
Predisposing Factors for Severe Complications after Cataract Surgery: A Nationwide Population-Based Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
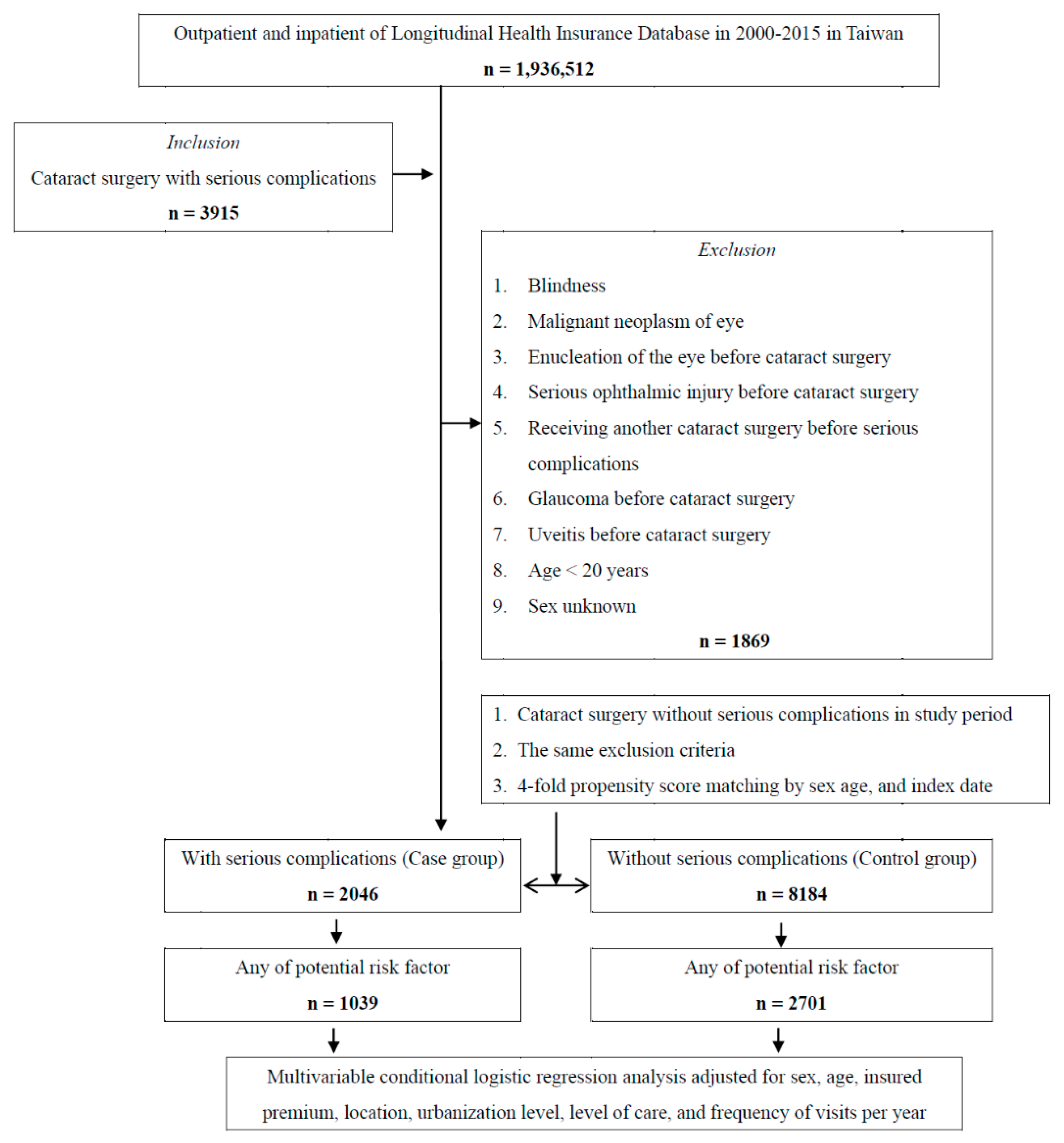
2.2. Study Population
2.3. Outcome Measures
2.4. Statistical Analyses
3. Results
3.1. Subject Characteristics
3.2. Comparisons of Systemic Disease with and without Serious Complications after Cataract Surgery
3.3. Comparisons of Demographic Data with and without Serious Complications after Cataract Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asbell, P.A.; Dualan, I.; Mindel, J.; Brocks, D.; Ahmad, M.; Epstein, S. Age-related cataract. Lancet 2005, 365, 599–609. [Google Scholar] [CrossRef]
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef]
- Tabin, G.; Chen, M.; Espandar, L. Cataract surgery for the developing world. Curr. Opin. Ophthalmol. 2008, 19, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Kumar, D.A. Cost-effectiveness of cataract surgery. Curr. Opin. Ophthalmol. 2011, 22, 15–18. [Google Scholar] [CrossRef]
- Abouzeid, H.; Ferrini, W. Femtosecond-laser assisted cataract surgery: A review. Acta Ophthalmol. 2014, 92, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.W.; Day, A.C.; O’Brart, D.P. Femtosecond laser-assisted cataract surgery: A review. Eur. J. Ophthalmol. 2020, 30, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Pricopie, S.; Istrate, S.; Voinea, L.; Leasu, C.; Paun, V.; Radu, C. Pseudophakic bullous keratopathy. Rom. J. Ophthalmol. 2017, 61, 90–94. [Google Scholar] [CrossRef]
- Han, J.V.; Patel, D.V.; Squirrell, D.; McGhee, C.N. Cystoid macular oedema following cataract surgery: A review. Clin. Exp. Ophthalmol. 2019, 47, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Haug, S.J.; Bhisitkul, R.B. Risk factors for retinal detachment following cataract surgery. Curr. Opin. Ophthalmol. 2012, 23, 7–11. [Google Scholar] [CrossRef]
- Kim, S.H.; Yu, M.H.; Lee, J.H.; Kim, S.W.; Rah, S.H. Endophthalmitis after cataract surgery in korea: A nationwide study evaluating incidence and risk factors in a Korean population. Yonsei Med. J. 2019, 60, 467–473. [Google Scholar] [CrossRef]
- Pérez-Campagne, E.; Basdekidou, C.; Petropoulos, I.K.; Noachovitch, B.; Moubri, M. Impact of preoperative and intraoperative factors in cataract surgery. Klin. Monbl. Augenheilkd. 2013, 230, 326–328. [Google Scholar] [CrossRef]
- Gaskin, G.L.; Pershing, S.; Cole, T.S.; Shah, N.H. Predictive modeling of risk factors and complications of cataract surgery. Eur. J. Ophthalmol. 2016, 26, 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Linton, M.M.; Kempen, J.H. Outcomes of cataract surgery in patients with uveitis: A systematic review and meta-analysis. Am. J. Ophthalmol. 2014, 158, 676–692.e677. [Google Scholar] [CrossRef] [PubMed]
- Grzybowski, A.; Kanclerz, P. Methods for achieving adequate pupil size in cataract surgery. Curr. Opin. Ophthalmol. 2020, 31, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Lara-Smalling, A.; Cakiner-Egilmez, T. Diabetes and cataract surgery: Preoperative risk factors and positive nursing interventions. Insight 2014, 39, 18–20. [Google Scholar]
- Haripriya, A.; Baam, Z.R.; Chang, D.F. Endophthalmitis prophylaxis for cataract surgery. Asia Pac. J. Ophthalmol. Phila 2017, 6, 324–329. [Google Scholar]
- Tuft, S.J.; Minassian, D.; Sullivan, P. Risk factors for retinal detachment after cataract surgery: A case-control study. Ophthalmology 2006, 113, 650–656. [Google Scholar] [CrossRef]
- Peterson, S.R.; Silva, P.A.; Murtha, T.J.; Sun, J.K. Cataract surgery in patients with diabetes: Management strategies. Semin. Ophthalmol. 2018, 33, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Ling, R.; Kamalarajah, S.; Cole, M.; James, C.; Shaw, S. Suprachoroidal haemorrhage complicating cataract surgery in the uk: A case control study of risk factors. Br. J. Ophthalmol. 2004, 88, 474–477. [Google Scholar] [CrossRef] [Green Version]
- Generali, E.; Cantarini, L.; Selmi, C. Ocular involvement in systemic autoimmune diseases. Clin. Rev. Allergy Immunol. 2015, 49, 263–270. [Google Scholar] [CrossRef]
- Lim, C.C.; Lee, C.Y.; Huang, F.C.; Huang, J.Y.; Hung, J.H.; Yang, S.F. Risk of glaucoma in patients receiving hemodialysis and peritoneal dialysis: A nationwide population-based cohort study. Int. J. Environ. Res. Public Health 2020, 17, 6774. [Google Scholar] [CrossRef] [PubMed]
- Poh, S.; Mohamed Abdul, R.B.; Lamoureux, E.L.; Wong, T.Y.; Sabanayagam, C. Metabolic syndrome and eye diseases. Diabetes Res. Clin. Pract. 2016, 113, 86–100. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.A.; Sun, L.M.; Muo, C.H.; Sung, F.C.; Chang, S.N.; Kao, C.H. The analysis of depression and subsequent cancer risk in Taiwan. Cancer Epidemiol. Biomark. Prev. 2011, 20, 473–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, I.C.; Lin, H.C.; Lin, C.C.; Sung, F.C.; Kao, C.H. Tourette syndrome and risk of depression: A population-based cohort study in Taiwan. J. Dev. Behav. Pediatr. 2013, 34, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.L.; Lee, C.H.; Chen, P.S.; Li, Y.H.; Lin, S.J.; Yang, Y.H. Validation of acute myocardial infarction cases in the national health insurance research database in Taiwan. J. Epidemiol. 2014, 24, 500–507. [Google Scholar] [CrossRef] [Green Version]
- Haddad, N.M.; Sun, J.K.; Abujaber, S.; Schlossman, D.K.; Silva, P.S. Cataract surgery and its complications in diabetic patients. Semin. Ophthalmol. 2014, 29, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Nowak, M.S.; Grzybowski, A.; Michalska-Małecka, K.; Szaflik, J.P.; Kozioł, M.; Niemczyk, W.; Grabska-Liberek, I. Incidence and characteristics of endophthalmitis after cataract surgery in Poland, during 2010–2015. Int. J. Environ. Res. Public Health 2019, 16, 2188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltzis, D.; Eleftheriadou, I.; Veves, A. Pathogenesis and treatment of impaired wound healing in diabetes mellitus: New insights. Adv. Ther. 2014, 31, 817–836. [Google Scholar] [CrossRef]
- Akash, M.S.H.; Rehman, K.; Fiayyaz, F.; Sabir, S.; Khurshid, M. Diabetes-associated infections: Development of antimicrobial resistance and possible treatment strategies. Arch. Microbiol. 2020, 202, 953–965. [Google Scholar] [CrossRef]
- Schmidt, M.I.; Duncan, B.B.; Sharrett, A.R.; Lindberg, G.; Savage, P.J.; Offenbacher, S.; Azambuja, M.I.; Tracy, R.P.; Heiss, G. Markers of inflammation and prediction of diabetes mellitus in adults (atherosclerosis risk in communities study): A cohort study. Lancet 1999, 353, 1649–1652. [Google Scholar] [CrossRef]
- Feener, E.P.; King, G.L. Vascular dysfunction in diabetes mellitus. Lancet 1997, 350 (Suppl. 1), SI9–S13. [Google Scholar] [CrossRef]
- Akiboye, F.; Rayman, G. Management of hyperglycemia and diabetes in orthopedic surgery. Curr. Diab Rep. 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holland, R.; Gomes, J.E.F.; Cintra, L.T.A.; Queiroz, Í.O.A.; Estrela, C. Factors affecting the periapical healing process of endodontically treated teeth. J. Appl. Oral. Sci. 2017, 25, 465–476. [Google Scholar] [CrossRef] [Green Version]
- Hurtubise, J.; McLellan, K.; Durr, K.; Onasanya, O.; Nwabuko, D.; Ndisang, J.F. The different facets of dyslipidemia and hypertension in atherosclerosis. Curr. Atheroscler. Rep. 2016, 18, 82. [Google Scholar] [CrossRef]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin. J. Am. Soc. Nephrol 2008, 3, 1526–1533. [Google Scholar] [CrossRef] [Green Version]
- Zhong, J.; Yang, H.C.; Fogo, A.B. A perspective on chronic kidney disease progression. Am. J. Physiol. Ren. Physiol. 2017, 312, F375–F384. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.L.; Wolfe, F.; Huizinga, T.W. Rheumatoid arthritis. Lancet 2010, 376, 1094–1108. [Google Scholar] [CrossRef]
- Bhamra, M.S.; Gondal, I.; Amarnani, A.; Betesh, S.; Zhyvotovska, A.; Scott, W.; Rodriguez-Alvarez, M.; Lazzaro, D.R.; McFarlane, I.M. Ocular manifestations of rheumatoid arthritis: Implications of recent clinical trials. Int. J. Clin. Res. Trials 2019, 4. [Google Scholar] [CrossRef] [Green Version]
- Geyer, O.; Levo, Y. Glaucoma is an autoimmune disease. Autoimmun. Rev. 2020, 19, 102535. [Google Scholar] [CrossRef]
- Scott, M.C.; Winters, M.E. Congestive heart failure. Emerg. Med. Clin. N. Am. 2015, 33, 553–562. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Zheng, J.; Zheng, Q.; Yang, F.; Ye, C.; Woo, D.M.; Jhanji, V.; Chen, W. Incidence and risk factors of new onset endotheliitis after cataract surgery. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5210–5216. [Google Scholar] [CrossRef]
- Grzybowski, A.; Kanclerz, P. Early postoperative intraocular pressure elevation following cataract surgery. Curr. Opin. Ophthalmol. 2019, 30, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Tsirouki, T.; Dastiridou, A.; Symeonidis, C.; Tounakaki, O.; Brazitikou, I.; Kalogeropoulos, C.; Androudi, S. A focus on the epidemiology of uveitis. Ocul. Immunol. Inflamm. 2018, 26, 2–16. [Google Scholar] [CrossRef]
- Jonas, J.B.; Aung, T.; Bourne, R.R.; Bron, A.M.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 390, 2183–2193. [Google Scholar] [CrossRef]
- Samson, S.L.; Garber, A.J. Metabolic syndrome. Endocrinol. Metab. Clin. N. Am. 2014, 43, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Young, C.E.C.; Seibold, L.K.; Kahook, M.Y. Cataract surgery and intraocular pressure in glaucoma. Curr. Opin. Ophthalmol. 2020, 31, 15–22. [Google Scholar] [CrossRef]
- Harbour, J.W.; Rubsamen, P.E.; Palmberg, P. Pars plana vitrectomy in the management of phakic and pseudophakic malignant glaucoma. Arch. Ophthalmol. 1996, 114, 1073–1078. [Google Scholar] [CrossRef]
- Seth, N.G.; Thattaruthody, F.; Jurangal, A.; Pandav, S.S. Late onset pupillary block glaucoma following phacoemulsification with posterior chamber intraocular lens implantation. Eur. J. Ophthalmol. 2020, 30, Np26–Np28. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | Case | Control | p | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | 0.999 | ||||||
| Male | 5620 | 54.94 | 1124 | 54.94 | 4496 | 54.94 | |
| Female | 4610 | 45.06 | 922 | 45.06 | 3688 | 45.06 | |
| Age group (years) | 0.999 | ||||||
| 20–29 | 1295 | 12.66 | 259 | 12.66 | 1036 | 12.66 | |
| 30–39 | 2415 | 23.61 | 483 | 23.61 | 1932 | 23.61 | |
| 40–49 | 2515 | 24.58 | 503 | 24.58 | 2012 | 24.58 | |
| 50–59 | 2125 | 20.77 | 425 | 20.77 | 1700 | 20.77 | |
| 60–69 | 1170 | 11.44 | 234 | 11.44 | 936 | 11.44 | |
| 70–79 | 555 | 5.43 | 111 | 5.43 | 444 | 5.43 | |
| ≧80 | 155 | 1.52 | 31 | 1.52 | 124 | 1.52 | |
| Insured premium (NT$) | 0.304 | ||||||
| <18,000 | 6667 | 65.17 | 1315 | 64.27 | 5352 | 65.40 | |
| 18,000–34,999 | 2516 | 24.59 | 503 | 24.58 | 2013 | 24.60 | |
| ≧35,000 | 1047 | 10.23 | 228 | 11.14 | 819 | 10.01 | |
| Urbanization level | <0.001 * | ||||||
| 1 (Highest) | 3915 | 38.27 | 903 | 44.13 | 3012 | 36.80 | |
| 2 | 3626 | 35.44 | 823 | 40.22 | 2803 | 34.25 | |
| 3 | 1446 | 14.13 | 211 | 10.31 | 1235 | 15.09 | |
| 4 (Lowest) | 1243 | 12.15 | 109 | 5.33 | 1134 | 13.86 | |
| Level of care | <0.001 * | ||||||
| Hospital center | 6145 | 60.07 | 1356 | 66.28 | 4789 | 58.52 | |
| Regional hospital | 2345 | 22.92 | 442 | 21.60 | 1903 | 23.25 | |
| Local hospital | 1740 | 17.01 | 248 | 12.12 | 1492 | 18.23 | |
| Frequency of visits per year | |||||||
| OPD | 4.57 ± 4.26 | 5.86 ± 4.89 | 4.25 ± 4.02 | <0.001 * | |||
| ED | 1.12 ± 1.21 | 1.27 ± 1.34 | 1.08 ± 1.17 | <0.001 * | |||
| IPD | 2.04 ± 1.87 | 2.89 ± 2.76 | 1.83 ± 1.50 | <0.001 * | |||
| Complications | n | % |
|---|---|---|
| Overall | 2046 | |
| Enucleation of the eye | 7 | 0.34 |
| Infectious endophthalmitis | 256 | 12.51 |
| Infectious keratitis | 311 | 15.20 |
| Bullous keratopathy | 241 | 11.78 |
| Perforated corneal ulcer | 32 | 1.56 |
| Hyphema | 35 | 1.71 |
| Glaucoma | 803 | 39.25 |
| Choroidal hemorrhage | 33 | 1.61 |
| Cystoid macular edema | 152 | 7.43 |
| Retinal detachment or defects | 87 | 4.25 |
| Rupture in Descemet’s membrane | 2 | 0.10 |
| Anterior uveitis | 130 | 6.35 |
| Serious Complications | Total | Case | Control | |||
|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % |
| Total | 10,230 | 2046 | 20.00 | 8184 | 80.00 | |
| Any of potential risk factor | ||||||
| Without | 6490 | 63.44 | 1007 | 49.22 | 5483 | 67.00 |
| With | 3740 | 36.56 | 1039 | 50.78 | 2701 | 33.00 |
| HTN | ||||||
| Without | 8321 | 81.34 | 1457 | 71.21 | 6864 | 83.87 |
| With | 1909 | 18.66 | 589 | 28.79 | 1320 | 16.13 |
| DM | ||||||
| Without | 7988 | 78.08 | 1260 | 61.58 | 6728 | 82.21 |
| With | 2242 | 21.92 | 786 | 38.42 | 1456 | 17.79 |
| IHD | ||||||
| Without | 9635 | 94.18 | 1922 | 93.94 | 7713 | 94.24 |
| With | 595 | 5.82 | 124 | 6.06 | 471 | 5.76 |
| Hyperlipidemia | ||||||
| Without | 8888 | 86.88 | 1716 | 83.87 | 7172 | 87.63 |
| With | 1342 | 13.12 | 330 | 16.13 | 1012 | 12.37 |
| CHF | ||||||
| Without | 10,129 | 99.01 | 2010 | 98.24 | 8119 | 99.21 |
| With | 101 | 0.99 | 36 | 1.76 | 65 | 0.79 |
| PVD | ||||||
| Without | 9685 | 94.67 | 1936 | 94.62 | 774 | 94.68 |
| With | 545 | 5.33 | 110 | 5.38 | 435 | 5.32 |
| CVD | ||||||
| Without | 9720 | 95.01 | 1942 | 94.92 | 7778 | 95.04 |
| With | 510 | 4.99 | 104 | 5.08 | 406 | 4.9 |
| Allergic pulmonary disease allergic dermatological disease | ||||||
| Without | 8803 | 86.05 | 1743 | 85.19 | 7060 | 86.27 |
| With | 1427 | 13.95 | 303 | 14.81 | 1124 | 13.73 |
| RD | ||||||
| Without | 10,124 | 98.96 | 2017 | 98.58 | 8107 | 99.06 |
| With | 106 | 1.04 | 29 | 1.42 | 77 | 0.94 |
| ESRD | ||||||
| Without | 9125 | 89.20 | 1647 | 80.50 | 7478 | 91.37 |
| With | 1105 | 10.80 | 399 | 19.50 | 706 | 8.63 |
| Purpura | ||||||
| Without | 10,172 | 99.43 | 2033 | 99.36 | 8139 | 99.45 |
| With | 58 | 0.57 | 13 | 0.64 | 45 | 0.55 |
| Allergic otolaryngologic disease | ||||||
| Without | 9689 | 94.71 | 1935 | 94.57 | 7754 | 94.75 |
| With | 541 | 5.29 | 111 | 5.43 | 430 | 5.25 |
| Allergic dermatological disease | ||||||
| Without | 9807 | 95.87 | 1958 | 95.70 | 7849 | 95.91 |
| With | 42 | 4.13 | 88 | 4.30 | 335 | 4.09 |
| Potential Risk Factors | Adjusted OR | Upper 95% CI | Lower 95% CI | p |
|---|---|---|---|---|
| Any potential risk factor | 2.008 | 1.256 | 2.785 | <0.001 * |
| HTN | 2.329 | 1.459 | 3.345 | <0.001 * |
| DM | 2.818 | 1.761 | 4.011 | <0.001 * |
| IHD | 1.374 | 0.852 | 1.925 | 0.229 |
| Hyperlipidemia | 1.702 | 1.063 | 2.372 | <0.001 * |
| CHF | 2.891 | 1.780 | 4.038 | <0.001 * |
| PVD | 1.310 | 0.811 | 1.835 | 0.305 |
| CVD | 1.337 | 0.824 | 1.856 | 0.297 |
| Allergic pulmonary diseases | 1.406 | 0.875 | 1.927 | 0.233 |
| RD | 1.965 | 1.230 | 2.733 | <0.001 * |
| ESRD | 2.942 | 1.875 | 4.088 | <0.001 * |
| Purpura | 1.503 | 0.921 | 2.096 | 0.165 |
| Allergic otolaryngologic disease | 1.342 | 0.831 | 1.834 | 0.284 |
| Allergic dermatological disease | 1.143 | 0.852 | 1.907 | 0.231 |
| Variables | Adjusted OR | Upper 95% CI | Lower 95% CI | p |
|---|---|---|---|---|
| Sex | ||||
| Male | 1.555 | 0.894 | 2.134 | 0.201 |
| Female | Reference | |||
| Age group (years) | ||||
| 20–29 | Reference | |||
| 30–39 | 1.098 | 0.976 | 1.135 | 0.072 |
| 40–49 | 1.251 | 1.100 | 1.378 | <0.001 * |
| 50–59 | 1.276 | 1.124 | 1.402 | <0.001 * |
| 60–69 | 1.488 | 1.301 | 1.547 | <0.001 * |
| 70–79 | 1.330 | 1.212 | 1.488 | <0.001 * |
| ≥80 | 1.392 | 1.246 | 1.490 | <0.001 * |
| Insured premium (NT$) | ||||
| <18,000 | Reference | |||
| 18,000–34,999 | 0.981 | 0.582 | 1.902 | 0.701 |
| ≥35,000 | 0.875 | 0.443 | 1.804 | 0.652 |
| Urbanization level | ||||
| 1 (highest) | 2.975 | 1.386 | 4.278 | <0.001 * |
| 2 | 2.703 | 1.233 | 3.902 | <0.001 * |
| 3 | 1.835 | 1.014 | 2.801 | 0.036 * |
| 4 (lowest) | Reference | |||
| Level of care | ||||
| Hospital center | 2.896 | 1.268 | 4.065 | <0.001 * |
| Regional hospital | 2.286 | 1.124 | 3.887 | <0.001 * |
| Local hospital | Reference | |||
| Frequency of visits per year | ||||
| OPD | 1.104 | 0.775 | 1.384 | 0.306 |
| ED | 1.156 | 0.894 | 1.422 | 0.227 |
| IPD | 1.277 | 1.043 | 1.356 | 0.003 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, I.-H.; Lee, C.-Y.; Chen, J.-T.; Chen, Y.-H.; Chung, C.-H.; Sun, C.-A.; Chien, W.-C.; Chen, H.-C.; Chen, C.-L. Predisposing Factors for Severe Complications after Cataract Surgery: A Nationwide Population-Based Study. J. Clin. Med. 2021, 10, 3336. https://doi.org/10.3390/jcm10153336
Lin I-H, Lee C-Y, Chen J-T, Chen Y-H, Chung C-H, Sun C-A, Chien W-C, Chen H-C, Chen C-L. Predisposing Factors for Severe Complications after Cataract Surgery: A Nationwide Population-Based Study. Journal of Clinical Medicine. 2021; 10(15):3336. https://doi.org/10.3390/jcm10153336
Chicago/Turabian StyleLin, I-Hung, Chia-Yi Lee, Jiann-Torng Chen, Yi-Hao Chen, Chi-Hsiang Chung, Chien-An Sun, Wu-Chien Chien, Hung-Chi Chen, and Ching-Long Chen. 2021. "Predisposing Factors for Severe Complications after Cataract Surgery: A Nationwide Population-Based Study" Journal of Clinical Medicine 10, no. 15: 3336. https://doi.org/10.3390/jcm10153336