
Differences in Sleep Disorders between HIV-Infected Persons and Matched Controls with Sleep Problems: A Matched-Cohort Study Based on Laboratory and Survey Data

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
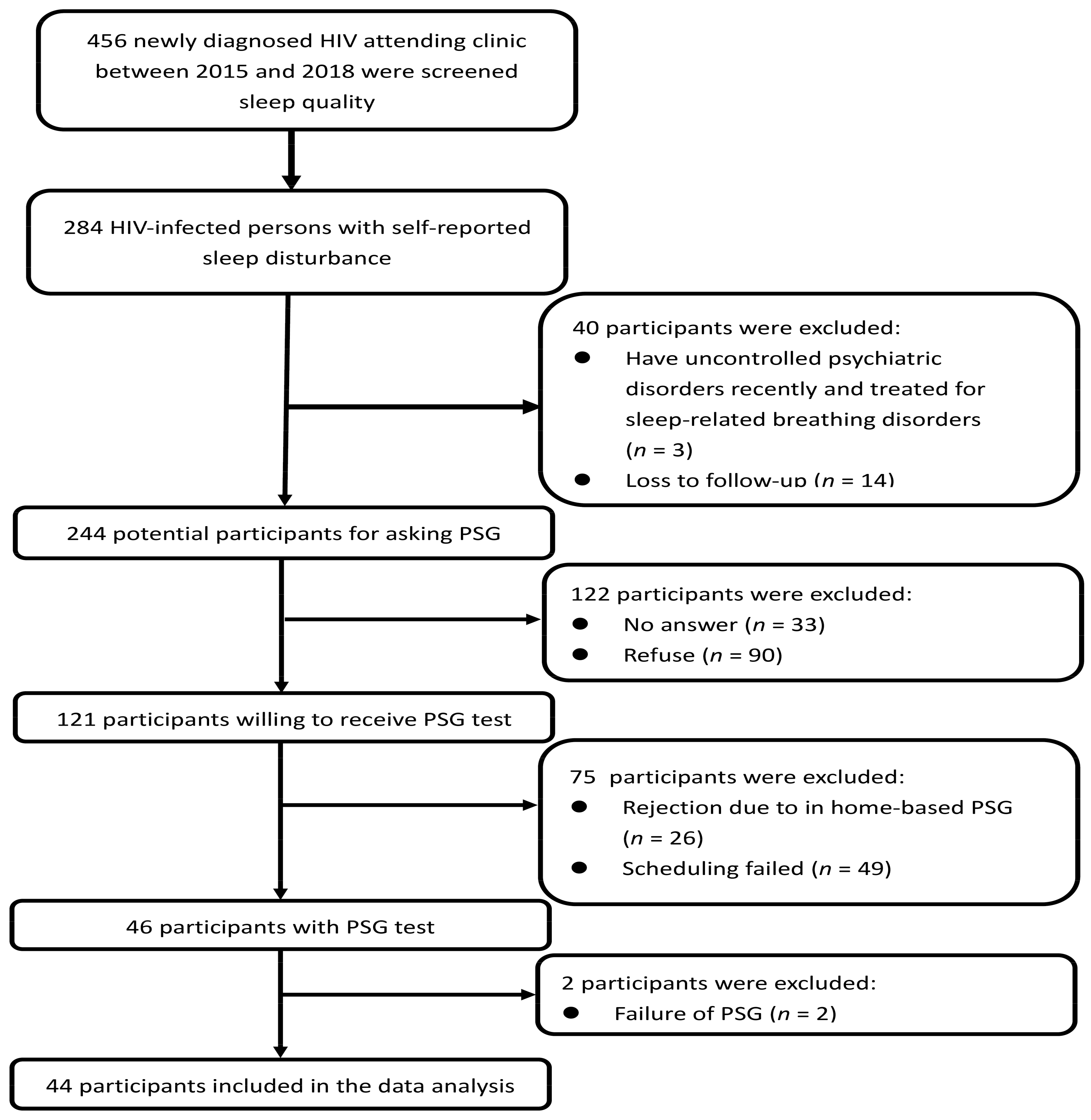
2.2. Study Participants
2.2.1. HIV-Infected Persons with Sleep Disturbances
2.2.2. Controls with Sleep Disturbances
2.3. Measures
2.3.1. Polysomnography Study
Sleep Architecture
- Sleep-disordered breathing:
- 2.
- Periodic limb movements
- 3.
- Suspected rapid eye movement behavior disorder
2.3.2. Questionnaire
Sleep-Related Physical Symptoms
Poor Sleep Quality
Psychological Disturbances
2.3.3. Clinical Data Collection
2.4. Data Analysis
3. Results
3.1. Demographics
3.2. Differences in Sleep Architecture
3.3. Types of Sleep Disorders
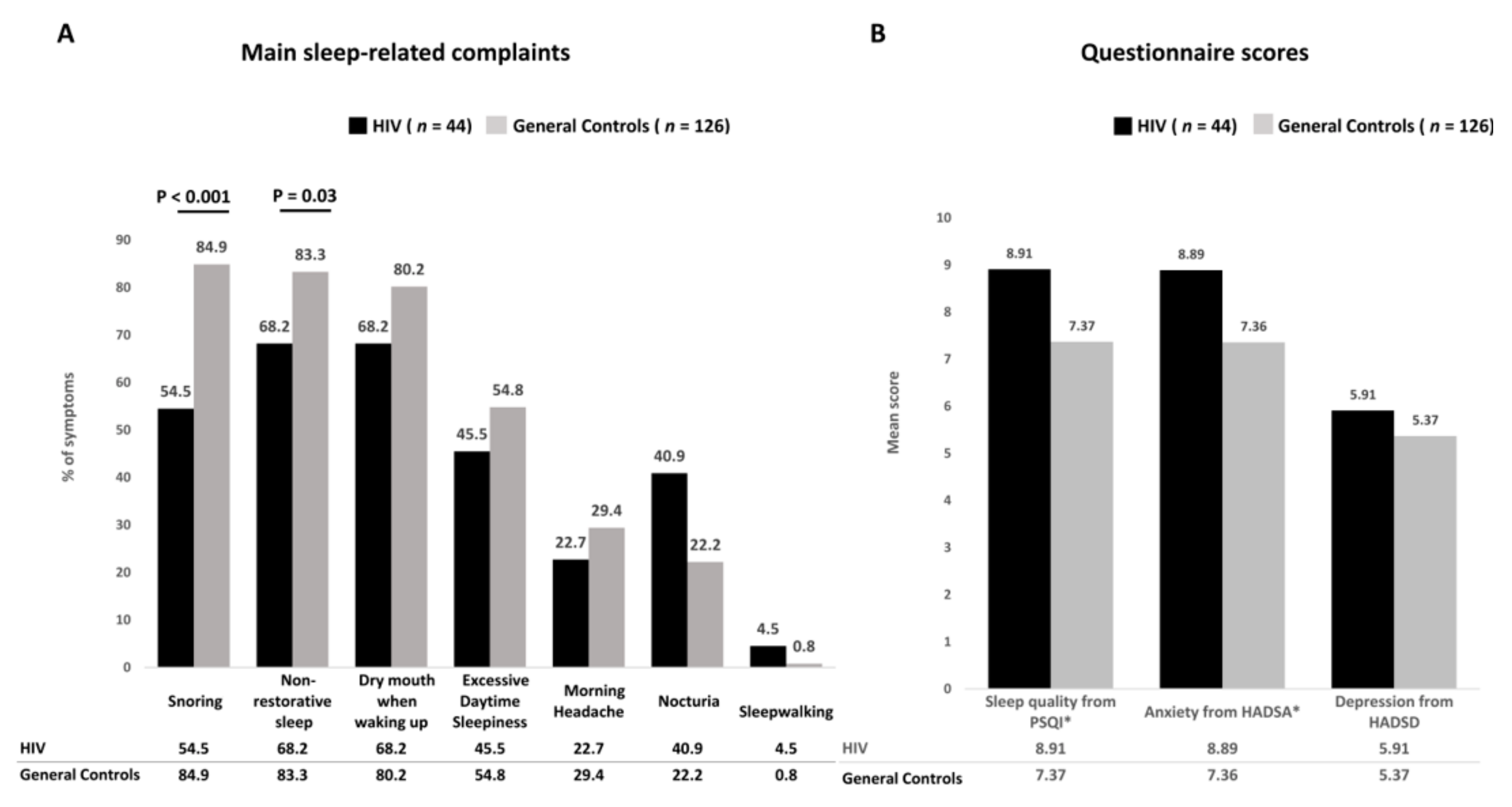
3.4. Differences in Sleep-Related Complaints
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AASM | American Academy of Sleep Medicine |
| AHI | apnea and hypopnea index |
| BMI | body mass index |
| CPSQI | the Chinese version of the Pittsburgh sleep quality index |
| HIV | human immunodeficiency virus |
| ICSD-3 | the International Classification of Sleep Disorders—third edition |
| OSA | obstructive sleep apnea |
References
- Allavena, C.; The COREVIH-Pays de la Loire Troubles du Sommeil Study Group; Guimard, T.; Billaud, E.; De La Tullaye, S.; Reliquet, V.; Pineau, S.; Hüe, H.; Supiot, C.; Chennebault, J.-M.; et al. Prevalence and Risk Factors of Sleep Disturbance in a Large HIV-Infected Adult Population. AIDS Behav. 2016, 20, 339–344. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Lin, C.-Y.; Strong, C.; Li, C.-Y.; Wang, J.-S.; Ko, W.-C.; Ko, N.-Y. Sleep disturbances at the time of a new diagnosis: A comparative study of human immunodeficiency virus patients, cancer patients, and general population controls. Sleep Med. 2017, 36, 38–43. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Cruess, D.G.; Antoni, M.H.; Gonzalez, J.; Fletcher, M.A.; Klimas, N.; Duran, R.; Ironson, G.; Schneiderman, N. Sleep disturbance mediates the association between psychological distress and immune status among HIV-positive men and women on combination antiretroviral therapy. J. Psychosom. Res. 2003, 54, 185–189. [Google Scholar] [CrossRef]
- Huang, X.; Li, H.; Meyers, K.; Xia, W.; Meng, Z.; Li, C.; Bai, J.; He, S.; Cai, W.; Huang, C.; et al. Burden of sleep disturbances and associated risk factors: A cross-sectional survey among HIV-infected persons on antiretroviral therapy across China. Sci. Rep. 2017, 7, 3657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gay, C.; Portillo, C.J.; Kelly, R.; Coggins, T.; Davis, H.; Aouizerat, B.E.; Pullinger, C.R.; Lee, K.A. Self-Reported Medication Adherence and Symptom Experience in Adults With HIV. J. Assoc. Nurses AIDS Care 2011, 22, 257–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saberi, P.; Neilands, T.B.; Johnson, M.O. Quality of Sleep: Associations with Antiretroviral Nonadherence. AIDS Patient Care STDs 2011, 25, 517–524. [Google Scholar] [CrossRef] [Green Version]
- Davis, S. Clinical Sequelae Affecting Quality of Life in the HIV-Infected Patient. J. Assoc. Nurses AIDS Care 2004, 15, S28–S33. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.; Dwyer, J. Insomnia in HIV Infection: A Systematic Review of Prevalence, Correlates, and Management. Psychosom. Med. 2005, 67, 260–269. [Google Scholar] [CrossRef]
- Brown, T.T.; Patil, S.P.; Jacobson, L.P.; Margolick, J.B.; Laffan, A.M.; Godfrey, R.J.; Johnson, J.R.; Johnson-Hill, L.M.; Reynolds, S.M.; Schwartz, A.R.; et al. Anthropometry in the prediction of sleep disordered breathing in HIV-positive and HIV-negative men. Antivir. Ther. 2010, 15, 651–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, S.P.; Brown, T.T.; Jacobson, L.P.; Margolick, J.B.; Laffan, A.; Johnson-Hill, L.; Godfrey, R.; Johnson, J.; Reynolds, S.; Schwartz, A.R.; et al. Sleep Disordered Breathing, Fatigue, and Sleepiness in HIV-Infected and -Uninfected Men. PLoS ONE 2014, 9, e99258. [Google Scholar] [CrossRef]
- Gingo, M.R.; Balasubramani, G.K.; Rice, T.B.; Kingsley, L.; Kleerup, E.C.; Detels, R.; Seaberg, E.C.; Greenblatt, R.M.; Holman, S.; Huang, L.; et al. Pulmonary symptoms and diagnoses are associated with HIV in the MACS and WIHS cohorts. BMC Pulm. Med. 2014, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunisaki, K.; Akgün, K.M.; Fiellin, D.; Gibert, C.L.; Kim, J.W.; Rimland, D.; Rodriguez-Barradas, M.C.; Yaggi, H.K.; Crothers, K. Prevalence and correlates of obstructive sleep apnoea among patients with and without HIV infection. HIV Med. 2015, 16, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Njoh, A.A.; Mbong, E.N.; Mbi, V.O.; Mengnjo, M.K.; Nfor, L.N.; Ngarka, L.; Chokote, S.E.; Fonsah, J.Y.; Kingue, S.; Ntone, F.E.; et al. Likelihood of obstructive sleep apnea in people living with HIV in Cameroon—Preliminary findings. Sleep Sci. Pr. 2017, 1, 4. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-C.; Lin, C.-Y.; Chen, Y.-C.; Ko, W.-C.; Li, C.-Y.; Ko, N.-Y. High sleep-related breathing disorders among HIV-infected patients with sleep complaints. Sleep Med. 2020, 75, 218–224. [Google Scholar] [CrossRef]
- Gamaldo, C.E.; Spira, A.P.; Hock, R.S.; Salas, R.M.E.; McArthur, J.C.; David, P.M.; Mbeo, G.; Smith, M.T. Sleep, Function and HIV: A Multi-Method Assessment. AIDS Behav. 2013, 17, 2808–2815. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine (AASM). AASM Clarifies Hypopnea Scoring Criteria. Available online: https://aasm.org/aasm-clarifies-hypopnea-scoring-criteria (accessed on 28 October 2017).
- Berry, R.B.; Gamaldo, C.E.; Harding, S.M. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specification; American Academy of Sleep Medicine: Darien, IL, USA, 2012. [Google Scholar]
- Bonnie Robertson, B.M.; Carno, M.-A. Polysomnography for the Sleep Technologist: Instrumentation, Monitoring, and Related Procedures; Elsevier: New York, NY, USA, 2014. [Google Scholar]
- Van Kerrebroeck, P.; Abrams, P.; Chaikin, D.; Donovan, J.; Fonda, D.; Jackson, S.; Jennum, P.; Johnson, T.; Lose, G.; Mattiasson, A.; et al. The standardisation of terminology in nocturia: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 179–183. [Google Scholar] [CrossRef]
- Tsai, P.-S.; Wang, S.-Y.; Wang, M.-Y.; Su, C.-T.; Yang, T.-T.; Huang, C.-J.; Fang, S.-C. Psychometric Evaluation of the Chinese Version of the Pittsburgh Sleep Quality Index (CPSQI) in Primary Insomnia and Control Subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale-A review of validation data and clinical results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Sale, S.; Dankishiya, F.S.; Gadanya, M.A. Validation of Hospital Anxiety and Depression Rating Scale among HIV/ AIDS Patients in Aminu Kano Teaching Hospital, Kano, North-Western Nigeria. J. Ther. Manag. HIV Infect. 2014, 2, 45–49. [Google Scholar]
- Bonnet, M.H.; Arand, D.L. EEG Arousal Norms by Age. J. Clin. Sleep Med. 2007, 3, 271–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soehner, A.M.; Kaplan, K.A.; Harvey, A.G. Prevalence and clinical correlates of co-occurring insomnia and hypersomnia symptoms in depression. J. Affect. Disord. 2014, 167, 93–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallego, L.; Barreiro, P.; Del Rio, R.; De Requena, D.G.; Rodríguez-Albariño, A.; González-Lahoz, J.; Soriano, V. Analyzing Sleep Abnormalities in HIV-Infected Patients Treated with Efavirenz. Clin. Infect. Dis. 2004, 38, 430–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, M.; Pearsall, J.; Buckner, R.L.; Walker, M.P. REM Sleep, Prefrontal Theta, and the Consolidation of Human Emotional Memory. Cereb. Cortex 2008, 19, 1158–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morlese, J.F.; Qazi, N.A.; Gazzard, B.G.; Nelson, M.R. Nevirapine-induced neuropsychiatric complications, a class effect of non-nucleoside reverse transcriptase inhibitors? AIDS 2002, 16, 1840–1841. [Google Scholar] [CrossRef]
- Pedrol, E.; Llibre, J.; Tasias, M.; Curran, A.; Guardiola, J.; Deig, E.; Guelar, A.; Martínez-Madrid, O.; Tikhomirova, L.; Ramirez, R.; et al. Outcome of neuropsychiatric symptoms related to an antiretroviral drug following its substitution by nevirapine: The RELAX study. HIV Med. 2015, 16, 628–634. [Google Scholar] [CrossRef]
- Kramer-Hämmerle, S.; Rothenaigner, I.; Wolff, H.; Bell, J.E.; Brack-Werner, R. Cells of the central nervous system as targets and reservoirs of the human immunodeficiency virus. Virus Res. 2005, 111, 194–213. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Gangwani, M.R.; Chaudhari, N.S.; Glazyrin, A.; Bhat, H.K.; Kumar, A. Neurotoxicity in the Post-HAART Era: Caution for the Antiretroviral Therapeutics. Neurotox. Res. 2016, 30, 677–697. [Google Scholar] [CrossRef] [PubMed]
- Bayard, S.; Dauvilliers, Y.; Yu, H.; Croisier-Langenier, M.; Rossignol, A.; Charif, M.; Geny, C.; Carlander, B.; De Cock, V.C. Impulse control disorder and rapid eye movement sleep behavior disorder in Parkinson’s disease. Parkinsonism Relat. Disord. 2014, 20, 1411–1414. [Google Scholar] [CrossRef]
- Cardoso, F. HIV-related movement disorders: Epidemiology, pathogenesis and management. CNS Drugs 2002, 16, 663–668. [Google Scholar] [CrossRef]
- Dehner, L.F.; Spitz, M.; Pereira, J.S. Parkinsonism in HIV infected patients during antiretroviral therapy—Data from a Brazilian tertiary hospital. Braz. J. Infect. Dis. 2016, 20, 499–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khazaie, H.; Negahban, S.; Ghadami, M.R.; Bahmani, D.S.; Holsboer-Trachsler, E.; Brand, S. Among middle-aged adults, snoring predicted hypertension independently of sleep apnoea. J. Int. Med Res. 2018, 46, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Léger, D.; Annesi-Maesano, I.; Carat, F.; Rugina, M.; Chanal, I.; Pribil, C.; El Hasnaoui, A.; Bousquet, J. Allergic rhinitis and its consequences on quality of sleep: An unexplored area. Arch. Intern. Med. 2006, 166, 1744–1748. [Google Scholar] [CrossRef] [Green Version]
- Van Herzeele, C.; Walle, J.V.; Dhondt, K.; Jull, K.V. Recent advances in managing and understanding enuresis. F1000Research 2017, 6, 1881. [Google Scholar] [CrossRef] [Green Version]
- Bruyneel, M.; Libert, W.; Ameye, L.; Ninane, V. Comparison between home and hospital set-up for unattended home-based polysomnography: A prospective randomized study. Sleep Med. 2015, 16, 1434–1438. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Neill, A.M. Home set-up polysomnography in the assessment of suspected obstructive sleep apnea. J. Sleep Res. 2011, 20, 207–213. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | HIV, n = 44 | Controls, n = 126 | p Value |
|---|---|---|---|
| Age (year) [mean, SD] | 34.2, 9.1 | 35.6, 10.0 | 0.40 |
| Body mass index (kg/cm2) [mean, SD] | 23.6, 4.0 | 23.1, 4.0 | 0.44 |
| Neck circumference (cm), [mean, SD] | 36.3, 2.2 | 36.3, 2.5 | 1.00 |
| Education level | 0.11 | ||
| Under junior | 3 (6.8) | 5 (4.2) | |
| Senior/college | 38 (86.4) | 90 (75.6) | |
| University and above | 3 (6.8) | 24 (20.2) | |
| Occupation | 0.17 | ||
| Non-shift worker | 31 (79.5) | 79 (88.8) | |
| Shift worker | 8 (20.5) | 10 (11.2) | |
| Use of hypnosis | 10 (22.7) | 23 (18.3) | 0.52 |
| Comorbidities | |||
| Rhinitis/sinusitis | 14 (31.8) | 67 (53.2) | 0.02 |
| Gastroesophageal reflux disease | 18 (40.9) | 45 (35.7) | 0.54 |
| Hypertension | 3 (6.8) | 15 (11.9) | 0.35 |
| Hyperuricemia | 2 (4.5) | 11 (8.7) | 0.37 |
| Asthma | 4 (9.1) | 10 (7.9) | 0.81 |
| Angina | 1 (2.3) | 9 (7.1) | 0.24 |
| Hyperlipidemia | 3 (6.8) | 7 (5.6) | 0.76 |
| Diabetes mellitus | 0 (0.0) | 1 (0.8) | 0.55 |
| Use of ART | 40 (90.9) | - | - |
| Years since ART initiation [mean, SD] | 1.9, 2.0 | - | - |
| ≤1 year | 14 (35.0) | - | |
| 1–3 years | 19 (47.5) | - | |
| >3 years | 7 (17.5) | - | |
| CD4 count (copies/mL) [mean, SD] | 557.5, 230.8 | - | - |
| ≤200 | 12 (28.6) | - | |
| >200 | 30 (71.4) | - | |
| Viral load (copies/mL) [median, SD] | 17,749.6, 103,463.3 | - | - |
| Undetectable | 32 (72.7) | ||
| Detectable | 12 (27.3) | ||
| Year since HIV diagnosis [mean, SD] | 2.7, 3.0 | - | - |
| ≤1 year | 15 (34.1) | - | |
| 1–3 years | 17 (38.6) | - | |
| >3 years | 12 (27.3) | - |
| Variables | HIV (n = 44) | Controls (n = 126) | p Value |
|---|---|---|---|
| n (%) | |||
| Total sleep time (min) | |||
| Mean, SD | 408.7, 95.9 | 356.4, 50.3 | <0.001 |
| Sleep latency (min) | |||
| <30 a | 39 (88.6) | 117 (92.9) | 0.38 |
| Mean, SD | 19.8, 55.4 | 12.5, 13.4 | 0.39 |
| Stage 1 (%) | |||
| ≥5% a | 42 (95.5) | 123 (97.6) | 0.46 |
| Mean, SD | 15.7, 8.4 | 21.8, 14.5 | <0.01 |
| Stage 2 (%) | |||
| ≥50% a | 32 (72.7) | 69 (54.8) | 0.04 |
| Mean, SD | 54.0, 9.5 | 50.9, 11.1 | 0.10 |
| Stage 3 (%) | |||
| ≥20% a | 5 (11.4) | 21 (16.7) | 0.40 |
| Mean, SD | 9.7, 8.6 | 10.7, 9.1 | 0.54 |
| Rapid eye movement stage (%) | |||
| ≥25% a | 9 (20.5) | 12 (9.5) | 0.05 |
| Mean, SD | 20.6, 5.4 | 16.6, 6.6 | <0.001 |
| Sleep efficiency (%) | |||
| ≥85% a | 30 (68.2) | 77 (61.1) | 0.40 |
| Mean, SD | 86.2, 10.6 | 84.7, 10.8 | 0.43 |
| Arousal index (events/hour) | |||
| ≥16.8 b | 19 (43.2) | 103 (81.7) | <0.001 |
| Mean, SD | 18.2, 11.8 | 30.4, 14.5 | <0.001 |
| Variables | HIV (n = 44) | Controls (n = 126) | p Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Sleep-disordered breathing (apnea-hypopnea index ≥ 5) | 25 (56.8%) | 110 (87.3%) | <0.01 |
| Apnea index (events/hour) [mean, SD] | 3.39, 8.72 | 6.80, 10.47 | 0.04 |
| Hypopnea index (events/hour) [mean, SD] | 8.53, 9.24 | 17.83, 15.07 | <0.001 |
| Obstructive sleep apnea index (events/hour) [mean, SD] | 2.91, 8.75 | 5.57, 8.86 | 0.09 |
| Central sleep apnea index (events/hour) [mean, SD] | 0.38, 0.52 | 0.28, 0.51 | 0.25 |
| Mixed apnea index (events/hour) [mean, SD] | 0.09, 0.25 | 0.99, 3.09 | <0.01 |
| Psychological disturbances | 32 (72.7%) | 51 (40.5%) | <0.001 |
| Rapid eye movement behavior disorder | 11 (25.0%) | 6 (4.8%) | <0.01 |
| Periodic limb movements | 5 (11.4%) | 18 (14.3%) | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Chen, C.-C.; Strollo, P.J., Jr.; Li, C.-Y.; Ko, W.-C.; Lin, C.-Y.; Ko, N.-Y. Differences in Sleep Disorders between HIV-Infected Persons and Matched Controls with Sleep Problems: A Matched-Cohort Study Based on Laboratory and Survey Data. J. Clin. Med. 2021, 10, 5206. https://doi.org/10.3390/jcm10215206
Chen Y-C, Chen C-C, Strollo PJ Jr., Li C-Y, Ko W-C, Lin C-Y, Ko N-Y. Differences in Sleep Disorders between HIV-Infected Persons and Matched Controls with Sleep Problems: A Matched-Cohort Study Based on Laboratory and Survey Data. Journal of Clinical Medicine. 2021; 10(21):5206. https://doi.org/10.3390/jcm10215206
Chicago/Turabian StyleChen, Yen-Chin, Chang-Chun Chen, Patrick J. Strollo, Jr., Chung-Yi Li, Wen-Chien Ko, Cheng-Yu Lin, and Nai-Ying Ko. 2021. "Differences in Sleep Disorders between HIV-Infected Persons and Matched Controls with Sleep Problems: A Matched-Cohort Study Based on Laboratory and Survey Data" Journal of Clinical Medicine 10, no. 21: 5206. https://doi.org/10.3390/jcm10215206