
Oral Antibiotic Prophylaxis Lowers Surgical Site Infection in Elective Colorectal Surgery: Results of a Pragmatic Cohort Study in Catalonia

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Outcomes Comparison BP–IP Groups
3.2. Overall SSI
3.3. Organ-Space SSI
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Members of the VINCat Colorectal Surveillance Team
References
- European Centre for Disease Prevention and Control. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals 2011. 2012; ECDC: Stockholm, Sweden, 2013. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-surgical-site-infections-europe-2010-2011 (accessed on 13 August 2021).
- Study of Prevalence of Nosocomial Infections in Spain. EPINE Website. 2016. Available online: https://epine.es/api/documento-publico/2019%20EPINE%20Informe%20Espa%C3%B1a%2027112019.pdf/reports-esp (accessed on 23 August 2021).
- Smith, R.L.; Bohl, J.K.; McElearney, S.T.; Friel, C.M.; Barclay, M.M.; Sawyer, R.G.; Foley, E.F. Wound infection after elective colorectal resection. Ann. Surg. 2004, 239, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.A.; Altom, L.K.; Deierhoi, R.J.; Morris, M.; Richman, J.S.; Vick, C.C.; Itani, K.M.; Hawn, M.T. Preoperative oral antibiotics reduce surgical site infection following elective colorectal resections. Dis. Colon Rectum 2012, 55, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Pujol, M.; Limón, E.; López-Contreras, J.; Sallés, M.; Bella, F.; Gudiol, F. Surveillance of surgical site infections in elective colorectal surgery. Results of the VINCat Program (2007–2010). Enferm. Infecc. Microbiol. Clin. 2012, 30, 20–25. [Google Scholar] [CrossRef]
- Paulson, E.C.; Thompson, E.; Mahmoud, N. Surgical Site Infection and Colorectal Surgical Procedures: A Prospective Analysis of Risk Factors. Surg. Infect. 2017, 18, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Badia, J.M.; Casey, A.L.; Petrosillo, N.; Hudson, P.; Mitchell, S.; Crosby, C. Impact of surgical site infection on healthcare costs and patient outcomes: A systematic review in six European countries. J. Hosp. Infect. 2017, 96, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Shaw, E.; Badia, J.M.; Piriz, M.; Escofet, R.; Limon, E.; Gudiol, F. O053: What surgical site infection rates in colorectal surgery should be considered for benchmarking standards? Antimicrob. Resist. Infect. Control. 2013, 2, O53. [Google Scholar] [CrossRef] [Green Version]
- Harbarth, S.; Sax, H.; Gastmeier, P. The preventable proportion of nosocomial infections: An overview of published reports. J. Hosp. Infect. 2003, 54, 258–266. [Google Scholar] [CrossRef]
- Keighley, M.R.; Arabi, Y.; Alexander-Williams, J.; Youngs, D.; Burdon, D.W. Comparison between systemic and oral antimicrobial prophylaxis in colorectal surgery. Lancet 1979, 1, 894–897. [Google Scholar] [CrossRef]
- Bucher, P.; Gervaz, P.; Soravia, C.; Mermillod, B.; Erne, M.; Morel, P. Randomized clinical trial of mechanical bowel preparation versus no preparation before elective left-sided colorectal surgery. Br. J. Surg. 2005, 92, 409–414. [Google Scholar] [CrossRef]
- Solla, J.A.; Rothenberger, D.A. Preoperative bowel preparation. A survey of colon and rectal surgeons. Dis. Colon Rectum 1990, 33, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Nichols, R.L.; Smith, J.W.; Garcia, R.Y.; Waterman, R.S.; Holmes, J.W. Current practices of preoperative bowel preparation among North American colorectal surgeons. Clin. Infect. Dis. 1997, 24, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Zmora, O.; Wexner, S.D.; Hajjar, L.; Park, T.; Efron, J.E.; Nogueras, J.J.; Weiss, E.G. Trends in preparation for colorectal surgery: Survey of the members of the American Society of Colon and Rectal Surgeons. Am. Surg. 2003, 69, 150–154. [Google Scholar]
- Markell, K.W.; Hunt, B.M.; Charron, P.D.; Kratz, R.J.; Nelson, J.; Isler, J.T.; Steele, S.R.; Billingham, R.P. Prophylaxis and management of wound infections after elective colorectal surgery: A survey of the American Society of Colon and Rectal Surgeons membership. J. Gastrointest. Surg. 2010, 14, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Badia, J.M.; Casey, A.L.; Rubio-Pérez, I.; Arroyo-García, N.; Espin, E.; Biondo, S.; Balibrea, J.M. Awareness of Practice and Comparison with Best Evidence in Surgical Site Infection Prevention in Colorectal Surgery. Surg Infect. 2020, 21, 218–226. [Google Scholar] [CrossRef]
- Zhu, Q.D.; Zhang, Q.Y.; Zeng, Q.Q.; Yu, Z.P.; Tao, C.L.; Yang, W.J. Efficacy of mechanical bowel preparation with polyethylene glycol in prevention of postoperative complications in elective colorectal surgery: A meta-analysis. Int. J. Colorectal Dis. 2010, 25, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Güenaga, K.F.; Matos, D.; Wille-Jørgensen, P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst. Rev. 2011, 2011, CD001544. [Google Scholar] [CrossRef]
- Cao, F.; Li, J.; Li, F. Mechanical bowel preparation for elective colorectal surgery: Updated systematic review and meta-analysis. Int. J. Colorectal Dis. 2012, 27, 803–810. [Google Scholar] [CrossRef]
- Courtney, D.E.; Kelly, M.E.; Burke, J.P.; Winter, D.C. Postoperative outcomes following mechanical bowel preparation before proctectomy: A meta-analysis. Colorectal Dis. 2015, 17, 862–869. [Google Scholar] [CrossRef]
- Dahabreh, I.J.; Steele, D.W.; Shah, N.; Trikalinos, T.A. Oral Mechanical Bowel Preparation for Colorectal Surgery: Systematic Review and Meta-Analysis. Dis. Colon Rectum 2015, 58, 698–707. [Google Scholar] [CrossRef]
- Rollins, K.E.; Javanmard-Emamghissi, H.; Lobo, D.N. Impact of mechanical bowel preparation in elective colorectal surgery: A meta-analysis. World J. Gastroenterol. 2018, 24, 519–536. [Google Scholar] [CrossRef]
- Lewis, R.T. Oral versus systemic antibiotic prophylaxis in elective colon surgery: A randomized study and meta-analysis send a message from the 1990s. Can. J. Surg. 2002, 45, 173–180. [Google Scholar]
- Oshima, T.; Takesue, Y.; Ikeuchi, H.; Matsuoka, H.; Nakajima, K.; Uchino, M.; Tomita, N.; Sasako, M. Preoperative oral antibiotics and intravenous antimicrobial prophylaxis reduce the incidence of surgical site infections in patients with ulcerative colitis undergoing IPAA. Dis. Colon Rectum 2013, 56, 1149–1155. [Google Scholar] [CrossRef]
- Sadahiro, S.; Suzuki, T.; Tanaka, A.; Okada, K.; Kamata, H.; Ozaki, T.; Koga, Y. Comparison between oral antibiotics and probiotics as bowel preparation for elective colon cancer surgery to prevent infection: Prospective randomized trial. Surgery 2014, 155, 493–503. [Google Scholar] [CrossRef]
- Anthony, T.; Murray, B.W.; Sum-Ping, J.T.; Lenkovsky, F.; Vornik, V.D.; Parker, B.J.; McFarlin, J.E.; Hartless, K.; Huerta, S. Evaluating an evidence-based bundle for preventing surgical site infection: A randomized trial. Arch. Surg. 2011, 146, 263–269. [Google Scholar] [CrossRef]
- Allegranzi, B.; Bischoff, P.; de Jonge, S.; Kubilay, N.Z.; Zayed, B.; Gomes, S.M.; Abbas, M.; Atema, J.J.; Gans, S.; van Rijen, M.; et al. New WHO recommendations on preoperative measures for surgical site infection prevention: An evidence-based global perspective. Lancet Infect. Dis. 2016, 16, e276–e287. [Google Scholar] [CrossRef]
- Nelson, R.L.; Glenny, A.M.; Song, F. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst. Rev. 2014, 2014, CD001181. [Google Scholar] [CrossRef]
- Fry, D.E. Colon preparation and surgical site infection. Am. J. Surg. 2011, 202, 225–232. [Google Scholar] [CrossRef]
- Bellows, C.F.; Mills, K.T.; Kelly, T.N.; Gagliardi, G. Combination of oral non-absorbable and intravenous antibiotics versus intravenous antibiotics alone in the prevention of surgical site infections after colorectal surgery: A meta-analysis of randomized controlled trials. Tech. Coloproctol. 2011, 15, 385–395. [Google Scholar] [CrossRef]
- Nelson, R.L.; Gladman, E.; Barbateskovic, M. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst. Rev. 2014, 2014, CD001181. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Song, X.; Chen, L.Z.; Lin, Z.D.; Zhang, X.L. Comparing Mechanical Bowel Preparation with Both Oral and Systemic Antibiotics Versus Mechanical Bowel Preparation and Systemic Antibiotics Alone for the Prevention of Surgical Site Infection After Elective Colorectal Surgery: A Meta-Analysis of Randomized Controlled Clinical Trials. Dis. Colon Rectum 2016, 59, 70–78. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Brooks, L.; Kubus, J.; Luchtefeld, M.; Lynch, J.; Senagore, A.; Eggenberger, J.C.; Velanovich, V.; Campbell, D.A., Jr. A statewide assessment of surgical site infection following colectomy: The role of oral antibiotics. Ann. Surg. 2010, 252, 514–519. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.S.; Graham, L.A.; Chu, D.I.; Cannon, J.A.; Hawn, M.T. Oral Antibiotic Bowel Preparation Significantly Reduces Surgical Site Infection Rates and Readmission Rates in Elective Colorectal Surgery. Ann. Surg. 2015, 261, 1034–1040. [Google Scholar] [CrossRef]
- Badia, J.M.; Arroyo-García, N. Bowel mechanical preparation and oral antibiotic prophylaxis in colorectal surgery. Analysis and narrative review of scientific evidence. Cir. Esp. 2018, 96, 317–325. [Google Scholar] [CrossRef]
- Nichols, R.L.; Choe, E.U.; Weldon, C.B. Mechanical and antibacterial bowel preparation in colon and rectal surgery. Chemotherapy 2005, 51, 115–121. [Google Scholar] [CrossRef]
- Hayashi, M.S.; Wilson, S.E. Is there a current role for preoperative non-absorbable oral antimicrobial agents for prophylaxis of infection after colorectal surgery? Surg. Infect. 2009, 10, 285–288. [Google Scholar] [CrossRef]
- Murray, B.W.; Huerta, S.; Dineen, S.; Anthony, T. Surgical site infection in colorectal surgery: A review of the nonpharmacologic tools of prevention. J. Am. Coll Surg. 2010, 211, 812–822. [Google Scholar] [CrossRef]
- Garner, J.S.; Jarvis, W.R.; Emori, T.G.; Horan, T.C.; Hughes, J.M. CDC definitions for nosocomial infections, 1988. Am. J. Infect. Control. 1988, 16, 128–140. [Google Scholar] [CrossRef]
- Horan, T.C.; Gaynes, R.P.; Martone, W.J.; Jarvis, W.R.; Emori, T.G. CDC definitions of nosocomial surgical site infections, 1992: A modification of CDC definitions of surgical wound infections. Infect. Control. Hosp. Epidemiol. 1992, 13, 606–608. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehlet, H.; Wilmore, D.W. Multimodal strategies to improve surgical outcome. Am. J. Surg. 2002, 183, 630–641. [Google Scholar] [CrossRef]
- Devane, L.A.; Proud, D.; O’Connell, P.R.; Panis, Y. A European survey of bowel preparation in colorectal surgery. Colorectal Dis. 2017, 11, O402–O406. [Google Scholar] [CrossRef]
- Fry, D.E. Infection control in colon surgery. Langenbecks Arch. Surg. 2016, 401, 581–597. [Google Scholar] [CrossRef]
- Alverdy, J.C.; Shogan, B.D. Preparing the bowel for surgery: Rethinking the strategy. Nat. Rev. Gastroenterol Hepatol. 2019, 16, 708709. [Google Scholar] [CrossRef] [PubMed]
- Pellino, G.; Espin-Basany, E. Bowel decontamination before colonic and rectal surgery. Br. J. Surg. 2021. [Google Scholar] [CrossRef]
- Koskenvuo, L.; Lehtonen, T.; Koskensalo, S.; Rasilainen, S.; Klintrup, K.; Ehrlich, A.; Pinta, T.; Scheinin, T.; Sallinen, V. Mechanical and oral antibiotic bowel preparation versus no bowel preparation for elective colectomy (MOBILE): A multicentre, randomised, parallel, single-blinded trial. Lancet 2019, 394, 840848. [Google Scholar] [CrossRef]
- Wexner, S.D.; Yellinek, S. Is preoperative bowel preparation needed before elective colectomy? Lancet 2019, 394, 808810. [Google Scholar] [CrossRef]
- Espin Basany, E.; Solís-Peña, A.; Pellino, G.; Kreisler, E.; Fraccalvieri, D.; Muinelo-Lorenzo, M.; Maseda-Díaz, O.; García-González, J.M.; Santamaría-Olabarrieta, M.; Codina-Cazador, A.; et al. Preoperative oral antibiotics and surgical-site infections in colon surgery (ORALEV): A multicentre, single-blind, pragmatic, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2020, 5, 729738. [Google Scholar] [CrossRef]
- Salkind, N.J. Pragmatic Study. In Encyclopedia of Research Design; Salkind, N.J., Ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010; Volume 5, p. 1073. Available online: https://methods.sagepub.com/Reference//encyc-of-research-design/n326.xml (accessed on 12 August 2021). [CrossRef]
- Papp, G.; Saftics, G.; Szabó, B.E.; Baracs, J.; Vereczkei, A.; Kollár, D.; Oláh, A.; Mészáros, P.; Dubóczki, Z.; Bursics, A. Systemic versus Oral and Systemic Antibiotic Prophylaxis (SOAP) study in colorectal surgery: Prospective randomized multicentre trial. Br. J. Surg. 2021, 108, 271276. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Liu, Z.; Pei, K.Y.; Khan, S.A.; Wang, X.; Yang, M.; Wang, X.; Zhang, Y. The Role of Bowel Preparation in Open, Minimally Invasive, and Converted-to-Open Colectomy. J. Surg. Res. 2019, 242, 183192. [Google Scholar] [CrossRef]
- Hoang, S.C.; Klipfel, A.A.; Roth, L.A.; Vrees, M.; Schechter, S.; Shah, N. Colon and rectal surgery surgical site infection reduction bundle: To improve is to change. Am. J. Surg. 2019, 217, 4045. [Google Scholar] [CrossRef]
- Holubar, S.D.; Hedrick, T.; Gupta, R.; Kellum, J.; Hamilton, M.; Gan, T.J.; Mythen, M.G.; Shaw, A.D.; Miller, T.E.; Perioperative Quality Initiative (POQI) I Workgroup. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on prevention of postoperative infection within an enhanced recovery pathway for elective colorectal surgery. Perioper. Med. 2017, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659695. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| “Adequate” antibiotic prophylaxis | According to hospital protocol Start 30–60 min before incision. Redosification when indicated. Do not prolong > 24 h. |
| Mechanical bowel preparation | Day before of the procedure |
| Oral antibiotic prophylaxis | Day before of the procedure |
| Laparoscopic surgery | |
| Maintenance of normothermia | Goal: >36° at the end of operation |
| Double-ring plastic wound edge retractor | In open or laparoscopic surgery |
| Overall | BP (2011–2015) | IP (2016–2019) | p | |
|---|---|---|---|---|
| Number of procedures | 34,421 | 17,643 | 16,778 | |
| Age, years (SD) | 68.67 (12.40) | 68.86 (12.37) | 68.46 (12.43) | 0.0026 |
| Sex, male (%) | 20,709 (60.16%) | 10,703 (60.66%) | 10,006 (59.64%) | 0.0518 |
| Adequate surgical prophylaxis (%) * | 28,800 (83.79%) | 15,069 (85.51%) | 13,731 (81.98%) | <0.0001 |
| Mean duration of intervention, minutes (SD) | 177.50 (76.12) | 175.35 (76.13) | 179.75 (76.05) | <0.0001 |
| ASA score > 1 (%) | 32,427 (94.62%) | 16,629 (94.39%) | 15,798 (94.86%) | 0.0548 |
| Laparoscopy (%) | 22,415 (65.39%) | 10,180 (57.90%) | 12,235 (73.28%) | <0.0001 |
| NNISS ≥ 1 (%) | 10,532 (30.60%) | 6044 (34.26%) | 4488 (30.60%) | <0.0001 |
| Overall SSI (2011–2019) | BP (2011–2015) | IP (2016–2019) | OR (CI95) | p | |
|---|---|---|---|---|---|
| SSI | 15.05% | 18.81% | 11.10% | 0.539 (0.507–0.573) | <0.0001 |
| Superficial-SSI | 5.3% | 6.3% | 3.6% | 0.549 (0.496–0.608) | <0.0001 |
| Deep-SSI | 2.5% | 3.4% | 1.6% | 0.448 (0.385–0.521) | <0.0001 |
| O/S-SSI | 8.2% | 9.8% | 6.5% | 0.633 (0.584–0.687) | <0.0001 |
| OAP | MBP | |||
|---|---|---|---|---|
| Yes | Not | Yes | Not | |
| SSI | 8.15% | 13.79% | 8.9% | 12.5% |
| Superficial SSI | 2.5% | 4.39% | 2.65% | 4.73% |
| Deep SSI | 1.04% | 1.84% | 1.23% | 1.34% |
| Organ-space SSI | 4.6% | 7.5% | 5.0% | 6.4% |
| Univariate | Multivariate * | |||||
|---|---|---|---|---|---|---|
| OR | CI95 | p | OR | CI95 | p | |
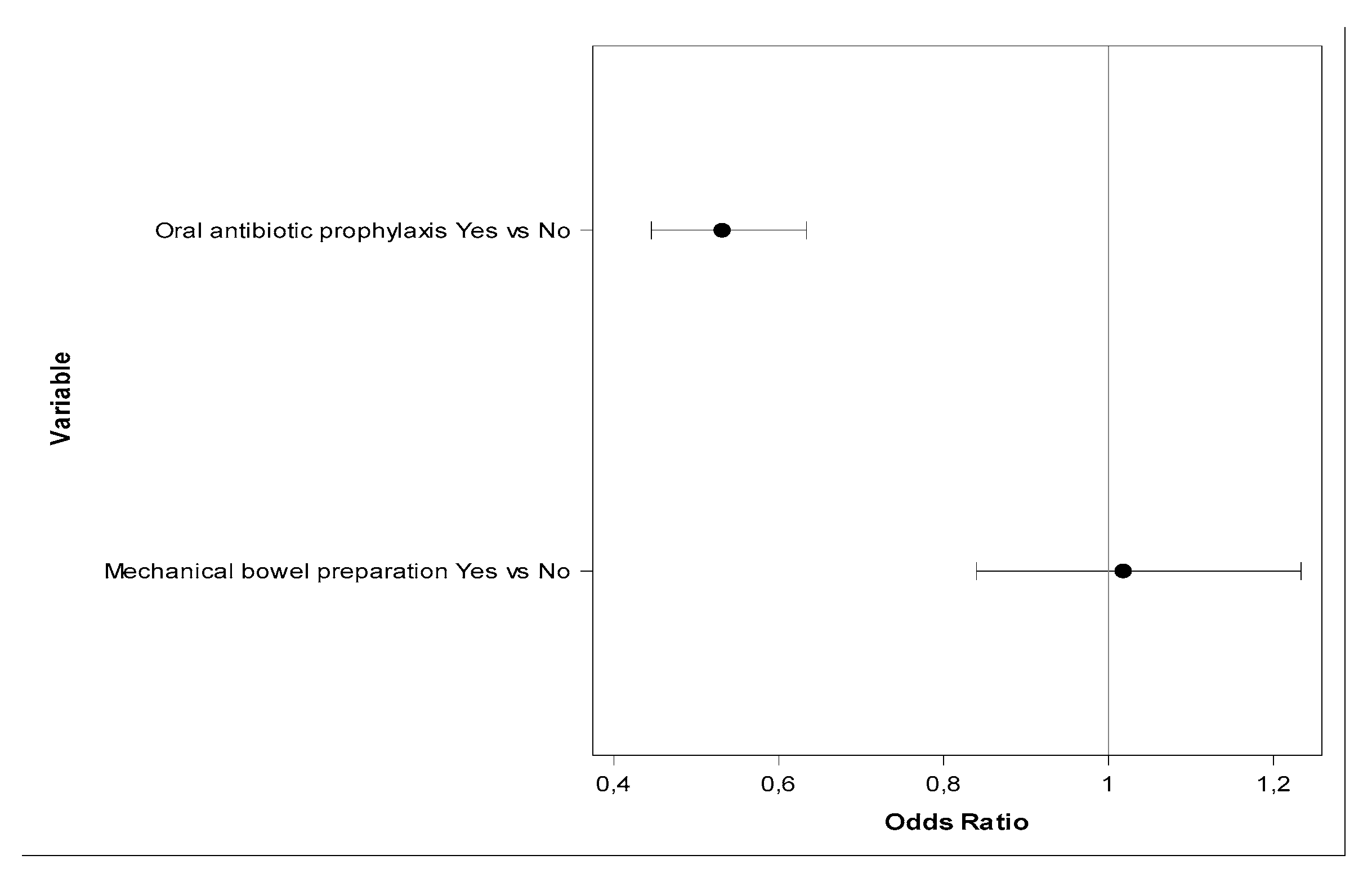
| OAP | 0.555 | 0.483–0.638 | <0.0001 | 0.531 | 0.445–0.634 | <0.0001 |
| MBP | 0.686 | 0.589–0.798 | <0.0001 | 1.017 | 0.839–1.23 | 0.8584 |
| Year of Intervention | ||||
|---|---|---|---|---|
| 2016 | 2017 | 2018 | 2019 | |
| Overall SSI with OAP | 7.2% | 8.7% | 8.9% | 7.3% |
| Overall SSI without OAP | 13.0% | 15.6% | 13.9% | 11.4% |
| Univariate | Multivariate * | |||||
|---|---|---|---|---|---|---|
| OR | CI95 | p | OR | CI95 | p | |
| OAP | 0.592 | 0.494–0.710 | <0.0001 | 0.585 | 0.465–0.735 | <0.0001 |
| MBP | 0.771 | 0.630–0.944 | 0.0117 | 1.101 | 0.854–1.418 | 0.4575 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badia, J.M.; Flores-Yelamos, M.; Vázquez, A.; Arroyo-García, N.; Puig-Asensio, M.; Parés, D.; Pera, M.; López-Contreras, J.; Limón, E.; Pujol, M.; et al. Oral Antibiotic Prophylaxis Lowers Surgical Site Infection in Elective Colorectal Surgery: Results of a Pragmatic Cohort Study in Catalonia. J. Clin. Med. 2021, 10, 5636. https://doi.org/10.3390/jcm10235636
Badia JM, Flores-Yelamos M, Vázquez A, Arroyo-García N, Puig-Asensio M, Parés D, Pera M, López-Contreras J, Limón E, Pujol M, et al. Oral Antibiotic Prophylaxis Lowers Surgical Site Infection in Elective Colorectal Surgery: Results of a Pragmatic Cohort Study in Catalonia. Journal of Clinical Medicine. 2021; 10(23):5636. https://doi.org/10.3390/jcm10235636
Chicago/Turabian StyleBadia, Josep M., Miriam Flores-Yelamos, Ana Vázquez, Nares Arroyo-García, Mireia Puig-Asensio, David Parés, Miguel Pera, Joaquín López-Contreras, Enric Limón, Miquel Pujol, and et al. 2021. "Oral Antibiotic Prophylaxis Lowers Surgical Site Infection in Elective Colorectal Surgery: Results of a Pragmatic Cohort Study in Catalonia" Journal of Clinical Medicine 10, no. 23: 5636. https://doi.org/10.3390/jcm10235636