
The P2Y12 Receptor Antagonist Selatogrel Dissolves Preformed Platelet Thrombi In Vivo

 , and
, and 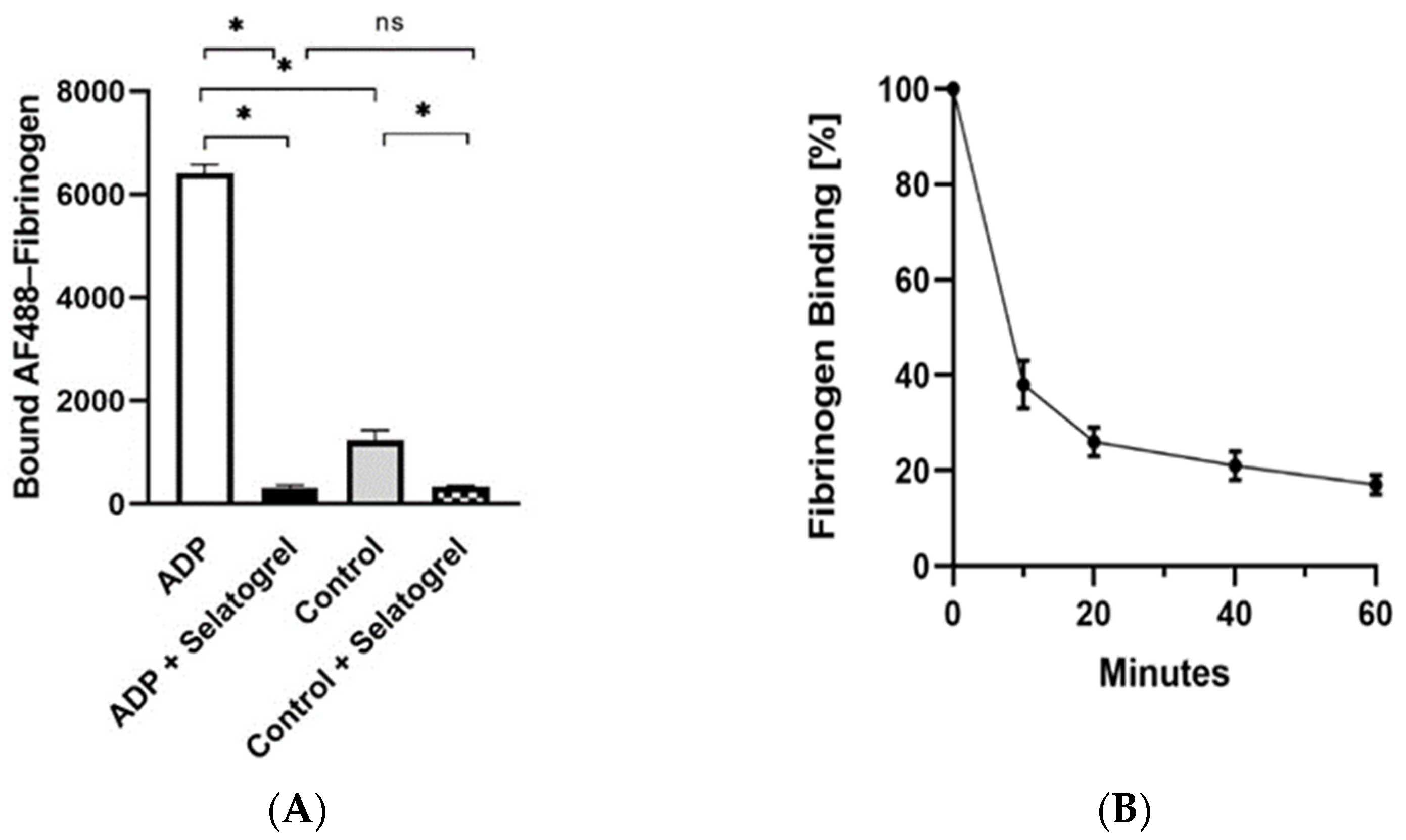{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Selatogrel Is Rapidly Absorbed after Subcutaneous Injection in Mice
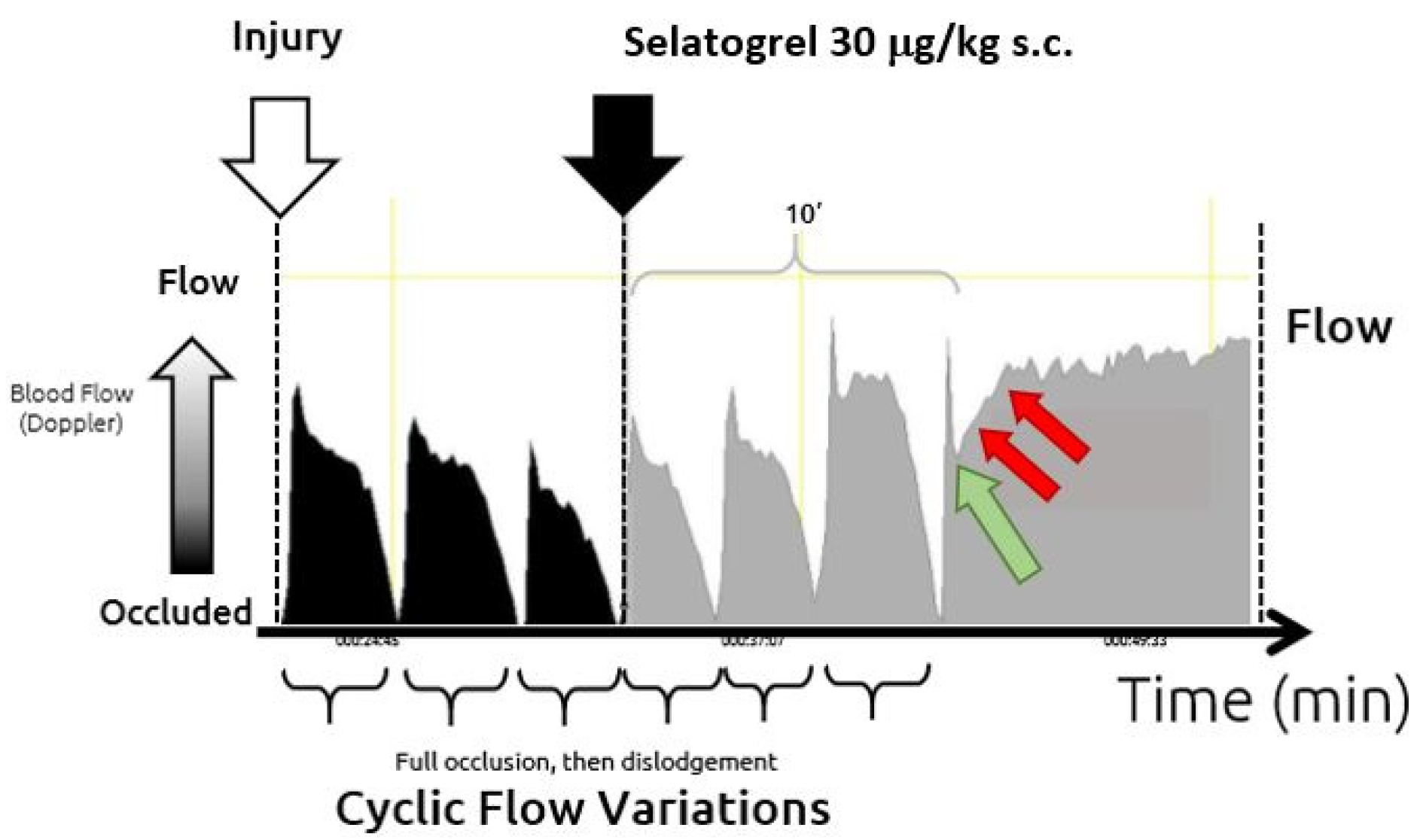
3.2. Subcutaneous Injection of Selatogrel Is Antithrombotic in Guinea Pigs
3.3. Selatogrel Dissolves Platelet Thrombi in Mice
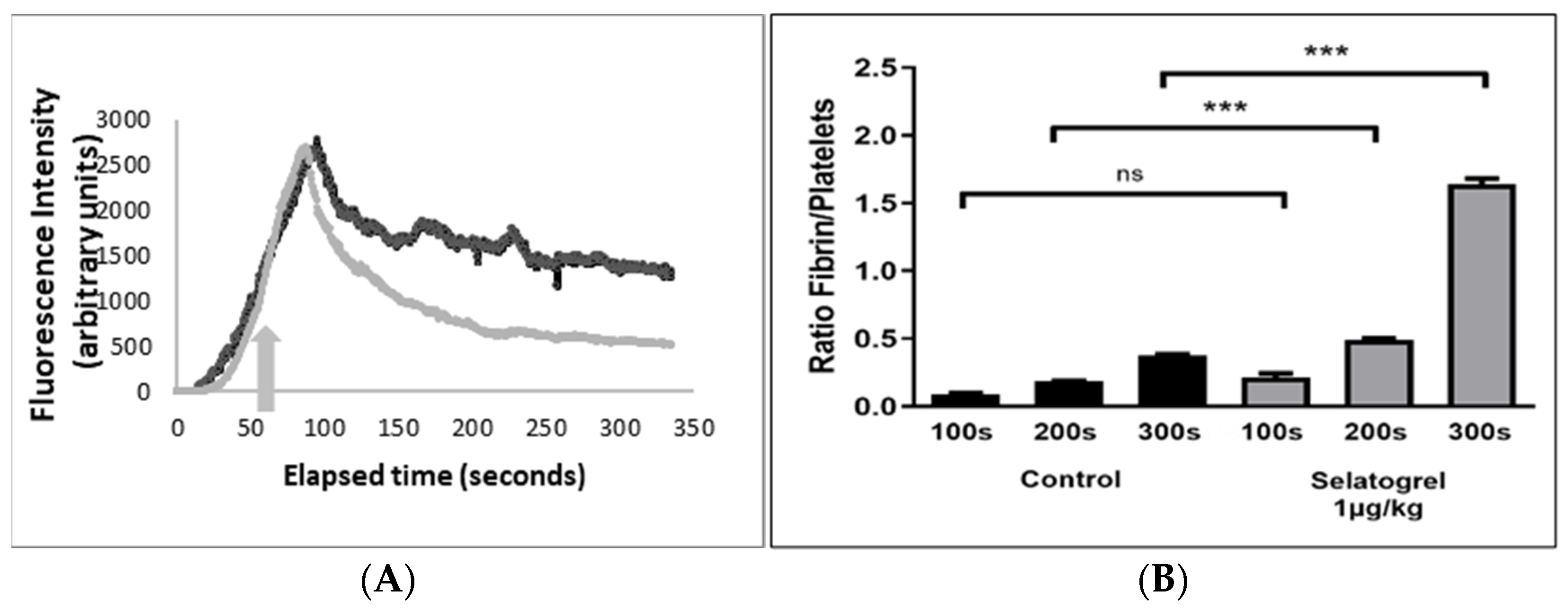
3.4. Selatogrel Dissolves Consolidated Platelet Thrombi
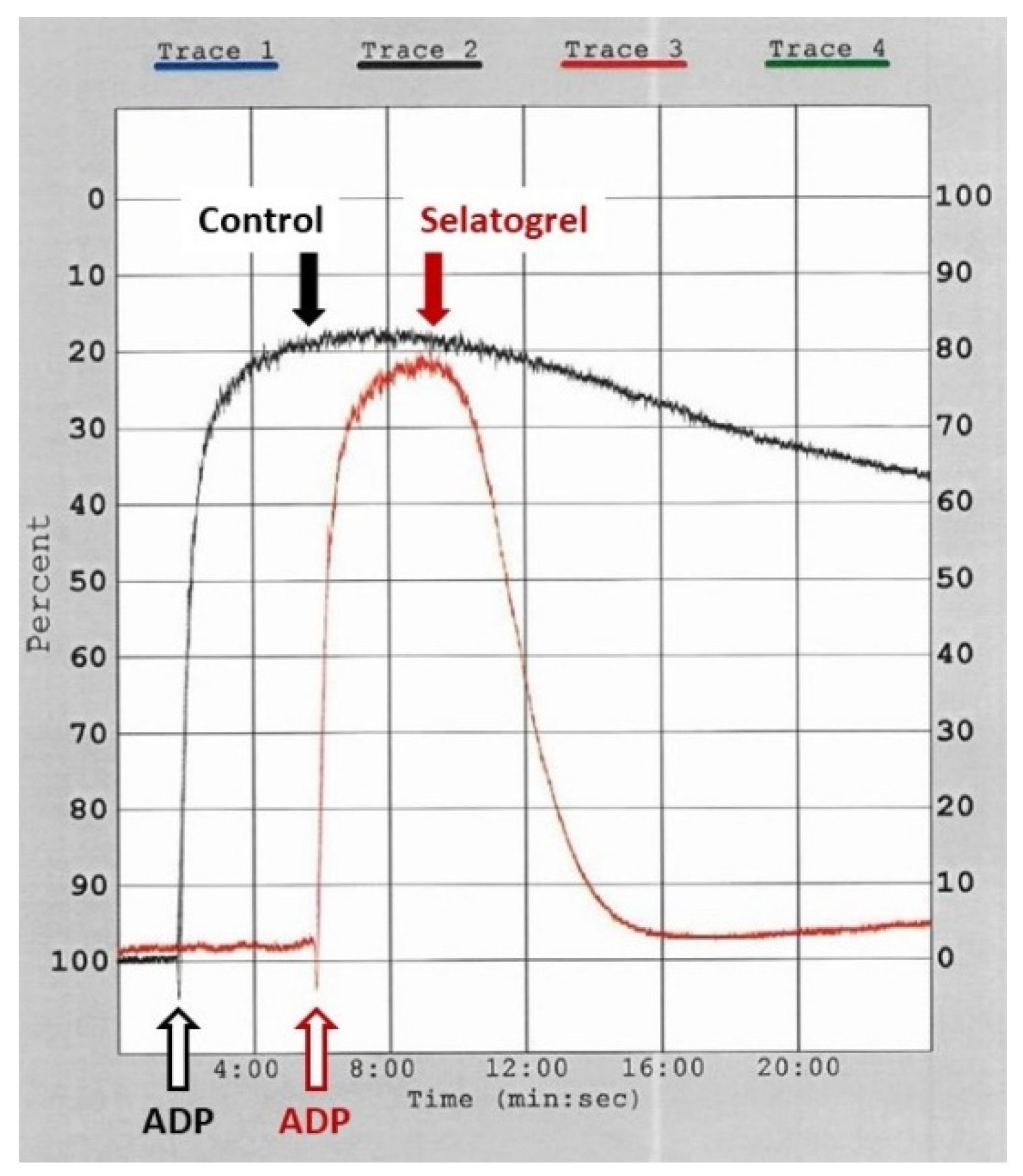
3.5. Selatogrel Dissolves Aggregated Human Platelets
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davies, M.J.; Thomas, A.C.; Knapman, P.A.; Hangartner, J.R. Intramyocardial Platelet Aggregation in Patients with Unstable Angina Suffering Sudden Ischemic Cardiac Death. Circulation 1986, 73, 418–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coller, B.S. Historical Perspective and Future Directions in Platelet Research: Platelet History and Future Directions. J. Thromb. Haemost. 2011, 9, 374–395. [Google Scholar] [CrossRef] [Green Version]
- Storey, R.F.; Sanderson, H.M.; White, A.E.; May, J.A.; Cameron, K.E.; Heptinstall, S. The Central Role of the P2T Receptor in Amplification of Human Platelet Activation, Aggregation, Secretion and Procoagulant Activity. Br. J. Haematol. 2000, 110, 925–934. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients with Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2016, 134, e123–e155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cayla, G.; Silvain, J.; Collet, J.-P.; Montalescot, G. Updates and Current Recommendations for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes: What It Means for Clinical Practice. Am. J. Cardiol. 2015, 115, 10A–22A. [Google Scholar] [CrossRef]
- Rodriguez, F.; Mahaffey, K.W. Management of Patients with NSTE-ACS. J. Am. Coll. Cardiol. 2016, 68, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.P. Arterial Thrombosis—Insidious, Unpredictable and Deadly. Nat. Med. 2011, 17, 1423–1436. [Google Scholar] [CrossRef]
- Parker, W.A.E.; Storey, R.F. Novel Approaches to P2Y12 Inhibition and Aspirin Dosing. Platelets 2021, 32, 7–14. [Google Scholar] [CrossRef]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of Plaque Formation and Rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef]
- Shattil, S.J.; Kim, C.; Ginsberg, M.H. The Final Steps of Integrin Activation: The End Game. Nat. Rev. Mol. Cell Biol. 2010, 11, 288–300. [Google Scholar] [CrossRef] [Green Version]
- Stephens, G.; He, M.; Wong, C.; Jurek, M.; Luedemann, H.-C.; Shapurian, G.; Munnelly, K.; Muir, C.; Conley, P.B.; Phillips, D.R.; et al. Development of a Perfusion Chamber Assay to Study in Real Time the Kinetics of Thrombosis and the Antithrombotic Characteristics of Antiplatelet Drugs. Thromb. J. 2012, 10, 11. [Google Scholar] [CrossRef]
- Goto, S.; Tamura, N.; Ishida, H.; Ruggeri, Z.M. Dependence of Platelet Thrombus Stability on Sustained Glycoprotein IIb/IIIa Activation Through Adenosine 5′-Diphosphate Receptor Stimulation and Cyclic Calcium Signaling. J. Am. Coll. Cardiol. 2006, 47, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Cosemans, J.M.E.M.; Munnix, I.C.A.; Wetzker, R.; Heller, R.; Jackson, S.P.; Heemskerk, J.W.M. Continuous Signaling via PI3K Isoforms Beta and Is Required for Platelet ADP Receptor Function in Dynamic Thrombus Stabilization. Blood 2006, 108, 3045–3052. [Google Scholar] [CrossRef] [PubMed]
- Phillips, D.R.; Teng, W.; Arfsten, A.; Nannizzi-Alaimo, L.; White, M.M.; Longhurst, C.; Shattil, S.J.; Randolph, A.; Jakubowski, J.A.; Jennings, L.K.; et al. Effect of Ca2+ on GP IIb-IIIa Interactions With Integrilin: Enhanced GP IIb-IIIa Binding and Inhibition of Platelet Aggregation by Reductions in the Concentration of Ionized Calcium in Plasma Anticoagulated With Citrate. Circulation 1997, 96, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Evans, R.J.; Mahaut-Smith, M.P. Extracellular Ca2+ Modulates ADP-Evoked Aggregation through Altered Agonist Degradation: Implications for Conditions Used to Study P2Y Receptor Activation: Role of Ectonucleotidases in Ca2+-Dependent Platelet Aggregation. Br. J. Haematol. 2011, 153, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pittens, C.A.C.M.; Bouman, H.J.; Van Werkum, J.W.; Ten Berg, J.M.; Hackeng, C.M. Comparison between Hirudin and Citrate in Monitoring the Inhibitory Effects of P2Y12 Receptor Antagonists with Different Platelet Function Tests. J. Thromb. Haemost. 2009, 7, 1929–1932. [Google Scholar] [CrossRef]
- Arnout, J.; Hoylaerts, M.F.; Lijnen, H.R. Haemostasis. In The Vascular Endothelium II; Moncada, S., Higgs, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2006; Volume 176/II, pp. 1–41. ISBN 978-3-540-36027-8. [Google Scholar]
- Stassen, J.; Arnout, J.; Deckmyn, H. The Hemostatic System. CMC 2004, 11, 2245–2260. [Google Scholar] [CrossRef]
- Caroff, E.; Hubler, F.; Meyer, E.; Renneberg, D.; Gnerre, C.; Treiber, A.; Rey, M.; Hess, P.; Steiner, B.; Hilpert, K.; et al. 4-((R)-2-{[6-((S)-3-Methoxypyrrolidin-1-Yl)-2-Phenylpyrimidine-4-Carbonyl]Amino}-3-Phosphonopropionyl)Piperazine-1-Carboxylic Acid Butyl Ester (ACT-246475) and Its Prodrug (ACT-281959), a Novel P2Y12 Receptor Antagonist with a Wider Therapeutic Window in the Rat Than Clopidogrel. J. Med. Chem. 2015, 58, 9133–9153. [Google Scholar] [CrossRef]
- Rey, M.; Kramberg, M.; Hess, P.; Morrison, K.; Ernst, R.; Haag, F.; Weber, E.; Clozel, M.; Baumann, M.; Caroff, E.; et al. The Reversible P2Y12 Antagonist ACT-246475 Causes Significantly Less Blood Loss than Ticagrelor at Equivalent Antithrombotic Efficacy in Rat. Pharmacol. Res. Perspect. 2017, 5, e00338. [Google Scholar] [CrossRef] [Green Version]
- Crescence, L.; Darbousset, R.; Caroff, E.; Hubler, F.; Riederer, M.A.; Panicot-Dubois, L.; Dubois, C. Selatogrel, a Reversible P2Y12 Receptor Antagonist, Has Reduced off-Target Interference with Haemostatic Factors in a Mouse Thrombosis Model. Thromb. Res. 2021, 200, 133–140. [Google Scholar] [CrossRef]
- Dubois, C.; Panicot-Dubois, L.; Gainor, J.F.; Furie, B.C.; Furie, B. Thrombin-Initiated Platelet Activation in Vivo Is VWF Independent during Thrombus Formation in a Laser Injury Model. J. Clin. Investig. 2007, 117, 953–960. [Google Scholar] [CrossRef] [Green Version]
- Mege, D.; Panicot-Dubois, L.; Ouaissi, M.; Robert, S.; Sielezneff, I.; Sastre, B.; Dignat-George, F.; Dubois, C. The Origin and Concentration of Circulating Microparticles Differ According to Cancer Type and Evolution: A Prospective Single-Center Study: Signature of Microparticles in Digestive Cancers. Int. J. Cancer 2016, 138, 939–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Born, G.V.R.; Haslam, R.J.; Goldman, M.; Lowe, R.D. Comparative Effectiveness of Adenosine Analogues as Inhibitors of Blood-Platelet Aggregation and as Vasodilators in Man. Nature 1965, 205, 678–680. [Google Scholar] [CrossRef]
- Lombardi, F.; De Chaumont, C.; Shields, D.C.; Moran, N. Platelet Signalling Networks: Pathway Perturbation Demonstrates Differential Sensitivity of ADP Secretion and Fibrinogen Binding. Platelets 2012, 23, 17–25. [Google Scholar] [CrossRef]
- Garcia, C.; Maurel-Ribes, A.; Nauze, M.; N’Guyen, D.; Martinez, L.O.; Payrastre, B.; Sénard, J.-M.; Galés, C.; Pons, V. Deciphering Biased Inverse Agonism of Cangrelor and Ticagrelor at P2Y12 Receptor. Cell. Mol. Life Sci. 2019, 76, 561–576. [Google Scholar] [CrossRef]
- Torr, S.; Noble, M.I.; Folts, J.D. Inhibition of Acute Platelet Thrombosis Formation in Stenosed Canine Coronary Arteries by Specific Serotonin 5HT2 Receptor Antagonist Ritanserin. Cardiovasc. Res. 1990, 24, 465–470. [Google Scholar] [CrossRef]
- Storey, R.F.; Gurbel, P.A.; ten Berg, J.; Bernaud, C.; Dangas, G.D.; Frenoux, J.-M.; Gorog, D.A.; Hmissi, A.; Kunadian, V.; James, S.K.; et al. Pharmacodynamics, Pharmacokinetics, and Safety of Single-Dose Subcutaneous Administration of Selatogrel, a Novel P2Y12 Receptor Antagonist, in Patients with Chronic Coronary Syndromes. Eur. Heart J. 2020, 41, 3132–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speich, H.E.; Bhal, V.; Houser, K.H.; Caughran, A.T.; Lands, L.T.; Houng, A.K.; Bäckstrom, J.; Enerbäck, M.; Reed, G.L.; Jennings, L.K. Signaling via P2Y12 May Be Critical for Early Stabilization of Platelet Aggregates. J. Cardiovasc. Pharmacol. 2014, 63, 520–527. [Google Scholar] [CrossRef]
- Kamae, T.; Shiraga, M.; Kashiwagi, H.; Kato, H.; Tadokoro, S.; Kurata, Y.; Tomiyama, Y.; Kanakura, Y. Critical Role of ADP Interaction with P2Y12 Receptor in the Maintenance of AlphaIIbbeta3 Activation: Association with Rap1B Activation. J. Thromb. Haemost. 2006, 4, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Podolnikova, N.P.; Yakovlev, S.; Yakubenko, V.P.; Wang, X.; Gorkun, O.V.; Ugarova, T.P. The Interaction of Integrin α IIb β 3 with Fibrin Occurs through Multiple Binding Sites in the α IIb β-Propeller Domain. J. Biol. Chem. 2014, 289, 2371–2383. [Google Scholar] [CrossRef] [Green Version]
- Andre, P.; DeGuzman, F.; Haberstock-Debic, H.; Mills, S.; Pak, Y.; Inagaki, M.; Pandey, A.; Hollenbach, S.; Phillips, D.R.; Conley, P.B. Thienopyridines, but Not Elinogrel, Result in Off-Target Effects at the Vessel Wall That Contribute to Bleeding. J. Pharmacol. Exp. Ther. 2011, 338, 22–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumann, M.; Lack, B.; Guillaumat, I.; Murphy, M.J.; Riederer, M.A. The Potency of Selatogrel, a Reversible Antagonist of the P2Y12 Receptor, Is Affected by Calcium Concentration. Platelets 2021. [Google Scholar] [CrossRef]
- Ivanciu, L.; Stalker, T.J. Spatiotemporal Regulation of Coagulation and Platelet Activation during the Hemostatic Response in Vivo. J. Thromb. Haemost. 2015, 13, 1949–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stalker, T.J.; Traxler, E.A.; Wu, J.; Wannemacher, K.M.; Cermignano, S.L.; Voronov, R.; Diamond, S.L.; Brass, L.F. Hierarchical Organization in the Hemostatic Response and Its Relationship to the Platelet-Signaling Network. Blood 2013, 121, 1875–1885. [Google Scholar] [CrossRef]
- Hulot, J.-S.; Montalescot, G. Do We Need a New P2Y12 Receptor Antagonist? Eur. Heart J. 2020, 41, 3141–3143. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crescence, L.; Kramberg, M.; Baumann, M.; Rey, M.; Roux, S.; Panicot-Dubois, L.; Dubois, C.; Riederer, M.A. The P2Y12 Receptor Antagonist Selatogrel Dissolves Preformed Platelet Thrombi In Vivo. J. Clin. Med. 2021, 10, 5349. https://doi.org/10.3390/jcm10225349
Crescence L, Kramberg M, Baumann M, Rey M, Roux S, Panicot-Dubois L, Dubois C, Riederer MA. The P2Y12 Receptor Antagonist Selatogrel Dissolves Preformed Platelet Thrombi In Vivo. Journal of Clinical Medicine. 2021; 10(22):5349. https://doi.org/10.3390/jcm10225349
Chicago/Turabian StyleCrescence, Lydie, Markus Kramberg, Martine Baumann, Markus Rey, Sebastien Roux, Laurence Panicot-Dubois, Christophe Dubois, and Markus A. Riederer. 2021. "The P2Y12 Receptor Antagonist Selatogrel Dissolves Preformed Platelet Thrombi In Vivo" Journal of Clinical Medicine 10, no. 22: 5349. https://doi.org/10.3390/jcm10225349