
Short-Term Outcome of Inpatient Treatment for Adolescents with Anorexia Nervosa Using DSM-5 Remission Criteria

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
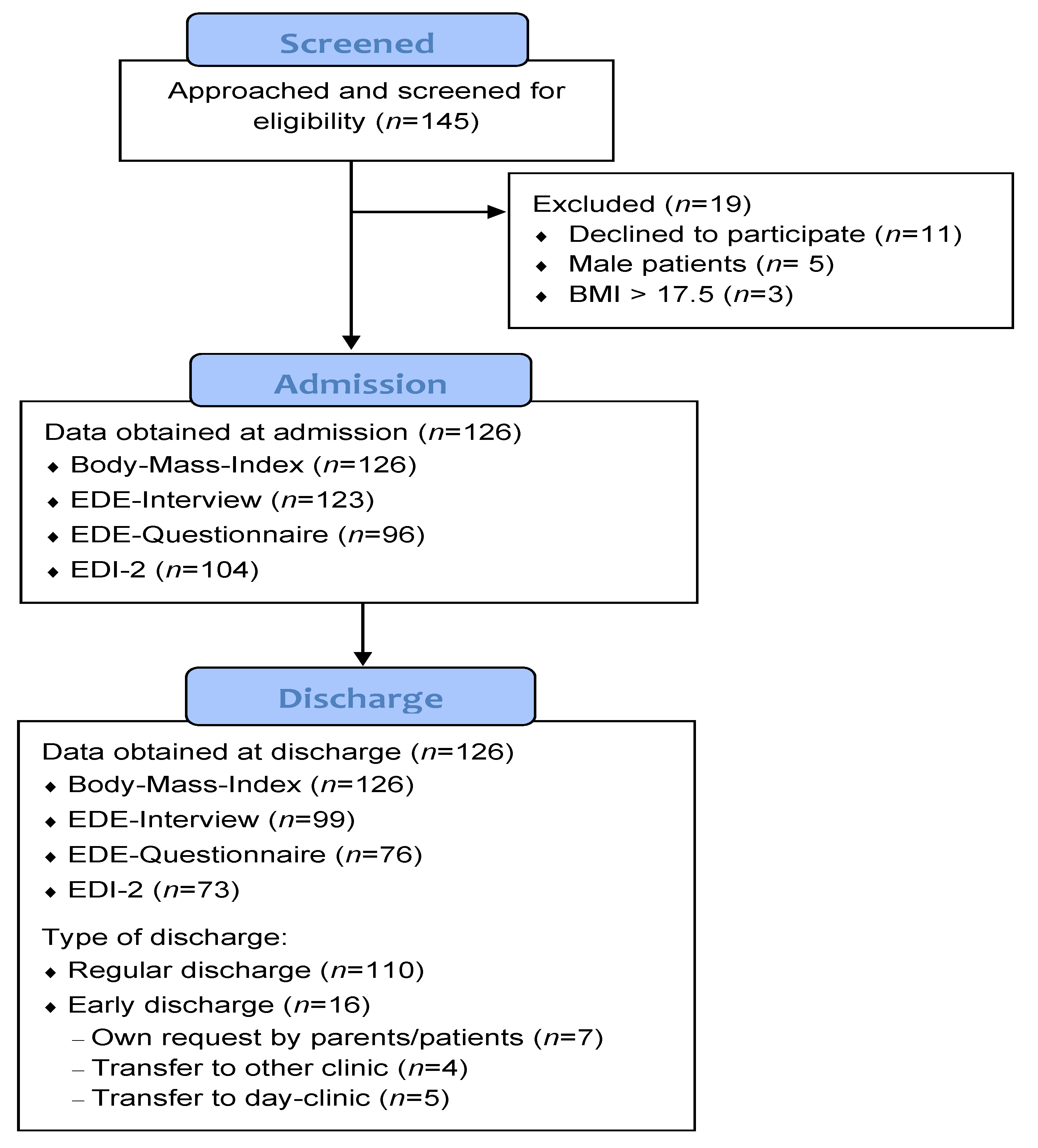
2.1. Study Population and Procedure
2.2. Treatment Concept (‘ViTAA’)
2.3. Measurements and Instruments
2.3.1. EDE & EDE-Q
2.3.2. EDI-2
2.3.3. Definition of Remission
2.4. Statistical Analyses
Power Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics of the Study Sample
3.2. Change in BMI and Eating Disorder Psychopathology
3.3. Outcomes Related to Remission According to DSM-5 Criteria
3.4. Predictors for Change in BMI and Length of Inpatient Stay
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Treasure, J.; Duarte, T.A.; Schmidt, U. Eating Disorders. Lancet 2020, 395, 899–911. [Google Scholar] [CrossRef]
- Treasure, J.; Zipfel, S.; Micali, N.; Wade, T.; Stice, E.; Claudino, A.; Schmidt, U.; Frank, G.K.; Bulik, C.M.; Wentz, E. Anorexia Nervosa. Nat. Rev. Dis. Primers 2015, 1, 15074. [Google Scholar] [CrossRef]
- Herpertz-Dahlmann, B.; Dahmen, B. Children in Need—Diagnostics, Epidemiology, Treatment and Outcome of Early Onset Anorexia Nervosa. Nutrients 2019, 11, 1932. [Google Scholar] [CrossRef] [Green Version]
- Brockmeyer, T.; Friederich, H.-C.; Schmidt, U. Advances in the Treatment of Anorexia Nervosa: A Review of Established and Emerging Interventions. Psychol. Med. 2018, 48, 1228–1256. [Google Scholar] [CrossRef]
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia Nervosa: Aetiology, Assessment, and Treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef]
- Fichter, M.M.; Quadflieg, N. Mortality in Eating Disorders—Results of a Large Prospective Clinical Longitudinal Study. Int. J. Eat. Disord. 2016, 49, 391–401. [Google Scholar] [CrossRef]
- Smink, F.R.E.; van Hoeken, D.; Hoek, H.W. Epidemiology of Eating Disorders: Incidence, Prevalence and Mortality Rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Ágh, T.; Kovács, G.; Supina, D.; Pawaskar, M.; Herman, B.K.; Vokó, Z.; Sheehan, D.V. A Systematic Review of the Health-Related Quality of Life and Economic Burdens of Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder. Eat. Weight Disord. 2016, 21, 353–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crow, S.J.; Nyman, J.A. The Cost-Effectiveness of Anorexia Nervosa Treatment. Int. J. Eat. Disord. 2004, 35, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Murray, S.B.; Quintana, D.S.; Loeb, K.L.; Griffiths, S.; Le Grange, D. Treatment Outcomes for Anorexia Nervosa: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Psychol. Med. 2019, 49, 535–544. [Google Scholar] [CrossRef] [PubMed]
- van Hoeken, D.; Hoek, H.W. Review of the Burden of Eating Disorders: Mortality, Disability, Costs, Quality of Life, and Family Burden. Curr. Opin. Psychiatry 2020, 33, 521–527. [Google Scholar] [CrossRef]
- Schmidt, U.; Adan, R.; Böhm, I.; Campbell, I.C.; Dingemans, A.; Ehrlich, S.; Elzakkers, I.; Favaro, A.; Giel, K.; Harrison, A.; et al. Eating Disorders: The Big Issue. Lancet Psychiatry 2016, 3, 313–315. [Google Scholar] [CrossRef]
- Madden, S. Systematic Review of Evidence for Different Treatment Settings in Anorexia Nervosa. World J. Psychiatry 2015, 5, 147. [Google Scholar] [CrossRef] [PubMed]
- Herpertz-Dahlmann, B.; Schwarte, R.; Krei, M.; Egberts, K.; Warnke, A.; Wewetzer, C.; Pfeiffer, E.; Fleischhaker, C.; Scherag, A.; Holtkamp, K.; et al. Day-Patient Treatment after Short Inpatient Care versus Continued Inpatient Treatment in Adolescents with Anorexia Nervosa (ANDI): A Multicentre, Randomised, Open-Label, Non-Inferiority Trial. Lancet 2014, 383, 1222–1229. [Google Scholar] [CrossRef]
- Martínez-González, L.; Fernández-Villa, T.; Molina, A.J.; Delgado-Rodríguez, M.; Martín, V. Incidence of Anorexia Nervosa in Women: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2020, 17, 3824. [Google Scholar] [CrossRef]
- Steinhausen, H.-C.; Jensen, C.M. Time Trends in Lifetime Incidence Rates of First-Time Diagnosed Anorexia Nervosa and Bulimia Nervosa across 16 Years in a Danish Nationwide Psychiatric Registry Study. Int. J. Eat. Disord. 2015, 48, 845–850. [Google Scholar] [CrossRef]
- Halmi, K.A. Anorexia Nervosa: An Increasing Problem in Children and Adolescents. Dialogues Clin. Neurosci. 2009, 11, 4. [Google Scholar] [CrossRef]
- Favaro, A.; Caregaro, L.; Tenconi, E.; Bosello, R.; Santonastaso, P. Time Trends in Age at Onset of Anorexia Nervosa and Bulimia Nervosa. J. Clin. Psychiatry 2009, 70, 1715–1721. [Google Scholar] [CrossRef]
- Treasure, J.; Oyeleye, O.; Bonin, E.-M.; Zipfel, S.; Fernandez-Aranda, F. Optimising Care Pathways for Adult Anorexia Nervosa. What Is the Evidence to Guide the Provision of High-Quality, Cost-Effective Services? Eur. Eat. Disord. Rev. 2021, 29, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Jansingh, A.; Danner, U.N.; Hoek, H.W.; van Elburg, A.A. Developments in the Psychological Treatment of Anorexia Nervosa and Their Implications for Daily Practice. Curr. Opin. Psychiatry 2020, 33, 534–541. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, E.; Houtzager, L.; de Vos, J.; Daemen, I.; Katsaragaki, G.; Karyotaki, E.; Cuijpers, P.; Dekker, J. Meta-Analysis on the Efficacy of Psychological Treatments for Anorexia Nervosa. Eur. Eat. Disord. Rev. 2019, 27, 331–351. [Google Scholar] [CrossRef] [PubMed]
- Berends, T.; Boonstra, N.; van Elburg, A. Relapse in Anorexia Nervosa: A Systematic Review and Meta-Analysis. Curr. Opin. Psychiatry 2018, 31, 445–455. [Google Scholar] [CrossRef]
- Zeeck, A. Psychotherapeutic Treatment for Anorexia Nervosa: A Systematic Review and Network Meta-Analysis. Front. Psychiatry 2018, 9, 158. [Google Scholar] [CrossRef] [Green Version]
- Steinhausen, H.-C. The Outcome of Anorexia Nervosa in the 20th Century. Am. J. Psychiatry 2002, 159, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Eating Disorders: Recognition and Treatment; NICE: London, UK, 2017; ISBN 978-1-4731-2508-7. [Google Scholar]
- Herpertz, S.; Fichter, M.; Herpertz-Dahlmann, B.; Hilbert, A.; Tuschen-Caffier, B.; Vocks, S.; Zeeck, A. Joint German Guideline “Diagnosis and Treatment of Eating Disorders”. 2020. Available online: https://www.awmf.org/fileadmin/user_upload/Leitlinien/051_D-Ges_Psychosom_Med_u_aerztliche_Psychotherapie/051-026e_S3_eating-disorders-diagnosis-treatment_2020-07.pdf (accessed on 24 May 2021).
- Herpertz-Dahlmann, B.; Salbach-Andrae, H. Overview of Treatment Modalities in Adolescent Anorexia Nervosa. Child. Adolesc. Psychiatr. Clin. N. Am. 2009, 18, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Föcker, M.; Heidemann-Eggert, E.; Antony, G.; Becker, K.; Egberts, K.; Ehrlich, S.; Fleischhaker, C.; Hahn, F.; Jaite, C.; Kaess, M.; et al. Die Versorgung von Kindern und Jugendlichen mit Anorexia nervosa in deutschen Kliniken. Z. Kinder-Und Jugendpsychiatrie Psychother. 2017, 45, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Madden, S.; Miskovic-Wheatley, J.; Wallis, A.; Kohn, M.; Lock, J.; Le Grange, D.; Jo, B.; Clarke, S.; Rhodes, P.; Hay, P.; et al. A Randomized Controlled Trial of In-Patient Treatment for Anorexia Nervosa in Medically Unstable Adolescents. Psychol. Med. 2015, 45, 415–427. [Google Scholar] [CrossRef] [Green Version]
- Gowers, S.; Clark, A.; Roberts, C.; Byford, S.; Barrett, B.; Griffiths, A.; Edwards, V.; Bryan, C.; Smethurst, N.; Rowlands, L.; et al. A Randomised Controlled Multicentre Trial of Treatments for Adolescent Anorexia Nervosa Including Assessment of Cost-Effectiveness and Patient Acceptability—the TOuCAN Trial. Health Technol. Assess. 2010, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Goddard, E.; Hibbs, R.; Raenker, S.; Salerno, L.; Arcelus, J.; Boughton, N.; Connan, F.; Goss, K.; Laszlo, B.; Morgan, J.; et al. A Multi-Centre Cohort Study of Short Term Outcomes of Hospital Treatment for Anorexia Nervosa in the UK. BMC Psychiatry 2013, 13, 287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, P.J.; Touyz, S.; Claudino, A.M.; Lujic, S.; Smith, C.A.; Madden, S. Inpatient versus Outpatient Care, Partial Hospitalisation and Waiting List for People with Eating Disorders. Cochrane Database Syst. Rev. 2019, 1, CD010827. [Google Scholar] [CrossRef]
- Lascar, R.; Letranchant, A.; Hirot, F.; Godart, N. Quels facteurs expliquent la durée d’hospitalisation pour anorexie mentale: Revue systématique de la littérature. L’Encéphale 2021, S0013700621000361. [Google Scholar] [CrossRef]
- Kästner, D.; Löwe, B.; Weigel, A.; Osen, B.; Voderholzer, U.; Gumz, A. Factors Influencing the Length of Hospital Stay of Patients with Anorexia Nervosa—Results of a Prospective Multi-Center Study. BMC Health Serv. Res. 2018, 18, 22. [Google Scholar] [CrossRef] [Green Version]
- Li, A.; Cunich, M.; Miskovic-Wheatley, J.; Maloney, D.; Madden, S.; Wallis, A.; Maguire, S. Factors Related to Length of Stay, Referral on Discharge and Hospital Readmission for Children and Adolescents with Anorexia Nervosa. Int. J. Eat. Disord. 2020, 54, 409–421. [Google Scholar] [CrossRef]
- Kan, C.; Hawkings, Y.; Cribben, H.; Treasure, J. Length of Stay for Anorexia Nervosa: Systematic Review and Meta-analysis. Eur. Eat. Disord. Rev. 2021, 29, 371–392. [Google Scholar] [CrossRef]
- Meule, A.; Schrambke, D.; Furst Loredo, A.; Schlegl, S.; Naab, S.; Voderholzer, U. Inpatient Treatment of Anorexia Nervosa in Adolescents: A 1-year Follow-up Study. Eur. Eat. Disord. Rev. 2020, 29, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Peckmezian, T.; Paxton, S.J. A Systematic Review of Outcomes Following Residential Treatment for Eating Disorders. Eur. Eat. Disord. Rev. 2020, 28, 246–259. [Google Scholar] [CrossRef] [Green Version]
- Halvorsen, I.; Reas, D.L.; Nilsen, J.-V.; Rø, Ø. Naturalistic Outcome of Family-Based Inpatient Treatment for Adolescents with Anorexia Nervosa. Eur. Eat. Disord. Rev. 2018, 26, 141–145. [Google Scholar] [CrossRef] [Green Version]
- Schlegl, S.; Diedrich, A.; Neumayr, C.; Fumi, M.; Naab, S.; Voderholzer, U. Inpatient Treatment for Adolescents with Anorexia Nervosa: Clinical Significance and Predictors of Treatment Outcome: Inpatient Treatment for Adolescents with AN. Eur. Eat. Disord. Rev. 2016, 24, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Dalle Grave, R.; Calugi, S.; El Ghoch, M.; Conti, M.; Fairburn, C.G. Inpatient Cognitive Behavior Therapy for Adolescents with Anorexia Nervosa: Immediate and Longer-Term Effects. Front. Psychiatry 2014, 5, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calugi, S.; Dalle Grave, R. Body Image Concern and Treatment Outcomes in Adolescents with Anorexia Nervosa. Int. J. Eat. Disord. 2019, 52, 582–585. [Google Scholar] [CrossRef]
- Fennig, S.; Brunstein Klomek, A.; Shahar, B.; Sarel-Michnik, Z.; Hadas, A. Inpatient Treatment Has No Impact on the Core Thoughts and Perceptions in Adolescents with Anorexia Nervosa: Core Thoughts in Anorexia. Early Interv. Psychiatry 2017, 11, 200–207. [Google Scholar] [CrossRef]
- Hetman, I.; Brunstein Klomek, A.; Goldzweig, G.; Hadas, A.; Horwitz, M.; Fennig, S. Percentage from Target Weight (PFTW) Predicts Re-Hospitalization in Adolescent Anorexia Nervosa. Isr. J. Psychiatry Relat. Sci. 2017, 54, 28–34. [Google Scholar] [PubMed]
- Vall, E.; Wade, T.D. Predictors and Moderators of Outcomes and Readmission for Adolescent Inpatients with Anorexia Nervosa: A Pilot Study. Clin. Psychol. 2017, 21, 143–152. [Google Scholar] [CrossRef]
- Collin, P.; Power, K.; Karatzias, T.; Grierson, D.; Yellowlees, A. The Effectiveness of, and Predictors of Response to, Inpatient Treatment of Anorexia Nervosa. Eur. Eat. Disord. Rev. 2010, 18, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Lock, J.; le GRANGE, D.; Forsberg, S.; Hewell, K. Is Family Therapy Useful for Treating Children With Anorexia Nervosa? Results of a Case Series. J. Am. Acad. Child. Adolesc. Psychiatry 2006, 45, 1323–1328. [Google Scholar] [CrossRef]
- Couturier, J.; Lock, J. What Is Remission in Adolescent Anorexia Nervosa? A Review of Various Conceptualizations and Quantitative Analysis. Int. J. Eat. Disord. 2006, 39, 175–183. [Google Scholar] [CrossRef]
- Wolk, S.L.; Loeb, K.L.; Walsh, B.T. Assessment of Patients with Anorexia Nervosa: Interview versus Self-Report. Int. J. Eat. Disord. 2005, 37, 92–99. [Google Scholar] [CrossRef]
- Passi, V.A.; Bryson, S.W.; Lock, J. Assessment of Eating Disorders in Adolescents with Anorexia Nervosa: Self-Report Questionnaire versus Interview. Int. J. Eat. Disord. 2003, 33, 45–54. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S.J. Assessment of Eating Disorders: Interview or Self-Report Questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar]
- Binford, R.B.; Le Grange, D.; Jellar, C.C. Eating Disorders Examination versus Eating Disorders Examination-Questionnaire in Adolescents with Full and Partial-Syndrome Bulimia Nervosa and Anorexia Nervosa. Int. J. Eat. Disord. 2005, 37, 44–49. [Google Scholar] [CrossRef]
- Isserlin, L.; Spettigue, W.; Norris, M.; Couturier, J. Outcomes of Inpatient Psychological Treatments for Children and Adolescents with Eating Disorders at Time of Discharge: A Systematic Review. J. Eat. Disord. 2020, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Hamadi, L.; Holliday, J. Moderators and Mediators of Outcome in Treatments for Anorexia Nervosa and Bulimia Nervosa in Adolescents: A Systematic Review of Randomized Controlled Trials. Int. J. Eat. Disord. 2020, 53, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Le Grange, D.; Huryk, K.M.; Murray, S.B.; Hughes, E.K.; Sawyer, S.M.; Loeb, K.L. Variability in Remission in Family Therapy for Anorexia Nervosa. Int. J. Eat. Disord. 2019, 52, 996–1003. [Google Scholar] [CrossRef] [Green Version]
- Richmond, T.K.; Woolverton, G.A.; Mammel, K.; Ornstein, R.M.; Spalding, A.; Woods, E.R.; Forman, S.F. How Do You Define Recovery? A Qualitative Study of Patients with Eating Disorders, Their Parents, and Clinicians. Int. J. Eat. Disord. 2020, 53, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Brown, T.A.; Murray, S.B.; Anderson, L.K.; Kaye, W.H. Early Predictors of Treatment Outcome in a Partial Hospital Program for Adolescent Anorexia Nervosa. Int. J. Eat. Disord. 2020, 53, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Jaite, C.; Bühren, K.; Dahmen, B.; Dempfle, A.; Becker, K.; Correll, C.U.; Egberts, K.M.; Ehrlich, S.; Fleischhaker, C.; von Gontard, A.; et al. Clinical Characteristics of Inpatients with Childhood vs. Adolescent Anorexia Nervosa. Nutrients 2019, 11, 2593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grave, R.D.; Sartirana, M.; Calugi, S. Enhanced Cognitive Behavioral Therapy for Adolescents with Anorexia Nervosa: Outcomes and Predictors of Change in a Real-World Setting. Int. J. Eat. Disord. 2019, 52, 1042–1046. [Google Scholar] [CrossRef]
- Errichiello, L.; Iodice, D.; Bruzzese, D.; Gherghi, M.; Senatore, I. Prognostic Factors and Outcome in Anorexia Nervosa: A Follow-up Study. Eat. Weight Disord. 2016, 21, 73–82. [Google Scholar] [CrossRef]
- Roux, H.; Ali, A.; Lambert, S.; Radon, L.; Huas, C.; Curt, F.; Berthoz, S.; Godart, N.; the EVHAN Group. Predictive Factors of Dropout from Inpatient Treatment for Anorexia Nervosa. BMC Psychiatry 2016, 16, 339. [Google Scholar] [CrossRef]
- Glasofer, D.R.; Muratore, A.F.; Attia, E.; Wu, P.; Wang, Y.; Minkoff, H.; Rufin, T.; Walsh, B.T.; Steinglass, J.E. Predictors of Illness Course and Health Maintenance Following Inpatient Treatment among Patients with Anorexia Nervosa. J. Eat. Disord. 2020, 8, 69. [Google Scholar] [CrossRef]
- Vall, E.; Wade, T.D. Predictors of Treatment Outcome in Individuals with Eating Disorders: A Systematic Review and Meta-Analysis. Int. J. Eat. Disord. 2015, 48, 946–971. [Google Scholar] [CrossRef] [PubMed]
- Gregertsen, E.C.; Mandy, W.; Kanakam, N.; Armstrong, S.; Serpell, L. Pre-Treatment Patient Characteristics as Predictors of Drop-out and Treatment Outcome in Individual and Family Therapy for Adolescents and Adults with Anorexia Nervosa: A Systematic Review and Meta-Analysis. Psychiatry Res. 2019, 271, 484–501. [Google Scholar] [CrossRef]
- Wales, J.; Brewin, N.; Cashmore, R.; Haycraft, E.; Baggott, J.; Cooper, A.; Arcelus, J. Predictors of Positive Treatment Outcome in People with Anorexia Nervosa Treated in a Specialized Inpatient Unit: The Role of Early Response to Treatment: Early Response to Inpatient Treatment. Eur. Eat. Disord. Rev. 2016, 24, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, J.C.; Mercer-Lynn, K.B.; Norwood, S.J.; Bewell-Weiss, C.V.; Crosby, R.D.; Woodside, D.B.; Olmsted, M.P. A Prospective Study of Predictors of Relapse in Anorexia Nervosa: Implications for Relapse Prevention. Psychiatry Res. 2012, 200, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Andrés-Pepiñá, S.; Plana, M.T.; Flamarique, I.; Romero, S.; Borràs, R.; Julià, L.; Gárriz, M.; Castro-Fornieles, J. Long-Term Outcome and Psychiatric Comorbidity of Adolescent-Onset Anorexia Nervosa. Clin. Child. Psychol. Psychiatry 2020, 25, 33–44. [Google Scholar] [CrossRef]
- Abd Elbaky, G.B.; Hay, P.J.; le Grange, D.; Lacey, H.; Crosby, R.D.; Touyz, S. Pre-Treatment Predictors of Attrition in a Randomised Controlled Trial of Psychological Therapy for Severe and Enduring Anorexia Nervosa. BMC Psychiatry 2014, 14, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahn, M.; Brunstein-Klomek, A.; Hadas, A.; Snir, A.; Fennig, S. Early Changes in Depression Predict Outcomes of Inpatient Adolescent Anorexia Nervosa. Eat. Weight Disord. 2020, 25, 777–785. [Google Scholar] [CrossRef]
- Zerwas, S.; Lund, B.C.; Von Holle, A.; Thornton, L.M.; Berrettini, W.H.; Brandt, H.; Crawford, S.; Fichter, M.M.; Halmi, K.A.; Johnson, C.; et al. Factors Associated with Recovery from Anorexia Nervosa. J. Psychiatr. Res. 2013, 47, 972–979. [Google Scholar] [CrossRef] [Green Version]
- Le Grange, D.; Fitzsimmons-Craft, E.E.; Crosby, R.D.; Hay, P.; Lacey, H.; Bamford, B.; Stiles-Shields, C.; Touyz, S. Predictors and Moderators of Outcome for Severe and Enduring Anorexia Nervosa. Behav. Res. Ther. 2014, 56, 91–98. [Google Scholar] [CrossRef]
- Calugi, S.; El Ghoch, M.; Conti, M.; Dalle Grave, R. Depression and Treatment Outcome in Anorexia Nervosa. Psychiatry Res. 2014, 218, 195–200. [Google Scholar] [CrossRef]
- Jordan, J.; McIntosh, V.V.W.; Carter, F.A.; Joyce, P.R.; Frampton, C.M.A.; Luty, S.E.; McKenzie, J.M.; Bulik, C.M. Clinical Characteristics Associated with Premature Termination from Outpatient Psychotherapy for Anorexia Nervosa. Eur. Eat. Disord. Rev. 2014, 22, 278–284. [Google Scholar] [CrossRef]
- Hubert, T.; Pioggiosi, P.; Huas, C.; Wallier, J.; Maria, A.-S.; Apfel, A.; Curt, F.; Falissard, B.; Godart, N. Drop-out from Adolescent and Young Adult Inpatient Treatment for Anorexia Nervosa. Psychiatry Res. 2013, 209, 632–637. [Google Scholar] [CrossRef]
- Himmerich, H.; Kan, C.; Au, K.; Treasure, J. Pharmacological Treatment of Eating Disorders, Comorbid Mental Health Problems, Malnutrition and Physical Health Consequences. Pharmacol. Ther. 2021, 217, 107667. [Google Scholar] [CrossRef] [PubMed]
- Aigner, M.; Treasure, J.; Kaye, W.; Kasper, S.; WFSBP Task Force on Eating Disorders. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Pharmacological Treatment of Eating Disorders. World J. Biol. Psychiatry 2011, 12, 400–443. [Google Scholar] [CrossRef] [PubMed]
- McElroy, S.L.; Guerdjikova, A.I.; Mori, N.; Keck, P.E. Psychopharmacologic Treatment of Eating Disorders: Emerging Findings. Curr. Psychiatry Rep. 2015, 17, 35. [Google Scholar] [CrossRef] [PubMed]
- Attia, E.; Steinglass, J.E.; Walsh, B.T.; Wang, Y.; Wu, P.; Schreyer, C.; Wildes, J.; Yilmaz, Z.; Guarda, A.S.; Kaplan, A.S.; et al. Olanzapine Versus Placebo in Adult Outpatients with Anorexia Nervosa: A Randomized Clinical Trial. Am. J. Psychiatry 2019, 176, 449–456. [Google Scholar] [CrossRef]
- Bissada, H.; Tasca, G.A.; Barber, A.M.; Bradwejn, J. Olanzapine in the Treatment of Low Body Weight and Obsessive Thinking in Women with Anorexia Nervosa: A Randomized, Double-Blind, Placebo-Controlled Trial. Am. J. Psychiatry 2008, 165, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Bulik, C.M.; Berkman, N.D.; Brownley, K.A.; Sedway, J.A.; Lohr, K.N. Anorexia Nervosa Treatment: A Systematic Review of Randomized Controlled Trials. Int. J. Eat. Disord. 2007, 40, 310–320. [Google Scholar] [CrossRef]
- Malina, A.; Gaskill, J.; McConaha, C.; Frank, G.K.; LaVia, M.; Scholar, L.; Kaye, W.H. Olanzapine Treatment of Anorexia Nervosa: A Retrospective Study. Int. J. Eat. Disord. 2003, 33, 234–237. [Google Scholar] [CrossRef]
- Mondraty, N.; Birmingham, C.L.; Touyz, S.; Sundakov, V.; Chapman, L.; Beumont, P. Randomized Controlled Trial of Olanzapine in the Treatment of Cognitions in Anorexia Nervosa. Australas. Psychiatry 2005, 13, 72–75. [Google Scholar] [CrossRef]
- Attia, E.; Haiman, C.; Walsh, B.T.; Flater, S.R. Does Fluoxetine Augment the Inpatient Treatment of Anorexia Nervosa? Am. J. Psychiatry 1998, 155, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Muratore, A.F.; Attia, E. Current Therapeutic Approaches to Anorexia Nervosa: State of the Art. Clin. Ther. 2021, 43, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Dold, M.; Aigner, M.; Klabunde, M.; Treasure, J.; Kasper, S. Second-Generation Antipsychotic Drugs in Anorexia Nervosa: A Meta-Analysis of Randomized Controlled Trials. Psychother. Psychosom. 2015, 84, 110–116. [Google Scholar] [CrossRef]
- Kafantaris, V.; Leigh, E.; Hertz, S.; Berest, A.; Schebendach, J.; Sterling, W.M.; Saito, E.; Sunday, S.; Higdon, C.; Golden, N.H.; et al. A Placebo-Controlled Pilot Study of Adjunctive Olanzapine for Adolescents with Anorexia Nervosa. J. Child. Adolesc. Psychopharmacol. 2011, 21, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Dilling, H.; World Health Organization. Internationale Klassifikation Psychischer Störungen: ICD-10 Kapitel V (F); Klinisch-Diagnostische Leitlinien, 6th ed.; Huber: Bern, Switzerland, 2008; ISBN 978-3-456-84558-6. [Google Scholar]
- Hilbert, A.; Tuschen-Caffier, B.; Ohms, M. Eating Disorder Examination: Deutschsprachige Version des strukturierten Essstörungsinterviews. Diagnostica 2004, 50, 98–106. [Google Scholar] [CrossRef]
- Hilbert, A.; Tuschen-Caffier, B.; Karwautz, A.; Niederhofer, H.; Munsch, S. Eating Disorder Examination-Questionnaire. Diagnostica 2007, 53, 144–154. [Google Scholar] [CrossRef]
- Rathner, G.; Waldherr, K. Eating Disorder Inventory-2: A German Language Validation with Norms for Female and Male Adolescents. Z. Für Klin. Psychol. Psychitrie Psychother. 1997, 45, 157–182. [Google Scholar]
- Philipp, J.; Franta, C.; Zeiler, M.; Truttmann, S.; Wittek, T.; Imgart, H.; Zanko, A.; Auer-Welsbach, E.; Mairhofer, D.; Mitterer, M.; et al. Does a Skills Intervention for Parents Have a Positive Impact on Adolescents’ Anorexia Nervosa Outcome? Answers from a Quasi-Randomised Feasibility Trial of SUCCEAT. Int. J. Environ. Res. Public Health 2021, 18, 4656. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; Wiley: New York, NY, USA, 2000. [Google Scholar]
- Graell, M.; Andrés, P.; Sepúlveda, A.R.; Moreno, A.; Villaseñor, Á.; Faya, M.; Martínez-Cantarero, C.; Gómez-Martínez, S.; Marcos, A.; Morandé, G.; et al. The Adolescent Onset Anorexia Nervosa Study (ANABEL): Design and Baseline Results. Int. J. Methods Psychiatr. Res. 2018, 27. [Google Scholar] [CrossRef] [Green Version]
- Morgan, H.G.; Russell, G.F.M. Value of Family Background and Clinical Features as Predictors of Long-Term Outcome in Anorexia Nervosa: Four-Year Follow-up Study of 41 Patients. Psychol. Med. 1975, 5, 355–371. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Truax, P. Clinical Significance: A Statistical Approach to Denning Meaningful Change in Psychotherapy Research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mean | SD | Range [Min, Max] | |
|---|---|---|---|
| Age at admission | 14.83 | 1.56 | 11–17 |
| Age of eating disorder onset | 13.83 | 1.71 | 8–17 |
| Mean duration of illness (in months) | 13.48 | 10.42 | 1–48 |
| BMI at admission | 14.40 | 1.32 | 10.50–17.42 |
| Weight (kg) at admission | 38.54 | 4.64 | 24.20–50.00 |
| Height (m) at admission | 1.63 | 0.07 | 1.41–1.77 |
| Lowest weight since age of 12(kg) | 36.83 | 4.48 | 24.00–46.70 |
| Highest weight since age of 12 (kg) | 50.79 | 8.59 | 28.15–76.00 |
| Weight suppression (kg) 1 | 13.75 | 6.42 | 1.40–34.00 |
| Age of mother | 45.23 | 5.05 | 32–55 |
| Age of father | 48.75 | 6.09 | 36–67 |
| N | % | ||
| Anorexia Nervosa subtype | |||
| Restrictive | 111 | 88.1% | |
| Binge/Purging | 15 | 11.9% | |
| Anorexia Nervosa severity according to DSM-5 2 | |||
| Mild | 23 | 18.3% | |
| Moderate | 30 | 23.8% | |
| Severe | 33 | 26.2% | |
| Extreme | 40 | 31.7% | |
| Psychiatric comorbidities (N, %Yes) | |||
| Any | 81 | 64.3% | |
| Obsessive-Compulsive Disorder | 18 | 14.3% | |
| Depressive Disorder | 49 | 38.9% | |
| Anxiety Disorder | 9 | 7.1% | |
| Personality Disorder | 5 | 4.0% | |
| Organic Brain Syndrome | 16 | 12.7% | |
| Other | 27 | 21.4% | |
| Medication use (N, %Yes) | |||
| Antidepressant medication | 55 | 43.7% | |
| Antipsychotics medication | 79 | 62.7% | |
| Anxiolytic medication | 25 | 19.8% | |
| Nutritional Supplements | 126 | 100% | |
| Referral to clinic | |||
| In-House outpatient clinic | 57 | 45.2% | |
| Private practice of CAP or psychotherapist | 18 | 14.3% | |
| Private practice of pediatrician | 8 | 6.3% | |
| General practitioner | 7 | 5.6% | |
| Other CAP clinic | 5 | 4.0% | |
| Psychosomatic clinic | 11 | 8.7% | |
| Pediatric clinic | 8 | 6.3% | |
| Other outpatient center | 12 | 9.5% | |
| Nationality | |||
| Austria | 120 | 95.2% | |
| Other | 6 | 4.8% | |
| School type | |||
| Grammar school | 91 | 72.2% | |
| Vocational school (with A-level) | 16 | 12.7% | |
| Vocational training school | 4 | 3.2% | |
| Secondary modern school | 13 | 10.4% | |
| Other school | 2 | 1.6% | |
| Family status (living with…) | |||
| both biological parents | 82 | 65.1% | |
| single parent | 43 | 34.7% | |
| no biological parent | 1 | 0.8% | |
| Highest education mother/father | |||
| University degree | 44/51 | 37.0%/43.6% | |
| A level degree | 24/18 | 20.2%/15.4% | |
| Below A-level degree | 51/48 | 42.9%/41.0% | |
| Missing | 7/9 | ||
| Marital status mother/father | |||
| Married/in partnership | 92/95 | 74.2%/78.5% | |
| Single | 2/1 | 1.6%/0.8% | |
| Divorced/widowed | 30/25 | 24.2%/20.6% | |
| Missing | 2/5 | ||
| Number of siblings | |||
| 0 | 15 | 14.3% | |
| 1 | 48 | 45.7% | |
| 2 | 27 | 25.7% | |
| ≥3 | 15 | 14.3% | |
| Missing | 21 | data 1 |
| Outcome Variable | Admission | Discharge | Test Statistic | Effect Size | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t (df) | p | Cohen’s d | 95% CI | |
| BMI | 14.40 | 1.32 | 17.01 | 1.29 | 20.269 (125) | <0.001 | 2.01 | [1.67; 2.34] |
| BMI Percentile | 1.47 | 3.41 | 12.77 | 11.97 | 11.812 (125) | <0.001 | 1.07 | [0.84; 1.29] |
| EDE Total score | 3.13 | 1.55 | 2.04 | 1.30 | 8.557 (95) | <0.001 | 0.75 | [0.55; 0.94] |
| EDE Restraint a | 3.14 | 1.87 | 1.42 | 1.21 | 9.642 (95) | <0.001 | 1.06 | [0.79; 1.33] |
| EDE Eating concern a | 2.62 | 1.60 | 1.48 | 1.25 | 7.677 (93) | <0.001 | 0.78 | [0.55; 1.01] |
| EDE Weight concern a | 3.18 | 1.84 | 2.31 | 1.68 | 4.884 (95) | <0.001 | 0.49 | [0.28; 0.70] |
| EDE Shape concern a | 3.55 | 1.63 | 2.98 | 1.71 | 3.940 (95) | <0.001 | 0.35 | [0.17; 0.52] |
| EDE-Q Total score | 2.88 | 1.63 | 1.83 | 1.39 | 6.861 (66) | <0.001 | 0.69 | [0.47; 0.91] |
| EDE-Q Restraint a | 2.93 | 2.04 | 1.25 | 1.30 | 7.526 (65) | <0.001 | 0.94 | [0.65; 1.24] |
| EDE-Q Eating concern a | 2.26 | 1.53 | 1.30 | 1.22 | 6.711 (66) | <0.001 | 0.68 | [0.46; 0.90] |
| EDE-Q Weight concern a | 2.88 | 1.66 | 2.07 | 1.67 | 4.618 (65) | <0.001 | 0.49 | [0.27; 0.71] |
| EDE-Q Shape concern a | 3.48 | 1.85 | 2.71 | 1.82 | 3.996 (66) | <0.001 | 0.42 | [0.20; 0.64] |
| EDI-2 Global score | 68.73 | 36.90 | 54.22 | 37.18 | 3.962 (66) | <0.001 | 0.39 | [0.19; 0.59] |
| EDI-2 Drive for thinness b | 8.55 | 7.20 | 6.07 | 7.13 | 3.210 (66) | 0.002 | 0.35 | [0.13; 0.57] |
| EDI-2 Bulimia b | 1.18 | 2.70 | 0.59 | 2.10 | 2.012 (65) | 0.048 | 0.24 | [0.00; 0.48] |
| EDI-2 Body dissatisfaction b | 11.48 | 7.86 | 10.45 | 8.65 | 1.085 (66) | 0.282 | 0.12 | [−0.10; 0.35] |
| EDI-2 Ineffectiveness b | 6.97 | 6.12 | 5.90 | 6.29 | 1.842 (66) | 0.070 | 0.17 | [−0.01; 0.36] |
| EDI-2 Perfectionism b | 6.18 | 4.27 | 6.04 | 4.53 | 0.330 (66) | 0.742 | 0.03 | [−0.15; 0.21] |
| EDI-2 Interpersonal distrust b | 4.72 | 4.49 | 3.39 | 3.81 | 3.856 (66) | <0.001 | 0.31 | [0.15; 0.48] |
| EDI-2 Interoceptive awareness b | 6.78 | 5.85 | 4.32 | 4.91 | 4.008 (66) | <0.001 | 0.45 | [0.22; 0.69] |
| EDI-2 Maturity fears b | 7.42 | 5.22 | 5.85 | 4.94 | 2.541 (66) | 0.013 | 0.31 | [0.06; 0.55] |
| EDI-2 Asceticism b | 5.57 | 4.53 | 4.57 | 4.83 | 2.041 (66) | 0.045 | 0.21 | [0.00; 0.42] |
| EDI-2 Impulse regulation b | 3.71 | 4.54 | 2.21 | 3.57 | 3.217 (66) | 0.002 | 0.36 | [0.13; 0.59] |
| EDI-2 Social insecurity b | 6.20 | 4.36 | 4.80 | 4.27 | 3.553 (66) | 0.001 | 0.32 | [0.14; 0.51] |
| No Remission (N = 45) a | Partial Remission (N = 32) b | Full Remission (N = 24) c | Test Statistic | Post-Hoc Analyses | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | F(df), p | ||
| Age at admission | 15.62 (1.32) | 14.23 (1.43) | 14.57 (1.88) | 8.900 (2,96), <0.001 | a > b,c |
| BMI at admission | 14.19 (1.11) | 14.71 (1.53) | 14.19 (1.44) | 1.654 (2,96), 0.197 | |
| BMI percentile at admission | 0.44 (1.27) | 2.24 (2.97) | 1.68 (4.20) | 4.249 (2,96), 0.017 | a < b |
| EDE total at admission | 3.47 (1.58) | 3.39 (1.31) | 2.16 (1.44) | 6.652 (2,93), 0.002 | c < a,b |
| EDE-Q total at admission | 3.39 (1.45) | 2.94 (1.48) | 2.01 (1.40) | 5.874 (2,78), 0.004 | c < a |
| EDI-2 total at admission | 76.68 (36.75) | 71.51 (36.19) | 52.68 (30.76) | 3.206 (2,81), 0.046 | c < a |
| Age of eating disorder onset | 14.62 (1.27) | 13.29 (1.74) | 13.52 (2.02) | 7.284 (2,96), 0.001 | a > b,c |
| Duration of illness | 13.56 (9.75) | 12.05 (10.71) | 14.37 (10.29) | 0.375 (2,96), 0.688 | |
| Duration of inpatient stay | 66.53 (35.48) | 81.60 (29.39) | 66.35 (30.53) | 2.243 (2,95), 0.112 | |
| Weight suppression | 14.30 (6.22) | 12.98 (4.91) | 14.50 (9.04) | 0.459 (2,95), 0.633 | |
| % | % | % | Chi2 (df), p | ||
| Any psychiatric comorbidity | 62.2% | 74.2% | 52.2% | 2.838(2), 0.242 | |
| Antidepressant medication | 42.2% | 61.3% | 26.1% | 6.792(2), 0.034 | b > c |
| Antipsychotic medication | 62.2% | 71.0% | 52.2% | 1.998(2), 368 | |
| Anxiolytic medication | 17.8% | 29.0% | 17.4% | 1.653(2), 0.438 | |
| Single parent families | 42.2% | 29.0% | 21.7% | 3.249(2), 0.197 |
| Predictor | b(SE) | Beta | t | p |
|---|---|---|---|---|
| Outcome: Change in BMI (R2 = 0.58; adjusted R2 = 0.56) 3 | ||||
| Constant | 7.449 (1.11) | 6.704 | <0.001 | |
| Sociodemographic predictors | ||||
| Family status 2 | 0.452 (0.18) | 0.148 | 2.460 | 0.015 |
| Clinical predictors | ||||
| BMI at admission | −0.504 (0.07) | −0.460 | −7.506 | <0.001 |
| Duration of inpatient stay | 0.020 (<0.01) | −0.459 | 7.005 | <0.001 |
| Psychopharmacological predictors | ||||
| Antipsychotic medication 1 | 0.439 (0.19) | 0.146 | 2.288 | 0.024 |
| Anxiolytic medication 1 | −0.111 (0.24) | −0.030 | −0.459 | 0.647 |
| Outcome: Duration of inpatient stay (R2 = 0.26; adjusted R2 = 0.22) 3,4 | ||||
| Constant | 149.358 (31.06) | 4.809 | <0.001 | |
| Clinical predictors | ||||
| BMI at admission | −7.250 (2.15) | −0.307 | −3.374 | 0.001 |
| EDE total at admission | 5.440 (1.90) | 0.259 | 2.858 | 0.005 |
| Psychopharmacological predictors | ||||
| Antidepressant medication 1 | 10.660 (5.91) | 0.169 | 1.803 | 0.074 |
| Antipsychotic medication 1 | 5.219 (6.11) | 0.080 | 0.854 | 0.395 |
| Anxiolytic medication 1 | 18.204 (7.14) | 0.233 | 2.549 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mairhofer, D.; Zeiler, M.; Philipp, J.; Truttmann, S.; Wittek, T.; Skala, K.; Mitterer, M.; Schöfbeck, G.; Laczkovics, C.; Schwarzenberg, J.; et al. Short-Term Outcome of Inpatient Treatment for Adolescents with Anorexia Nervosa Using DSM-5 Remission Criteria. J. Clin. Med. 2021, 10, 3190. https://doi.org/10.3390/jcm10143190
Mairhofer D, Zeiler M, Philipp J, Truttmann S, Wittek T, Skala K, Mitterer M, Schöfbeck G, Laczkovics C, Schwarzenberg J, et al. Short-Term Outcome of Inpatient Treatment for Adolescents with Anorexia Nervosa Using DSM-5 Remission Criteria. Journal of Clinical Medicine. 2021; 10(14):3190. https://doi.org/10.3390/jcm10143190
Chicago/Turabian StyleMairhofer, Dunja, Michael Zeiler, Julia Philipp, Stefanie Truttmann, Tanja Wittek, Katrin Skala, Michaela Mitterer, Gabriele Schöfbeck, Clarissa Laczkovics, Julia Schwarzenberg, and et al. 2021. "Short-Term Outcome of Inpatient Treatment for Adolescents with Anorexia Nervosa Using DSM-5 Remission Criteria" Journal of Clinical Medicine 10, no. 14: 3190. https://doi.org/10.3390/jcm10143190