
Is Negative Pressure Wound Therapy with Instillation Suitable for the Treatment of Acute Periprosthetic Hip Joint Infection?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort
2.2. Statistics
3. Results
3.1. Summary of Outcome
3.2. Outcome of Groups One and Two by Endpoint
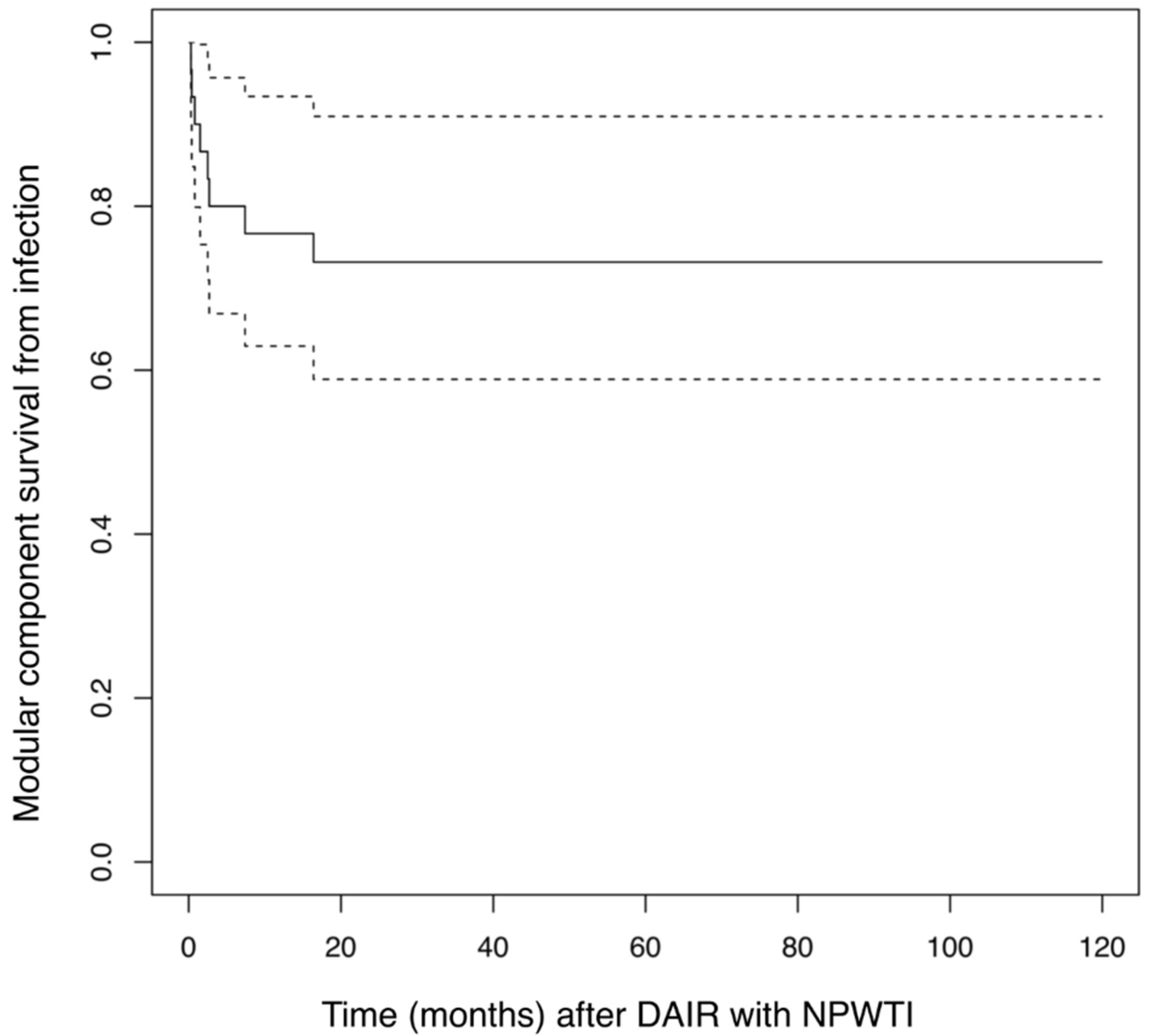
3.3. Kaplan–Maier Analysis of Infection Related Implant Survival
3.4. Organisms Cultured from Tissue Samples
3.5. Postoperative Function Scores
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The epidemiology of revision total hip arthroplasty in the United States. J. Bone Jt. Surg. 2009, 91, 128–133. [Google Scholar] [CrossRef] [PubMed]
- McLawhorn, A.S.; Nawabi, D.H.; Ranawat, A.S. Management of Resistant, Atypical and Culture-negative Periprosthetic Joint Infections after Hip and Knee Arthroplasty. Open Orthop. J. 2016, 10, 615–632. [Google Scholar] [CrossRef]
- Goswami, K.; Parvizi, J.; Maxwell Courtney, P. Current Recommendations for the Diagnosis of Acute and Chronic PJI for Hip and Knee-Cell Counts, Alpha-Defensin, Leukocyte Esterase, Next-generation Sequencing. Curr. Rev. Musculoskelet. Med. 2018, 11, 428–438. [Google Scholar] [CrossRef]
- Hackett, D.J.; Rothenberg, A.C.; Chen, A.F.; Gutowski, C.; Jaekel, D.; Tomek, I.M.; Parsley, B.S.; Ducheyne, P.; Manner, P.A. The economic significance of orthopaedic infections. J. Am. Acad. Orthop. Surg. 2015, 23, S1–S7. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J Arthroplast. 2012, 27, 61–65.e1. [Google Scholar] [CrossRef]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States. J. Bone Jt. Surg. Am. 2015, 97, 1386–1397. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, J.; Ghanem, E.; Azzam, K.; Davis, E.; Jaberi, F.; Hozack, W. Periprosthetic infection: Are current treatment strategies adequate? Acta Orthop. Belg. 2008, 74, 793–800. [Google Scholar] [PubMed]
- Zmistowski, B.; Karam, J.A.; Durinka, J.B.; Casper, D.S.; Parvizi, J. Periprosthetic joint infection increases the risk of one-year mortality. J. Bone Jt. Surg. 2013, 95, 2177–2184. [Google Scholar] [CrossRef] [Green Version]
- Lehner, B.; Omlor, G.W.; Schwarze, M. Periprosthetic joint infections: Latest developments, strategies and treatment algorithms. Orthopade 2020, 49, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetic joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success after treatment of periprosthetic joint infection: A Delphi-based international multidisciplinary consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [Green Version]
- Kunutsor, S.K.; Beswick, A.D.; Whitehouse, M.R.; Wylde, V.; Blom, A.W. Debridement, antibiotics and implant retention for periprosthetic joint infections: A systematic review and meta-analysis of treatment outcomes. J. Infect. 2018, 77, 479–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.S. Management of bone and joint infections due to Staphylococcus aureus. Intern. Med. J. 2005, 35, S79–S96. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Jt. J. 2013, 95, 1450–1452. [Google Scholar] [CrossRef]
- Tsang, S.J.; Ting, J.; Simpson, A.; Gaston, P. Outcomes following debridement, antibiotics and implant retention in the management of periprosthetic infections of the hip: A review of cohort studies. Bone Jt. J. 2017, 99, 1458–1466. [Google Scholar] [CrossRef] [PubMed]
- Grammatopoulos, G.; Kendrick, B.; McNally, M.; Athanasou, N.A.; Atkins, B.; McLardy-Smith, P.; Taylor, A.; Gundle, R. Outcome Following Debridement, Antibiotics, and Implant Retention in Hip Periprosthetic Joint Infection-An 18-Year Experience. J Arthroplast. 2017, 32, 2248–2255. [Google Scholar] [CrossRef]
- Tsukayama, D.T.; Estrada, R.; Gustilo, R.B. Infection after total hip arthroplasty. A study of the treatment of one hundred and six infections. J. Bone Jt. Surg. Am. 1996, 78, 512–523. [Google Scholar] [CrossRef]
- Koyonos, L.; Zmistowski, B.; Della Valle, C.J.; Parvizi, J. Infection control rate of irrigation and debridement for periprosthetic joint infection. Clin. Orthop. Relat. Res. 2011, 469, 3043–3048. [Google Scholar] [CrossRef] [Green Version]
- Sendi, P.; Banderet, F.; Graber, P.; Zimmerli, W. Clinical comparison between exogenous and haematogenous periprosthetic joint infections caused by Staphylococcus aureus. Clin. Microbiol. Infect. 2011, 17, 1098–1100. [Google Scholar] [CrossRef] [Green Version]
- Sukeik, M.; Patel, S.; Haddad, F.S. Aggressive early debridement for treatment of acutely infected cemented total hip arthroplasty. Clin. Orthop. Relat. Res. 2012, 470, 3164–3170. [Google Scholar] [CrossRef] [Green Version]
- Doyle, D.J.; Garmon, E.H. American Society of Anesthesiologists Classification (ASA Class); StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- V.A.C. Instill® therapy—Indications and technical applications. Infection 2009, 37, 1–46.
- V.A.C. Instill therapy—Indications and technical applications. Abstracts of the First V.A.C. Instill Symposium. Heidelberg, Germany. November 21, 2008. Infection 2010, 37, 3–45.
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial biofilms: A common cause of persistent infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.H. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Jt. Surg. Am. 1969, 51, 737–755. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Zahiri, C.A.; Schmalzried, T.P.; Szuszczewicz, E.S.; Amstutz, H.C. Assessing activity in joint replacement patients. J. Arthroplast. 1998, 13, 890–895. [Google Scholar] [CrossRef]
- Tegner, Y.; Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin. Orthop. Relat. Res. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- R Core Team. R: A language and environment for statistical computing. In R Foundation for Statistical Computing; Austria, V., Ed.; R Foundation for Statistical Computing: Vienna, Austria, 2020; ISBN 3-900051-07-0. Available online: https://www.R-project.org/ (accessed on 19 July 2021).
- Bryan, A.J.; Abdel, M.P.; Sanders, T.L.; Fitzgerald, S.F.; Hanssen, A.D.; Berry, D.J. Irrigation and Debridement with Component Retention for Acute Infection After Hip Arthroplasty: Improved Results with Contemporary Management. J. Bone Jt. Surg. Am. 2017, 99, 2011–2018. [Google Scholar] [CrossRef]
- Westberg, M.; Grogaard, B.; Snorrason, F. Early prosthetic joint infections treated with debridement and implant retention: 38 primary hip arthroplasties prospectively recorded and followed for median 4 years. Acta Orthop. 2012, 83, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Lowik, C.A.M.; Parvizi, J.; Jutte, P.C.; Zijlstra, W.P.; Knobben, B.A.S.; Xu, C.; Goswami, K.; Belden, K.A.; Sousa, R.; Carvalho, A.; et al. Debridement, antibiotics and implant retention is a viable treatment option for early periprosthetic joint infection presenting more than four weeks after index arthroplasty. Clin. Infect. Dis. 2019, 71, 630–636. [Google Scholar] [CrossRef]
- Zimmerli, W. Prosthetic Joint Infection: Diagnosis and Treatment. Curr. Infect. Dis. Rep. 2000, 2, 377–379. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, D.; Pigrau, C.; Euba, G.; Cobo, J.; Garcia-Lechuz, J.; Palomino, J.; Riera, M.; del Toro, M.D.; Granados, A.; Ariza, X.; et al. Acute haematogenous prosthetic joint infection: Prospective evaluation of medical and surgical management. Clin. Microbiol. Infect. 2010, 16, 1789–1795. [Google Scholar] [CrossRef] [PubMed]
- Fink, B.; Schuster, P.; Schwenninger, C.; Frommelt, L.; Oremek, D. A Standardized Regimen for the Treatment of Acute Postoperative Infections and Acute Hematogenous Infections Associated With Hip and Knee Arthroplasties. J. Arthroplast. 2017, 32, 1255–1261. [Google Scholar] [CrossRef]
- Kuiper, J.W.; Willink, R.T.; Moojen, D.J.; van den Bekerom, M.P.; Colen, S. Treatment of acute periprosthetic infections with prosthesis retention: Review of current concepts. World J. Orthop. 2014, 5, 667–676. [Google Scholar] [CrossRef]
- Fehring, T.K.; Odum, S.M.; Berend, K.R.; Jiranek, W.A.; Parvizi, J.; Bozic, K.J.; Della Valle, C.J.; Gioe, T.J. Failure of irrigation and debridement for early postoperative periprosthetic infection. Clin. Orthop. Relat. Res. 2013, 471, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Sousa, R.; Abreu, M.A. Treatment of Prosthetic Joint Infection with Debridement, Antibiotics and Irrigation with Implant Retention—A Narrative Review. J. Bone Jt. Infect. 2018, 3, 108–117. [Google Scholar] [CrossRef] [Green Version]
- Triantafyllopoulos, G.K.; Poultsides, L.A.; Zhang, W.; Sculco, P.K.; Ma, Y.; Sculco, T.P. Periprosthetic knee infections treated with irrigation and debridement: Outcomes and preoperative predictive factors. J Arthroplast. 2015, 30, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Zaruta, D.A.; Qiu, B.; Liu, A.Y.; Ricciardi, B.F. Indications and Guidelines for Debridement and Implant Retention for Periprosthetic Hip and Knee Infection. Curr. Rev. Musculoskelet. Med. 2018, 11, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Mooney, J.A.; Pridgen, E.M.; Manasherob, R.; Suh, G.; Blackwell, H.E.; Barron, A.E.; Bollyky, P.L.; Goodman, S.B.; Amanatullah, D.F. Periprosthetic bacterial biofilm and quorum sensing. J. Orthop. Res. 2018, 36, 2331–2339. [Google Scholar] [CrossRef]
- Gbejuade, H.O.; Lovering, A.M.; Webb, J.C. The role of microbial biofilms in prosthetic joint infections. Acta Orthop. 2015, 86, 147–158. [Google Scholar] [CrossRef]
- Donlan, R.M.; Costerton, J.W. Biofilms: Survival mechanisms of clinically relevant microorganisms. Clin. Microbiol. Rev. 2002, 15, 167–193. [Google Scholar] [CrossRef] [Green Version]
- Marić, S.; Vranes, J. Characteristics and significance of microbial biofilm formation. Periodicum. Biologorum. 2007, 109, 115–121. [Google Scholar]
- Arnold, W.V.; Shirtliff, M.E.; Stoodley, P. Bacterial biofilms and periprosthetic infections. J. Bone Jt. Surg. Am. 2013, 95, 2223–2229. [Google Scholar]
- Krasowski, G.; Junka, A.; Paleczny, J.; Czajkowska, J.; Makomaska-Szaroszyk, E.; Chodaczek, G.; Majkowski, M.; Migdał, P.; Fijałkowski, K.; Kowalska-Krochmal, B.; et al. In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens. Membranes 2021, 11, 62. [Google Scholar] [CrossRef]
- Lora-Tamayo, J.; Murillo, O.; Iribarren, J.A.; Soriano, A.; Sanchez-Somolinos, M.; Baraia-Etxaburu, J.M.; Rico, A.; Palomino, J.; Rodríguez-Pardo, D.; Horcajada, J.P.; et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin. Infect. Dis. 2013, 56, 182–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tornero, E.; Morata, L.; Martinez-Pastor, J.C.; Angulo, S.; Combalia, A.; Bori, G.; García-Ramiro, S.; Bosch, J.; Mensa, J.; Soriano, A. Importance of selection and duration of antibiotic regimen in prosthetic joint infections treated with debridement and implant retention. J. Antimicrob. Chemother. 2016, 71, 1395–1401. [Google Scholar] [PubMed] [Green Version]
- Byren, I.; Bejon, P.; Atkins, B.L.; Angus, B.; Masters, S.; McLardy-Smith, P.; Gundle, R.; Berendt, A. One hundred and twelve infected arthroplasties treated with ‘DAIR’ (debridement, antibiotics and implant retention): Antibiotic duration and outcome. J. Antimicrob. Chemother. 2009, 63, 1264–1271. [Google Scholar] [CrossRef] [Green Version]
- Hirsiger, S.; Betz, M.; Stafylakis, D.; Gotschi, T.; Lew, D.; Uckay, I. The Benefice of Mobile Parts’ Exchange in the Management of Infected Total Joint Arthroplasties with Prosthesis Retention (DAIR Procedure). J. Clin. Med. 2019, 8, 226. [Google Scholar] [CrossRef] [Green Version]
- Crockarell, J.R.; Hanssen, A.D.; Osmon, D.R.; Morrey, B.F. Treatment of infection with debridement and retention of the components following hip arthroplasty. J. Bone Jt. Surg. Am. 1998, 80, 1306–1313. [Google Scholar] [CrossRef]
- Trampuz, A.; Widmer, A.F. Infections associated with orthopedic implants. Curr. Opin. Infect. Dis. 2006, 19, 349–356. [Google Scholar] [CrossRef]
- Klouche, S.; Lhotellier, L.; Mamoudy, P. Infected total hip arthroplasty treated by an irrigation-debridement/component retention protocol. A prospective study in a 12-case series with minimum 2 years’ follow-up. Orthop. Traumatol. Surg. Res. 2011, 97, 134–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, R.S.; Paxton, L.; Fithian, D.C.; Stone, M.L. Obesity and perioperative morbidity in total hip and total knee arthroplasty patients. J. Arthroplast. 2005, 20, 46–50. [Google Scholar] [CrossRef]
- Veltman, E.S.; Moojen, D.J.F.; Nelissen, R.G.; Poolman, R.W. Antibiotic Prophylaxis and DAIR Treatment in Primary Total Hip and Knee Arthroplasty, A National Survey in The Netherlands. J. Bone Jt. Infect. 2018, 3, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Estes, C.S.; Beauchamp, C.P.; Clarke, H.D.; Spangehl, M.J. A two-stage retention debridement protocol for acute periprosthetic joint infections. Clin. Orthop. Relat. Res. 2010, 468, 2029–2038. [Google Scholar] [CrossRef] [Green Version]
- Romano, C.; Logoluso, N.; Drago, L.; Peccati, A.; Romano, D. Role for irrigation and debridement in periprosthetic infections. J. Knee Surg. 2014, 27, 267–272. [Google Scholar]
- Romano, C.L.; Manzi, G.; Logoluso, N.; Romano, D. Value of debridement and irrigation for the treatment of peri-prosthetic infections. A systematic review. Hip Int. 2012, 22, S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Aboltins, C.; Dowsey, M.M.; Peel, T.; Lim, W.K.; Parikh, S.; Stanley, P.; Choong, P.F. Early prosthetic hip joint infection treated with debridement, prosthesis retention and biofilm-active antibiotics: Functional outcomes, quality of life and complications. Intern. Med. J. 2013, 43, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Azzam, K.A.; Seeley, M.; Ghanem, E.; Austin, M.S.; Purtill, J.J.; Parvizi, J. Irrigation and debridement in the management of prosthetic joint infection: Traditional indications revisited. J. Arthroplast. 2010, 25, 1022–1027. [Google Scholar] [CrossRef]
- Van Kleunen, J.P.; Knox, D.; Garino, J.P.; Lee, G.C. Irrigation and debridement and prosthesis retention for treating acute periprosthetic infections. Clin. Orthop. Relat. Res. 2010, 468, 2024–2028. [Google Scholar] [CrossRef] [Green Version]
- Moojen, D.J.; Zwiers, J.H.; Scholtes, V.A.; Verheyen, C.C.; Poolman, R.W. Similar success rates for single and multiple debridement surgery for acute hip arthroplasty infection. Acta Orthop. 2014, 85, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Gardner, J.; Gioe, T.J.; Tatman, P. Can this prosthesis be saved? Implant salvage attempts in infected primary TKA. Clin. Orthop. Relat. Res. 2011, 469, 970–976. [Google Scholar] [CrossRef] [Green Version]
- Sherrell, J.C.; Fehring, T.K.; Odum, S.; Hansen, E.; Zmistowski, B.; Dennos, A.; Kalore, N. The Chitranjan Ranawat Award: Fate of two-stage reimplantation after failed irrigation and debridement for periprosthetic knee infection. Clin. Orthop. Relat. Res. 2011, 469, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Nodzo, S.R.; Boyle, K.K.; Nocon, A.A.; Henry, M.W.; Mayman, D.J.; Westrich, G.H. The Influence of a Failed Irrigation and Debridement on the Outcomes of a Subsequent 2-Stage Revision Knee Arthroplasty. J. Arthroplast. 2017, 32, 2508–2512. [Google Scholar] [CrossRef]
- Brimmo, O.; Ramanathan, D.; Schiltz, N.K.; Pillai, A.L.; Klika, A.K.; Barsoum, W.K. Irrigation and Debridement Before a 2-Stage Revision Total Knee Arthroplasty Does Not Increase Risk of Failure. J. Arthroplast. 2016, 31, 461–464. [Google Scholar] [CrossRef] [Green Version]
- Lehner, B.; Fleischmann, W.; Becker, R.; Jukema, G.N. First experiences with negative pressure wound therapy and instillation in the treatment of infected orthopaedic implants: A clinical observational study. Int. Orthop. 2011, 35, 1415–1420. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Moser, C.; Wang, H.Z.; Hoiby, N.; Song, Z.J. Strategies for combating bacterial biofilm infections. Int. J. Oral. Sci. 2015, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- McConoughey, S.J.; Howlin, R.; Granger, J.F.; Manring, M.M.; Calhoun, J.H.; Shirtliff, M.; Kathju, S.; Stoodley, P. Biofilms in periprosthetic orthopedic infections. Future Microbiol. 2014, 9, 987–1007. [Google Scholar] [CrossRef] [Green Version]
- Brandt, C.M.; Sistrunk, W.W.; Duffy, M.C.; Hanssen, A.D.; Steckelberg, J.M.; Ilstrup, D.M.; Osmon, D.R. Staphylococcus aureus prosthetic joint infection treated with debridement and prosthesis retention. Clin. Infect. Dis. 1997, 24, 914–919. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Procedure | Indication | Number (n) | |
|---|---|---|---|
| Primary Index Operation | Idiopathic Osteoarthritis | 15 | hips |
| Osteoarthritis secondary to hip dysplasia | 5 | hips | |
| Osteoarthritis secondary to trauma | 1 | hip | |
| Revision Index Operation | Liner wear | 1 | hip |
| Dislocation | 3 | hips | |
| Metallosis | 1 | hip | |
| Loosening of femoral shaft | 1 | hip | |
| Loosening of acetabular cup | 1 | hip | |
| Pseudarthrosis after periprosthetic fracture | 1 | hip | |
| THA Reimplantation after Girdlestone | 2 | hips | |
| Outcome | Group I (19 Hips) | Group II (12 Hips) | Total (31 Hips) |
|---|---|---|---|
| Infection eliminated with no further surgery for infection (B + E) | 13 (68%) | 9 (75%) | 22 (71.0%) |
| Infection related implant survival (B + E + I) | 14 (73.6%) | 9 (75%) | 23 (74.2%) |
| Implant survival from all causes (B + I) | 14 (73.6%) | 8 (66.7%) | 22 (71.0%) |
| Organism(s) Isolated | Total # Isolated | Monomicrobial | Polymicrobial |
|---|---|---|---|
| Staph. Aureus | 6 | 3 | 3 |
| MRSA | 1 | 1 | 0 |
| Coagulase Negative Staphylococcus Epidermidis | 5 | 2 | 3 |
| Coagulase Negative Staphylococcus Hominis | 1 | 1 | 0 |
| Coagulase Negative Staphylococcus lugdunesis | 2 | 1 | 1 |
| Coagulase Negative Unspecified | 2 | 0 | 2 |
| Streptococcus non-Haemolytic | 6 | 5 | 1 |
| Haemolytic Group G | 1 | 1 | 0 |
| Enterococcus | 3 | 2 | 1 |
| Enterobacter | 2 | 1 | 1 |
| Escherichia coli | 3 | 1 | 2 |
| Miscellaneous/other | 4 | 0 | 4 |
| Culture negative | 4 |
| Post-Operative Scores | Mean ± Standard Deviation | Median | Range | Interquartile Range |
|---|---|---|---|---|
| Harris Hip Score | 81.1 ± 11.8 | 52–95 | 73.5–91.5 | |
| WOMAC | 33.3 ± 20.1 | 2.1–67.7 | 12.0–46.4 | |
| Pain (VAS) (0–10) | 1 | 0–5 | 0–2 | |
| Satisfaction (1–5) | 2 | 1–5 | 2–3.5 | |
| Activity (UCLA) (1–10 Scale) | 5 | 2–8 | 3–6 | |
| Activity (Tegner) (0–10 scale) | 3 | 1–4 | 2–3 |
| Author | Year | # of Acute PJI of Hip | Follow Up Months | Primary, p. Revision, R | Success | Modular Exchange | Long-Term Antibiotics |
|---|---|---|---|---|---|---|---|
| Crockarel | 1998 | 23 | 75 | p = 20; R = 3 | 26% | 0% | No |
| Westberg | 2012 | 38 | 48 | p = 38 | 71% | 100% | No |
| Sukeik | 2012 | 26 | 79 | p = 16, R = 10 | 77% | 100% | No |
| Triantafyllopoulos | 2015 | 60 | 59 | p = 38, R = 22 | 79% | 100% | No |
| Grammatopoulos | 2017 | 122 | 84 | p = 82, R = 40 | 85% | 53% | Yes |
| Bryan | 2017 | 90 | 72 | p = 90 | 83% | 70% | Yes |
| Beckmann | 2021 | 31 | 52 | p = 21, R = 10 | 74.2% | 100% | No |
| Author | Year | # of Acute PJI of Hip | Follow Up Months | Primary, p. Revision, R | Success | Modular Exchange |
|---|---|---|---|---|---|---|
| Tsukayama | 1996 | 41 | 45 | Unknown | 68% | 100% |
| Klouche | 2011 | 12 | 40 | p = 6, R = 6 | 75% | 40% |
| Beckmann | 2021 | 31 | 52 | p = 21, R = 10 | 71% | 200% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beckmann, N.A.; Hanslmeier, M.G.; Omlor, G.W.; Feisst, M.; Maier, M.W.; Lehner, B. Is Negative Pressure Wound Therapy with Instillation Suitable for the Treatment of Acute Periprosthetic Hip Joint Infection? J. Clin. Med. 2021, 10, 3246. https://doi.org/10.3390/jcm10153246
Beckmann NA, Hanslmeier MG, Omlor GW, Feisst M, Maier MW, Lehner B. Is Negative Pressure Wound Therapy with Instillation Suitable for the Treatment of Acute Periprosthetic Hip Joint Infection? Journal of Clinical Medicine. 2021; 10(15):3246. https://doi.org/10.3390/jcm10153246
Chicago/Turabian StyleBeckmann, Nicholas A., Maximilian G. Hanslmeier, Georg W. Omlor, Manuel Feisst, Michael W. Maier, and Burkhard Lehner. 2021. "Is Negative Pressure Wound Therapy with Instillation Suitable for the Treatment of Acute Periprosthetic Hip Joint Infection?" Journal of Clinical Medicine 10, no. 15: 3246. https://doi.org/10.3390/jcm10153246