
Predictors of Lymph Node Metastasis in T1 Colorectal Cancer in Young Patients: Results from a National Cancer Registry

 ,
,  ,
,
Abstract
:1. Introduction
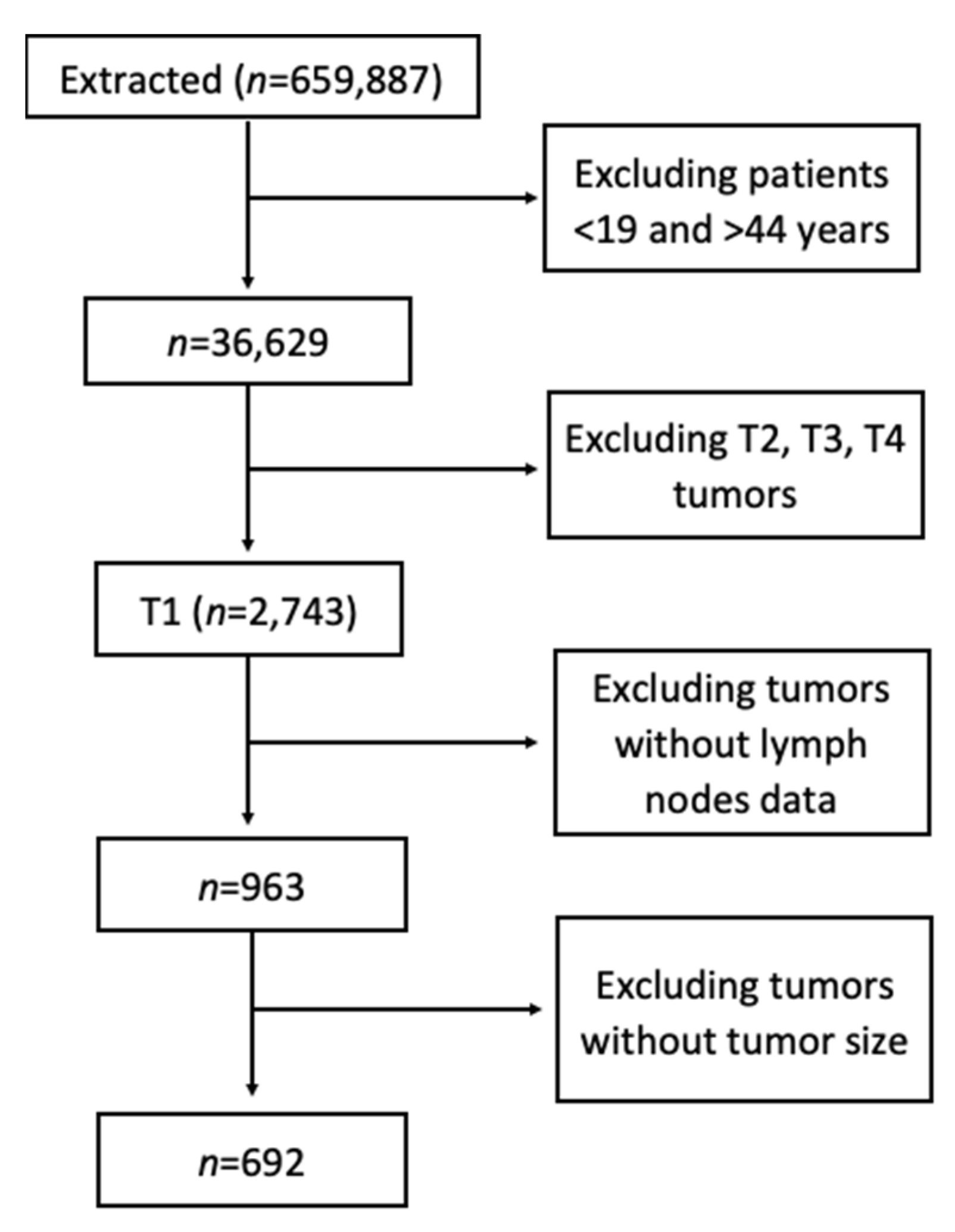
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographics and Tumor Characteristics
3.2. Predictors of Lymph Node Metastasis (LNM)
3.3. Clinical Predictors of Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Me, J.F.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Guo, K.; Feng, Y.; Yuan, L.; Wasan, H.S.; Sun, L.; Shen, M.; Ruan, S. Risk factors and predictors of lymph nodes metastasis and distant metastasis in newly diagnosed T1 colorectal cancer. Cancer Med. 2020, 9, 5095–5113. [Google Scholar] [CrossRef]
- Dai, W.; Mo, S.; Xiang, W.; Han, L.; Li, Q.; Wang, R.; Xu, Y.; Cai, G. The Critical Role of Tumor Size in Predicting Prognosis for T1 Colon Cancer. Oncologist 2020, 25, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Xie, X.; Yin, J.; Zhou, Z.; Dang, C.; Zhang, H.; Zhang, Y. Young age increases the risk for lymph node metastasis in patients with early Colon Cancer. BMC Cancer 2019, 19, 803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramai, D.; Ofosu, A.; Solanki, V.; Lai, J.K.; Barakat, M.; Dhaliwal, A.; Aamar, A.; Aloreidi, K.; Mohan, B.P.; Reddy, M.; et al. Incidence Rates, Treatment, and Survival of Rectal Cancer Among Young Patients: A Nationwide Cohort Study. J. Clin. Gastroenterol. 2021, 55, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Loomans-Kropp, H.A.; Umar, A. Increasing Incidence of Colorectal Cancer in Young Adults. J. Cancer Epidemiol. 2019, 2019, 9841295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wada, H.; Shiozawa, M.; Katayama, K.; Okamoto, N.; Miyagi, Y.; Rino, Y.; Masuda, M.; Akaike, M. Systematic review and meta-analysis of histopathological predictive factors for lymph node metastasis in T1 colorectal cancer. J. Gastroenterol. 2015, 50, 727–734. [Google Scholar] [CrossRef]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Abdelsattar, Z.M.; Wong, S.L.; Regenbogen, S.E.; Bs, D.M.J.; Hardiman, K.M.; Hendren, S. Colorectal cancer outcomes and treatment patterns in patients too young for average-risk screening. Cancer 2016, 122, 929–934. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Zhang, C.; Ni, X.; Wu, J.; Pan, C.; Wang, S.; Yu, J. Population-based analysis on predictors for lymph node metastasis in T1 colon cancer. Surg. Endosc. 2020, 34, 4030–4040. [Google Scholar] [CrossRef] [Green Version]
- Triantafillidis, J.K.; Nasioulas, G.; Kosmidis, P.A. Colorectal cancer and inflammatory bowel disease: Epidemiology, risk factors, mechanisms of carcinogenesis and prevention strategies. Anticancer Res. 2009, 29, 2727–2737. [Google Scholar] [PubMed]
- Liang, J.T.; Huang, K.-C.; Cheng, A.-L.; Jeng, Y.M.; Wu, M.-S.; Wang, S.M. Clinicopathological and molecular biological features of colorectal cancer in patients less than 40 years of age. Br. J. Surg. 2003, 90, 205–214. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force. Screening for colorectal cancer: Recommendation and rationale. Ann. Intern. Med. 2002, 137, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.E.; Murphy, J.D.; Gomez, S.L. Black–White Disparities in Young-Onset Colorectal Cancer: Understanding Complexity in Reported Differences. Gastroenterology 2019, 156, 858–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, K.; Hill, E.G.; Lewin, D.N.; Williamson, G.; Oppenheimer, S.; Ford, M.E.; Wargovich, M.J.; Berger, F.G.; Bolick, S.W.; Thomas, M.B.; et al. Racial disparities in advanced-stage colorectal cancer survival. Cancer Causes Control. 2013, 24, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, D.A.; Furman, W.L.; Billups, C.A.; Riedley, S.E.; Cain, A.M.; Rao, B.N.; Pratt, C.B.; Spunt, S.L. Colorectal Carcinoma in Childhood and Adolescence: A Clinicopathologic Review. J. Clin. Oncol. 2007, 25, 5808–5814. [Google Scholar] [CrossRef]
- Ballester, V.; Rashtak, S.; Boardman, L. Clinical and molecular features of young-onset colorectal cancer. World J. Gastroenterol. 2016, 22, 1736–1744. [Google Scholar] [CrossRef]
- Davis, D.M.; Marcet, J.E.; Frattini, J.C.; Prather, A.D.; Mateka, J.J.; Nfonsam, V.N. Is It Time to Lower the Recommended Screening Age for Colorectal Cancer? J. Am. Coll. Surg. 2011, 213, 352–361. [Google Scholar] [CrossRef]
- Ahnen, D.J.; Wade, S.W.; Jones, W.F.; Sifri, R.; Silveiras, J.M.; Greenamyer, J.; Guiffre, S.; Axilbund, J.; Spiegel, A.; You, Y.N. The Increasing Incidence of Young-Onset Colorectal Cancer: A Call to Action. Mayo Clin. Proc. 2014, 89, 216–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, J.B.; Maggard, M.A.; Liu, J.H.; Etzioni, D.A.; Livingston, E.H.; Ko, C.Y. Do Young Colon Cancer Patients Have Worse Outcomes? World J. Surg. 2004, 28, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Yeo, S.A.; Chew, M.H.; Koh, P.K.; Tang, C.L. Young colorectal carcinoma patients do not have a poorer prognosis: A comparative review of 2426 cases. Tech. Coloproctol. 2013, 17, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Kastrinos, F.; Syngal, S. Inherited Colorectal Cancer Syndromes. Cancer J. 2011, 17, 405–415. [Google Scholar] [CrossRef] [Green Version]
- Hampel, H.; Frankel, W.L.; Martin, E.; Arnold, M.; Khanduja, K.; Kuebler, P.; Clendenning, M.; Sotamaa, K.; Prior, T.; Westman, J.A.; et al. Feasibility of Screening for Lynch Syndrome Among Patients With Colorectal Cancer. J. Clin. Oncol. 2008, 26, 5783–5788. [Google Scholar] [CrossRef] [PubMed]
- Aarnio, M.; Sankila, R.; Pukkala, E.; Salovaara, R.; Aaltonen, L.; de la Chapelle, A.; Mecklin, J.-P. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int. J. Cancer 1999, 81, 214–218. [Google Scholar] [CrossRef]
- Atikukke, G.; Alkhateeb, A.; Porter, L.; Fifield, B.; Cavallo-Medved, D.; Facca, J.; Elfiki, T.; Elkeilani, A.; Rueda, L.; Misra, S. P-370 Comprehensive targeted genomic profiling and comparative genomic analysis to identify molecular mechanisms driving cancer progression in young-onset sporadic colorectal cancer. Ann. Oncol. 2020, 31, S209–S210. [Google Scholar] [CrossRef]
- Perea, J.; Rueda, D.; Canal, A.; Rodríguez, Y.; Álvaro, E.; Osorio, I.; Alegre, C.; Rivera, B.; Martinez-Lopez, J.; Benítez, J.; et al. Age at Onset Should Be a Major Criterion for Subclassification of Colorectal Cancer. J. Mol. Diagn. 2014, 16, 116–126. [Google Scholar] [CrossRef]
- Ogino, S.; Nosho, K.; Kirkner, G.J.; Kawasaki, T.; Chan, A.T.; Schernhammer, E.S.; Giovannucci, E.L.; Fuchs, C.S. A Cohort Study of Tumoral LINE-1 Hypomethylation and Prognosis in Colon Cancer. J. Natl. Cancer Inst. 2008, 100, 1734–1738. [Google Scholar] [CrossRef] [Green Version]
- Antelo, M.; Balaguer, F.; Shia, J.; Shen, Y.; Hur, K.; Moreira, L.; Cuatrecasas, M.; Bujanda, L.; Giraldez, M.D.; Takahashi, M.; et al. A High Degree of LINE-1 Hypomethylation Is a Unique Feature of Early-Onset Colorectal Cancer. PLoS ONE 2012, 7, e45357. [Google Scholar] [CrossRef]
- Overwater, A.; Kessels, K.; Elias, S.G.; Backes, Y.; Spanier, B.W.M.; Seerden, T.C.J.; Pullens, H.J.M.; van den Blink, A.; Offerhaus, G.J.A.; van Bergeijk, J.; et al. Endoscopic resection of high-risk T1 colorectal carcinoma prior to surgical resection has no adverse effect on long-term outcomes. Gut 2018, 67, 284–290. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | Percent |
|---|---|---|
| Sex | ||
| Male | 319 | 46.1% |
| Female | 373 | 53.9% |
| Race | ||
| White | 538 | 77.7% |
| Black | 85 | 12.3% |
| American Indian/Alaska Native | 54 | 7.8% |
| Asian or Pacific Islander | 7 | 1.0% |
| Unknown | 8 | 1.2% |
| Age | ||
| 19–24 years | 37 | 5.3% |
| 25–29 years | 57 | 8.2% |
| 30–34 years | 107 | 15.5% |
| 35–39 years | 149 | 21.5% |
| 40–44 years | 342 | 49.4% |
| N Staging (TNM) | ||
| N0 | 536 | 77.5% |
| N1 | 156 | 22.5% |
| Regional Nodes | ||
| Negative regional node | 543 | 78.5% |
| Positive regional node | 149 | 21.5% |
| Tumor Grade | ||
| Well differentiated; Grade I | 57 | 8.2% |
| Moderately differentiated; Grade II | 176 | 25.5% |
| Poorly differentiated; Grade III | 413 | 59.8% |
| Undifferentiated; anaplastic; Grade IV | 36 | 5.2% |
| Unknown | 10 | 1.4% |
| Tumor Size | ||
| ≤0.9 cm | 197 | 28.5% |
| 1 cm–1.9 cm | 223 | 32.2% |
| 2.0 cm–2.9 cm | 130 | 18.8% |
| ≥3.0 cm | 142 | 20.5% |
| Laterality | ||
| Left side | 423 | 61.1% |
| Right side | 231 | 33.4% |
| Unknown | 38 | 5.5.% |
| Histology | ||
| Adenocarcinoma | 522 | 75.4% |
| Mucinous type | 18 | 2.6% |
| Unknown | 152 | 22.0% |
| Multivariate | Univariate | |||||
|---|---|---|---|---|---|---|
| Characteristics | Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value |
| Sex | ||||||
| Male | 1.00 | 1.00 | ||||
| Female | 0.93 | 0.63–1.35 | 0.693 | 0.95 | 0.66–1.37 | 0.791 |
| Age Group | ||||||
| 19–24 years | 1.00 | 1.00 | ||||
| 25–29 years | 2.10 | 0.67–6.64 | 0.548 | 2.08 | 0.68–6.38 | 0.198 |
| 30–34 years | 1.52 | 0.50–4.58 | 0.206 | 1.38 | 0.48–4.01 | 0.552 |
| 35–39 years | 2.21 | 0.75–6.47 | 0.461 | 2.06 | 0.75–5.67 | 0.163 |
| 40–44 years | 2.02 | 0.71–5.72 | 0.149 | 1.80 | 0.68–4.77 | 0.239 |
| Race | ||||||
| White | 1.00 | 1.00 | ||||
| Black | 1.20 | 0.68–2.10 | 0.527 | 1.16 | 0.67–1.99 | 0.604 |
| Asian or Pacific Islander | 1.29 | 0.66–2.52 | 0.461 | 1.31 | 0.69–2.50 | 0.406 |
| American Indian/Alaska Native | 1.86 | 0.33–10.36 | 0.480 | 1.50 | 0.29–7.84 | 0.630 |
| Tumor Grade | ||||||
| Well differentiated; Grade I | 1.00 | 1.00 | ||||
| Moderately differentiated; Grade II | 1.04 | 0.47–2.31 | 0.922 | 0.97 | 0.45–2.06 | 0.927 |
| Poorly differentiated; Grade III | 1.24 | 0.58–2.66 | 0.579 | 1.15 | 0.57–2.31 | 0.697 |
| Undifferentiated; anaplastic; Grade IV | 2.94 | 1.06–8.12 | 0.038 | 2.66 | 1.04–6.81 | 0.041 |
| Tumor Size | ||||||
| ≤0.9 cm | 1.00 | 1.00 | ||||
| 1 cm–1.9 cm | 2.92 | 1.71–4.97 | <0.001 | 2.92 | 1.74–4.89 | <0.001 |
| 2.0 cm–2.9 cm | 2.00 | 1.05–3.77 | 0.034 | 1.80 | 0.983–3.30 | 0.057 |
| ≥3.0 cm | 2.68 | 1.43–5.01 | 0.002 | 2.36 | 1.33–4.18 | 0.003 |
| Laterality | ||||||
| Left side | 1.00 | 1.00 | ||||
| Right side | 0.64 | 0.38–1.08 | 0.091 | 0.81 | 0.54–1.20 | 0.288 |
| Histology | ||||||
| Adenocarcinoma | 1.00 | 1.00 | ||||
| Mucinous type | 0.87 | 0.23–3.28 | 0.833 | 1.35 | 0.38–4.75 | 0.640 |
| Unknown | 2.37 | 1.18–4.74 | 0.015 | 1.51 | 0.41–5.51 | 0.534 |
| Multivariate | Univariate | |||||
|---|---|---|---|---|---|---|
| Characteristics | Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value |
| Sex | ||||||
| Male | 1.00 | 1.00 | ||||
| Female | 0.58 | 0.18–1.89 | 0.365 | 0.61 | 0.19–1.9 | 0.396 |
| Age Group | ||||||
| 19–24 years | 1.00 | 1.00 | ||||
| 25–29 years | 22,042 | 0.00–2.15 × 10127 | 0.945 | 9932.075 | 0.00–6.92 × 10108 | 0.940 |
| 30–34 years | 5751.15 | 0.00–5.61 × 10126 | 0.952 | 4424.739 | 0.00–3.08 × 10108 | 0.946 |
| 35–39 years | 7052.66 | 0.00–6.86 × 10126 | 0.951 | 10,214.540 | 0.00–7.08 × 10108 | 0.940 |
| 40–44 years | 7385.87 | 0.00–7.18 × 10126 | 0.951 | 9932.075 | 0.00–6.76 × 10108 | 0.941 |
| Race | ||||||
| White | 1.00 | 1.00 | ||||
| Black | <0.01 | 0.00–3.45 × 1012 | 0.718 | 0.034 | 0.00–76.81 | 0.390 |
| Asian or Pacific Islander | <0.01 | 0.00–1.03 × 1019 | 0.783 | 0.034 | 0.00–535.59 | 0.492 |
| American Indian/Alaska Native | <0.01 | 0.00–0.00 | 0.982 | 0.034 | 0.00–3.2 × 1010 | 0.810 |
| Regional Nodes | ||||||
| Negative regional node | 1.00 | 1.00 | ||||
| Positive regional node | 4.43 | 1.27–15.52 | 0.020 | 5.45 | 1.73–17.18 | 0.004 |
| Tumor Grade | ||||||
| Well differentiated; Grade I | 1.00 | 1.00 | ||||
| Moderately differentiated; Grade II | <0.01 | 0.00–2.04 × 1054 | 0.881 | <0.01 | 0.00–5.01 × 10216 | 0.961 |
| Poorly differentiated; Grade III | 0.20 | 0.03–1.25 | 0.086 | 0.43 | 0.09–2.13 | 0.302 |
| Undifferentiated; anaplastic; Grade IV | 1.34 | 0.20–8.98 | 0.764 | 3.34 | 0.61–18.29 | 0.164 |
| Tumor Size | ||||||
| ≤0.9 cm | 1.00 | 1.00 | ||||
| 1 cm–1.9 cm | 488.62 | 0.00–4.08 × 1012 | 0.595 | 55,877.89 | 0.00–3.00 × 1096 | 0.919 |
| 2.0 cm–2.9 cm | 0.43 | 0.00–1.29 × 1020 | 0.972 | 1.01 | 0.00–2.83 × 10139 | 1.00 |
| ≥3.0 cm | 633.04 | 0.00–5.31 × 1012 | 0.582 | 80,201.33 | 0.00–4.31 × 1096 | 0.917 |
| Laterality | ||||||
| Left side | 1.00 | 1.00 | ||||
| Right side | 1.52 | 0.34–6.80 | 0.586 | 0.76 | 0.20–2.88 | 0.690 |
| Histology | ||||||
| Adenocarcinoma | 1.00 | 1.00 | ||||
| Mucinous type | 4881.73 | 0.00–8.83 × 1093 | 0.981 | 25,990.41 | 0.00–1.44 × 10234 | 0.970 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramai, D.; Singh, J.; Facciorusso, A.; Chandan, S.; Dhindsa, B.; Dhaliwal, A.; Galassi, B.; Tomasello, G.; Ghidini, M. Predictors of Lymph Node Metastasis in T1 Colorectal Cancer in Young Patients: Results from a National Cancer Registry. J. Clin. Med. 2021, 10, 5511. https://doi.org/10.3390/jcm10235511
Ramai D, Singh J, Facciorusso A, Chandan S, Dhindsa B, Dhaliwal A, Galassi B, Tomasello G, Ghidini M. Predictors of Lymph Node Metastasis in T1 Colorectal Cancer in Young Patients: Results from a National Cancer Registry. Journal of Clinical Medicine. 2021; 10(23):5511. https://doi.org/10.3390/jcm10235511
Chicago/Turabian StyleRamai, Daryl, Jameel Singh, Antonio Facciorusso, Saurabh Chandan, Banreet Dhindsa, Amaninder Dhaliwal, Barbara Galassi, Gianluca Tomasello, and Michele Ghidini. 2021. "Predictors of Lymph Node Metastasis in T1 Colorectal Cancer in Young Patients: Results from a National Cancer Registry" Journal of Clinical Medicine 10, no. 23: 5511. https://doi.org/10.3390/jcm10235511