1. Introduction
Nosocomial infections (NI) tend to appear in patients hospitalized in public hospitals, and are not the reason the patient was admitted in the first place [
1]. NI may appear during the patients stay in the hospital, or even after the patient have been released from the hospital [
2]. Other classifications that define NI are: infections occurring 48 h after the beginning of hospitalization, 3 days after patients release or 1 month after surgery [
1].
NI are caused by bacteria, fungi, and viruses [
2]. Frequently they are caused by bacteria, existing in the hospital as well as in the natural microbiome of a human organism. These bacteria cause infections especially at the moment of decreased immunity in patients [
2]. The most common infections are blood, urinary tract, areas of surgery or pneumonia [
3].
Data show, that in countries with high standard of healthcare, 7 out of 100 patients are diagnosed with NI, but in countries with lower standards of healthcare, the number of infected patients is higher, reaching up to 10 per 100 patients [
2,
4]. Clinical observations in the USA in 2003 presented that about two million patients annually admitted to hospital are diagnosed with NI [
5]. Other studies have found that healthcare-associated infections are one of the top ten causes of patient death in the United States [
6]. Subsequent studies on the epidemiology of HAI (hospital-acquired infection) showed that in developed countries, healthcare-associated infections occur in 5% to 15% of patients treated in hospitals, of which 9% to 37% occur in Intensive Care Units (ICU) [
6,
7,
8]. In Europe, 4.6–9.3% of hospitalized patients are diagnosed with HAI [
6].
NI are a major problem, because they are caused frequently by bacteria resistant to antibiotics, and increase recovery time for about 6.4 days to 12.7 days, while at the same time increasing the cost of hospitalization. NI also increases the risk of patient death [
3,
5]. In the USA alone, in Intensive Care Units about 90 thousand patients die because of infections, indicating that HAI are the most common cause of death in those units, not severe accidents [
5].
HAI appear not only on the ICU, transplantology and surgery wards, but also on wards where surgical procedures are not conducted [
9]. Development of NI is positively corelated with extended periods of hospitalization. Most common wards with prolonged patient persistence are rehabilitation wards, where patients are admitted with a variety of injuries or disabilities, which further translates to longer times of hospitalization [
10].
Studies concerning the frequency of appearance of HAI are often conducted on the ICU, as well as on transplantology wards and infant care wards [
2,
4]. There is an abundance of studies showing the true number of HAI on rehabilitation wards, where patients with various injuries or after prior stay in the ICU are hospitalized, and their time of hospitalization is a big risk factor for the appearance of these infections [
2,
3].
Studies conducted in France in the 1990s showed a frequent appearance of HAI (most common in the urinary tract and the area of surgery) in patients on the rehabilitation wards and with long-term care [
3]. The maximal general level of infections in this research reached 6.7% [
3,
11]. However, studies conducted in rehabilitation wards in the 2000s showed a general increase in the levels of the infections, some reaching from 8.2% to 12%, mostly concerning the urinary tract [
6,
12]. In 2005, 5.2% of patients had urinary tract infections [
13].
Because of the few data and incomplete information, it seems crucial to gather data about up-to-date NI frequency in the rehabilitation ward in Poland. The available literature contains data from the 1990s, and the years 2000 and 2005, generally from France. It is crucial to remember that the prevention methods and the treatment itself changed dramatically in the last decade alone. The first step to eliminate the problem and subsequently decrease additional patients’ hospitalization costs is to present the severity of the issue.
The aim of the study is to evaluate the frequency of the appearance of HAI during 20 months between 2018–2020 on the rehabilitation ward. Additionally, it is to determine the specific groups of patients most prone to those infections and collect information about the most frequently used treatments on the rehabilitation ward.
4. Discussion
Nosocomial infections are important problems because they increase mortality and contribute to lengthening the hospitalization period of patients, thus increasing general healthcare costs [
3,
5]. The current literature is concerned with healthcare associated infections in intensive care unit, transplantology, burns and neonatal care units [
2,
4]. Research on nosocomial infections was also conducted in both rehabilitation centres and departments [
3,
9,
13]. However, it should be noted that these studies are rare, only few attempts were made to analyse the problem [
3,
9,
11,
12,
13]. The lack of current data on the frequency of nosocomial infections in rehabilitation wards is probably due to the fact that often the branches accepted only patients with current microbiological culture tests confirming the absence of such infections [
9,
13].
Our clinic uses a number of procedures aimed at preventing the development of nosocomial infections during the patient’s hospitalization. The preventive measures used in the clinic include training of medical personnel, maintaining hand hygiene and the use of protective gloves and gowns. Insulation is also used in high-risk patients, as well as additional masks and protective glasses. Whenever possible, single-use equipment is used to care for the patient. Medical devices are disinfected after each patient. The applied preventive measures are the standard procedures used in the world [
14]. However, despite the application of appropriate preventive procedures against the development of HAI, nosocomial infections were detected in our clinic.
NI is most often caused by microorganisms belonging to the patients and that exist in the hospital [
2]. In our work, 88.89% of the cases were endogenous infections caused by bacteria belonging to human microflora. Only in 11.11% of cases, nosocomial infections were caused by bacteria present in the hospital environment.
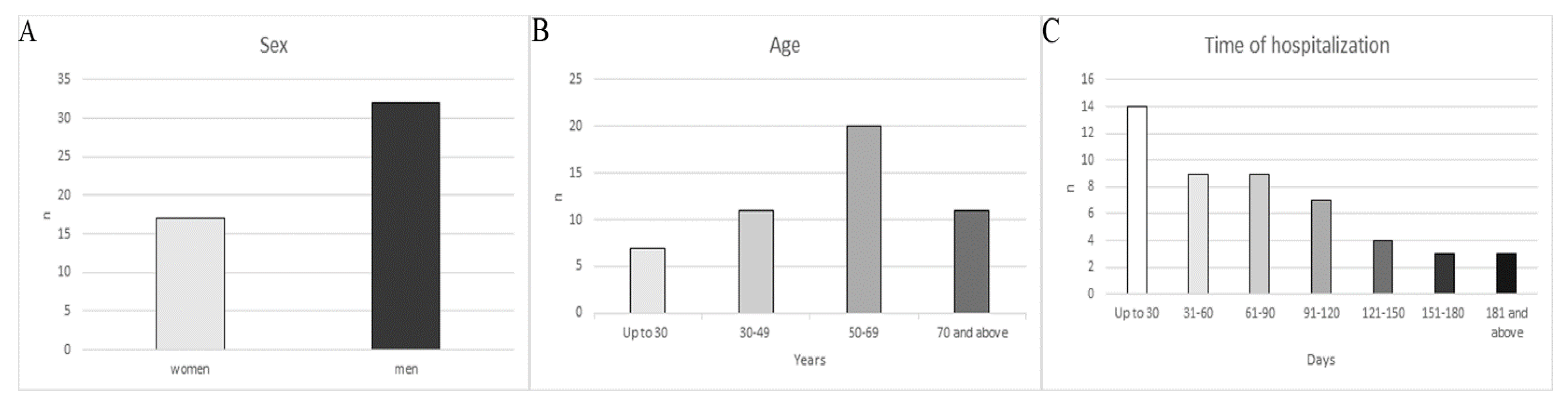
In our study, a higher frequency of nosocomial infections was observed in men than in women. Men represent 65.31% of the study group, while women 34.69%. Dividing the number of nosocomial infections according to sex, as many as 75% of all NI were diagnosed in men. This is confirmed by clinical studies which have demonstrated that males are more prone to nosocomial infections [
15]. Research conducted in 2019 on a large group of patients by Aghdassi et al. [
16] showed that men were also more sensitive to surgical site infections. The same studies showed a much higher rate of nosocomial infections after orthopaedic and trauma surgery [
16]. The research conducted by Colbert et al. showed a lower frequency of pneumonia and inpatient sepsis in women with acute ischemic stroke [
17]. It should also be noted that men are much more likely to suffer more severe accidents than women, which also significantly affects the decrease in immunity [
18].
Age is another important risk factor in the development of nosocomial infections. This is confirmed by the research conducted by Bochicchio et al., which showed a significantly higher incidence of nosocomial infection in aging patients [
19]. Other studies also confirm the significant influence of age on the emergence of NI in patients [
19,
20]. Different results showed a lower incidence of NI in patients over 60 years of age compared to other studies in this field [
19,
20]. Additionally, it has been shown that age significantly influences the appearance of NI in patients, but it is related to the presence of other risk factors, such as long hospitalization, chronic diseases, etc. [
21].
In our study, patients were divided into four age groups up to 30, 30–49, 50–69 and over 70 years old. There was an increased frequency of nosocomial infections of 12.50%, 26.38%, 38.89% and 22.23%, respectively. The data show that the highest number of nosocomial infections was found in patients of 50–69 years. A lower number of infections was observed in patients over 70 years, i.e., 22.23%. However, this may be due to a significantly smaller group of this age patients and a more responsible approach of the staff in caring for this group, as they are more sensitive to complications. Based on the obtained results, it can be concluded that age generally influences the frequency of NI.
The duration of hospitalization increased the risk of nosocomial infections [
10]. It exposes the patients to pathogens present in the hospital environment, which may be contaminated by another patient, hospital staff or by microorganisms that are infiltrating the hospital environment [
22]. The appearance of NI in a patient as a result of a long stay in the hospital also causes the extension of hospitalization time. In another study, which was conducted in 68 hospitals, it was shown that this period will be extended by an average of 10.4 days [
23].
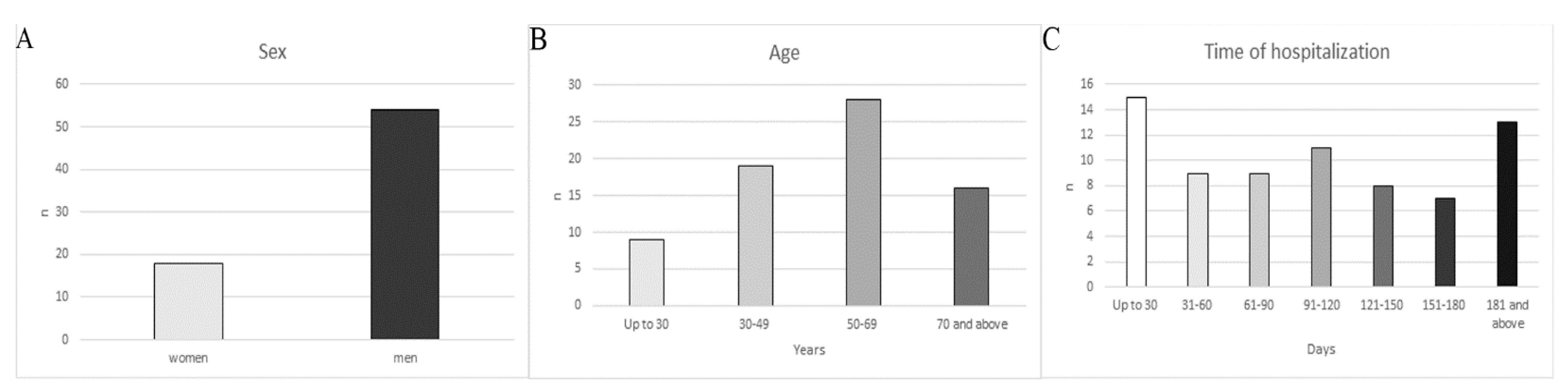
In our study, the hospitalization time was divided into seven periods, i.e., up to 30, 31–60, 61–90, 91–120, 121–150, 151–180 and over 180 days, and the frequency of nosocomial infections was 20.83%, 12.50%, 12.50%, 15.28%, 11.11%, 9.73%, and 18.05%, respectively. The division of hospitalization time was standardized according to Liu et al. [
24]. In the presented study, hospitalized patients were also divided in the same groups, and the following results were obtained: 28.57%, 18.37%, 18.37%, 14.29%, 8.16%, 6.12% and 6.12%. The results show that the number of infected patients decreases with the duration of hospitalization.
In the first period of hospitalization, the highest number of nosocomial infections can be observed, and in the next two periods they are decreased and maintained at the same level. It is most likely related to the detection time of NI and the introduction of appropriate treatment. The increase in the frequency of infections can also be observed in days 121–150, but in 151–180 days a decrease was noted. However, it can be seen that the highest number of infections was observed in the first stay, where the largest number of patients were hospitalized but in the period of hospitalization over 181 days, when fewer patients were hospitalized the number of infections was the highest, which suggests that the duration of hospitalization increases the risk of developing NI. In studies conducted by Sulzgruber et al., it can also be noted that the frequency of nosocomial infections associated with postoperative care increased significantly with the length of the patient’s pre-operative hospitalization [
25].
The evaluation of the conducted studies shows that in patients with spinal cord injuries, who were also hospitalized in the orthopaedic and rehabilitation clinic, the risk of developing NI was higher [
26,
27]. These studies show that this type of infection occurs both during the first hospitalization and subsequent hospitalizations. This suggests that frequent and long duration stays in the hospital increases the risk of developing nosocomial infections in these patients [
26,
27].
Our study also shows that the highest number of infections was detected in patients with paralysis, which accounts for 57.14% of all patients included in the study, and the frequency was 69.44%. Due to the type of paralysis, the highest frequency of nosocomial infections was noted in patients with tetraplegia, at 45.83%. However, in the case of the limb paralysis or hemiplegia, the frequency of NI development was 13.89% and 9.72%, respectively. Observations may indicate a significant influence of motor limitation in patients on the emergence of NI development.
The presented study also shows that nosocomial infections occur not only in patients with damaged spinal cords, but also in other diseases, for example: complications after surgery, primary bilateral gonarthrosis, other primary coxarthrosis, head injuries, idiopathic childhood scoliosis, spondylolisthesis and other diseases listed in
Table 2. It may be related to the weakness of the patient’s organism due to primary disease and the time of hospitalization [
10].
In our work, Pseudomonas aeruginosa was a dominant infectious mediator. It was detected in 22.22% of hospitalized patients. Often the isolated bacterium was Klebsiella pneumoniae, which was detected in 20.83% cases. Proteus mirabilis was noted in 13.89% studies. Clostridium difficile was diagnosed in 12.50% cases. Other bacteria such as: Staphylococcus aureus, Escherichia coli, Acinetobacter baumannii complex, Enterococcus faecalis, Providencia stuartii, Staphylococcus epidermidis, and Enterobacter cloacase complex were also detected in patients hospitalized in our clinic.
According to Mylotte et al. the most frequently detected infections are caused by
Pseudomonas aeruginosa and
Klebsiella pneumoniae [
9]. The study was conducted on a narrow group of patients, which compared NI in patients with spinal cord injury to patients without spinal cord injuries [
9]. Our study covers a more diverse groups of patients, because the rehabilitation clinic treats not only patients with spinal cord injury, but also patients with other diseases that prolong hospitalization. Additionally, the Mylotte et al. study also presents that
Clostridium difficile was responsible for nosocomial infections in 15% of patients hospitalized in acute rehabilitation unit [
9]. In our studies, 12.50% of cases were also infected by
Clostridium difficile.
However, the Girard et al. study presents the most frequent cases infected by
Staphylococcus aureus and
Escherichia coli [
3]. Differences in diagnosed infectious bacteria between our study and the studies of Mylotte et al. and Girard et al. is probably caused by the different duration of the studies [
3,
9]. Our study lasted 20 months, and the study by Mylotte et al. was for 19 months, which gives a similar duration of study [
6]. In contrast, the study by Girard et al. lasted from May 21 to June 15 of the same year, which could have contributed to the detection of other infectious bacteria in the studied group of patients [
3].
The most common NI was urinary tract and infections of this type appear mainly in patients with spinal cord injury who have neurogenic bladders that require use of a urinary catheter [
28]. According to data from 2014, 30% of all nosocomial infections are urinary tract infections connected with risk factors such as use of urinary catheter, surgery, other urological procedures, long hospitalization, age, male sex and chronic diseases [
29].
Our patients also had 43.06% nosocomial urinary tract infection. Surgical areas infections and gastrointestinal tract infections were diagnosed for 13.89%.
The research conducted by Mylotte et al. [
9] supports our data connected with the urinary tract, as well as skin and wound infections. In our study, it can be seen that gastrointestinal tract infections also appear frequently. In patients hospitalized in our clinic, which deals with the rehabilitation of individuals with various degrees of disability and undergoing orthopaedic and traumatic surgery, other clinical forms of hospital infections have also been diagnosed, such as: urosepsis, pneumonia, bacteremia, sepsis, respiratory system infections, skin and soft tissue infections, infections of the reproductive system and catheter vascular-related infections.
The most frequently identified risk factors in our work was the use of urinary catheters, which was the cause of 84.45% of all cases. Other frequent risk factors were peripheral venous catheter, blood sampling, peripheral puncture, and previous infections, which were noted with the following frequency: 81.94%, 65.28%, 63.89%, 40.28% and 27.78%, respectively.
The urinary catheter is always considered as the risk factor for the development of nosocomial infection, as it can introduce into the patient’s urinary tract microorganisms that contribute to the development of urinary tract infection [
28]. In our study, the most common clinical form was urinary tract infection, which occurred as much as 81.94%, so urinary catheter infections are considered as a risk factor. Additionally, catheterization of the urinary bladder in men also increases the risk of developing NI, which is related to the anatomical structure of the urethra, which is much longer in men than in women. It additionally increases the risk of development nosocomial infections [
29]. Studies indicate that urinary catheters in almost half of patients are incorrectly inserted and not replaced for long time [
28,
30]. The number of diagnosed pathogens responsible for causing HAI could also significantly affect the frequency of urinary tract infections. The most frequently exuded bacterium was
Pseudomonas aeruginosa, which significantly increases the risk of developing urinary tract infections [
31].
Peripheral venous catheters, peripheral puncture and blood sampling were also frequently considered as risk factors. Peripheral venous catheter and peripheral punctures are the main source of bacteremia and sepsis in patients during hospitalization [
32].
Past infections are also marked as risk factors, as they significantly reduce the patient’s immunity and extend the duration of hospitalization, and thus contribute to an increased risk of developing further nosocomial infections [
23].
Our observations also identified multichannel catheters, epidural catheters, central venous puncture, gastric tube, respirator, surgery, prosthesis implantation, previous operations, blood transfusion, kidney failure, malnutrition and cancer as risk factors consistent with the previous data [
33,
34,
35].
In our examination the most frequent symptom of NI was fever, which was recorded in 69.06% of cases. A common symptom was also exudate from the surgical site, which was noted in twelve (16.67%) patients, and redness was noted in nine (12.50%) cases. Diarrhoea was also noted in nine (12.50%), dysuria in six (8.33%), edema in four (5.56%), blood pressure decrease in two (2.78%) and nausea in one (1, 39%) of the presented subjects.
In our work, we decided to include data about the drugs which were most frequently used to treat patients with diagnosed hospital infections. It can be concluded that the most frequently used therapeutic substances were antibiotics. Studies by other authors of similar topics support our use of antibiotics as the most common choice in the treatment of NI [
36].


 ,
, 




{kind=link}
{kind=link}