
Long-Term Safety and Efficacy of Subcutaneous Cladribine Used in Increased Dosage in Patients with Relapsing Multiple Sclerosis: 20-Year Observational Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Treatments
2.3. Assessments
2.4. Data Analysis and Statistics
3. Results
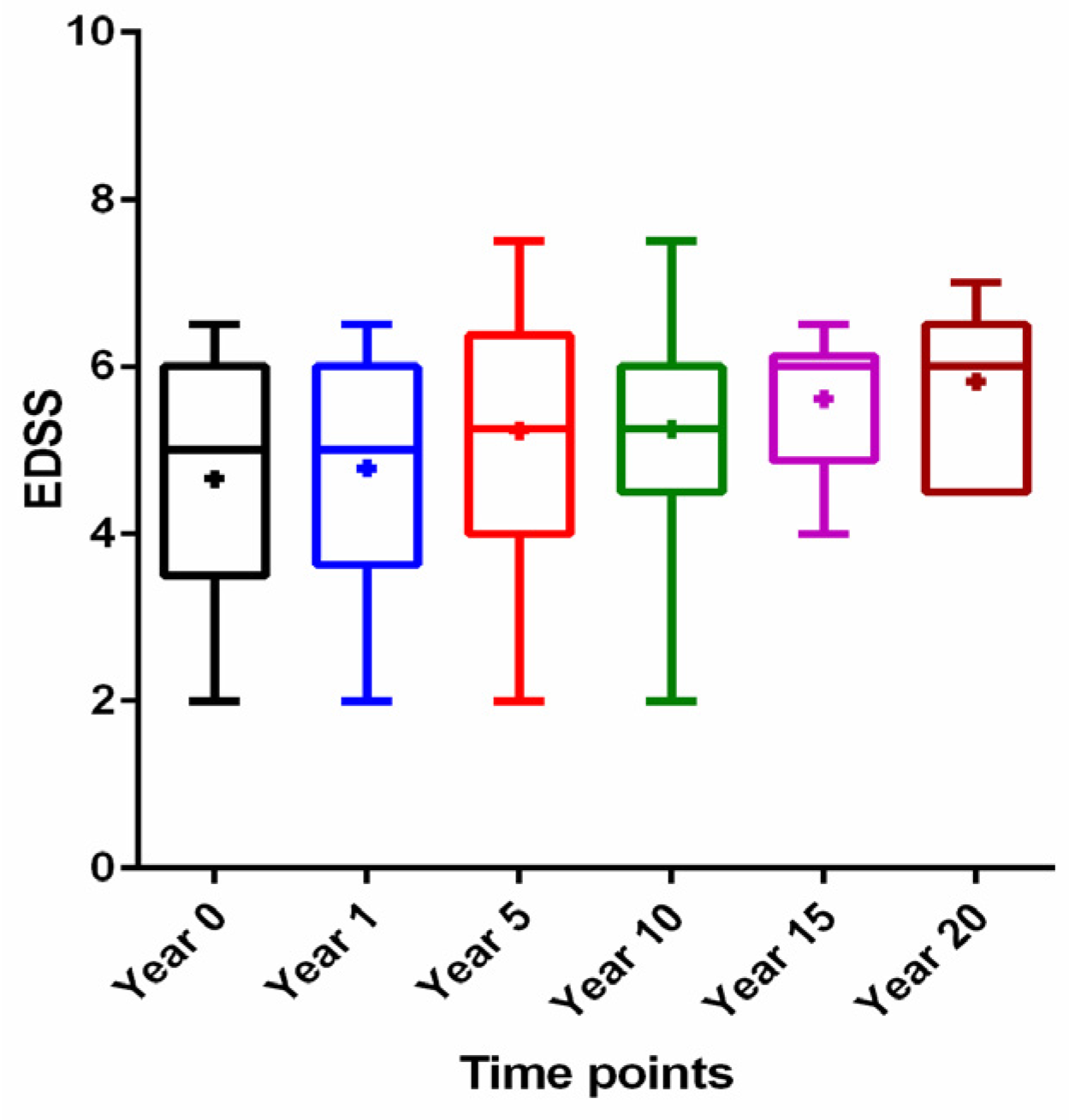
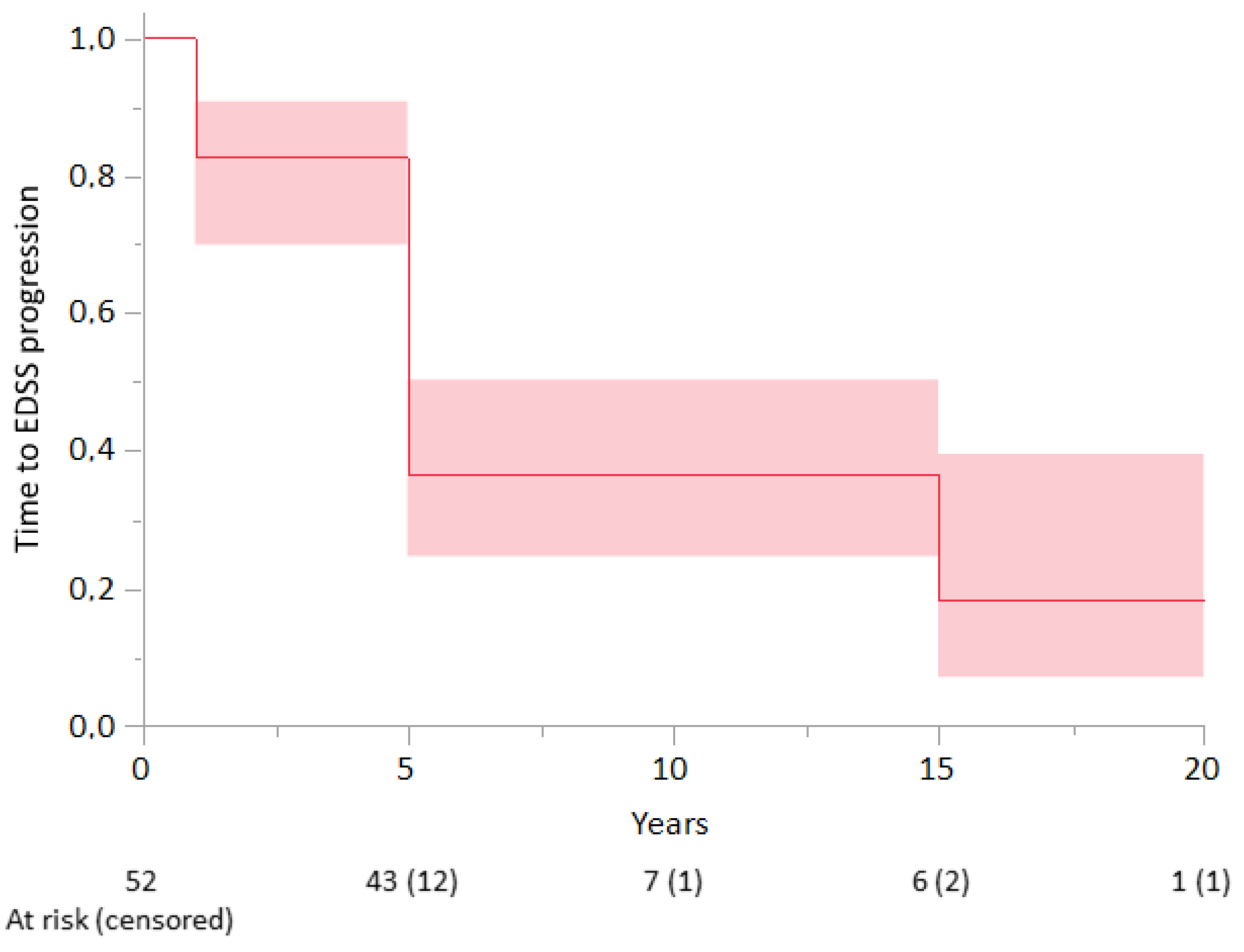
3.1. Efficacy
Progression Analysis
3.2. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cree, B.A.C.; Mares, J.; Hartung, H.P. Current therapeutic landscape in multiple sclerosis: An evolving treatment paradigm. Curr. Opin. Neurol. 2019, 32, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Rammohan, K.; Coyle, P.K.; Sylvester, E.; Galazka, A.; Dangond, F.; Grosso, M.; Leist, T.P. The Development of Cladribine Tablets for the Treatment of Multiple Sclerosis: A Comprehensive Review. Drugs 2020, 80, 1901–1928. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.; Pryce, G.; Herrod, S.S.; Schmierer, K. Potential mechanisms of action related to the efficacy and safety of cladribine. Mult. Scler. Relat. Disord. 2019, 30, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Grieb, P.; Ryba, M.; Stelmasiak, Z.; Nowicki, J.; Solski, J.; Jakubowska, B. Cladribine treatment of multiple sclerosis. Lancet 1994, 344, 538. [Google Scholar] [PubMed]
- Grieb, P.; Stelmasiak, Z.; Solski, J.; Nowicki, J.; Jakubowska, B.; Ryba, M. Effect of repeated treatments with cladribine (2-chlorodeoxyadenosine) on blood counts in multiple sclerosis patients. Arch. Immunol. Ther. Exp. 1995, 43, 323–327. [Google Scholar]
- Sipe, J.C.; Romine, J.S.; Koziol, J.A.; McMillan, R.; Beutler, E.; Sipe, J.C.; Romine, J.S.; Zyroff, J. Cladribine in treatment of chronic progressive multiple sclerosis. Lancet 1994, 344, 9–13. [Google Scholar] [CrossRef]
- Giovannoni, G.; Comi, G.; Cook, S.; Rammohan, K.; Rieckmann, P.; Sørensen, P.S.; Vermersch, P.; Chang, P.; Hamlett, A.; Musch, B.; et al. A Placebo-Controlled Trial of Oral Cladribine for Relapsing Multiple Sclerosis. N. Engl. J. Med. 2010, 362, 416–426. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, P.S.; Centonze, D.; Giovannoni, G.; Montalban, X.; Selchen, D.; Vermersch, P.; Wiendl, H.; Yamout, B.; Salloukh, H.; Rieckmann, P. Expert opinion on the use of cladribine tablets in clinical practice. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420935019. [Google Scholar] [CrossRef]
- Lünemann, J.D.; Ruck, T.; Muraro, P.A.; Bar-Or, A.; Wiendl, H. Immune reconstitution therapies: Concepts for durable remission in multiple sclerosis. Nat. Rev. Neurol. 2020, 16, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Rejdak, K.; Stelmasiak, Z.; Grieb, P. Cladribine induces long lasting oligoclonal bands disappearance in relapsing multiple sclerosis patients: 10-year observational study. Mult. Scler. Relat. Disord. 2019, 27, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Stelmasiak, Z.; Solski, J.; Nowicki, J.; Jakubowska, B.; Ryba, M.; Grieb, P. Effect of parenteral cladribine on relapse rates in patients with relapsing forms of multiple sclerosis: Results of a 2-year, double-blind, placebo-controlled, crossover study. Mult. Scler. 2009, 15, 767–770. [Google Scholar] [CrossRef] [PubMed]
- McDonald, W.I.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.P.; Lublin, F.D.; McFarland, H.F.; Paty, D.W.; Polman, C.H.; Reingold, S.C.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Liliemark, J.; Albertioni, F.; Hassan, M.; Juliusson, G. On the bioavailability of oral and subcutaneous 2-chloro-2′-deoxyadenosine in humans: Alternative routes of administration. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1992, 10, 1514–1518. [Google Scholar] [CrossRef] [PubMed]
- Stelmasiak, Z.; Solski, J.; Nowicki, J.; Porebska-Piwowarczyk, E.; Jakubowska, B.; Ryba, M.S.; Grieb, P. A pilot trial of cladribine (2-chlorodeoxyadenosine) in remitting- relapsing multiple sclerosis. Med. Sci. Monit. 1998, 4, 4–8. [Google Scholar]
- Giovannoni, G.; Cook, S.; Rammohan, K.; Rieckmann, P.; Sørensen, P.S.; Vermersch, P.; Hamlett, A.; Viglietta, V.; Greenberg, S. Sustained disease-activity-free status in patients with relapsing-remitting multiple sclerosis treated with cladribine tablets in the CLARITY study: A post-hoc and subgroup analysis. Lancet Neurol. 2011, 10, 329–337. [Google Scholar] [CrossRef]
- Magyari, M.; Sorensen, P.S. Comorbidity in Multiple Sclerosis. Front. Neurol. 2020, 11, 851. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Leist, T.; Comi, G.; Montalban, X.; Giovannoni, G.; Nolting, A.; Hicking, C.; Galazka, A.; Sylvester, E. Safety of cladribine tablets in the treatment of patients with multiple sclerosis: An integrated analysis. Mult. Scler. Relat. Disord. 2019, 29, 157–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leist, T.; Cook, S.; Comi, G.; Montalban, X.; Giovannoni, G.; Nolting, A.; Damian, D.; Syed, S.; Galazka, A. Long-term safety data from the cladribine tablets clinical development program in multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 46, 102572. [Google Scholar] [CrossRef] [PubMed]
- GLOBOCAN. Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012 v1.0. Available online: https://publications.iarc.fr/Databases/Iarc-Cancerbases/GLOBOCAN-2012-Estimated-Cancer-Incidence-Mortality-And-Prevalence-Worldwide-In-2012-V1.0-2012 (accessed on 26 July 2021).



{kind=link}
{kind=link}
| Baseline Characteristics | Total (n = 52) | 5 Years (n = 26) | 10 Years (n = 8) | 15 Years (n = 7) | 20 Years (n = 11) | p-Value |
|---|---|---|---|---|---|---|
| Gender (female/male) | 37/15 | 18/8 | 6/2 | 5/2 | 8/3 | >0.05 |
| Age at MS onset, years (mean ± SD) | 30.9 ± 8.2 | 32.2 ± 9.8 | 28.4 ± 5.4 | 31.5 ± 6.7 | 29.4 ± 6.1 | >0.05 |
| Age at treatment initiation, years (mean ± SD) | 39.2 ± 8.6 | 44.2 ± 8.9 | 34.0 ± 3.8 | 33.5 ± 6.7 | 34.3 ± 4.6 | >0.05 |
| Cladribine (s.c.) cumulative dose at final follow-up (mg/kg body weight; mean ± SD) | 2.6 ± 1.1 | 2.1 ± 0.4 | 2.7 ± 1.4 | 2.7 ± 1.3 | 3.8 ± 1.4 | <0.001 * |
| EDSS score at treatment initiation (mean ± SD) | 4.7 ± 1.4 | 5.5 ± 1.1 | 4.3 ± 1.6 | 3.9 ± 1.2 | 3.6 ± 1.0 | <0.001 ** |
| Prior treatment (n (%)) | 5 (10) | |||||
| Interferon beta-1a | 1 (2) | 1 (12) | ||||
| Interferon beta-1b | 3 (6) | 3 (12) | ||||
| Glatiramer acetate | 1 (2) | 1 (4) | ||||
| Comorbidities (n (%)) | 11 (21) | |||||
| Hypertension | 2 (4) | 2 (7) | ||||
| Dyslipidemia | 2 (4) | 1 (4) | 1 (9) | |||
| Paroxysmal atrial fibrillation | 1 (2) | 1 (4) | - | |||
| Bradycardia (transient) | 1 (2) | 1 (9) | ||||
| Fatty liver disease | 1 (2) | 1 (9) | ||||
| Microcytic anemia | 1 (2) | 1 (4) | ||||
| Pulmonary emphysema | 1 (2) | 1 (12) | ||||
| Thyroid nodules | 1 (2) | 1 (4) | ||||
| Hypothyroidism | 1 (2) | 1 (12) | ||||
| Appendicitis (with appendectomy) | 1 (2) | 1 (9) | ||||
| Nephrolithiasis | 1 (2) | 1 (9) | ||||
| Baseline Characteristics | 5 Years (n = 52) | 10 Years (n = 26) | 15 Years (n = 18) | 20 Years (n = 11) | p-Value |
|---|---|---|---|---|---|
| Gender (female/male) | 37/15 | 19/7 | 13/5 | 8/3 | >0.05 |
| Cladribine (s.c.) cumulative dose at time point (mg/kg body weight; mean ± SD) | 2.1 ± 0.4 | 2.5 ± 1.0 | 2.7 ± 1.1 | 3.8 ± 1.4 | <0.001 * |
| Age at treatment initiation (mean ± SD) | 39.5 ± 8.8 | 34.8 ± 5.9 | 35.2 ± 6.7 | 34.2 ± 4.6 | 0.02 ** |
| Disease duration to treatment initiation (mean ± SD) | 9.0 ± 8.6 | 5.5 ± 5.1 | 5.5 ± 5.4 | 5.1 ± 5.0 | >0.05 |
| EDSS score at treatment initiation (mean ± SD) | 4.6 ± 1.4 | 3.8 ± 1.2 | 3.6 ± 1.0 | 3.4 ± 1.0 | 0.002 *** |
| Variable | Univariate Cox Regression | Multivariate Cox Regression | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Gender (male vs. female) | 1.28 (0.62; 2.63) | 0.5162 | 1.47 (0.69; 3.13) | 0.3223 |
| Disease duration to treatment initiation, years | 0.97 (0.92; 1.01) | 0.1428 | 0.96 (0.91; 1.02) | 0.1585 |
| Age at treatment initiation, years | 0.99 (0.95; 1.03) | 0.4702 | 1.00 (0.96; 1.05) | 0.9584 |
| Cumulative s.c. cladribine dose, per 1 mg/kg body weight | 0.94 (0.69; 1.28) | 0.6916 | 0.93 (0.68; 1.28) | 0.6556 |
| Baseline Characteristics | Non-Progressive (n = 16) | Progressive (n = 36) | p-Value |
|---|---|---|---|
| Gender (female/male) | 12/4 | 25/11 | >0.05 |
| Age at treatment initiation, years (mean ± SD) | 42.8 ± 9.1 | 38.9 ± 8.4 | >0.05 |
| Disease duration to treatment initiation, years (mean ± SD) | 10.1 ± 5.8 | 11.1 ± 6.0 | >0.05 |
| Cladribine (s.c.) cumulative dose at year 5 (mg/kg body weight; mean ± SD) | 2.3 ± 0.6 | 1.9 ± 0.4 | 0.02 |
| EDSS score at cladribine initiation (mean ± SD) | 4.2 ± 1.2 | 5.5 ± 1.4 | 0.03 |
| Baseline Characteristics | Non-Progressive (n = 5) | Progressive (n = 21) | p-Value |
|---|---|---|---|
| Gender (female/male) | 5/0 | 14/7 | >0.05 |
| Age at treatment initiation, years (mean ± SD) | 32.8 ± 2.6 | 35.3 ± 6.4 | >0.05 |
| Disease duration to treatment initiation, years (mean ± SD) | 8.1 ± 3.8 | 9.1 ± 2.1 | >0.05 |
| Cladribine (s.c.) cumulative dose at year 10 (mg/kg body weight; mean ± SD) | 3.2 ± 1.0 | 2.3 ± 1.0 | 0.01 |
| EDSS score at cladribine initiation (mean ± SD) | 4.2 ± 1.4 | 3.7 ± 1.2 | 0.05 |
| Medical History Diagnosed after s.c. Cladribine Treatment Initiation (n (%)) | Year 5 (n = 15) | Year 10 (n = 8) | Year 15 (n = 7) | Year 20 (n = 11) |
|---|---|---|---|---|
| Appendicitis (with appendectomy) | 1 (9.1) | |||
| Atrial fibrillation (paroxysmal) | 1 (6.7) | |||
| Bradycardia (transient) | 1 (9.1) | |||
| Breast cancer | 1 (12.5) | |||
| Cataract | 1 (6.7) | 1 (9.1) | ||
| Cervical cancer (preinvasive, Grade 0) | 1 (9.1) | |||
| Cholecystolithiasis | 2 (13.3) | 1 (14.3) | ||
| Diabetes type 2 | 1 (6.7) | 1 (14.3) | 1 (9.1) | |
| Dyslipidemia | 3 (20.0) | 1 (12.5) | 1 (14.3) | 3 (27.3) |
| Fatty liver disease (non-alcoholic) | 1 (6.7) | 2 (18.2) | ||
| Hypertension | 5 (33.3) | 1 (14.3) | 2 (18.2) | |
| Ischemic heart disease | 1 (6.7) | |||
| Kidney cysts | 1 (6.7) | |||
| Lumbosacral discogenic syndrome | 2 (18.2) | |||
| Lymphopenia (prolonged >1 month, reversible) | 1 (6.7) | 1 (12.5) | 2 (18.2) | |
| Microcytic anemia | 1 (6.7) | 1 (12.5) | ||
| Mood disorder | 1 (12.5) | |||
| Nephrolithiasis | 2 (18.2) | |||
| Osteoporosis | 1(12.5) | |||
| Ovarian cyst | 1 (9.1) | |||
| Peptic ulcer disease (with gastrectomy) | 1 (14.3) | |||
| Pulmonary emphysema | 1 (14.3) | |||
| Renal fibrosis | 1 (9.1) | |||
| Thyroid disorders * | 6 (40.0) | 2 (25.0) | ||
| Trigeminal neuralgia | 1 (9.1) | |||
| Tuberculosis | 1 (9.1) | |||
| Urinary tract infection (frequent) | 2 (13.3) | |||
| Uterine fibroids | 1 (12.5) | 1 (9.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rejdak, K.; Zasybska, A.; Pietruczuk, A.; Baranowski, D.; Szklener, S.; Kaczmarek, M.; Stelmasiak, Z. Long-Term Safety and Efficacy of Subcutaneous Cladribine Used in Increased Dosage in Patients with Relapsing Multiple Sclerosis: 20-Year Observational Study. J. Clin. Med. 2021, 10, 5207. https://doi.org/10.3390/jcm10215207
Rejdak K, Zasybska A, Pietruczuk A, Baranowski D, Szklener S, Kaczmarek M, Stelmasiak Z. Long-Term Safety and Efficacy of Subcutaneous Cladribine Used in Increased Dosage in Patients with Relapsing Multiple Sclerosis: 20-Year Observational Study. Journal of Clinical Medicine. 2021; 10(21):5207. https://doi.org/10.3390/jcm10215207
Chicago/Turabian StyleRejdak, Konrad, Adriana Zasybska, Aleksandra Pietruczuk, Dariusz Baranowski, Sebastian Szklener, Magda Kaczmarek, and Zbigniew Stelmasiak. 2021. "Long-Term Safety and Efficacy of Subcutaneous Cladribine Used in Increased Dosage in Patients with Relapsing Multiple Sclerosis: 20-Year Observational Study" Journal of Clinical Medicine 10, no. 21: 5207. https://doi.org/10.3390/jcm10215207