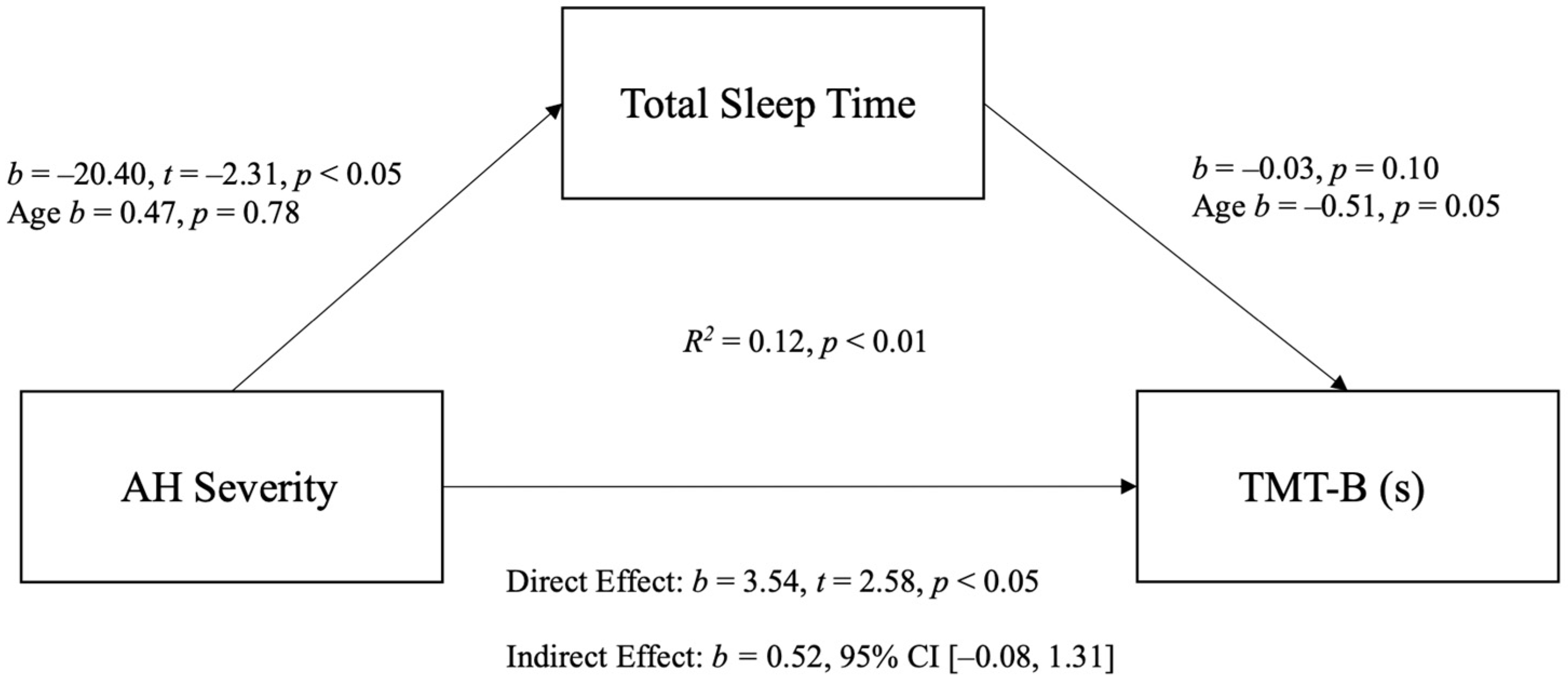
3.4. Mediation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Verster, J.C.; Scholey, A.; van de Loo, A.J.A.E.; Benson, S.; Stock, A.-K. Updating the Definition of the Alcohol Hangover. J. Clin. Med. 2020, 9, 823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schrojenstein Lantman, M.; van de Loo, A.J.A.E.; Mackus, M.; Verster, J.C. Development of a Definition for the Alcohol Hangover: Consumer Descriptions and Expert Consensus. Curr. Drug Abus. Rev. 2017, 9, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Kruisselbrink, L.D.; Slot, K.A.; Anogeianaki, A.; Adams, S.; Alford, C.; Arnoldy, L.; Ayre, E.; Balikji, S.; Benson, S.; et al. Sensitivity to Experiencing Alcohol Hangovers: Reconsideration of the 0.11% Blood Alcohol Concentration (BAC) Threshold for Having a Hangover. J. Clin. Med. 2020, 9, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, S.; Ayre, E.; Garrisson, H.; Wetherell, M.A.; Verster, J.C.; Scholey, A. Alcohol Hangover and Multitasking: Effects on Mood, Cognitive Performance, Stress Reactivity, and Perceived Effort. J. Clin. Med. 2020, 9, 1154. [Google Scholar] [CrossRef] [PubMed]
- Penning, R.; McKinney, A.; Verster, J.C. Alcohol Hangover Symptoms and Their Contribution to the Overall Hangover Severity. Alcohol Alcohol. 2012, 47, 248–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slutske, W.S.; Piasecki, T.M.; Hunt-Carter, E.E. Development and Initial Validation of the Hangover Symptoms Scale: Prevalence and Correlates of Hangover Symptoms in College Students. Alcohol. Clin. Exp. Res. 2003, 27, 1442–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verster, J.C.; Bervoets, A.C.; De Klerk, S.; Vreman, R.A.; Olivier, B.; Roth, T.; Brookhuis, K.A. Effects of alcohol hangover on simulated highway driving performance. Psychopharmacology 2014, 231, 2999–3008. [Google Scholar] [CrossRef] [PubMed]
- Gunn, C.; Mackus, M.; Griffin, C.; Munafò, M.R.; Adams, S. A systematic review of the next-day effects of heavy alcohol consumption on cognitive performance. Addiction 2018, 113, 2182–2193. [Google Scholar] [CrossRef] [PubMed]
- Gunn, C.; Fairchild, G.; Verster, J.C.; Adams, S. The Effects of Alcohol Hangover on Executive Functions. J. Clin. Med. 2020, 9, 1148. [Google Scholar] [CrossRef] [Green Version]
- Rohsenow, D.J.; Howland, J.; Arnedt, J.T.; Almeida, A.B.; Greece, J.; Minsky, S.; Kempler, C.S.; Sales, S. Intoxication with bourbon versus vodka: Effects on hangover, sleep, and next-day neurocognitive performance in young adults. Alcohol. Clin. Exp. Res. 2010, 34, 509–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grange, J.A.; Stephens, R.; Jones, K.; Owen, L. The effect of alcohol hangover on choice response time. J. Psychopharmacol. 2016, 30, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Van Duin, D.; Volkerts, E.R.; Schreuder, A.H.C.M.L.; Verbaten, M.N. Alcohol Hangover Effects on Memory Functioning and Vigilance Performance after an Evening of Binge Drinking. Neuropsychopharmacology 2002, 28, 740–746. [Google Scholar] [CrossRef]
- McKinney, A.; Coyle, K.; Penning, R.; Verster, J.C. Next day effects of naturalistic alcohol consumption on tasks of attention. Hum. Psychopharmacol. Clin. Exp. 2012, 27, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, A. Financial Headache: The Cost of Workplace Hangover and Intoxication to the UK Economy; Institute for Alcohol Studies: London, UK, 2019. [Google Scholar]
- Sacks, J.J.; Gonzales, K.R.; Bouchery, E.E.; Tomedi, L.E.; Brewer, R.D. 2010 National and State Costs of Excessive Alcohol Consumption. Am. J. Prev. Med. 2015, 49, e73–e79. [Google Scholar] [CrossRef] [PubMed]
- Penning, R.; Van Nuland, M.; Fliervoet, L.A.; Olivier, B.; Verster, J.C. The Pathology of Alcohol Hangover. Curr. Drug Abus. Rev. 2010, 3, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Tipple, C.T.; Benson, S.; Scholey, A. A Review of the Physiological Factors Associated with Alcohol Hangover. Curr. Drug Abus. Rev. 2017, 9, 93–98. [Google Scholar] [CrossRef]
- Van de Loo, A.J.A.E.; Mackus, M.; Kwon, O.; Krishnakumar, I.M.; Garssen, J.; Kraneveld, A.D.; Scholey, A.; Verster, J.C. The Inflammatory Response to Alcohol Consumption and Its Role in the Pathology of Alcohol Hangover. J. Clin. Med. 2020, 9, 2081. [Google Scholar] [CrossRef] [PubMed]
- Rohsenow, D.J.; Howland, J. The role of beverage congeners in hangover and other residual effects of alcohol in-toxication: A review. Curr. Drug Abus. Rev. 2010, 3, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Tolstrup, J.S.; Stephens, R.; Grønbaek, M. Does the Severity of Hangovers Decline with Age? Survey of the Incidence of Hangover in Different Age Groups. Alcohol. Clin. Exp. Res. 2013, 38, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Roehrs, T.; Roth, T. Sleep, sleepiness, and alcohol use. Alcohol Res. Health J. Natl. Inst. Alcohol Abuse Alcohol. 2001, 25, 101–109. [Google Scholar]
- Roehrs, T.; Roth, T. Sleep, sleepiness, sleep disorders and alcohol use and abuse. Sleep Med. Rev. 2001, 5, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Roehrs, T.; Yoon, J.; Roth, T. Nocturnal and next-day effects of ethanol and basal level of sleepiness. Hum. Psychopharmacol. Clin. Exp. 1991, 6, 307–311. [Google Scholar] [CrossRef]
- Verster, J.C.; van de Loo, A.J.A.E.; Adams, S.; Stock, A.-K.; Benson, S.; Scholey, A.; Alford, C.; Bruce, G. Advantages and Limitations of Naturalistic Study Designs and Their Implementation in Alcohol Hangover Research. J. Clin. Med. 2019, 8, 2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohsenow, D.J.; Howland, J.; Minsky, S.J.; Arnedt, J.T. Effects of Heavy Drinking by Maritime Academy Cadets on Hangover, Perceived Sleep, and Next-Day Ship Power Plant Operation. J. Stud. Alcohol 2006, 67, 406–415. [Google Scholar] [CrossRef]
- Hogewoning, A.; van de Loo, A.; Mackus, M.; Raasveld, S.J.; De Zeeuw, R.; Bosma, E.R.; Bouwmeester, N.; Brookhuis, K.; Garssen, J.; Verster, J.C. Characteristics of social drinkers with and without a hangover after heavy alcohol consumption. Subst. Abus. Rehabil. 2016, 7, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, R.; Grange, J.A.; Jones, K.; Owen, L. A critical analysis of alcohol hangover research methodology for surveys or studies of effects on cognition. Psychopharmacology 2014, 231, 2223–2236. [Google Scholar] [CrossRef] [PubMed]
- Devenney, L.E.; Coyle, K.B.; Roth, T.; Verster, J.C. Sleep after Heavy Alcohol Consumption and Physical Activity Levels during Alcohol Hangover. J. Clin. Med. 2019, 8, 752. [Google Scholar] [CrossRef] [Green Version]
- McKinney, A.; Coyle, K. Alcohol hangover effects on measures of affect the morning after a normal night’s drinking. Alcohol Alcohol. 2006, 41, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnigan, F.; Hammersley, R.; Cooper, T. An examination of next-day hangover effects after a 100 mg/100 mL dose of alcohol in heavy social drinkers. Addiction 1998, 93, 1829–1838. [Google Scholar] [CrossRef]
- Stephens, R.; Ling, J.; Heffernan, T.M.; Heather, N.; Jones, K. A review of the literature on the cognitive effects of alcohol hangover. Alcohol Alcohol. 2008, 43, 163–170. [Google Scholar] [CrossRef]
- Scholey, A.; Benson, S.; Kaufman, J.; Terpstra, C.; Ayre, E.; Verster, J.C.; Allen, C.; Devilly, G.J. Effects of Alcohol Hangover on Cognitive Performance: Findings from a Field/Internet Mixed Methodology Study. J. Clin. Med. 2019, 8, 440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schrojenstein Lantman, M.; Mackus, M.; Roth, T.; Verster, J.C. Total sleep time, alcohol consumption, and the duration and severity of alcohol hangover. Nat. Sci. Sleep 2017, 9, 181–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schrojenstein Lantman, M.; Roth, T.; Roehrs, T.; Verster, J.C. Alcohol hangover, sleep quality, and daytime sleepiness. Sleep Vigil. 2017, 1, 37–41. [Google Scholar] [CrossRef]
- Alford, C.; Martinkova, Z.; Tiplady, B.; Reece, R.; Verster, J.C. The effects of alcohol hangover on mood and performance assessed at home. J. Clin. Med. 2020, 9, 1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKinney, A.; Coyle, K. Next day effects of a normal night’s drinking on memory and psychomotor performance. Alcohol Alcohol. 2004, 39, 509–513. [Google Scholar] [CrossRef] [PubMed]
- McKinney, A.; Coyle, K. Next-day effects of alcohol and an additional stressor on memory and psychomotor performance. J. Stud. Alcohol Drugs 2007, 68, 446–454. [Google Scholar] [CrossRef]
- Devenney, L.E.; Coyle, K.B.; Verster, J.C. Memory and attention during an alcohol hangover. Human Psychopharmacol. Clin. Exp. 2019, 34, e2701. [Google Scholar] [CrossRef] [Green Version]
- Devenney, L.E.; Coyle, K.B.; Verster, J.C. Cognitive performance and mood after a normal night of drinking: A naturalistic alcohol hangover study in a non-student sample. Addict. Behav. Rep. 2019, 10, 100197. [Google Scholar] [CrossRef]
- Lim, J.; Dinges, D.F. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol. Bull. 2010, 136, 375–389. [Google Scholar] [CrossRef]
- Pilcher, J.J.; Huffcutt, A.I. Effects of Sleep Deprivation on Performance: A Meta-Analysis. Sleep 1996, 19, 318–326. [Google Scholar] [CrossRef]
- Arbuthnott, K.; Frank, J. Trail Making Test, Part B as a Measure of Executive Control: Validation Using a Set-Switching Paradigm. J. Clin. Exp. Neuropsychol. 2000, 22, 518–528. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Administration and interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef]
- Titova, O.E.; Lindberg, E.; Elmståhl, S.; Lind, L.; Schiöth, H.B.; Benedict, C. Association between shift work history and performance on the trail making test in middle-aged and elderly humans: The EpiHealth study. Neurobiol. Aging 2016, 45, 23–29. [Google Scholar] [CrossRef]
- Saint Martin, M.; Sforza, E.; Barthélémy, J.C.; Thomas-Anterion, C.; Roche, F. Does subjective sleep affect cognitive function in healthy elderly subjects? The Proof cohort. Sleep Med. 2012, 13, 1146–1152. [Google Scholar] [CrossRef]
- Wimmer, F.; Hoffmann, R.F.; Bonato, R.A.; Moffitt, A.R. The effects of sleep deprivation on divergent thinking and attention processes. J. Sleep Res. 1992, 1, 223–230. [Google Scholar] [CrossRef]
- Dry, M.J.; Burns, N.R.; Nettelbeck, T.; Farquharson, A.L.; White, J.M. Dose-Related Effects of Alcohol on Cognitive Functioning. PLoS ONE 2012, 7, e50977. [Google Scholar] [CrossRef] [Green Version]
- Guillot, C.R.; Fanning, J.R.; Bullock, J.S.; McCloskey, M.S.; Berman, M.E. Effects of alcohol on tests of executive functioning in men and women: A dose response examination. Exp. Clin. Psychopharmacol. 2010, 18, 409–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbertson, R.; Prather, R.; Nixon, S. Acute alcohol administration and placebo effectiveness in older moderate drinkers: Influences on cognitive performance. J. Stud. Alcohol Drugs 2010, 71, 345–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howse, A.D.; Hassall, C.D.; Williams, C.C.; Hajcak, G.; Krigolson, O.E. Alcohol hangover impacts learning and reward processing within the medial-frontal cortex. Psychophysiology 2018, 55, e13081. [Google Scholar] [CrossRef]
- Murgia, M.; Mingolo, S.; Prpic, V.; Sors, F.; Santoro, I.; Bilotta, E.; Agostini, T. University Students’ Hangover May Affect Cognitive Research. Front. Psychol. 2020, 11, 573291. [Google Scholar] [CrossRef] [PubMed]
- Devilly, G.J.; Allen, C.; Brown, K. SmartStart: Results of a large point of entry study into preloading alcohol and associated behaviours. Int. J. Drug Policy 2017, 43, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Devilly, G.J.; Greber, M.; Brown, K.; Allen, C. Drinking to go out or going out to drink? A longitudinal study of alcohol in night-time entertainment districts. Drug Alcohol Depend. 2019, 205, 107603. [Google Scholar] [CrossRef]
- Devilly, G.J.; Hides, L.; Kavanagh, D.J. A big night out getting bigger: Alcohol consumption, arrests and crowd numbers, before and after legislative change. PLoS ONE 2019, 14, e0218161. [Google Scholar] [CrossRef] [Green Version]
- Sorbello, J.G.; Devilly, G.J.; Allen, C.; Hughes, L.R.; Brown, K. Fuel-cell breathalyser use for field research on alcohol intoxication: An independent psychometric evaluation. PeerJ 2018, 6, e4418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Government Department of Health. Standard Drinks Guide; Australian Government Department of Health: Canberra, Australia, 2020.
- Penning, R.; McKinney, A.; Bus, L.D.; Olivier, B.; Slot, K.; Verster, J.C. Measurement of alcohol hangover severity: Development of the Alcohol Hangover Severity Scale (AHSS). Psychopharmacology 2012, 225, 803–810. [Google Scholar] [CrossRef]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The consensus sleep diary: Standardizing prospective sleep self-monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [Green Version]
- Devenney, L.E.C.; Coyle, K.B.; Verster, J.C. The impact of expectancy on cognitive performance during alcohol hangover. BMC Res. Notes 2018, 11, 730. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007; Volume 5. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, E.; Tyacke, R.; Sastre, M.; Lingford-Hughes, A.; Nutt, D.; Ward, R.J. Alcohol hangover: Underlying biochemical, inflammatory and neurochemical mechanisms. Alcohol Alcohol. 2019, 54, 196–203. [Google Scholar] [CrossRef]
- Kim, D.-J.; Kim, W.; Yoon, S.-J.; Choi, B.-M.; Kim, J.-S.; Go, H.J.; Kim, Y.-K.; Jeong, J. Effects of alcohol hangover on cytokine production in healthy subjects. Alcohol 2003, 31, 167–170. [Google Scholar] [CrossRef]
- Verster, J.C.; Arnoldy, L.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. The Impact of Mood and Subjective Intoxication on Hangover Severity. J. Clin. Med. 2020, 9, 2462. [Google Scholar] [CrossRef]
- Scholey, A.B.; Benson, S.; Neale, C.; Owen, L.; Tiplady, B. Neurocognitive and mood effects of alcohol in a naturalistic setting. Hum. Psychopharmacol. 2012, 27, 514–516. [Google Scholar] [CrossRef]
- Tiplady, B.; Franklin, N.; Scholey, A. Effect of ethanol on judgements of performance. Br. J. Psychol. 2004, 95, 105–118. [Google Scholar] [CrossRef]
- Benson, S.; Tiplady, B.; Scholey, A. Attentional and working memory performance following alcohol and energy drink: A randomised, double-blind, placebo-controlled, factorial design laboratory study. PLoS ONE 2019, 14, e0209239. [Google Scholar] [CrossRef] [Green Version]
- Scholey, A.; Ayre, E.; Stock, A.-K.; Verster, J.C.; Benson, S. Effects of rapid recovery on alcohol hangover severity: A double-blind, placebo-controlled, factorial design laboratory study. J. Clin. Med. 2020, 9, 2175. [Google Scholar] [CrossRef]
- Prat, G.; Adan, A.; Pérez-Pàmies, M.; Sànchez-Turet, M. Neurocognitive effects of alcohol hangover. Addict. Behav. 2008, 33, 15–23. [Google Scholar] [CrossRef]
- Verster, J.C.; van de Loo, A.J.; Benson, S.; Scholey, A.; Stock, A.-K. The Assessment of Overall Hangover Severity. J. Clin. Med. 2020, 9, 786. [Google Scholar] [CrossRef] [Green Version]
- Arnedt, J.T.; Rohsenow, D.J.; Almeida, A.B.; Hunt, S.K.; Gokhale, M.; Gottlieb, D.J.; Howland, J. Sleep Following Alcohol Intoxication in Healthy, Young Adults: Effects of Sex and Family History of Alcoholism. Alcohol. Clin. Exp. Res. 2011, 35, 870–878. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Mean | SD |
|---|---|---|
| Sleep Characteristics | ||
| Time to bed (h:m) | 3:41 | 1:07 |
| Sleep onset latency (h:m) | 0:32 | 0:47 |
| No. nightly awakenings | 1.32 | 1.84 |
| Duration of nightly awakenings (min) | 0:07 | 0:16 |
| Time of final wake up (h:m) | 9:29 | 1:48 |
| Total sleep time (h:m) | 4:58 | 2:06 |
| Total time in bed (h:m) | 6:32 | 1:50 |
| Sleep quality | 3.31 | 1.15 |
| Normal sleep quality | 3.73 | 0.9 |
| AH Symptoms | ||
| Total AH severity | 3.85 | 1.42 |
| Fatigue | 7.55 | 2.49 |
| Apathy | 4.57 | 2.88 |
| Clumsiness | 3.86 | 2.51 |
| Confusion | 2.76 | 2.19 |
| Thirst | 7.15 | 2.47 |
| Sweating | 3.08 | 2.53 |
| Shivering | 1.25 | 1.05 |
| Stomach pain | 2.72 | 2.56 |
| Nausea | 3.87 | 2.78 |
| Dizziness | 3 | 2.27 |
| Heart pounding | 2.55 | 2.36 |
| Cognitive Performance—TMT-B | ||
| Completion time (s) | 55.29 | 20.12 |
| Number of errors | 2.57 | 7.19 |
| Variables | Sleep Characteristics | Cognitive Performance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Time to Bed | Sleep Onset Latency | N°. Nightly Awakenings | Duration of Nightly Awakenings | Time of Final Wake Up | Total Sleep Time | Total Time in Bed | Sleep Quality | TMT-B (s) | TMT-B (Err) | |
| Drinking Characteristics | ||||||||||
| BrAC | 0.160 | −0.169 | −0.010 | −0.035 | 0.096 | 0.041 | −0.152 | 0.040 | 0.186 | −0.028 |
| Hours drinking | 0.341 ** | −0.039 | 0.197 | 0.182 | −0.033 | −0.238 * | −0.258 ** | −0.164 | 0.294 ** | 0.108 |
| Total drinks | 0.235 * | 0.037 | −0.018 | −0.033 | 0.073 | −0.076 | −0.165 | 0.025 | 0.212 * | 0.102 |
| AH Symptoms | ||||||||||
| Total AH severity | 0.174 | 0.024 | 0.252 * | 0.302 * | 0.032 | −0.229 a | −0.112 | −0.236 * | 0.286 b | 0.114 |
| Fatigue | 0.180 | 0.085 | 0.153 | 0.188 | −0.164 | −0.320 ** | −0.241 * | −0.309 ** | 0.289 ** | 0.219 * |
| Apathy | 0.090 | 0.001 | 0.033 | 0.117 | 0.222 a | 0.028 | 0.093 | −0.100 | 0.131 | −0.067 |
| Clumsiness | 0.066 | 0.099 | 0.162 | 0.216 * | 0.058 | −0.193 | −0.028 | −0.153 | 0.199 * | −0.003 |
| Confusion | 0.178 | 0.028 | 0.117 | 0.162 | 0.027 | −0.126 | −0.167 | −0.203 * | 0.253 * | 0.101 |
| Thirst | −0.011 | 0.055 | 0.132 | 0.204 * | −0.171 | −0.243 * | −0.165 | −0.169 | 0.253 * | 0.052 |
| Sweating | 0.119 | 0.030 | 0.251 * | 0.218 * | −0.044 | −0.116 | −0.133 | −0.182 | 0.161 | 0.102 |
| Shivering | 0.053 | −0.075 | 0.341 * | 0.280 ** | 0.014 | −0.158 | −0.021 | −0.193 | 0.087 | 0.010 |
| Stomach pain | 0.196 | 0.059 | 0.163 | 0.138 | −0.018 | −0.263 * | −0.177 | −0.184 | 0.203 * | 0.138 |
| Nausea | 0.090 | −0.028 | 0.145 | 0.202 * | 0.024 | −0.048 | −0.037 | −0.060 | 0.234 * | 0.052 |
| Dizziness | −0.053 | −0.031 | 0.140 | 0.141 | 0.003 | −0.080 | 0.099 | −0.039 | 0.125 | −0.019 |
| Heart pounding | 0.163 | −0.018 | 0.308 ** | 0.276 ** | 0.041 | −0.101 | −0.031 | −0.241 * | 0.292 ** | 0.137 |
| Cognitive Performance | ||||||||||
| TMT-B (s) | 0.214 * | −0.013 | 0.118 | 0.191 | −0.188 | −0.235 a | −0.207 * | −0.130 | - | - |
| TMT-B (Err) | 0.148 | −0.032 | −0.080 | −0.041 | −0.201 * | −0.145 | −0.210 * | −0.005 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayre, E.; Scholey, A.; White, D.; Devilly, G.J.; Kaufman, J.; Verster, J.C.; Allen, C.; Benson, S. The Relationship between Alcohol Hangover Severity, Sleep and Cognitive Performance; a Naturalistic Study. J. Clin. Med. 2021, 10, 5691. https://doi.org/10.3390/jcm10235691
Ayre E, Scholey A, White D, Devilly GJ, Kaufman J, Verster JC, Allen C, Benson S. The Relationship between Alcohol Hangover Severity, Sleep and Cognitive Performance; a Naturalistic Study. Journal of Clinical Medicine. 2021; 10(23):5691. https://doi.org/10.3390/jcm10235691
Chicago/Turabian StyleAyre, Elizabeth, Andrew Scholey, David White, Grant J. Devilly, Jordy Kaufman, Joris C. Verster, Corey Allen, and Sarah Benson. 2021. "The Relationship between Alcohol Hangover Severity, Sleep and Cognitive Performance; a Naturalistic Study" Journal of Clinical Medicine 10, no. 23: 5691. https://doi.org/10.3390/jcm10235691