
Elbow Stiffness Imaging: A Practical Diagnostic and Pretherapeutic Approach

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Anatomy and Biomechanics
3. Clinical Presentation
3.1. Extra-Articular Elbow Stiffness
3.2. Intra-Articular Stiffness
4. Imaging Assessment of Elbow Stiffness
5. Imaging Workup
5.1. Conventional Radiographs
5.2. Ultrasonography
5.3. CT and CT Arthrography
5.4. MR Imaging
5.5. Dynamic and Kinematic CT
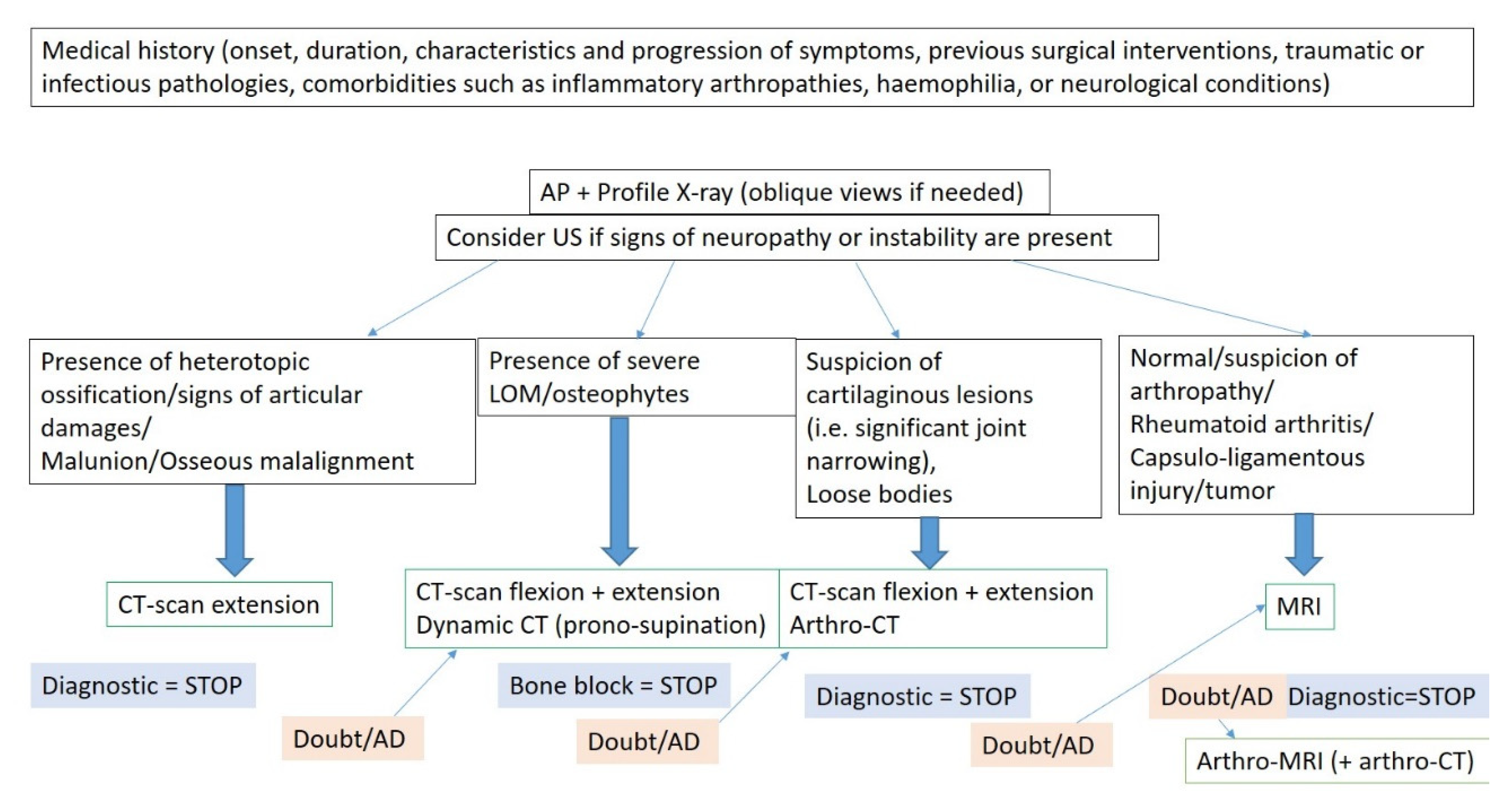
5.6. Rationale for Determining the Optimal Imaging Workup and Diagnostic Algorithm
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fornalski, S.; Gupta, R.; Lee, T.Q. Anatomy and Biomechanics of the Elbow Joint. Tech. Hand Up. Extrem. Surg. 2003, 7, 168–178. [Google Scholar] [CrossRef] [Green Version]
- Masci, G.; Cazzato, G.; Milano, G.; Ciolli, G.; Malerba, G.; Perisano, C.; Greco, T.; Osvaldo, P.; Maccauro, G.; Liuzza, F. The Stiff Elbow: Current Concepts. Orthop. Rev. 2020, 12, 8661. [Google Scholar] [CrossRef] [PubMed]
- Adolfsson, L. Post-Traumatic Stiff Elbow. EFORT Open Rev. 2018, 3, 210–216. [Google Scholar] [CrossRef]
- Morrey, B.F. The Posttraumatic Stiff Elbow. Clin. Orthop. 2005, 431, 26–35. [Google Scholar]
- Lenoir, H.; Carlier, Y.; Ferrand, M.; Vidil, A.; Desmoineaux, P. Can Preoperative Imaging Predict the Outcomes after Arthroscopic Release for Elbow Arthritis? Orthop. Traumatol. Surg. Res. 2019, 105, S229–S234. [Google Scholar] [CrossRef] [PubMed]
- Patiño, J.M.; Saenz, V.P. Stiff Elbow. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Gauger, E.M.; Rhee, P.C. Surgical Management of the Posttraumatic Stiff Elbow: A Step-Wise Algorithm for Open Osteocapsular Release. Tech. Hand Up. Extrem. Surg. 2018, 22, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Kodde, I.F.; van Rijn, J.; van den Bekerom, M.P.J.; Eygendaal, D. Surgical Treatment of Post-Traumatic Elbow Stiffness: A Systematic Review. J. Shoulder Elb. Surg. 2013, 22, 574–580. [Google Scholar] [CrossRef]
- Pederzini, L.A.; Nicoletta, F.; Tosi, M.; Prandini, M.; Tripoli, E.; Cossio, A. Elbow Arthroscopy in Stiff Elbow. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 467–473. [Google Scholar] [CrossRef]
- Morrey, B.F.; Askew, L.J.; Chao, E.Y. A Biomechanical Study of Normal Functional Elbow Motion. J. Bone Joint Surg. Am. 1981, 63, 872–877. [Google Scholar] [CrossRef]
- Sardelli, M.; Tashjian, R.Z.; MacWilliams, B.A. Functional Elbow Range of Motion for Contemporary Tasks. J. Bone Joint Surg. Am. 2011, 93, 471–477. [Google Scholar] [CrossRef]
- Qian, Y.; Yu, S.; Shi, Y.; Huang, H.; Fan, C. Risk Factors for the Occurrence and Progression of Posttraumatic Elbow Stiffness: A Case-Control Study of 688 Cases. Front. Med. 2020, 7, 604056. [Google Scholar] [CrossRef]
- Sun, Z.; Li, J.; Cui, H.; Ruan, H.; Wang, W.; Fan, C. A New Pathologic Classification for Elbow Stiffness Based on Our Experience in 216 Patients. J. Shoulder Elb. Surg. 2020, 29, e75–e86. [Google Scholar] [CrossRef]
- Manske, M.C.; Hanel, D.P. Postburn Contractures of the Elbow and Heterotopic Ossification. Hand Clin. 2017, 33, 375–388. [Google Scholar] [CrossRef]
- Nandi, S.; Maschke, S.; Evans, P.J.; Lawton, J.N. The Stiff Elbow. HAND 2009, 4, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R. Posttraumatic Stiff Elbow. Indian J. Orthop. 2017, 51, 4–13. [Google Scholar] [CrossRef]
- Freibott, C.E.; Bäcker, H.C.; Shoap, S.C.; Tedesco, L.J.; Galle, S.E.; Rosenwasser, M.P. Treatment Methods for Post-Traumatic Elbow Stiffness Caused by Heterotopic Ossification. J. Shoulder Elb. Surg. 2020, 29, 1380–1386. [Google Scholar] [CrossRef]
- Papatheodorou, L.K.; Baratz, M.E.; Sotereanos, D.G. Elbow Arthritis: Current Concepts. J. Hand Surg. 2013, 38, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Guitton, T.G.; Zurakowski, D.; van Dijk, N.C.; Ring, D. Incidence and Risk Factors for the Development of Radiographic Arthrosis after Traumatic Elbow Injuries. J. Hand Surg. 2010, 35, 1976–1980. [Google Scholar]
- D’Ambrosi, R.; Formiconi, F.; Ursino, N.; Rubino, M. Treatment of Complete Ankylosed Elbow with Total Arthroplasty. BMJ Case Rep. 2019, 12, e231123. [Google Scholar] [CrossRef] [PubMed]
- Schaeffeler, C.; Waldt, S.; Woertler, K. Traumatic Instability of the Elbow—Anatomy, Pathomechanisms and Presentation on Imaging. Eur. Radiol. 2013, 23, 2582–2593. [Google Scholar] [PubMed]
- Klauser, A.S.; Tagliafico, A.; Allen, G.M.; Boutry, N.; Campbell, R.; Court-Payen, M.; Grainger, A.; Guerini, H.; McNally, E.; O’Connor, P.J.; et al. Clinical Indications for Musculoskeletal Ultrasound: A Delphi-Based Consensus Paper of the European Society of Musculoskeletal Radiology. Eur. Radiol. 2012, 22, 1140–1148. [Google Scholar] [CrossRef]
- Brandão, A.T.; Amaro, E.; Francisco, M.J.; Tanaka, R.M.; Santos, D.D.C.B.; Miranda, F.C.; Rahal, A.; Rosemberg, L.A. Ultrasonography and Magnetic Resonance Imaging of Elbow Ligaments: A Comparative Study. Einstein São Paulo 2019, 17, eAO4579. [Google Scholar] [CrossRef] [Green Version]
- Zubler, V.; Saupe, N.; Jost, B.; Pfirrmann, C.W.A.; Hodler, J.; Zanetti, M. Elbow Stiffness: Effectiveness of Conventional Radiography and CT to Explain Osseous Causes. AJR Am. J. Roentgenol. 2010, 194, W515–W520. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.-M.; Kim, H.; Sun, Y.; Kholinne, E.; Koh, K.H.; Jeon, I.-H. Arthroscopic Osteocapsular Arthroplasty for Advanced-Stage Primary Osteoarthritis of the Elbow Using a Computed Tomography–Based Classification. J. Shoulder Elb. Surg. 2020, 29, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Carlier, Y.; Lenoir, H.; Rouleau, D.M.; Mansat, P.; Vidil, A.; Ferrand, M.; Bleton, R.; Herrisson, O.; Salabi, V.; Duparc, F.; et al. Arthroscopic Debridement for Osteoarthritis of the Elbow: Results and Analysis of Predictive Factors. Orthop. Traumatol. Surg. Res. 2019, 105, S221–S227. [Google Scholar] [CrossRef] [PubMed]
- Everding, N.G.; Maschke, S.D.; Hoyen, H.A.; Evans, P.J. Prevention and Treatment of Elbow Stiffness: A 5-Year Update. J. Hand Surg. 2013, 38, 2496–2507. [Google Scholar] [CrossRef]
- Goyal, N.; Luchetti, T.J.; Blank, A.T.; Cohen, M.S. Atraumatic, Progressive, and Painful Elbow Contracture From a Ganglion Cyst. J. Hand Surg. 2021, 46, 345.e1–e345.e3. [Google Scholar] [CrossRef] [PubMed]
- Abou Arab, W.; Rauch, A.; Chawki, M.B.; Dap, F.; Dautel, G.; Blum, A.; Gondim Teixeira, P.A. Scapholunate Instability: Improved Detection with Semi-Automated Kinematic CT Analysis during Stress Maneuvers. Eur. Radiol. 2018, 28, 4397–4406. [Google Scholar] [CrossRef]
- Athlani, L.; Rouizi, K.; Granero, J.; Hossu, G.; Blum, A.; Dautel, G.; Gondim Teixeira, P.A. Assessment of Scapholunate Instability with Dynamic Computed Tomography. J. Hand Surg. Eur. Vol. 2020, 45, 375–382. [Google Scholar] [CrossRef]
- Gondim Teixeira, P.A.; Formery, A.-S.; Balazuc, G.; Lux, G.; Loiret, I.; Hossu, G.; Blum, A. Comparison between Subtalar Joint Quantitative Kinematic 4-D CT Parameters in Healthy Volunteers and Patients with Joint Stiffness or Chronic Ankle Instability: A Preliminary Study. Eur. J. Radiol. 2019, 114, 76–84. [Google Scholar] [CrossRef]
- Gondim Teixeira, P.A.; Formery, A.-S.; Jacquot, A.; Lux, G.; Loiret, I.; Perez, M.; Blum, A. Quantitative Analysis of Subtalar Joint Motion With 4D CT: Proof of Concept With Cadaveric and Healthy Subject Evaluation. AJR Am. J. Roentgenol. 2017, 208, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.A.G.; Gervaise, A.; Louis, M.; Raymond, A.; Formery, A.-S.; Lecocq, S.; Blum, A. Musculoskeletal Wide-Detector CT Kinematic Evaluation: From Motion to Image. Semin. Musculoskelet. Radiol. 2015, 19, 456–462. [Google Scholar] [PubMed]
- Teixeira, P.A.G.; Blanc, J.-B.; Rauch, A.; Arab, W.A.; Hossu, G.; Athlani, L.; Blum, A. Evaluation of Dorsal Subluxation of the Scaphoid in Patients with Scapholunate Ligament Tears: A 4D CT Study. AJR Am. J. Roentgenol. 2020, 216, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Blum, A.; Gillet, R.; Rauch, A.; Urbaneja, A.; Biouichi, H.; Dodin, G.; Germain, E.; Lombard, C.; Jaquet, P.; Louis, M.; et al. 3D Reconstructions, 4D Imaging and Postprocessing with CT in Musculoskeletal Disorders: Past, Present and Future. Diagn. Interv. Imaging 2020, 100, 693–705. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Extension Dysfunction | |
|---|---|
| Anterior Tether | Posterior Block |
| Thickened anterior capsule | Entrapped synovium |
| Contracture or HO of the anterior band of the medial collateral ligament | Osteophytes of the olecranon process or fossa |
| Contracture or HO of the flexor muscle/tendon | Loose bodies in the olecranon fossa |
| Anterior scarred skin | Posterior elbow ho |
| Posterior articular osteochondral lesion | |
| Flexion Dysfunction | |
| Posterior Tether | Anterior Block |
| Thickened posterior capsule | Entrapped synovium |
| Contracture or HO of the posterior band of the medial collateral ligament | Osteophytes of the coronoid process or fossa |
| Triceps contracture or HO | Loose bodies in the coronoid fossa |
| Posterior scarred skin | Anterior elbow ho |
| Anterior articular osteochondral lesion | |
| Items to be Checked on Radiographs | |
|---|---|
| Anteroposterior view | Profile |
| Malunion | Malunion |
| Malalignment in the frontal plane | Malalignment |
| Loose bodies | Loose bodies (olecranon and coronoid fossae) |
| Joint space narrowing | Radial head subluxation or dislocation |
| Periarticular calcification | Drop sign * (instability?) |
| Heterotopic ossification | Heterotopic ossification |
| Osteophytes (radial head) | Capsular ossification (anterior +++) |
| Osteophytes (olecranon and coronoid +++) | |
| Olecranon, coronoid, or radial fossae osteophytic filling | |
| Ulnar neuropathy +++ |
| Heterotopic ossification vasculonervous relations, if present |
| Cartilaginous lesions |
| Joint effusion and synovitis |
| Loose bodies (and their mobility) |
| Ligamentous pathology in case of instability |
| Osteophytes’ location |
| Loss of flexion | CT/CT-Arthrography |
| Posterior tethers/anterior blocks | |
| HO | |
| Anterior synovitis | |
| Loose bodies | |
| Osteophytes/fibrosis in the radial or coronoid fossa | |
| Osteophytes around the coronoid | |
| Joint space narrowing | |
| Loss of extension | CT/CT-Arthrography |
| Posterior blocks/anterior tethers | |
| HO | |
| Posterior synovitis | |
| Free bodies | |
| Osteophytes/fibrosis in the olecranon fossa | |
| Osteophytes around the olecranon | |
| Joint space narrowing | |
| Forearm rotation dysfunction | CT |
| Proximal radioulnar bony ankylosis | |
| Malunion or nonunion of the radial head | |
| Posttraumatic sequelae of the radial head | |
| Any stiffness | CT-Arthrography |
| Humeroulnar joint cartilaginous lesion (absent/mild/moderate/severe) | |
| Humeroradial joint cartilaginous lesion (absent/mild/moderate/severe) |
| Loss of Flexion |
|---|
| Anterior tethers/posterior blocks |
| Capsular scarring (lateral and medial ligament complex) |
| Brachialis scar |
| HO |
| Anterior synovitis (consider IV contrast media if needed) |
| Loose bodies |
| Osteophytes in the radial or coronoid fossa |
| Osteophytes around the coronoid |
| Joint space narrowing |
| Loss of extension |
| Posterior blocks/anterior tethers |
| Capsular scarring (lateral and medial ligament complex) |
| Triceps scar |
| HO |
| Posterior synovitis |
| Loose bodies |
| Osteophytes in the olecranon fossa |
| Osteophytes around the olecranon |
| Joint space narrowing |
| Forearm rotation dysfunction |
| Not initially indicated |
| Chondropathy of the radial head |
| Annular ligament scar |
| Radioulnar synostosis |
| Any stiffness |
| Humeroulnar joint impingement (absent/partial/severe) |
| Humeroradial joint impingement (absent/partial/severe) |
| Soft tissue lesion |
| Ulnar nerve injury |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombard, C.; Teixeira, P.; Germain, E.; Dodin, G.; Louis, M.; Blum, A.; Gillet, R. Elbow Stiffness Imaging: A Practical Diagnostic and Pretherapeutic Approach. J. Clin. Med. 2021, 10, 5348. https://doi.org/10.3390/jcm10225348
Lombard C, Teixeira P, Germain E, Dodin G, Louis M, Blum A, Gillet R. Elbow Stiffness Imaging: A Practical Diagnostic and Pretherapeutic Approach. Journal of Clinical Medicine. 2021; 10(22):5348. https://doi.org/10.3390/jcm10225348
Chicago/Turabian StyleLombard, Charles, Pedro Teixeira, Edouard Germain, Gauthier Dodin, Mathias Louis, Alain Blum, and Romain Gillet. 2021. "Elbow Stiffness Imaging: A Practical Diagnostic and Pretherapeutic Approach" Journal of Clinical Medicine 10, no. 22: 5348. https://doi.org/10.3390/jcm10225348