
Evaluation of the Efficacy and Safety of Canaloplasty and iStent Bypass Implantation in Patients with Open-Angle Glaucoma: A Review of the Literature


Abstract
:1. Introduction
2. Materials and Methods
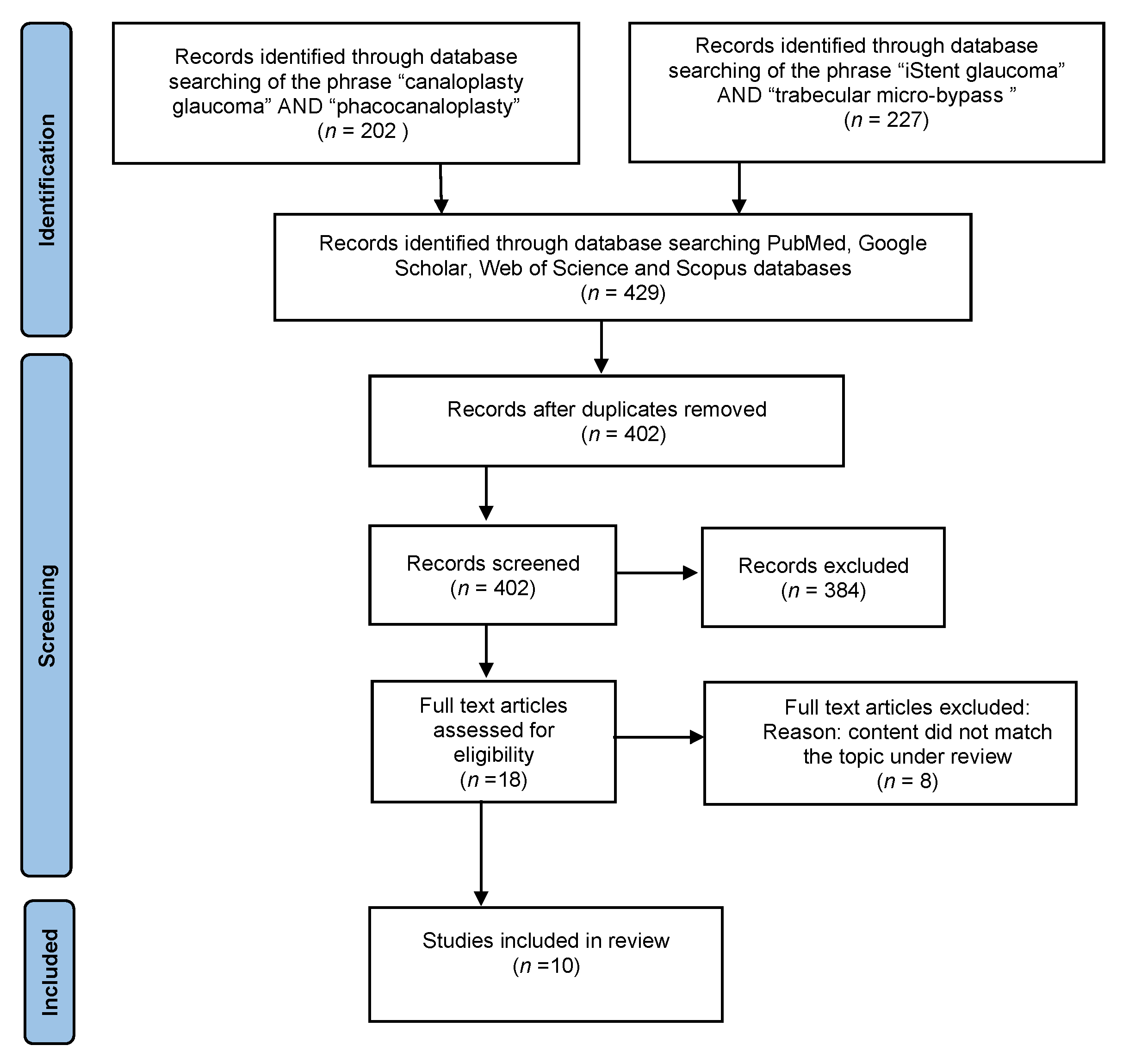
2.1. Search Strategy
2.2. Inclusion Criteria
- The study is a PRCT.
- The study involves patients with a diagnosis of POAG.
- One of the following surgical procedures was used: iStent bypass implantation with or without phacoemulsification, or canaloplasty with or without phacoemulsification.
- The study analyzes variables such as best corrected visual acuity (BCVA), IOP, and number of glaucoma drops used before and after surgery.
- The study shall include an adequate follow-up period.
2.3. Exlusion Criteria
- A case report, review, or experimental study.
- Studies describing partial results.
- Review-type papers.
- Studies not including all analyzed factors.
2.4. Risk of Bias Assessment
2.5. Data Extraction
3. Canaloplasty
4. iStent
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, G.L.; Lopes, J.F.; Junk, A.; Grigorian, A.P.; Henderer, J. Systems for Staging the Amount of Optic Nerve Damage in Glaucoma: A Critical Review and New Material. Surv. Ophthalmol. 2006, 51, 293–315. [Google Scholar] [CrossRef] [PubMed]
- The Advanced Glaucoma Intervention Study (AGIS): The relationship between control of intraocular pressure and visual field deterioration.The AGIS Investigators. Am. J. Ophthalmol. 2000, 130, 429–440. [CrossRef]
- Saheb, H.; Ahmed, I.I. Micro-invasive glaucoma surgery: Current perspectives and future directions. Curr. Opin. Ophthalmol. 2012, 23, 96–104. [Google Scholar] [CrossRef]
- Caprioli, J.; Kim, J.H.; Friedman, D.S.; Kiang, T.; Moster, M.R.; Parrish, R.K.; Rorer, E.M.; Samuelson, T.; Tarver, M.E.; Singh, K.; et al. Special commentary: Supporting innovation for safe and effective minimally invasive glaucoma surgery: Summary of a Joint Meeting of the American Glaucoma Society and the Food and Drug Administration, Washington, DC, February 26, 2014. Ophthalmology 2014, 122, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.A.; Von Wolff, K.; Tetz, M.; Korber, N.; Kearney, J.R.; Shingleton, B.; Samuelson, T.W. Canaloplasty: Circumferential viscodilation and tensioning of Schlemm’s canal using a flexible microcatheter for the treatment of open-angle glaucoma in adults: Interim clinical study analysis. J. Cataract Refract. Surg. 2007, 33, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, M.J.; Supnet, R.A.; Ahmed, I.I.K. Viscodilation of Schlemm’s canal for the reduction of IOP via an ab-interno approach. Clin. Ophthalmol. 2018, 12, 2149–2155. [Google Scholar] [CrossRef] [Green Version]
- Rekas, M.; Konopińska, J.; Byszewska, A.; Mariak, Z. Mini-canaloplasty as a modified technique for the surgical treatment of open-angle glaucoma. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Konopińska, J.; Lewczuk, K.; Jabłońska, J.; Mariak, Z.; Rękas, M. Microinvasive Glaucoma Surgery: A Review of Schlemm’s Canal-Based Procedures. Clin. Ophthalmol. 2021, 15, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Koerber, N.; Kearney, J.R.; Shingleton, B.; Samuelson, T.W. Canaloplasty: Three-year results of circumferential viscodilation and tensioning of Schlemm canal using a microcatheter to treat open-angle glaucoma. J. Cataract. Refract. Surg. 2011, 37, 682–690. [Google Scholar] [CrossRef]
- Battista, S.A.; Lu, Z.; Hofmann, S.; Freddo, T.; Overby, D.; Gong, H. Reduction of the Available Area for Aqueous Humor Outflow and Increase in Meshwork Herniations into Collector Channels Following Acute IOP Elevation in Bovine Eyes. Investig. Opthalmology Vis. Sci. 2008, 49, 5346–5352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grieshaber, M.C.; Pienaar, A.; Olivier, J.; Stegmann, R. Canaloplasty for primary open-angle glaucoma: Long-term outcome. Br. J. Ophthalmol. 2010, 94, 1478–1482. [Google Scholar] [CrossRef] [PubMed]
- Grieshaber, M.C.; Pienaar, A.; Olivier, J.; Stegmann, R. Comparing two tensioning suture sizes for 360 degrees viscocanalostomy (canaloplasty): A randomised controlled trial. Eye 2010, 24, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Bull, H.; Von Wolff, K.; Körber, N.; Tetz, M. Three-year canaloplasty outcomes for the treatment of open-angle glaucoma: European study results. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 1537–1545. [Google Scholar] [CrossRef]
- Matlach, J.; Dhillon, C.; Hain, J.; Schlunck, G.; Grehn, F.; Klink, T. Trabeculectomy versus canaloplasty ( TVC study) in the treatment of patients with open-angle glaucoma: A prospective randomized clinical trial. Acta Ophthalmol. 2015, 93, 753–761. [Google Scholar] [CrossRef]
- Rękas, M.; Byszewska, A.; Petz, K.; Wierzbowska, J.; Jünemann, A. Canaloplasty versus non-penetrating deep sclerectomy—A prospective, randomised study of the safety and efficacy of combined cataract and glaucoma surgery; 12-month follow-up. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 591–599. [Google Scholar] [CrossRef]
- Fea, A.M. Phacoemulsification versus phacoemulsification with micro-bypass stent implantation in primary open-angle glaucoma: Randomized double-masked clinical trial. J. Cataract. Refract. Surg. 2010, 36, 407–412. [Google Scholar] [CrossRef]
- Samuelson, T.W.; Katz, L.J.; Wells, J.M.; Duh, Y.-J.; Giamporcaro, J.E. Randomized Evaluation of the Trabecular Micro-Bypass Stent with Phacoemulsification in Patients with Glaucoma and Cataract. Ophthalmology 2011, 118, 459–467. [Google Scholar] [CrossRef]
- Craven, E.; Katz, J.L.; Wells, J.M.; Giamporcaro, J.E. Cataract surgery with trabecular micro-bypass stent implantation in patients with mild-to-moderate open-angle glaucoma and cataract: Two-year follow-up. J. Cataract. Refract. Surg. 2012, 38, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.I.K.; Fea, A.; Au, L.; Ang, R.E.; Harasymowycz, P.; Jampel, H.D.; Samuelson, T.W.; Chang, D.F.; Rhee, D.J. A Prospective Randomized Trial Comparing Hydrus and iStent Microinvasive Glaucoma Surgery Implants for Standalone Treatment of Open-Angle Glaucoma: The COMPARE Study. Ophthalmology 2020, 127, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Kozera, M.; Konopińska, J.; Mariak, Z.; Rękas, M. Effectiveness of iStent trabecular micro-bypass system combined with phacoemulsification vs. phacoemulsification alone in patients with glaucoma and cataract depending on the initial intraocular pressure. Ophthalmic Res. 2021, 64, 327–336. [Google Scholar] [CrossRef]
- Konopinska, J.; Deniziak, M.; Saeed, E.; Bartczak, A.; Zalewska, R.; Ariak, Z.; Rękas, M. Prospective Randomized Study Comparing Combined Phaco-ExPress and Phacotrabeculectomy in Open Angle Glaucoma Treatment: 12-Month Follow-up. J. Ophthalmol. 2015, 720109. [Google Scholar] [CrossRef] [PubMed]
- Bluwol, E. [Glaucoma treatment]. Rev. Prat. 2016, 66, 508–513. [Google Scholar] [PubMed]
- Chou, J.; Turalba, A.; Hoguet, A. Surgical Innovations in Glaucoma: The Transition From Trabeculectomy to MIGS. Int. Ophthalmol. Clin. 2017, 57, 39–55. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, T.J.; Berdahl, J.P.; Schweitzer, J.A.; Sudhagoni, R.G. Clinical evaluation of a trabecular microbypass stent with phacoemulsification in patients with open-angle glaucoma and cataract. Clin. Ophthalmol. 2016, 10, 1767–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rulli, E.; Biagioli, E.; Riva, I.; Gambirasio, G.; De Simone, I.; Floriani, I.; Quaranta, L. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: A systematic review and meta-analysis. JAMA Ophthalmol. 2013, 131, 1573–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Zhang, H.; Li, Y.; Yu, H. Safety and efficacy of canaloplasty versus trabeculectomy in treatment of glaucoma. Oncotarget 2017, 8, 44811–44818. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author | Year | Setting | Type of Surgery of Studied Group | Sample Size: Studied Group (Control Group) | Follow-Up (Months) |
|---|---|---|---|---|---|
| Grieshaber et al. [12] | 2010 | Southern Africa | Canaloplasty | 60 * | 30.6 ± 8.4 |
| Grieshaber et al. [13] | 2010 | Southern Africa | Canaloplasty | 90 ** | 15 |
| Bull et al. [14] | 2011 | Multicenter | Canaloplasty | 109 ** | 36 |
| Matlach et al. [15] | 2015 | Germany | Canaloplasty | 30 (32) | 24 |
| Rękas et al. [16] | 2015 | Poland | Canaloplasty + Phacoemulsification | 29 (30) | 12 |
| Fea et al. [17] | 2010 | Italy | iStent + Phacoemulsification | 12 (24) | 15 |
| Samuelson et al. [18] | 2010 | Multicenter | iStent + Phacoemulsification | 117 (123) | 24 |
| Craven et al. [19] | 2012 | Multicenter | iStent + Phacoemulsification | 117 (123) | 24 |
| Ahmed et al. [20] | 2019 | Multicenter | 2 by-pass iStent | 77 (75) | 12 |
| Kozera et al. [21] | 2021 | Poland | iStent + Phacoemulsification | 44 (36) | 24 |
| Author | Mean Preoperative BCVA * | Mean Preoperative IOP ** | Preoperative Number of Applied Eye Drops | Mean BCVA * after Follow-Up Period | Mean IOP ** after Follow-Up Period | Number of Applied Eye Drops after Follow-Up Period |
|---|---|---|---|---|---|---|
| Grieshaber et al. [12] | 0.61 ± 0.42 | 45.0 ± 12.1 mmHg | Without eye drops | 0.58 ± 0.31 | 13.3 ± 1.7 mmHg | Without eye drops |
| Grieshaber et al. [13] | LOD **** | 42.7 ± 12.5 (Prolene 6-0) 45.0 ± 12.1 (Prolene 10-0) | Without eye drops | LOD **** | 19.2 ± 6.4 mmHg (Prolene 6-0) 16.4 ± 4.9 (Prolene 10-0) | Without eye drops |
| Bull et al. [14] | 0.22 ± 0.25 | 23.0 ± 4.3 mmHg | 1.9 ± 0.7 | 0.20± 0.26 | 15.1 ± 3.1 mmHg | 0.9 ± 0.9 |
| Matlach et al. [15] | 0.08–0.40 logMAR *** | 23.7 ± 5.1 mmHg | 2.6 ± 1.6 | 0.20 ± 0.26 logMAR | 14.4 ± 4.2 mmHg | 0.9 ± 1.1 |
| Rękas et al. [16] | 0.74 ± 0.70 logMAR *** | 19.0 ± 6.9 mmHg | 2.64 ± 0.68 | 0.11 ± 0.17 logMAR | 12.6 ± 2.7 mmHg | 0.27 ± 0.67 |
| Author | Mean Preoperative BCVA * | Mean Preoperative IOP ** | Preoperative Number of Applied Eye Drops | Mean BCVA * after Follow-Up Period | Mean IOP ** after Follow-Up Period | Number of Applied Eye Drops after Follow-Up Period |
|---|---|---|---|---|---|---|
| Fea et al. [17] | no better than 0.6 | 17.9 ± 2.6 mmHg | 1.9 ± 0.7 | LOD *** | 14.8 ± 1.2 mmHg | 0.4 ± 0.7 |
| Samuelson et al. [18] | no better than 0.5 | 18.4 ± 3.2 mmHg | 1.5 ± 0.6 | 0.36 ± 0.23 log MAR | mean reduction in IOP compared with the preoperative unmedicated baseline IOP was 8.4 ± 3.6 mmHg | 0.2 ± 0.6 |
| Craven et al. [19] | 0.75 ± 0.25 | 18.6 ± 3.4 mmHg | 1.6 ± 0,8 | 0.75 ± 0.25 | 17.1 ± 2.9 mmHg | 0.3 ± 0.6 |
| Ahmed et al. [20] | 0.83 | 19.1 ± 3.6 mmHg | 2.7 ± 0.8 | BCVA loss > 2 lines at 12 months, n (%)1 (1.3) | 19.2 ± 2.4 mmHg | Without eye drops |
| Kozera et al. [21] | 0.56 ± 0.23 | 22.04 ± 1.64 mmHg | 1.32 ± 0.55 | 0.95 ± 0.12 | 15.57 ± 2.13 mmHg | 0.32 ± 0.55 |
| Author | Grieshaber et al. [12] n (%) | Grieshaber et al. [13] | Bull et al. [14] n (%) | Matlach et al. [15] n (%) | Rękas et al. [16] n (%) | Fea et al. [17] n (%) | Samuelson et al. [18] n (%) | Craven et al. [19] n (%) | Ahmed et al. [20] n (%) | Kozera et al. [21] n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Complication | |||||||||||
| Stent obstruction | NA | NA | NA | NA | NA | NR | 4 (4%) | 5 (4.3%) | NR | NR | |
| Stent malposition | NA | NA | NA | NA | NA | 2 | 3 (3%) | 3 (2.6%) | 0 | NR | |
| Elevated IOP | 1 (1.67%) | 4 (4.4%) | 6 (5.5%) | 1 (3.4%) | NR | NR | 2 (2%) | 5 (4.3%) | NR | NR | |
| Posterior capsule opacification | NR | NR | NR | NR | NR | NR | 3 (3%) | 7 (6%) | 5% | 4 (9.1%) | |
| Blurry vision or visual disturbance | NR | NR | NR | NR | NR | NR | 1 (1%) | 4 (3.4%) | 1 | NR | |
| Microhyphema | 42 (70%) | 25 (27.8%) | 14 (12.8%) | NR | 10 (34.5%) | NR | NR | NR | NR | 5 (11.4%) | |
| Hyphema | 7 (22.3%) | NR | 6 (5.5%) | NR | 17 (58.0%) | NR | NR | NR | NR | NR | |
| Descemet’s membrane detachment | 2 (3.33%) | 1 (1.1%) | 4 (3.7%) | NR | 1 (3.4%) | NR | NR | NR | NR | NR | |
| Cataract | NR | NR | 17 (19.2%) | NR | NR | NR | NR | NR | 1 | NR | |
| Iritis | NR | NR | NR | 1 (3.4%) | 2 (6.9%) | NR | 1 (1%) | 1 (0.9%) | NR | 1 (2.3%) | |
| Hypotony | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gołaszewska, K.; Konopińska, J.; Obuchowska, I. Evaluation of the Efficacy and Safety of Canaloplasty and iStent Bypass Implantation in Patients with Open-Angle Glaucoma: A Review of the Literature. J. Clin. Med. 2021, 10, 4881. https://doi.org/10.3390/jcm10214881
Gołaszewska K, Konopińska J, Obuchowska I. Evaluation of the Efficacy and Safety of Canaloplasty and iStent Bypass Implantation in Patients with Open-Angle Glaucoma: A Review of the Literature. Journal of Clinical Medicine. 2021; 10(21):4881. https://doi.org/10.3390/jcm10214881
Chicago/Turabian StyleGołaszewska, Kinga, Joanna Konopińska, and Iwona Obuchowska. 2021. "Evaluation of the Efficacy and Safety of Canaloplasty and iStent Bypass Implantation in Patients with Open-Angle Glaucoma: A Review of the Literature" Journal of Clinical Medicine 10, no. 21: 4881. https://doi.org/10.3390/jcm10214881