
Prevalence and Causes of Myocardial Infarction with Non-Obstructive Coronary Arteries in a Contemporary Cohort of Patients with Suspected Myocardial Infarction

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
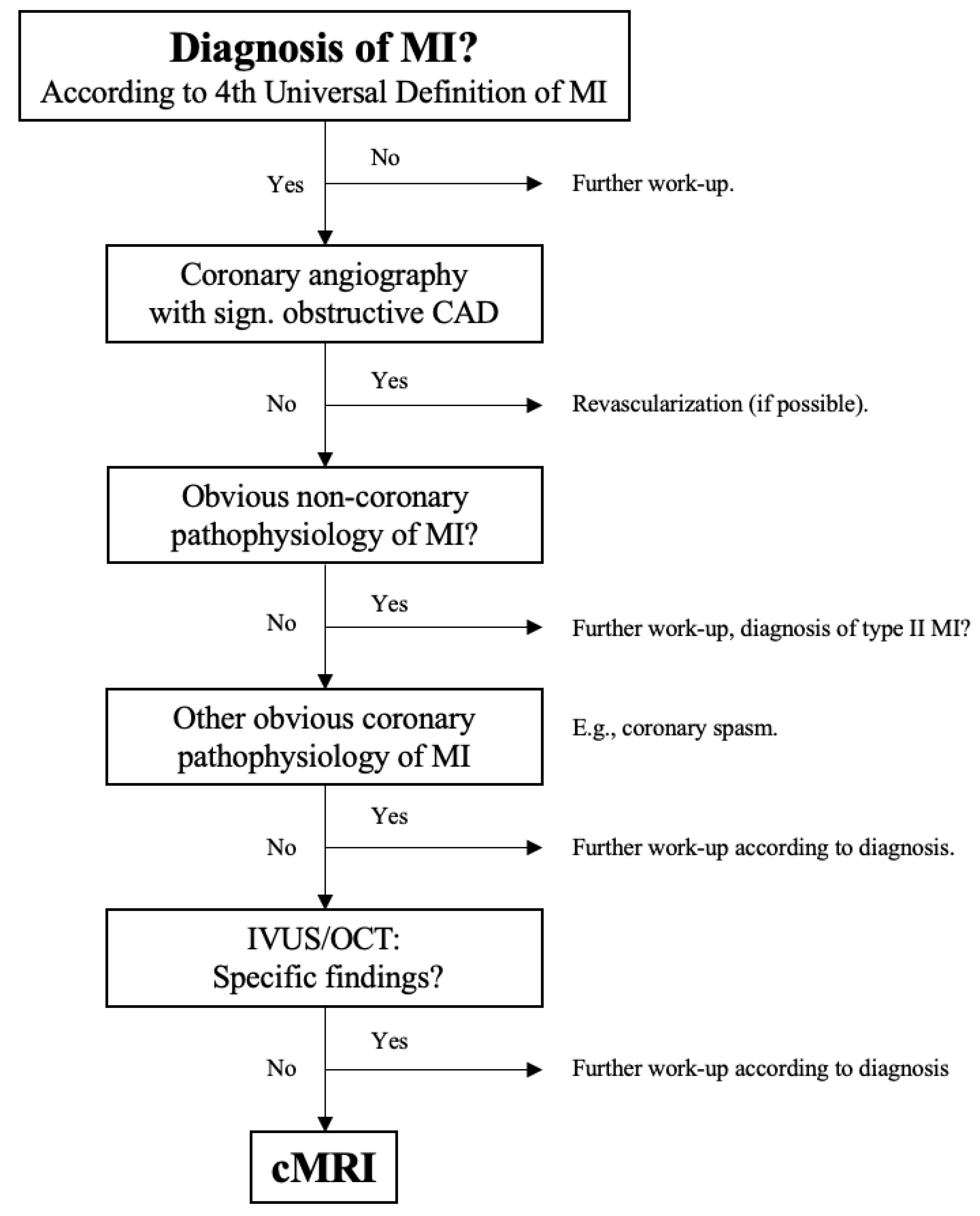
2.2. MINOCA Work-Up
2.3. Statistical Analysis
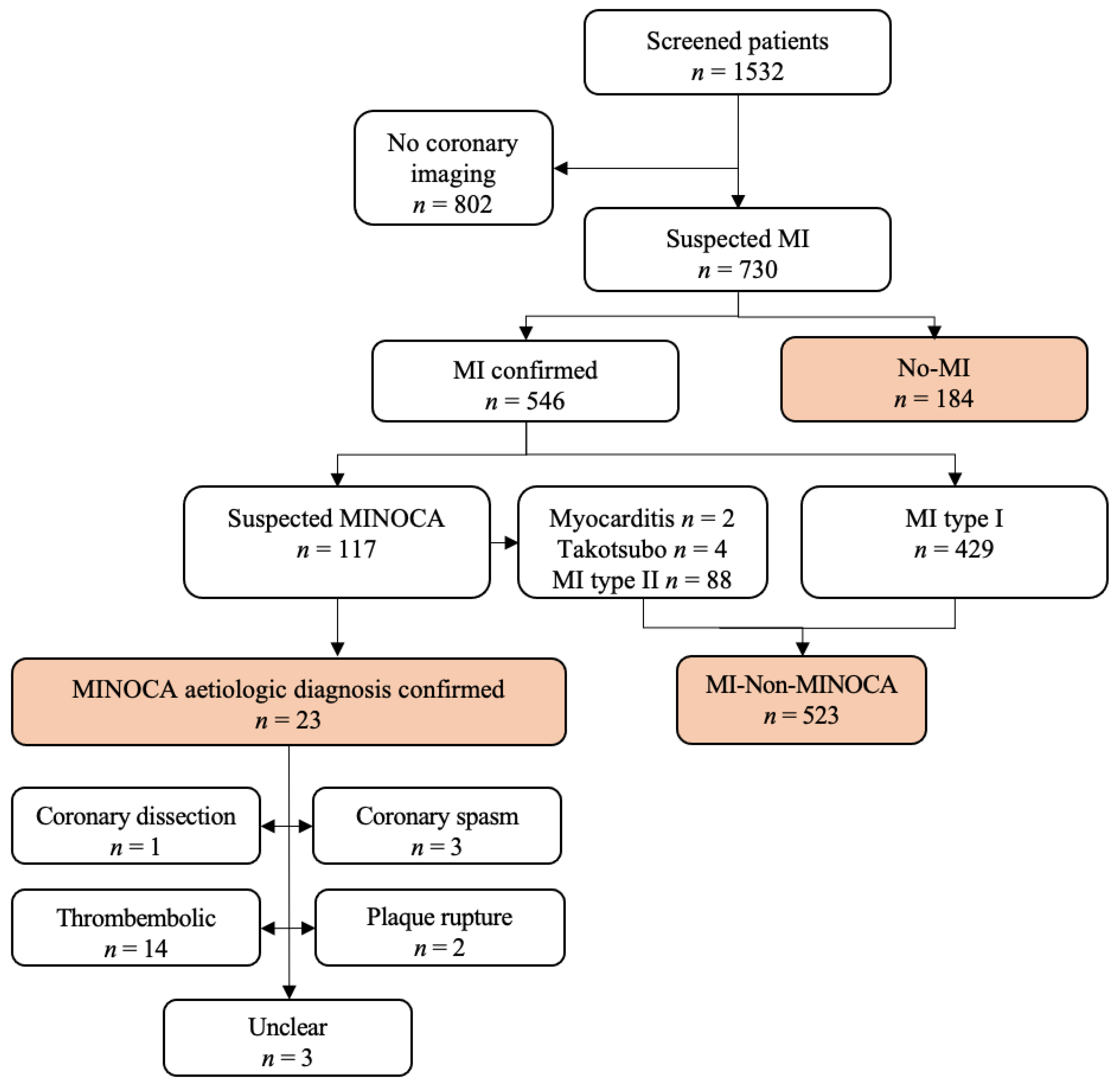
3. Results
3.1. Patient Classification and Characteristics
3.2. Predictors for MINOCA
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjöld, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- DeWood, M.A.; Spores, J.; Notske, R.; Mouser, L.T.; Burroughs, R.; Golden, M.S.; Lang, H.T. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N. Engl. J. Med. 1980, 303, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Planer, D.; Mehran, R.; Ohman, E.M.; White, H.D.; Newman, J.D.; Xu, K.; Stone, G.W. Prognosis of patients with non-ST-segment-elevation myocardial infarction and nonobstructive coronary artery disease: Propensity-matched analysis from the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circ. Cardiovasc. Interv. 2014, 7, 285–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. The Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar]
- Mukherjee, D. Myocardial Infarction With Nonobstructive Coronary Arteries: A Call for Individualized Treatment. J. Am. Heart Assoc. 2019, 8, e013361. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.R.; Harrison, W.; Smyth, D.; Flynn, C.; Lee, M.; Kerr, A.J. Myocardial Infarction without Obstructive Coronary Artery Disease is Not a Benign Condition (ANZACS-QI 10). Heart Lung Circ. 2018, 27, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 2015, 131, 861–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.; de Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2017, 38, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients with Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar]
- Amann, M.; Gaiser, F.; Schwenk, S.I.; Rahimi, F.; Schmitz, R.; Mashayekhi, K.; Ferenc, M.; Neumann, F.; Valina, C.M.; Hochholzer, W. Evaluation of a 1-h troponin algorithm for diagnosing myocardial infarction in high-risk patients admitted to a chest pain unit: The prospective FAST-MI cohort study. BMJ Open 2019, 9, e032124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasupathy, S.; Tavella, R.; Beltrame, J.F. Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): The Past, Present, and Future Management. Circulation 2017, 135, 1490–1493. [Google Scholar] [CrossRef] [PubMed]
- Choo, E.H.; Chang, K.; Lee, K.Y.; Lee, D.; Kim, J.G.; Ahn, Y.; Kim, Y.J.; Chae, S.C.; Cho, M.C.; Kim, C.J.; et al. Prognosis and Predictors of Mortality in Patients Suffering Myocardial Infarction with Non-Obstructive Coronary Arteries. J. Am. Heart Assoc. 2019, 8, e011990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyer, R.P.; Tavella, R.; Curtis, J.P.; Wang, Y.; Pauspathy, S.; Messenger, J.; Rumsfeld, J.S.; Maddox, T.M.; Krumholz, H.M.; Spertus, J.A.; et al. Myocardial infarction with non-obstructive coronary arteries as compared with myocardial infarction and obstructive coronary disease: Outcomes in a Medicare population. Eur. Heart J. 2020, 41, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros-Ortega, D.; Martínez-González, O.; Gómez-Casero, R.B.; Quintana-Díaz, M.; de Miguel-Balsa, E.; Martín-Parra, C.; López-Matamala, B.; Chana-García, M.; Alonso-Fernández, M.Á.; Manso-Álvarez, M.; et al. Characteristics of patients with myocardial infarction with nonobstructive coronary arteries (MINOCA) from the ARIAM-SEMICYUC registry: Development of a score for predicting MINOCA. Vasc Health Risk Manag. 2019, 15, 57–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dokainish, H.; Pillai, M.; Murphy, S.A.; DiBattiste, P.M.; Schweiger, M.J.; Lotfi, A.; Morrow, D.A.; Cannon, C.P.; Braunwald, E.; Lakkis, N.; et al. Prognostic implications of elevated troponin in patients with suspected acute coronary syndrome but no critical epicardial coronary disease: A TACTICS-TIMI-18 substudy. J. Am. Coll. Cardiol. 2005, 45, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| MINOCA n = 23 | MI-Non-MINOCA n = 523 | No-MI n = 184 | p-Value | |
|---|---|---|---|---|
| Age, years | 63.2 {54.0–7.0} | 69.8 {62.0–79.0} | 68.9 {61.0–78.0} | 0.81 |
| Male | 12 (52.2%) | 389 (74.4%) | 114 (62.0%) | 0.001 |
| Body mass index, kg/m2 | 26.5 {24.6–28.3} | 27.7 {24.7–29.7} | 27.9 {24.7–30.3} | 0.36 |
| Cardiovascular risk factors | ||||
| Arterial hypertension | 12 (52.2%) | 437 (83.6%) | 155 (84.2%) | <0.001 |
| Diabetes mellitus | 1 (4.3%) | 161 (30.8%) | 37 (20.1%) | 0.001 |
| Hypercholesterolemia | 10 (43.5%) | 394 (75.3%) | 133 (72.3%) | 0.003 |
| Current smoking | 3 (13.0%) | 120 (22.9%) | 32 (17.4%) | 0.12 |
| Medical history | ||||
| Previous PCI | 4 (17.4%) | 232 (44.4%) | 75 (40.7%) | 0.03 |
| Previous CABG | 0 (0%) | 57 (10.9%) | 12 (6.5%) | 0.06 |
| Previous myocardial infarction | 4 (17.4%) | 125 (12.9%) | 38 (20.6%) | 0.54 |
| Congestive heart failure | 0 (0%) | 25 (4.8%) | 7 (3.8%) | 0.49 |
| Peripheral artery disease | 0 0%) | 64 (12.2%) | 13 (7.1%) | 0.04 |
| Previous Stroke/TIA | 1 (4.3%) | 53 (2.8%) | 12 (6.5%) | 0.25 |
| Previous severe bleeding | 0 (0%) | 15 (2.6%) | 9 (4.8%) | 0.28 |
| Chronic pulmonary disease | 0 (0%) | 38 (7.2%) | 21 (11.4%) | 0.07 |
| Leading symptom | 0.46 | |||
| Chest pain | 19 (82.6%) | 376 (71.9%) | 126 (68.5%) | |
| Dyspnea | 1 (4.3%) | 88 (16.8%) | 32 (17.4%) | |
| Collapse | 0 (0%) | 13 (2.5%) | 8 (4.3%) | |
| Others | 3 (13.0%) | 46 (8.7%) | 14 (7.6%) | |
| Medication on admission | ||||
| Aspirin | 6 (26.1%) | 282 (53.9%) | 82 (44.6%) | 0.005 |
| P2Y12-receptor inhibitor | 0 (0%) | 62 (11.9%) | 29 (15.8%) | 0.07 |
| Oral anticoagulants | 2 (8.7%) | 107 (20.5%) | 48 (26.1%) | 0.09 |
| ß-Blocker | 7 (30.4%) | 254 (48.6%) | 98 (53.2%) | 0.11 |
| Nitrates | 0 (0%) | 32 (6.1%) | 8 (4.3%) | 0.33 |
| Statin | 7 (30.4%) | 257 (49.3%) | 90 (48.9%) | 0.83 |
| MINOCA n = 23 | MI-Non-MINOCA n = 523 | No MI n = 184 | p-Value | |
|---|---|---|---|---|
| Baseline blood testing | ||||
| High-sensitive troponin T, ng/mL | 0.11 {0.02–0.45} | 0.26 {0.02–0.51} | 0.01 {0.007–0.03} | <0.001 |
| LDL-cholesterol, mg/dL | 117 {39–183} | 119 {30–359} | 108 {41–230} | 0.22 |
| Cholesterol, mg/dL | 182 {106–280} | 183 {150–450} | 175 {143–297} | 0.99 |
| Creatinine, mg/dL | 1.0 {0.6-1.5} | 1.2 {0.4-6.6} | 1.1 {0.4-6.2} | 0.98 |
| Urea, mg/dL | 39 {21–77} | 43 {16–187} | 41.0 {30–143} | 0.02 |
| Glomerular filtration rate, mL/min | 76 {41–115} | 75 {9–178} | 76 {61–172} | 0.87 |
| Hemoglobin, g/dL | 14 {11–17} | 13 {6–19} | 14 {13–18} | 0.99 |
| C-reactive protein, mg/dL | 1.3 {0.3–11.2} | 1.5 {0.3–24.0} | 0.8 {0.3–16.6} | 0.46 |
| ECG at baseline | ||||
| Initial rhythm | 0.62 | |||
| Sinus rhythm | 21 (91.3%) | 452 (86.4%) | 154 (83.7%) | |
| Atrial fibrillation | 2 (8.7%) | 57 (10.9%) | 25 (13.6%) | |
| Ventricular tachycardia | 0 (0%) | 0 (0.0%) | 1 (0.5%) | |
| Supraventricular tachycardia | 0 (0%) | 4 (0.8%) | 0 (0.0%) | |
| ST-segment changes | 4 (17.4%) | 102 (19.5%) | 12 (6.5%) | <0.001 |
| T-wave inversion | 3 (13.0%) | 87 (16.6%) | 20 (10.9%) | 0.16 |
| Bundle branch block | 4 (17.4%) | 92 (17.6%) | 28 (15.2%) | 0.76 |
| Echocardiography | ||||
| Impaired left ventricular function | 2 (8.7%) | 259 (49.5%) | 52 (9.9%) | <0.001 |
| Moderate/severe aortic stenosis | 1 (0.5%) | 32 (6.1%) | 12 (6.5%) | 0.92 |
| Moderate/severe aortic insufficiency | 1 (3.6%) | 8 (1.2%) | 5 (2.7%) | 0.41 |
| Moderate/severe mitral insufficiency | 1 (4.3%) | 57 (10.9%) | 20 (10.9%) | 0.61 |
| Univariable Analyses | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Diagnosis | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Age per year | 0.96 | (0.93–0.99) | 0.01 | 0.98 | (0.94–1.02) | 0.18 |
| Female Sex | 2.67 | (1.15–6.18) | 0.02 | 3.33 | (1.24–8.93) | 0.02 |
| Cardiovascular risk factors | ||||||
| Arterial hypertension | 0.21 | (0.09–0.50) | <0.001 | 0.56 | (0.20–1.57) | 0.27 |
| Diabetes mellitus | 0.10 | (0.01–0.76) | 0.03 | 0.16 | (0.02–1.28) | 0.08 |
| Hypercholesterolemia | 0.25 | (0.11–0.59) | 0.002 | 0.36 | (0.14–0.95 | 0.04 |
| Current smoking | 0.51 | (0.15–1.73) | 0.28 | |||
| Medical history | ||||||
| Previous PCI | 0.27 | (0.09–0.79) | 0.02 | 0.98 | (0.22–4.29) | 0.98 |
| Previous CABG | not in group | |||||
| Previous MI | 0.67 | (0.22–2.01) | 0.48 | |||
| Congestive heart failure | not in group | |||||
| Previous stroke/TIA | 0.40 | (0.05–3.06) | 0.38 | |||
| Previous severe bleeding | not in group | |||||
| Chronic pulmonary disease | not in group | |||||
| Leading symptom | ||||||
| Chest pain | 0.22 | (0.03–1.68) | 0.15 | |||
| Dyspnea | not in group | |||||
| Collapse | 1.29 | (0.37–4.53) | 0.69 | |||
| Medicaments on admission | not in group | |||||
| Aspirin | 0.30 | (1.12–0.78) | 0.01 | 0.80 | (0.23–2.86) | 0.73 |
| Oral anticoagulant | 0.37 | (0.09–1.59) | 0.18 | |||
| ß-Blocker | 0.46 | (0.19–1.14) | 0.09 | |||
| Nitrates | not in group | |||||
| Statins | 0.45 | (0.18–1.12) | 0.09 | |||
| Baseline blood test results | ||||||
| High-sensitivity Troponin T per 1 ng/mL | 0.98 | (0.57–1.70) | 0.95 | |||
| Hemoglobin per 1 g/L | 1.10 | (0.88–1.38) | 0.40 | |||
| Glomerular filtration rate per 1 mL/min | 0.99 | (0.98–1.01) | 0.83 | |||
| C-reactive protein per 1 mg/L | 0.98 | (0.84–1.13) | 0.77 | |||
| LDL-cholesterol per 1 mmol/L | 1.00 | (0.99–1.01) | 0.81 | |||
| ECG | ||||||
| Atrial fibrillation | 0.59 | (0.14–2.60) | 0.49 | |||
| ST-segment changes | 0.87 | (0.29–2.62) | 0.81 | |||
| T-wave inversion | 0.75 | (0.22–2.59) | 0.65 | |||
| Bundle branch block | 1.01 | (0.33–2.97) | 0.98 | |||
| Echocardiography | ||||||
| Impaired left ventricular function | 0.09 | (0.02–0.42) | 0.002 | 0.14 | (0.03–0.61) | 0.009 |
| Moderate/Severe aortic stenosis | 0.69 | (0.09–5.35) | 0.73 | |||
| Moderate/Severe mitral insufficiency | 0.37 | (0.05–2.82) | 0.33 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dees, D.; Rahimi, F.; Amann, M.; Nührenberg, T.G.; Löffelhardt, N.; Schmitz, R.; Valina, C.M.; Neumann, F.-J.; Hochholzer, W. Prevalence and Causes of Myocardial Infarction with Non-Obstructive Coronary Arteries in a Contemporary Cohort of Patients with Suspected Myocardial Infarction. J. Clin. Med. 2021, 10, 5188. https://doi.org/10.3390/jcm10215188
Dees D, Rahimi F, Amann M, Nührenberg TG, Löffelhardt N, Schmitz R, Valina CM, Neumann F-J, Hochholzer W. Prevalence and Causes of Myocardial Infarction with Non-Obstructive Coronary Arteries in a Contemporary Cohort of Patients with Suspected Myocardial Infarction. Journal of Clinical Medicine. 2021; 10(21):5188. https://doi.org/10.3390/jcm10215188
Chicago/Turabian StyleDees, Dominik, Faridun Rahimi, Michael Amann, Thomas G. Nührenberg, Nikolaus Löffelhardt, Roland Schmitz, Christian M. Valina, Franz-Josef Neumann, and Willibald Hochholzer. 2021. "Prevalence and Causes of Myocardial Infarction with Non-Obstructive Coronary Arteries in a Contemporary Cohort of Patients with Suspected Myocardial Infarction" Journal of Clinical Medicine 10, no. 21: 5188. https://doi.org/10.3390/jcm10215188