
Prospective Evaluation of Resection Margins Using Standardized Specimen Protocol Analysis among Patients with Distal Cholangiocarcinoma and Pancreatic Ductal Adenocarcinoma

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. Surgery and Specimen Management
3. PDAC, Pancreatic Ductal Adenocarcinoma
3.1. Pathologic Analysis and Margin Assessment
3.2. Study Parameters
3.3. Statistical Analysis
4. Results
4.1. Patient Characteristics, Surgery, and Postoperative Courses
4.2. Pathological Data
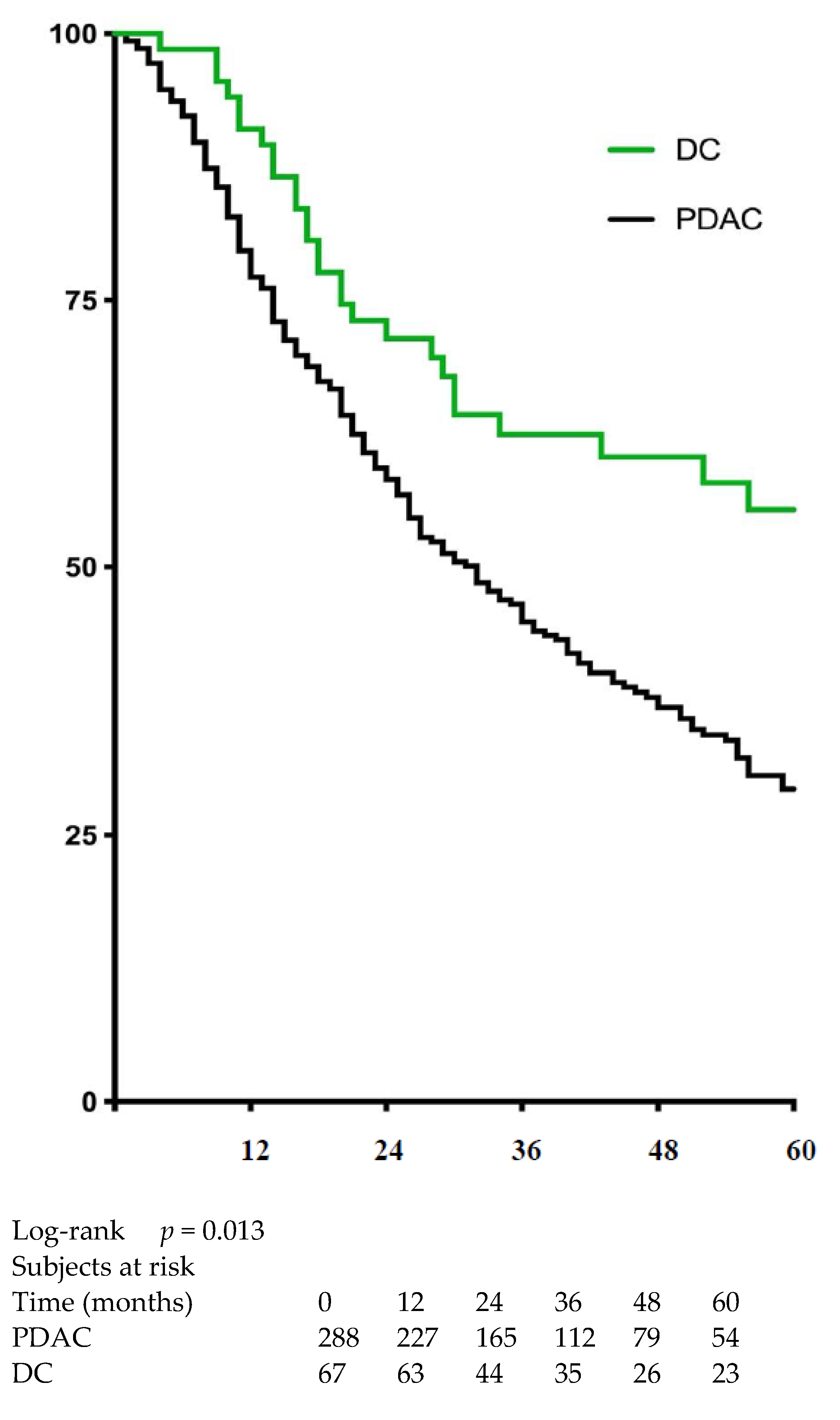
4.3. Impact of Resection Margin on Survival
5. Discussion
5.1. Patient Characteristics, Surgery, and Postoperative Course
5.2. Pathologic Data
5.3. Survival
5.4. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ethun, C.G.; Lopez-Aguiar, A.G.; Pawlik, T.M.; Poultsides, G.; Idrees, K.; Fields, R.C.; Maithel, S.K.; Weber, S.M.; Cho, C.; Martin, R.C.; et al. Distal cholangiocarcinoma and pancreas adenocarcinoma: Are they really the same disease? A 13-institution study from the US extrahepatic biliary malignancy consortium and the central pancreas consortium. J. Am. Coll. Surg. 2017, 224, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Pathologists. Standards and Minimum Datasets for Reporting Cancers: Dataset for the Histopathological Reporting of Carcinomas of the Pancreas, Ampulla of Vater and Common Bile Duct; Royal College of Pathologists: London, UK, 2010. [Google Scholar]
- Royal College of Pathologists. Dataset for Histopathological Reporting of Carcinomas of the Pancreas, Ampulla of Vater and Common Bile Duct; Royal College of Pathologists: London, UK, 2019. [Google Scholar]
- Rau, B.M.; Moritz, K.; Schuschan, S.; Alsfasser, G.; Prall, F.; Klar, E. R1 resection in pancreatic cancer has significant impact on long-term outcome in standardized pathology modified for routine use. Surgery 2012, 152, S103–S111. [Google Scholar] [CrossRef]
- Delpero, J.R.; Jeune, F.; Bachellier, P.; Regenet, N.; Le Treut, Y.P.; Paye, F.; Carrere, N.; Sauvanet, A.; Adham, M.; Autret, A.; et al. Prognostic value of resection margin involvement after pancreaticoduodenectomy for ductal adenocarcinoma: Updates from a French prospective multicentre study. Ann. Surg. 2017, 266, 787–796. [Google Scholar] [CrossRef]
- Kamposioras, K.; Anthoney, A.; Fernandez Moro, C.; Cairns, A.; Smith, A.M.; Liaskos, C.; Verbeke, C.S. Impact of intrapancreatic or extrapancreatic bile duct involvement on survival following pancreatoduodenectomy for common bile duct cancer. Br. J. Surg. 2014, 101, 89–99. [Google Scholar] [CrossRef]
- Marchese, U.; Ewald, J.; Gilabert, M.; Delpero, J.R.; Turrini, O. Outcomes of pancreatic adenocarcinoma that was not resected because of isolated para-aortic lymph node involvement. J. Visc. Surg. 2019, 156, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Al Faraï, A.; Garnier, J.; Ewald, J.; Marchese, U.; Gilabert, M.; Moureau-Zabotto, L.; Turrini, O.; Poizat, F.; Giovannini, M.; Delpero, J.-R. International study group of pancreatic surgery type 3 and 4 venous resections in patients with pancreatic adenocarcinoma: The paoli-calmettes institute experience. Eur. J. Surg. Oncol. 2019, 45, 1912–1918. [Google Scholar] [CrossRef] [PubMed]
- Van Roessel, S.; Kasumova, G.G.; Tabatabaie, O.; Ng, S.C.; van Rijssen, L.B.; Verheij, J.; Tseng, J.F.; Najarian, R.M.; van Gulik, T.M.; Besselink, M.G. Pathological margin clearance and survival after pancreaticoduodenectomy in a US and European pancreatic center. Ann. Surg. Oncol. 2018, 25, 1760–1767. [Google Scholar] [CrossRef]
- Chang, D.K.; Johns, A.L.; Merrett, N.D.; Gill, A.J.; Colvin, E.K.; Nguyen, C.J.S.Q.; Leong, R.W.L.; Cosman, P.H.; Kelly, M.I.; Sutherland, R.L.; et al. Margin clearance and outcome in resected pancreatic cancer. J. Clin. Oncol. 2009, 27, 2855–2862. [Google Scholar] [CrossRef]
- Kooby, D.A.; Lad, N.L.; Squires, M.H., III; Maithel, S.K.; Sarmiento, J.M.; Staley, C.A.; Merchant, N.B.; Volkan Adsay, N.; El-Rayes, B.F.; Weber, S.M.; et al. Value of intraoperative neck margin analysis during whipple for pancreatic adenocarcinoma: A multicenter analysis of 1399 patients. Ann. Surg. 2014, 260, 494–503. [Google Scholar] [CrossRef]
- Park, Y.; Hwang, D.W.; Kim, J.H.; Hong, S.-M.; Jun, S.-Y.; Lee, J.H.; Song, K.B.; Jun, E.S.; Kim, S.C.; Park, K.-M.; et al. Prognostic comparison of the longitudinal margin status in distal bile duct cancer: R0 on first bile duct resection versus R0 after additional resection. J. Hepato-Biliary-Pancreat Sci. 2019, 26, 169–178. [Google Scholar] [CrossRef]
- Zhang, B.; Lee, G.C.; Qadan, M.; Fong, Z.V.; Mino-Kenudson, M.; Desphande, V.; Fernández-del Castillo, C.; Giuseppe, M.; Laura, M.; Giovanni, M.; et al. Revision of pancreatic neck margins based on intraoperative frozen section analysis is associated with improved survival in patients undergoing pancreatectomy for ductal adenocarcinoma. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Dervenis, C.; Butturini, G.; Fingerhut, A.; Yeo, C.; Izbicki, J.; Neoptolemos, J.; Sarr, M.; Traverso, W.; Buchler, M.; et al. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005, 138, 8–13. [Google Scholar] [CrossRef]
- Farges, O.; Bendersky, N.; Truant, S.; Delpero, J.R.; Pruvot, F.R.; Sauvanet, A. The theory and practice of pancreatic surgery in France. Ann. Surg. 2017, 266, 797–804. [Google Scholar] [CrossRef]
- Sheetz, K.H.; Dimick, J.B.; Nathan, H. Centralization of high-risk cancer surgery within existing hospital systems. J. Clin. Oncol. 2019, 37, 3234–3242. [Google Scholar] [CrossRef] [PubMed]
- Kleive, D.; Labori, K.J.; Line, P.D.; Gladhaug, I.P.; Verbeke, C.S. Pancreatoduodenectomy with venous resection for ductal adenocarcinoma rarely achieves complete (R0) resection. HPB 2020, 22, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Takenami, T.; Maeda, S.; Karasawa, H.; Suzuki, T.; Furukawa, T.; Morikawa, T.; Takadate, T.; Hayashi, H.; Nakagawa, K.; Motoi, F.; et al. Novel biomarkers distinguishing pancreatic head cancer from distal cholangiocarcinoma based on proteomic analysis. BMC Cancer 2019, 19, 318. [Google Scholar] [CrossRef] [Green Version]
- Schmuck, R.B.; Brokat, C.; Andreou, A.; Felsenstein, M.; Klein, F.; Sinn, B.; Pratschke, J.; Bahra, M. Clinicopathological stratification and long-term follow-up of patients with periampullary carcinomas. Anticancer Res. 2018, 38, 5379–5386. [Google Scholar] [CrossRef]
- Li, X.; Lin, H.; Sun, Y.; Gong, J.; Feng, H.; Tu, J. Prognostic significance of the lymph node ratio in surgical patients with distal cholangiocarcinoma. J. Surg. Res. 2019, 236, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Bolm, L.; Petrova, E.; Weitz, J.; Rückert, F.; Wittel, U.A.; Makowiec, F.; Lapshyn, H.; Bronsert, P.; Rau, B.M.; Khatkov, I.E. Prognostic relevance of preoperative bilirubin-adjusted serum carbohydrate antigen 19-9 in a multicenter subset analysis of 179 patients with distal cholangiocarcinoma. HPB 2019, 21, 1513–1519. [Google Scholar] [CrossRef]
- Hoshimoto, S.; Hishinuma, S.; Shirakawa, H.; Tomikawa, M.; Ozawa, I.; Ogata, Y. Association of preoperative platelet-to-lymphocyte ratio with poor outcome in patients with distal cholangiocarcinoma. Oncology 2019, 96, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Wellner, U.F.; Shen, Y.; Keck, T.; Jin, W.; Xu, Z. The survival outcome and prognostic factors for distal cholangiocarcinoma following surgical resection: A meta-analysis for the 5-year survival. Surg. Today 2017, 47, 271–279. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PDAC | DC | p-Value | |
|---|---|---|---|
| N | 288 | 67 | - |
| Sex ratio (M/F) | 0.97 | 1.8 | 0.028 |
| Median age (range) | 65 (29–86) | 68 (52–81) | 0.033 |
| Mean BMI (±SD) | 24.1 (±4.03) | 24.3(±4.23) | 0.81 |
| Mean serum CA 19-9 level a (UI) (±SD) | 438 (±1056) | 164 (±365) | 0.13 |
| Biliary stenting (%) | 220 (77) | 62 (93) | <0.01 |
| Neoadjuvant treatment (%) | 123 (43) | 3 (4.5) | <0.001 |
| Total pancreatectomy (%) | 25 (8.7) | 2 (3) | 0.11 |
| Vascular resection (%) | |||
| Venous resection | 112 (39) | 10 (15) | <0.001 |
| Arterial resection | 16 (5.6) | 2 (3) | 0.54 |
| Enlarged resection (%) | 8 (2.8) | 2 (3) | 1 |
| Perioperative RBC transfusion (%) | 68 (24) | 24 (36) | 0.04 |
| Reintervention (%) | 19 (6.6) | 3 (4.5) | 0.78 |
| Morbidity rate (%) | |||
| Overall | 142 (49) | 34 (51) | 0.83 |
| Clavien–Dindo grade 3–5 | 32 (11) | 13 (19) | 0.07 |
| Mortality rate (%) | |||
| 30-day | 5 (1.7) | 1 (1.5) | 1 |
| 90-day | 7 (2.4) | 1 (1.5) | 1 |
| Postoperative pancreatic fistula b (%) | 52 (20) | 27 (42) | <0.001 |
| Biliary fistula (%) | 5 (1.7) | 1 (1.5) | 1 |
| Hemorrhage (%) | 17 (5.9) | 5 (7.5) | 0.58 |
| Median length of hospital stays (days) (range) | 18 (8–83) | 19 (10–41) | 0.12 |
| Adjuvant treatment (%) | 195 (68) | 38 (57) | 0.63 |
| PDAC | DC | p-Value | |
|---|---|---|---|
| Mean tumor size (mm) (±SD) | 28.6 (±13.2) | 24 (±12.4) | <0.01 |
| T 3/4 stage (%) | 185 (64) | 39 (58) | 0.36 |
| Median number of examined lymph nodes (range) | 16 (2–42) | 15 (5–33) | 0.4 |
| Lymph node invasion (N+) (%) | 186 (65) | 40 (60) | 0.45 |
| Perineural invasion (%) | 210 (73) | 54 (81) | 0.19 |
| Lymphovascular invasion (%) | 151 (52) | 34 (51) | 0.89 |
| Carcinoma differentiation grade (%) | |||
| Low | 35 (12) | 10 (15) | 0.66 |
| Intermediate | 134 (47) | 33 (49) | |
| High | 119 (41) | 24 (36) | |
| Final positive pancreatic neck margin a (%) | 11 (3.8) | 4 (6.2) | 0.5 |
| Final positive biliary transection margin (%) | 8 (4.2) | 4 (6) | 0.25 |
| R1 resection on inked margin (%) | |||
| 0 mm clearance | 33 (11.5) | 5 (7.5) | 0.5 |
| <1 mm clearance b | 109 (38) | 20 (30) | 0.22 |
| <1.5 mm clearance | 142 (49.3) | 25 (37.3) | 0.08 |
| Location of R1 margin (%) | |||
| Venous margin | 67 (23) | 11 (16) | 0.22 |
| Arterial margin | 36 (12) | 7 (10) | 0.64 |
| Retroperitoneal margin | 52 (18) | 10 (15) | 0.54 |
| Mean (mm) (±SD)/median (mm) margin clearance | |||
| Venous margin | 3.57 (±3.99)/6 | 7.74 (±6.6)/2 | <0.001 |
| Arterial margin | 5.03 (±4.7)/7 | 8.74 (±6.86)/4 | <0.001 |
| Retroperitoneal margin | 5.37 (±5.6)/5 | 6.79 (±6.14)/4 | 0.09 |
| Number of involved inked-margins (%) | |||
| 1 | 63 (22) | 13 (19) | 0.66 |
| 2 | 39 (14) | 6 (9) | 0.31 |
| 3 | 7 (2.4) | 1 (1.5) | 1 |
| Univariate p-Value | OR (95% CI) | Multivariate p-Value | |
|---|---|---|---|
| Neoadjuvant treatment | |||
| PDAC | 0.47 | 1.68 (1.14–2.48) | <0.01 |
| DC | 0.24 | - | - |
| Perioperative RBC transfusion | |||
| PDAC | 0.016 | 1.68 (1.12–2.51) | 0.011 |
| DC | 0.48 | - | - |
| Adjuvant treatment | |||
| PDAC | 0.01 | 0.533 (0.366–0.778) | <0.001 |
| DC | 0.57 | - | - |
| T 3/4 stage | |||
| PDAC | <0.001 | 4.47 (2.65–7.55) | <0.001 |
| DC | <0.001 | 4.45 (1.44–13.8) | <0.01 |
| Lymph node invasion (N+) | |||
| PDAC | <0.001 | 2.35 (1.41–3.90) | <0.01 |
| DC | 0.013 | 2.06 (0.687–6.18) | 0.2 |
| Perineural invasion | |||
| PDAC | <0.001 | 1.69 (1.00–2.85) | 0.049 |
| DC | 0.026 | 3.38 (0.737–15.5) | 0.12 |
| Differentiation grade | |||
| Low vs intermediate PDAC | <0.01 | 0.704 (0.401–1.23) | 0.22 |
| Low vs. high PDAC | 0.6 | 0.551 (0.304–0.997) | 0.049 |
| DC | - | - | - |
| R1 resection inked-margin (1 mm clearance) | |||
| PDAC | <0.01 | 0.889 (0.496–1.59) | 0.69 |
| DC | 0.22 | - | - |
| Venous location of R1 margin | |||
| PDAC | <0.001 | 1.70 (0.974–2.98) | 0.062 |
| DC | 0.38 | - | - |
| Bile duct location of R1 margin | |||
| PDAC | 0.069 | - | - |
| DC | 0.024 | 2.91 (0.628–13.5) | 0.17 |
| Number of involved inked-margins | |||
| 2 in PDAC | <0.001 | 1.45 (0.866–2.43) | 0.16 |
| 3 in PDAC | 0.22 | 2.57 (0.967–6.80) | 0.058 |
| 2 in DC | 0.071 | - | - |
| 3 in DC | 0.46 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garnier, J.; Ewald, J.; Poizat, F.; Traversari, E.; Marchese, U.; Palen, A.; Delpero, J.R.; Turrini, O. Prospective Evaluation of Resection Margins Using Standardized Specimen Protocol Analysis among Patients with Distal Cholangiocarcinoma and Pancreatic Ductal Adenocarcinoma. J. Clin. Med. 2021, 10, 3247. https://doi.org/10.3390/jcm10153247
Garnier J, Ewald J, Poizat F, Traversari E, Marchese U, Palen A, Delpero JR, Turrini O. Prospective Evaluation of Resection Margins Using Standardized Specimen Protocol Analysis among Patients with Distal Cholangiocarcinoma and Pancreatic Ductal Adenocarcinoma. Journal of Clinical Medicine. 2021; 10(15):3247. https://doi.org/10.3390/jcm10153247
Chicago/Turabian StyleGarnier, Jonathan, Jacques Ewald, Flora Poizat, Eddy Traversari, Ugo Marchese, Anais Palen, Jean Robert Delpero, and Olivier Turrini. 2021. "Prospective Evaluation of Resection Margins Using Standardized Specimen Protocol Analysis among Patients with Distal Cholangiocarcinoma and Pancreatic Ductal Adenocarcinoma" Journal of Clinical Medicine 10, no. 15: 3247. https://doi.org/10.3390/jcm10153247