
Comparison of Efficacy between 120° and 180° Schlemm’s Canal Incision Microhook Ab Interno Trabeculotomy

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauhan, B.C.; Mikelberg, F.S.; Balaszi, A.G.; LeBlanc, R.P.; Lesk, M.R.; Trope, G.E.; Canadian Glaucoma Study Group. Canadian Glaucoma Study: 2. risk factors for the progression of open-angle glaucoma. Arch. Ophthalmol. 2008, 126, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Bengtsson, B.; Hussein, M.; Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M. What controls aqueous humor outflow resistance? Exp. Eye Res. 2006, 82, 545–557. [Google Scholar] [CrossRef] [Green Version]
- Tanito, M.; Sano, I.; Ikeda, Y.; Fujihara, E. Shore-term results of microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery in Japanese eyes: Initial case series. Acta. Ophthalmol. 2017, 95, e354–e360. [Google Scholar] [CrossRef] [PubMed]
- Tanito, M.; Ikeda, Y.; Fujihara, E. Effectiveness and safety of combined cataract surgery and microhook ab interno trabeculotomy in Japanese eyes with glaucoma: Report of an initial case series. Jpn. J. Ophthalmol. 2017, 61, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Onoe, H.; Hirooka, K.; Okumichi, H.; Sakata, H.; Murakami, Y.; Kiuchi, Y. Corneal higher-order aberrations after microhook ab interno trabeculotomy and goniotomy with the Kahook Dual Blade. Under submission.
- Aoki, R.; Hirooka, K.; Goda, E.; Yuasa, Y.; Okumichi, H.; Onoe, H.; Kiuchi, Y. Comparison of surgical outcomes between microhook ab interno trabeculotomy and goniotomy with the Kahook Dual Blade in combination with phacoemulsification: A retrospective, comparative case series. Adv. Ther. 2021, 38, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Tanihara, H.; Negi, A.; Akimoto, M.; Terauchi, H.; Okudaira, A.; Kozaki, J.; Takeuchi, A.; Nagata, M. Surgical effects of trabeculotomy ab externo on adult eyes with primary open angle glaucoma and pseudoexfoliation syndrome. Arch. Ophthalmol. 1993, 111, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Brandt, M.T.; Haug, R.H. Traumatic hyphema: A comprehensive review. J. Oral Maxillofac. Surg. 2001, 59, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Manabe, S.; Sawaguchi, S.; Hayashi, K. The effect of the extent of the incision in the Schlemm canal on the surgical outcomes of suture trabeculotomy for open-angle glaucoma. Jpn. J. Ophthalmol. 2017, 61, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Kawaji, T. 12-month randomized trial of 360° and 180° Schlemm’s canal incisions in suture trabeculotomy ab interno for open-angle glaucoma. Br. J. Ophthalmol. Online ahead of print. [CrossRef] [PubMed]
- Mori, S.; Murai, Y.; Ueda, K.; Sakamoto, M.; Kurimoto, T.; Yamada-Nakanishi, Y.; Nakamura, M. Comparison of efficacy and early surgery-related complications between one-quadrant and two-quadrant microhook ab interno trabeculotomy: A propensity score matched study. Acta. Ophthalmol. Online ahead of print. [CrossRef] [PubMed]
- Rosenquist, R.; Epstein, D.; Melamed, S.; Johnson, M.; Grant, W.M. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr. Eye Res. 1989, 8, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Chin, S.; Nitta, T.; Shinmei, Y.; Aoyagi, M.; Nitta, A.; Ohno, S.; Ishida, S.; Yoshida, K. Reduction of intraocular pressure using a modified 360-degree suture trabeculotomy technique in primary and secondary open-angle glaucoma: A pilot study. J. Glaucoma. 2012, 21, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.P.; Lin, S.C.; Junk, A.K.; Radhakrishnan, S.; Singh, K.; Chen, T.C. The effect of phacoemulsification on intraocular pressure in glaucoma patients: A report by the American academy of ophthalmology. Ophthalmology 2015, 122, 1294–1307. [Google Scholar] [CrossRef] [PubMed]
- Bovee, C.E.; Pasquale, L.R. Evolving surgical interventions in the treatment of glaucoma. Semin. Ophthalmol. 2017, 31, 91–95. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 120° | 180° | p Value | |
|---|---|---|---|
| No. eyes | 30 | 22 | |
| Age (years) | 72.3 ± 10.4 | 75.4 ± 10.8 | 0.30 |
| Gender (M/F) | 18/12 | 13/9 | 0.94 |
| Type of glaucoma | 0.82 | ||
| POAG | 20 | 14 | |
| Exfoliation glaucoma | 10 | 8 | |
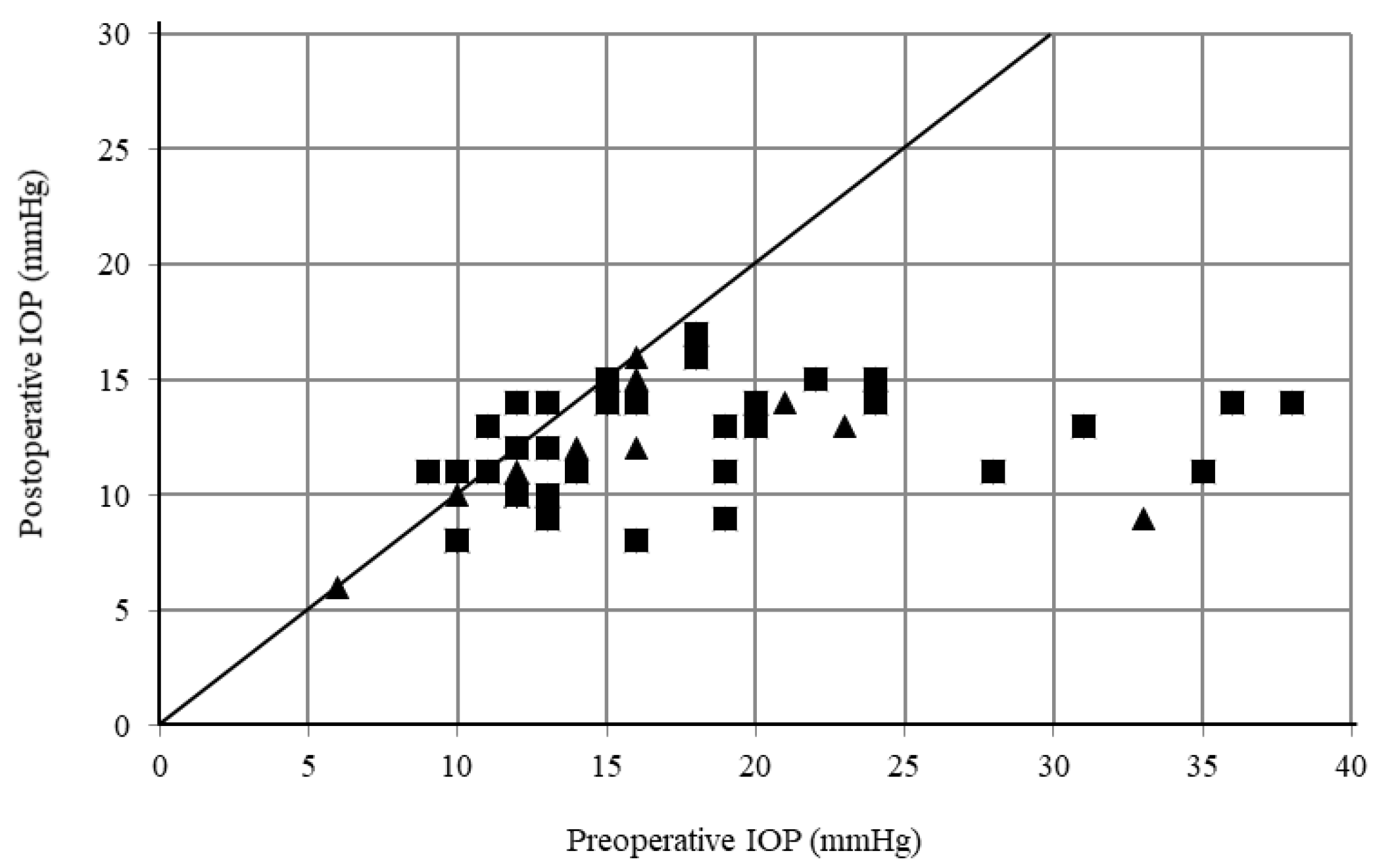
| Preoperative IOP (mmHg) | 16.9 ± 7.6 | 17.1 ± 7.0 | 0.94 |
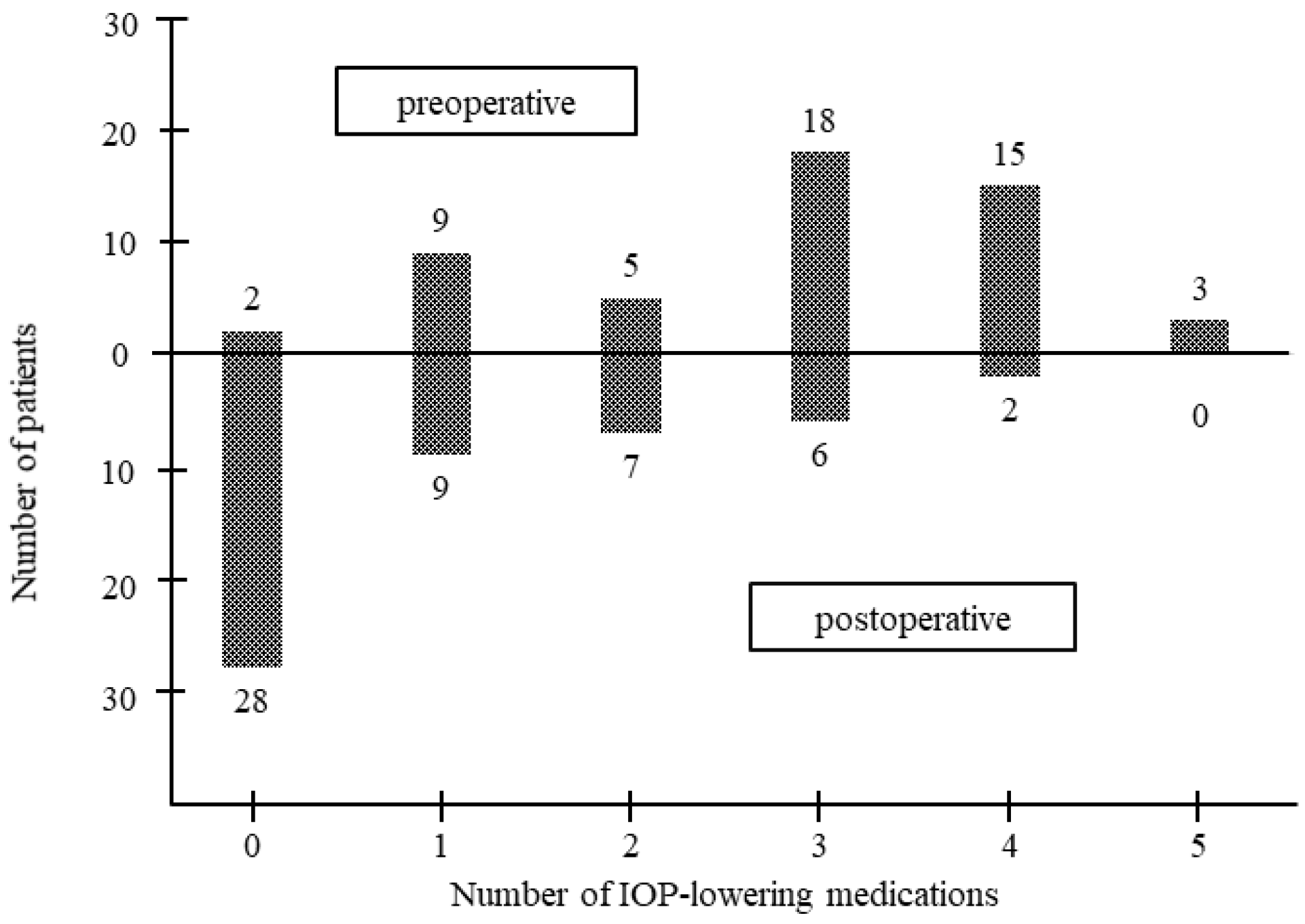
| No. IOP-lowering medications | 2.8 ± 1.4 | 2.9 ± 1.2 | 0.89 |
| Mean deviation (dB) | −13.9 ± 1.4 | −9.2 ± 1.7 | 0.03 |
| 120° | 180° | ||||||
|---|---|---|---|---|---|---|---|
| IOP at Each Time Point (mmHg) | Change from Baseline (%) | p Value * | IOP at Each Time Point (mmHg) | Change from Baseline (%) | p Value * | p Value ** | |
| Baseline | 16.9 ± 7.6 (n = 30) | 17.1 ± 7.0 (n = 22) | 0.94 | ||||
| Month 6 | 12.5 ± 2.7 (n = 25) | 18.8 ± 26.6 | 0.01 | 12.9 ± 2.4 (n = 22) | 15.3 ± 28.6 | 0.045 | 0.62 |
| Month 12 | 10.9 ± 2.7 (n = 14) | 29.5 ± 29.7 | <0.01 | 12.1 ± 3.2 (n = 21) | 24.1 ± 25.4 | 0.02 | 0.27 |
| Month 18 | 11.2 ± 3.0 (n = 13) | 26.1 ± 31.2 | <0.01 | 12.6 ± 2.7 (n = 16) | 22.7 ± 29.3 | 0.02 | 0.77 |
| Month 24 | 11.1 ± 3.1 (n = 10) | 34.2 ± 27.2 | 0.01 | 12.9 ± 1.4 (n = 13) | 23.1 ± 26.4 | 0.01 | 0.07 |
| 120° | 180° | ||||
|---|---|---|---|---|---|
| Number of Medications at Each Time Point | p Value * | Number of Medications at Each Time Point | p Value * | p Value ** | |
| Baseline | 2.8 ± 1.4 (n = 30) | 2.9 ± 1.2 (n = 22) | 0.89 | ||
| Month 6 | 0.9 ± 1.1 (n = 25) | <0.01 | 0.9 ± 1.1 (n = 22) | <0.01 | 0.94 |
| Month 12 | 1.0 ± 1.3 (n = 14) | <0.01 | 0.9 ± 1.1 (n = 21) | <0.01 | 0.86 |
| Month 18 | 1.1 ± 1.3 (n = 13) | <0.01 | 1.2 ± 1.3 (n = 16) | <0.01 | 0.78 |
| Month 24 | 1.4 ± 1.4 (n = 10) | <0.01 | 1.4 ± 1.5 (n = 13) | <0.01 | >0.99 |
| 120° | 180° | p Value | |
|---|---|---|---|
| Hyphema with niveau formation | 5 (16.7%) | 4 (18.2%) | 0.89 |
| Transient IOP elevation > 30 mmHg | 2 (6.7%) | 1 (4.6%) | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okada, N.; Hirooka, K.; Onoe, H.; Murakami, Y.; Okumichi, H.; Kiuchi, Y. Comparison of Efficacy between 120° and 180° Schlemm’s Canal Incision Microhook Ab Interno Trabeculotomy. J. Clin. Med. 2021, 10, 3181. https://doi.org/10.3390/jcm10143181
Okada N, Hirooka K, Onoe H, Murakami Y, Okumichi H, Kiuchi Y. Comparison of Efficacy between 120° and 180° Schlemm’s Canal Incision Microhook Ab Interno Trabeculotomy. Journal of Clinical Medicine. 2021; 10(14):3181. https://doi.org/10.3390/jcm10143181
Chicago/Turabian StyleOkada, Naoki, Kazuyuki Hirooka, Hiromitsu Onoe, Yumiko Murakami, Hideaki Okumichi, and Yoshiaki Kiuchi. 2021. "Comparison of Efficacy between 120° and 180° Schlemm’s Canal Incision Microhook Ab Interno Trabeculotomy" Journal of Clinical Medicine 10, no. 14: 3181. https://doi.org/10.3390/jcm10143181