
Post-COVID-19 Sydrome and Decrease in Health-Related Quality of Life in Kidney Transplant Recipients after SARS-COV-2 Infection—A Cohort Longitudinal Study from the North of Poland

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
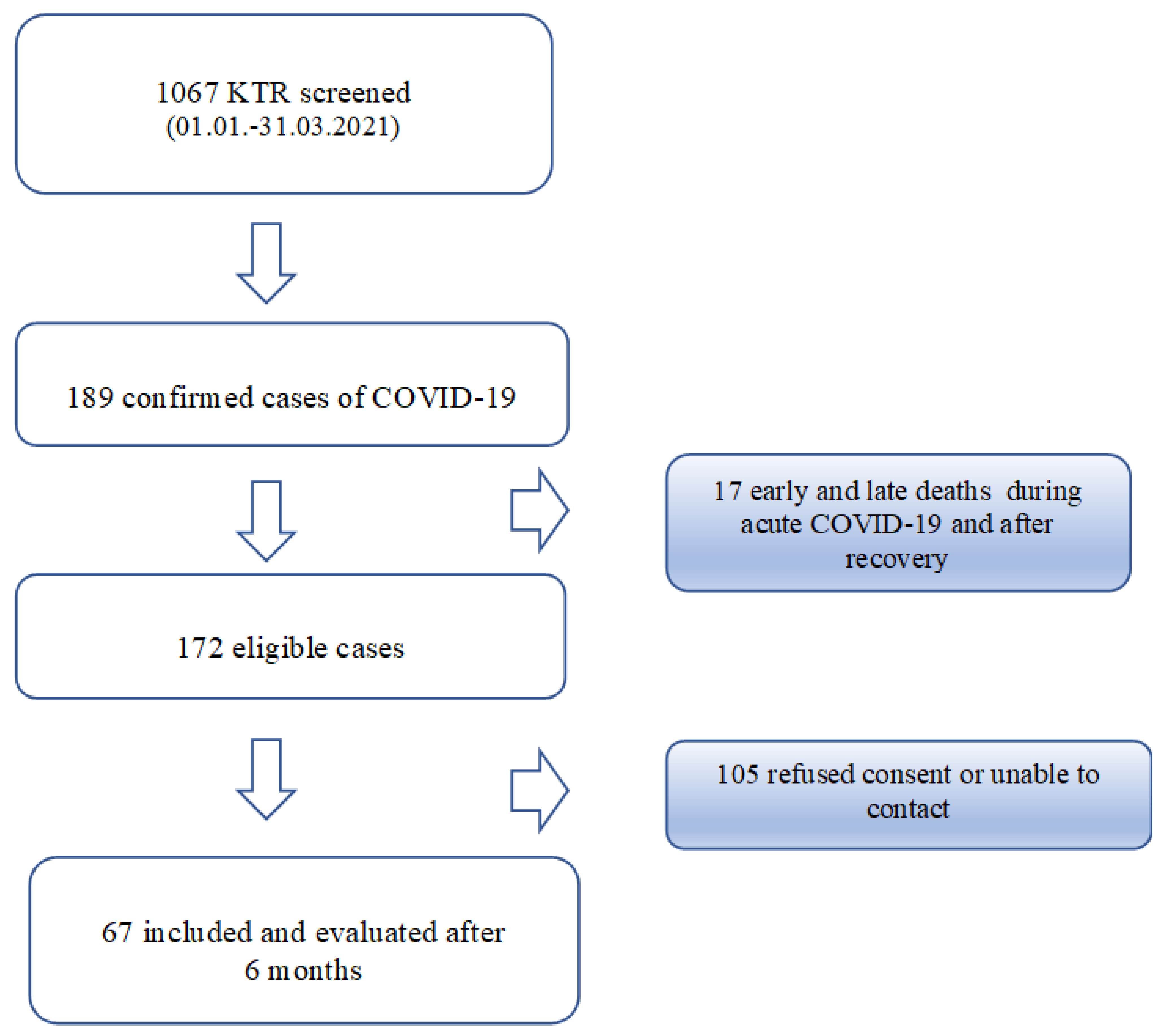
2.1. Design and Participants
2.2. Procedures and Questionaires
2.3. Statisitcs
3. Results
3.1. Patients
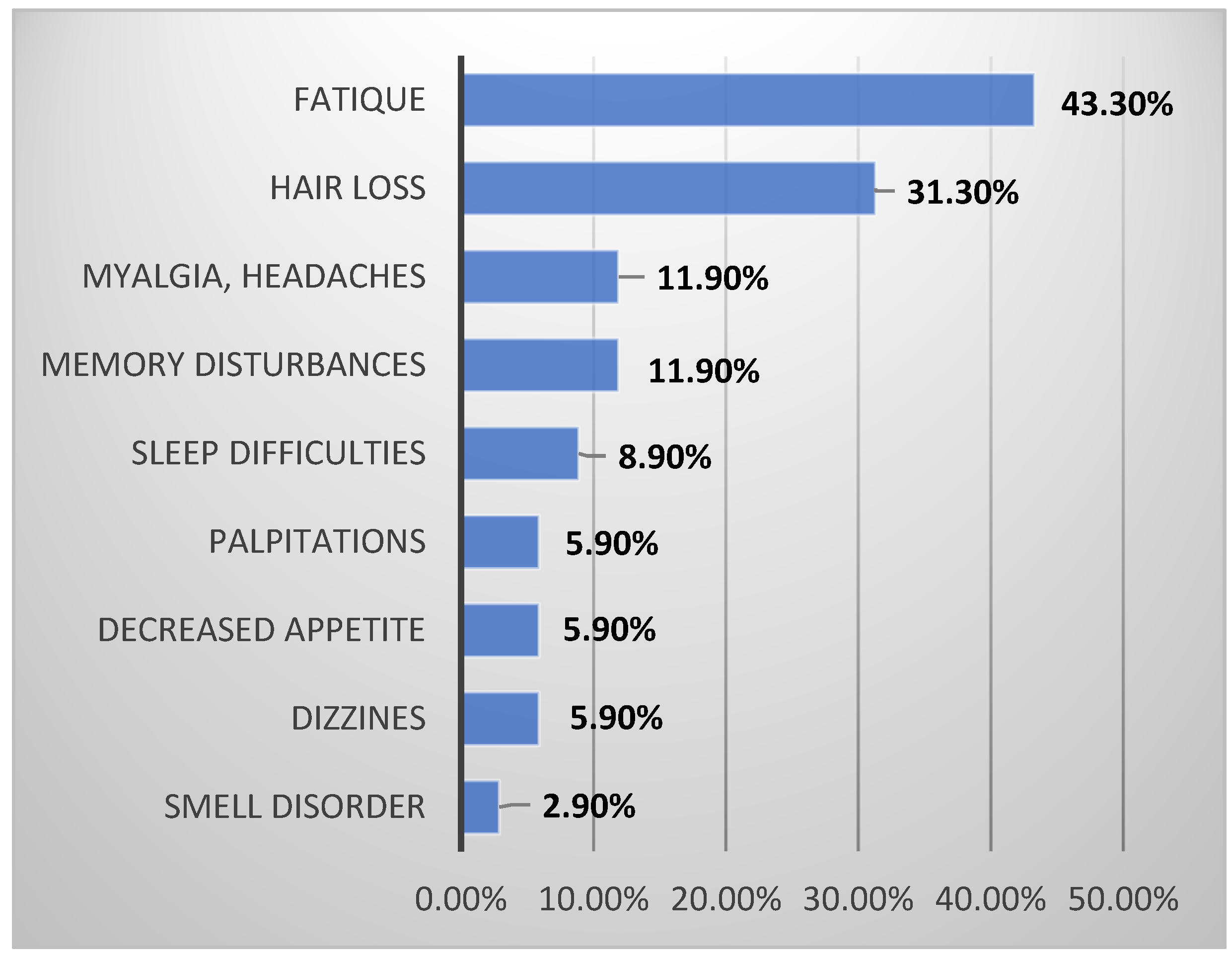
3.2. Self-Reported Symptoms (SRSQ)
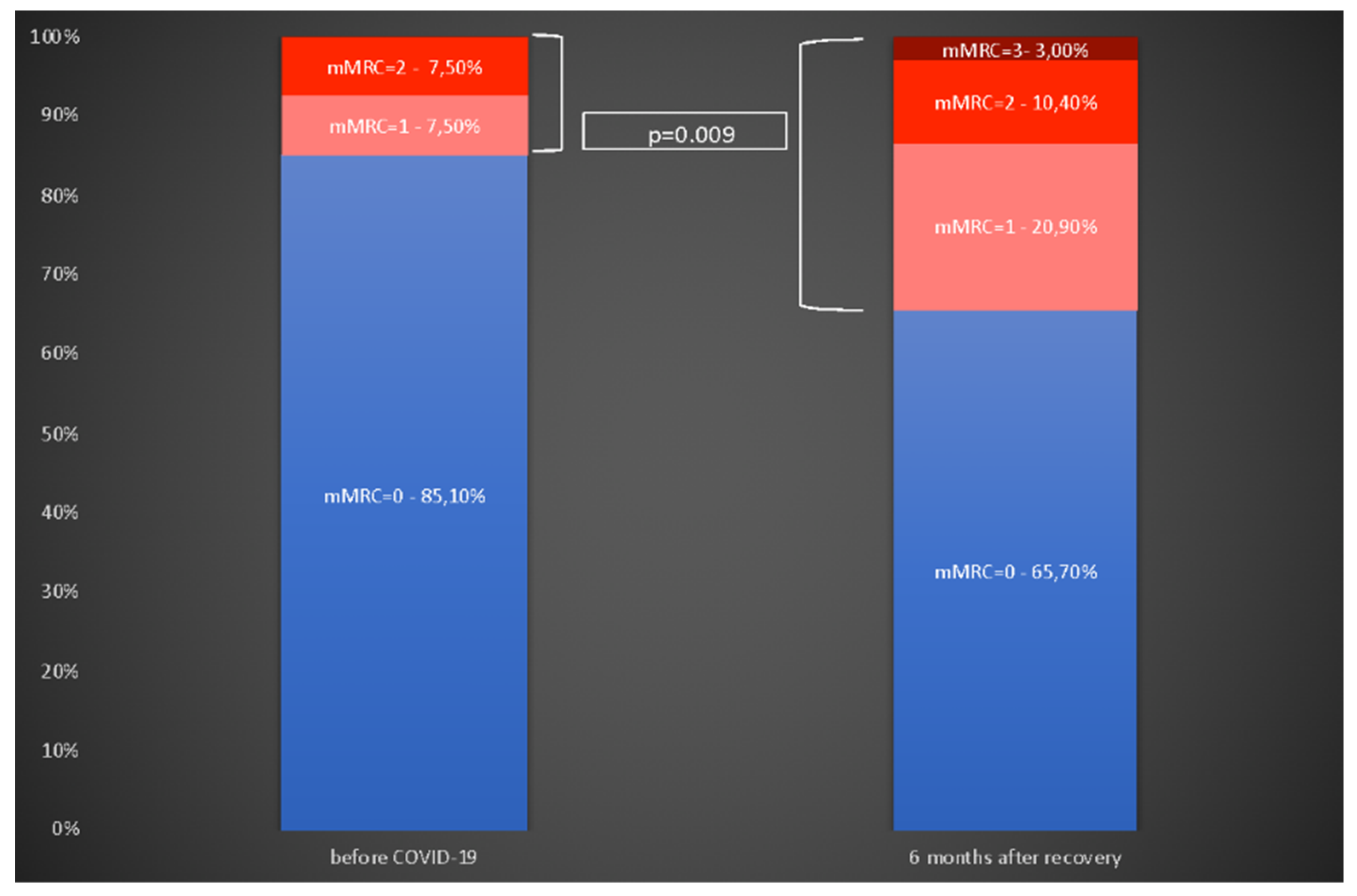
3.3. Self-Reported Dyspnea (mMRC)
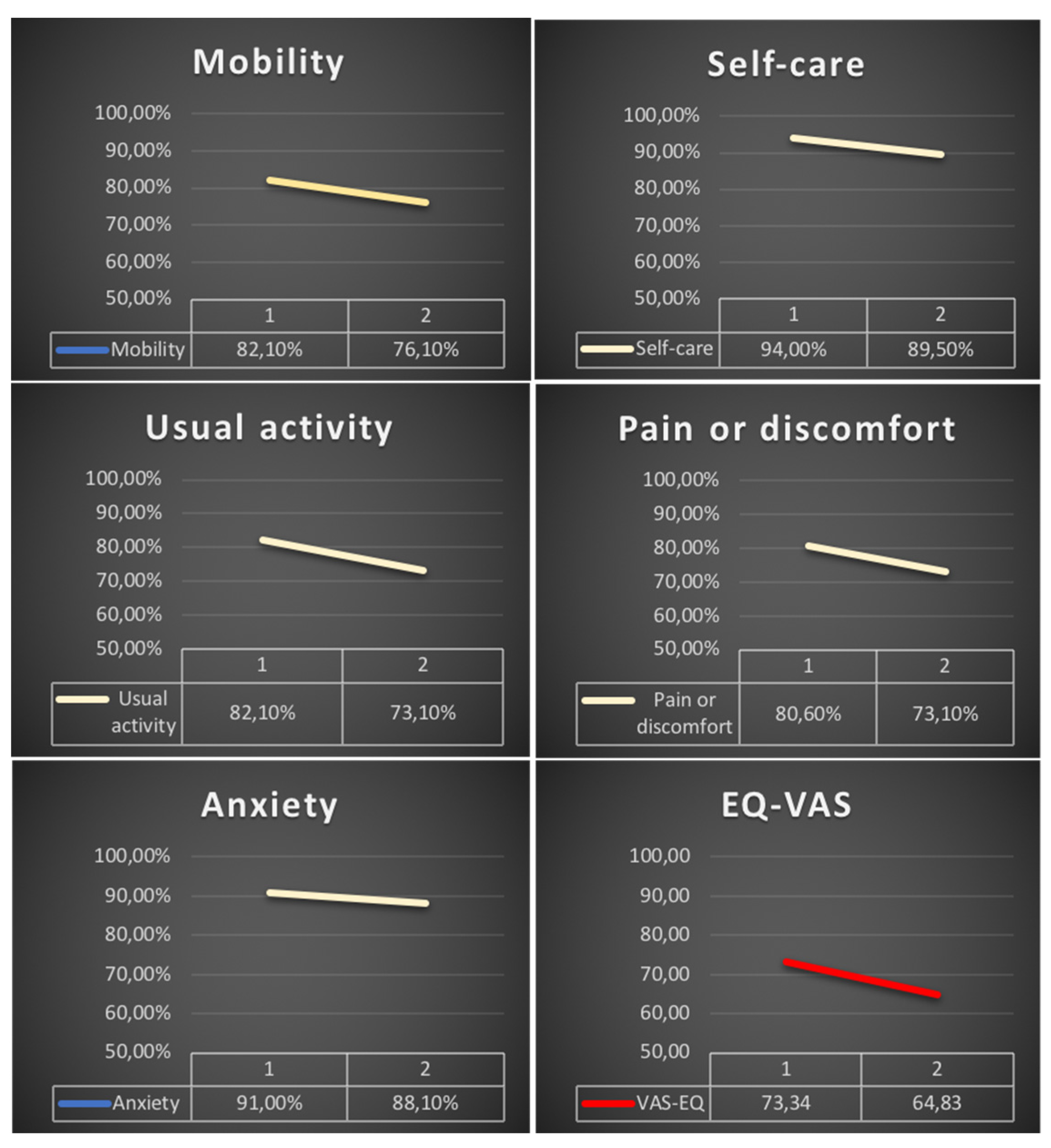
3.4. Health Related Quality of Life (EuroQoL)
3.5. Predictors of Post-COVID-19 Syndrome
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Ambardar, S.R.; Hightower, S.L.; Huprikar, N.A.; Chung, K.K.; Singhal, A.; Collen, J.F. Post-COVID-19 Pulmonary Fibrosis: Novel Sequelae of the Current Pandemic. J. Clin. Med. 2021, 10, 2452. [Google Scholar] [CrossRef] [PubMed]
- Och, A.; Tylicki, P.; Polewska, K.; Puchalska-Reglińska, E.; Parczewska, A.; Szabat, K.; Biedunkiewicz, B.; Debska Slizien, A.; Tylicki, L. Persistent post-COVID-19 syndrome in hemodialyzed patients—A longitudinal cohort study from the North of Poland. J. Clin. Med. 2021, 10, 4451. [Google Scholar] [CrossRef] [PubMed]
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmeh, L. Managing the long term effects of COVID-19: Summary of NICE, SIGN, and RCGP rapid guideline. BMJ 2021, 372, n136. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef]
- Azzi, Y.; Bartash, R.; Scalea, J.; Loarte-Campos, P.; Akalin, E. COVID-19 and Solid Organ Transplantation: A Review Article. Transplantation 2021, 105, 37–55. [Google Scholar] [CrossRef]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef]
- Basic-Jukic, N.; Juric, I.; Furic-Cunko, V.; Katalinic, L.; Radic, J.; Bosnjak, Z.; Jelakovic, B.; Kastelan, Z. Follow-up of renal transplant recipients after acute COVID-19-A prospective cohort single-center study. Immun. Inflamm. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Elec, A.D.; Oltean, M.; Goldis, P.; Cismaru, C.; Lupse, M.; Muntean, A.; Elec, F.I. COVID-19 after kidney transplantation: Early outcomes and renal function following antiviral treatment. Int. J. Infect. Dis. 2021, 104, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Debska-Slizien, A.; Slizien, Z.; Muchlado, M.; Kubanek, A.; Piotrowska, M.; Dabrowska, M.; Tarasewicz, A.; Chamienia, A.; Biedunkiewicz, B.; Renke, M.; et al. Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study-The COViNEPH Project. Vaccines 2021, 9, 1165. [Google Scholar] [CrossRef]
- Puchalska-Reglińska, E.; Debska-Slizien, A.; Biedunkiewicz, B.; Tylicki, P.; Polewska, K.; Rutkowski, B.; Gellert, R.; Tylicki, L. Extremely high mortality in COVID-19 hemodialyzed patients before the anti-SARS-CoV-2 vaccination era. Large database from the North of Poland. Pol. Arch. Intern. Med. 2021, 131, 643–648. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, S.; Meshram, H.S.; Kute, V.; Patel, H.; Desai, S.; Dave, R. Long-term follow-up of SARS-CoV-2 recovered renal transplant recipients: A single-center experience from India. Transpl. Infect. Dis. 2021, e13735. [Google Scholar] [CrossRef]
- Baig, A.M. Chronic COVID syndrome: Need for an appropriate medical terminology for long-COVID and COVID long-haulers. J. Med. Virol. 2021, 93, 2555–2556. [Google Scholar] [CrossRef]
- Carfi, A.; Bernabei, R.; Landi, F.; Gemelli Against, C.-P.-A.C.S.G. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Sykes, D.L.; Holdsworth, L.; Jawad, N.; Gunasekera, P.; Morice, A.H.; Crooks, M.G. Post-COVID-19 Symptom Burden: What is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Amin-Chowdhury, Z.; Harris, R.J.; Aiano, F.; MZavala, M.; Bertran, M.; Borrow, R.; Linley, E.; Ahmad, S.; Parker, B.; Horsley, A.; et al. Characterising post-COVID syndrome more than 6 months after acute infection in adults; prospective longitudinal cohort study, England. medRxiv 2021. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Tricot, L.; Lebbe, C.; Pillebout, E.; Martinez, F.; Legendre, C.; Thervet, E. Tacrolimus-induced alopecia in female kidney-pancreas transplant recipients. Transplantation 2005, 80, 1546–1549. [Google Scholar] [CrossRef] [PubMed]
- Mieczkowska, K.; Deutsch, A.; Borok, J.; Guzman, A.K.; Fruchter, R.; Patel, P.; Wind, O.; McLellan, B.N.; Mann, R.E.; Halverstam, C.P. Telogen effluvium: A sequela of COVID-19. Int. J. Dermatol. 2021, 60, 122–124. [Google Scholar] [CrossRef]
- Tielemans, M.M.; van Boekel, G.A.J.; van Gelder, T.; Tjwa, E.T.; Hilbrands, L.B. Immunosuppressive drugs and the gastrointestinal tract in renal transplant patients. Transplant. Rev. 2019, 33, 55–63. [Google Scholar] [CrossRef]
- Anand, S.; Montez-Rath, M.; Han, J.; Bozeman, J.; Kerschmann, R.; Beyer, P.; Parsonnet, J.; Chertow, G.M. Prevalence of SARS-CoV-2 antibodies in a large nationwide sample of patients on dialysis in the USA: A cross-sectional study. Lancet 2020, 396, 1335–1344. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-COVID syndrome in individuals admitted to hospital with COVID-19: Retrospective cohort study. BMJ 2021, 372, n693. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | 67 |
|---|---|
| Age years mean ± SD | 53.14 ± 14.0 |
| Male sex n (%) | 38 (56.7) |
| Charlson Comorbidity Index mean ± SD | 4.15 ± 2.26 |
| Fragility index mean ± SD | 3.25 ± 0.68 |
| Primary nephropathy n (%) | |
| Unknown | 13 (19.4) |
| Glomerulonephritis | 23 (34.3) |
| Diabetes nephropathy | 7 (10.4) |
| Hereditary nephropathies | 11 (16.4) |
| Transplantation vintage years mean ± SD | 7.3 ± 6.4 |
| Deceased donor n (%) | 61 (91.1) |
| Immunosuppression protocol n (%) | |
| TAC + MMF/MPS + steroids | 45 (67.2) |
| CYS + MMF/MPS + steroids | 21 (31.3) |
| Protocol without steroids | 5 (7.5) |
| Protocol without MMF/MPS | 16 (23.9) |
| SARS-COV-2 infection severity | |
| COVID-19 asymptomatic | 2 (3.0) |
| COVID-19 symptomatic without hospitalization | 28 (41.8) |
| COVID-19 symptomatic with hospitalization | 39 (58.2) |
| COVID-19 symptomatic with respiratory therapy | 0 (0.0) |
| Total duration of hospitalization due to COVID-19 days mean ± SD | 16.5 ± 9.54 |
| No Post COVID n = 20 | Post COVID n = 47 | p-Value | |
|---|---|---|---|
| Age years mean ± SD | 46.67 ± 16.7 | 57.02 ± 11.57 | p = 0.002 |
| Sex woman n (%) | 6 (30) | 22 (46.8) | ns |
| CCI mean ± SD | 3.09 ± 1.3 | 4.64 ± 2.43 | p = 0.006 |
| Transplant vintage years mean ± SD | 6.21 ± 6.63 | 7.76 ± 6.3 | ns |
| Serum creatinine mg/dl mean ± SD | 1.76 ± 0.92 | 1.73 ± 1.06 | ns |
| Hospitalization due to COVID-19 n (%) | 9 (45) | 31 (66) | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malinowska, A.; Muchlado, M.; Ślizień, Z.; Biedunkiewicz, B.; Heleniak, Z.; Dębska-Ślizień, A.; Tylicki, L. Post-COVID-19 Sydrome and Decrease in Health-Related Quality of Life in Kidney Transplant Recipients after SARS-COV-2 Infection—A Cohort Longitudinal Study from the North of Poland. J. Clin. Med. 2021, 10, 5205. https://doi.org/10.3390/jcm10215205
Malinowska A, Muchlado M, Ślizień Z, Biedunkiewicz B, Heleniak Z, Dębska-Ślizień A, Tylicki L. Post-COVID-19 Sydrome and Decrease in Health-Related Quality of Life in Kidney Transplant Recipients after SARS-COV-2 Infection—A Cohort Longitudinal Study from the North of Poland. Journal of Clinical Medicine. 2021; 10(21):5205. https://doi.org/10.3390/jcm10215205
Chicago/Turabian StyleMalinowska, Agnieszka, Marta Muchlado, Zuzanna Ślizień, Bogdan Biedunkiewicz, Zbigniew Heleniak, Alicja Dębska-Ślizień, and Leszek Tylicki. 2021. "Post-COVID-19 Sydrome and Decrease in Health-Related Quality of Life in Kidney Transplant Recipients after SARS-COV-2 Infection—A Cohort Longitudinal Study from the North of Poland" Journal of Clinical Medicine 10, no. 21: 5205. https://doi.org/10.3390/jcm10215205