
Relationship between Prognostic Stage in Breast Cancer and Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. 18F-FDG PET/CT Protocol
2.3. 18F-FDG PET/CT Analysis
2.4. Clinicopathological Evaluation
2.5. Anatomical and Prognostic Stages
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. Anatomical and Prognostic Stages
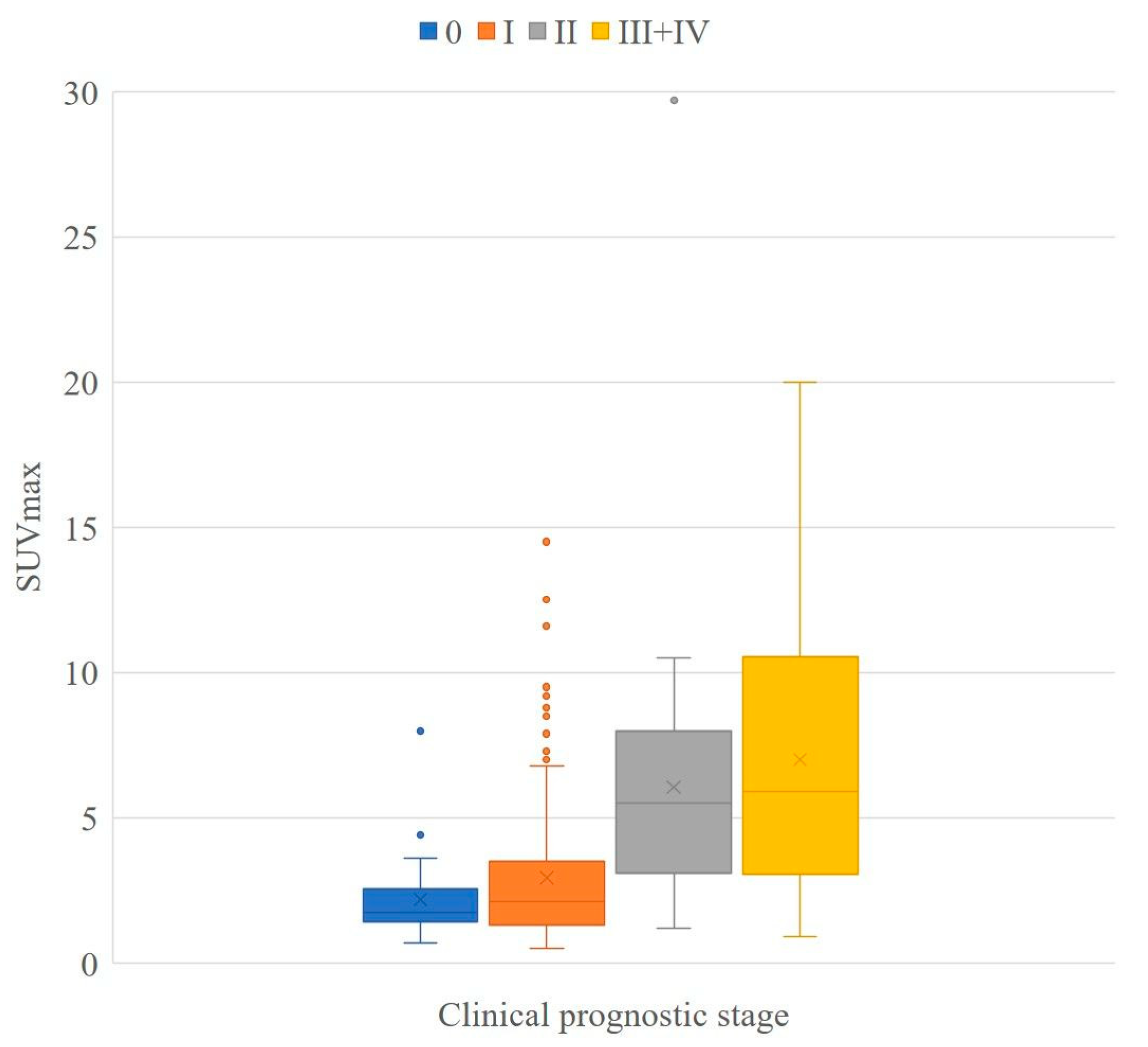
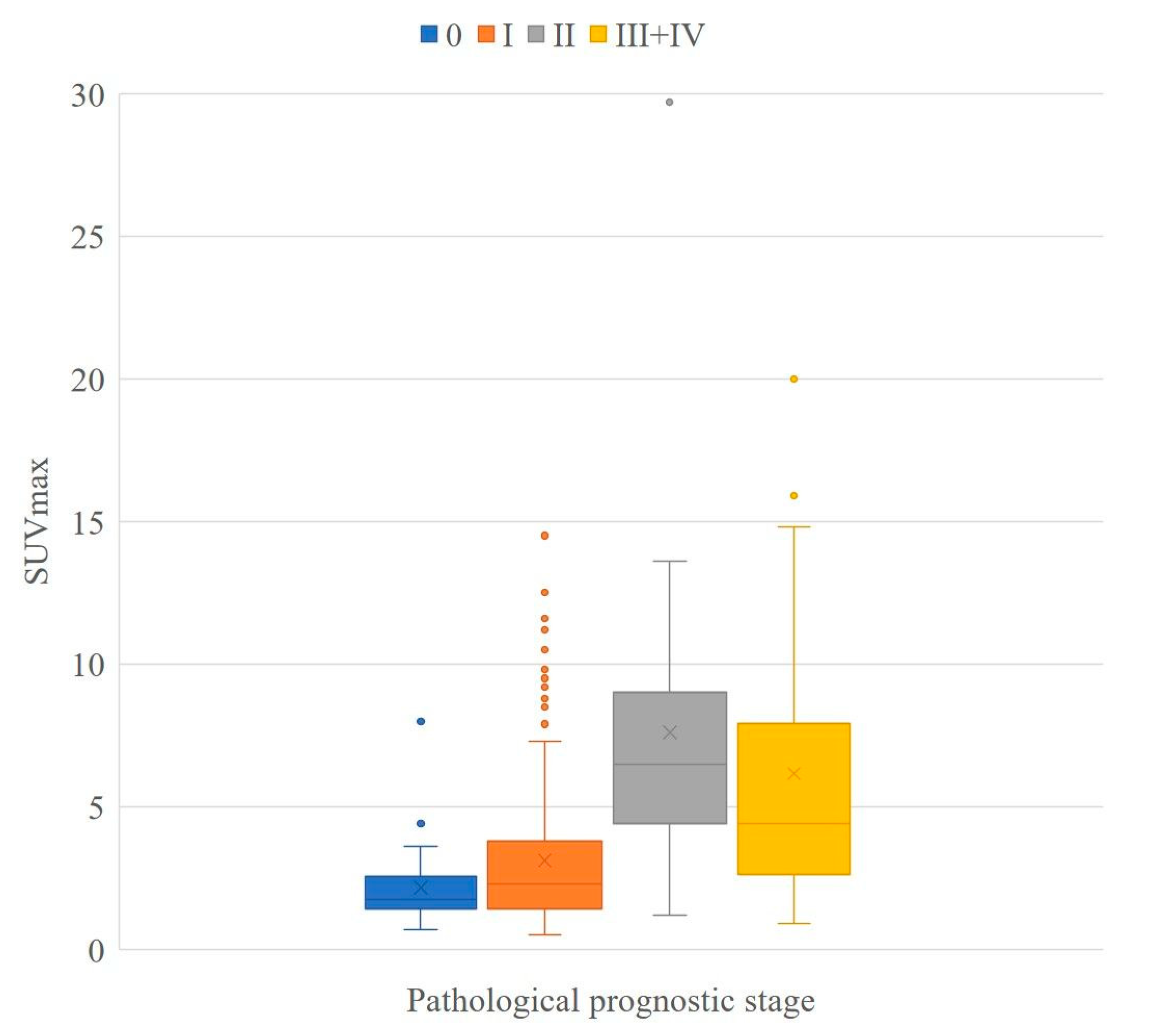
3.3. SUVmax at Each Prognostic Stage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Weiss, A.; Mac Gregor, M.C.; Lichtensztajn, D.; Yi, M.; Tadros, A.; Hortobagyi, G.N.; Giordano, S.H.; Hunt, K.K.; Mittendorf, E.A. Validation Study of the American Joint Committee on Cancer Eighth Edition Prognostic Stage Compared with the Anatomic Stage in Breast Cancer. JAMA Oncol. 2018, 4, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth dditionedition of the AJCC cancer staging manual: Breast cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef]
- Wang, M.; Chen, H.; Wu, K.; Ding, A.; Zhang, M.; Zhang, P. Evaluation of the prognostic stage in the 8th edition of the American Joint Committee on Cancer in locally advanced breast cancer: An analysis based on SEER 18 database. Breast 2018, 37, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Rahman, O. Validation of the 8th AJCC prognostic staging system for breast cancer in a population-based setting. Breast Cancer Res. Treat. 2018, 168, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Fujioka, T.; Katsuta, L.; Tsuchiya, J.; Kubota, K.; Kasahara, M.; Oda, G.; Nakagawa, T.; Onishi, I.; Tateishi, U. Diagnostic performance of time-of-flight PET/CT for evaluating nodal metastasis of the axilla in breast cancer. Nucl. Med. Commun. 2019, 40, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Kadoya, T.; Aogi, K.; Kiyoto, S.; Masumoto, N.; Sugawara, Y.; Okada, M. Role of maximum standardized uptake value in fluorodeoxyglucose positron emission tomography/computed tomography predicts malignancy grade and prognosis of oper-able breast cancer: A multi-institute study. Breast Cancer Res. Treat. 2013, 141, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Ishiba, T.; Nakagawa, T.; Sato, T.; Nagahara, M.; Oda, G.; Sugimoto, H.; Kasahara, M.; Hosoya, T.; Kubota, K.; Fujioka, T.; et al. Efficiency of fluorodeoxyglucose positron emission tomography/computed tomography to predict prognosis in breast cancer patients received neoadjuvant chemotherapy. SpringerPlus 2015, 4, 817. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.G.; Lee, M.; Jeon, T.J.; Han, K.; Lee, H.M.; Lee, S.A.; Ryu, Y.H.; Son, E.J.; Jeong, J. [18F]-Fluorodeoxyglucose Positron Emission Tomography Can Contribute to Discriminate Patients with Poor Prognosis in Hormone Receptor-Positive Breast Cancer. PLoS ONE 2014, 9, e105905. [Google Scholar] [CrossRef]
- Wen, W.; Xuan, D.; Hu, Y.; Li, X.; Liu, L.; Xu, D. Prognostic value of maximum standard uptake value, metabolic tumor volume, and total lesion glycolysis of positron emission tomography/computed tomography in patients with breast cancer: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0225959. [Google Scholar] [CrossRef]
- Fujioka, T.; Kubota, K.; Kikuchi, Y.; Tsuchiya, J.; Tateishi, U.; Kasaharak, M.; Oda, G.; Ishiba, T.; Nakagawa, T. The feasibility of using 18F-FDG-PET/CT in patients with mucinous breast carcinoma. Nucl. Med. Commun. 2018, 39, 1033–1038. [Google Scholar] [CrossRef]
- Shimoda, W.; Hayashi, M.; Murakami, K.; Oyama, T.; Sunagawa, M. The relationship between FDG uptake in PET scans and biological behavior in breast cancer. Breast Cancer 2007, 14, 260–268. [Google Scholar] [CrossRef]
- Sanli, Y.; Kuyumcu, S.; Ozkan, Z.G.; Işik, G.; Karanlik, H.; Guzelbey, B.; Turkmen, B.; Ozel, S.; Yavuz, E.; Mudun, A. Increased FDG uptake in breast cancer is asso-ciated with prognostic factors. Ann. Nucl. Med. 2012, 26, 345–350. [Google Scholar] [CrossRef]
- Osborne, J.R.; Port, E.; Gonen, M.; Doane, A.S.; Yeung, H.; Gerald, W.; Cook, J.B.; Larson, S. 18F-FDG PET of locally invasive breast cancer and association of estrogen receptor status with standardized uptake value: Microarray and immunohistochemical analysis. J. Nucl. Med. 2010, 51, 543–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Francis, G.; Goldstein, N.S.; Hayes, M.; Hicks, D.G.; et al. American Society of Clinical Oncol-ogy/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and proges-terone receptors in breast cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, A.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Koh, J.; Kim, M.J. Introduction of a New Staging System of Breast Cancer for Radiologists: An Emphasis on the Prognostic Stage. Korean J. Radiol. 2019, 20, 69–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, L.N.; Ismaila, N.; McShane, L.M.; Andre, F.; Collyar, D.E.; Gonzalez-Angulo, A.M.; Hammond, E.H.; Kuderer, N.M.; Liu, M.C.; Mennel, R.G.; et al. Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women with Early-Stage Invasive Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 1134–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, M.; Mittendorf, E.A.; Cormier, J.N.; Buchholz, T.; Bilimoria, K.; Sahin, A.A.; Hortobagyi, G.N.; Gonzalez-Angulo, A.M.; Luo, S.; Buzdar, A.U.; et al. Novel Staging System for Predicting Disease-Specific Survival in Patients with Breast Cancer Treated with Surgery As the First Intervention: Time to Modify the Current American Joint Committee on Cancer Staging System. J. Clin. Oncol. 2011, 29, 4654–4661. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, U.; Zurrida, S.; Viale, G.; Galimberti, V.; Arnone, P.; Nolè, F. Rethinking TNM: A Breast Cancer Classification to Guide to Treatment and Facilitate Research. Breast J. 2009, 15, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Bagaria, S.P.; Ray, P.S.; Sim, M.-S.; Ye, X.; Shamonki, J.M.; Cui, X.; Giuliano, A.E. Personalizing Breast Cancer Staging by the Inclusion of ER, PR, and HER2. JAMA Surg. 2014, 149, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalli, S.; Semine, A.; Cohen, S.; Naber, S.P.; Makim, S.S.; Bahl, M. American Joint Committee on Cancer’s Staging System for Breast Cancer, Eighth Edition: What the Radiologist Needs to Know. Radiographics 2018, 38, 1921–1933. [Google Scholar] [CrossRef]
- Qu, Y.-H.; Long, N.; Ran, C.; Sun, J. The correlation of 18F-FDG PET/CT metabolic parameters, clinicopathological factors, and prognosis in breast cancer. Clin. Transl. Oncol. 2021, 23, 620–627. [Google Scholar] [CrossRef]
- Shin, Y.J.; Kim, S.M.; La Yun, B.; Jang, M.; Kim, B.; Lee, S.H. Predictors of Invasive Breast Cancer in Patients with Ductal Carcinoma in Situ in Ultrasound-Guided Core Needle Biopsy. J. Ultrasound Med. 2019, 38, 481–488. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Prognostic Stage | Anatomical Stage | ||||||
|---|---|---|---|---|---|---|---|
| TNM | Grade | Triple Positive HR+, HER2+ | Luminal-Like HR+, HER2- | HER2-Like HR±, HER2+ | HR±, HER2- | Triple Negative HR-, HER2- | |
| TisN0 | G1–3 | 0 | 0 | 0 | 0 | 0 | 0 |
| T1N0 T0–1N1mi | G1/G2 G3 | IA | IA | IA | IA | IB | IA(/IB) |
| IA | IA | IA | IA/IB(ER-) | IB | |||
| T1N1 T2N0 | G1/G2 G3 | IB | IB | IIA | IIA | IIA/IIB(G2) | IIA |
| IB | IIA | IIA | IIB | IIB | |||
| T2N1 T3N0 | G1/G2 G3 | IB | IIA | IIA/IIB(HR-) | IIB | IIB/IIIB(G2) | IIB |
| IB | IIB | IIB | IIIA | IIIB | |||
| T0–3N2 T3N1 | G1/G2 G3 | IIA | IIA | IIIA | IIIA | IIIB | IIIA |
| IIB | IIIA | IIIA | IIIB | IIIC | |||
| T4N0–2 Any N3 | G1/G2 G3 | IIIA | IIIB | IIIB | IIIB | IIIC | IIIB, IIIC |
| IIIB | IIIB | IIIB | IIIC | IIIC | |||
| Any M1 | G1–3 | IV | IV | IV | IV | IV | IV |
| Clinical Prognostic Stage | Anatomical Stage | ||||||
|---|---|---|---|---|---|---|---|
| TNM | Grade | Triple Positive HR+, HER2+ | Luminal-Like HR+, HER2- | HER2-Like HR±, HER2+ | HR±, HER2- | Triple Negative HR-, HER2- | |
| TisN0 | G1–3 | 0 | 0 | 0 | 0 | 0 | 0 |
| T1N0 T0-1N1mi | G1/G2 G3 | IA | IA | IA | IA | IA/IB(G2) | IA(/IB) |
| IA | IA | IA | IA | IB | |||
| T1N1 T2N0 | G1/G2 G3 | IA | IA | IB/IIA(HR-) | IB/IIA(G2) | IIA | IIA |
| IA | IA | IIA | IIA | IIA | |||
| T2N1 T3N0 | G1/G2 G3 | IA/IB(G2) | IA/IB(G2) | IIB | IIB | IIB | IIB |
| IB | IIA | IIB | IIB | IIIA | |||
| T0–3N2 T3N1 | G1/G2 G3 | IB | IB | IIIA | IIIA | IIIA/IIIB(G2) | IIIA |
| IIA | IIB | IIIA | IIIA | IIIC | |||
| T4N0–2 Any N3 | G1/G2 G3 | IIIA | IIIA | IIIB | IIIB | IIIB/IIIC(G2) | IIIB, IIIC |
| IIIB | IIIB | IIIB | IIIC | IIIC | |||
| Any M1 | G1–3 | IV | IV | IV | IV | IV | IV |
| Anatomical Stage (n = 358) | Clinical Prognostic Stage (n = 323) | Pathological Prognostic Stage (n = 313) | ||
|---|---|---|---|---|
| Age (years) | 58.9 ± 12.9 | 58.9 ± 12.9 | 59.0 ± 12.9 | |
| T | Tis | 37 (10.3%) | 36 (11.1%) | 36 (11.5%) |
| 1 | 196 (54.7%) | 175 (54.2%) | 186 (59.4%) | |
| 2 | 100 (27.9%) | 88 (27.2%) | 82 (26.2%) | |
| 3 | 13 (3.6%) | 12 (3.7%) | 9 (2.9%) | |
| 4 | 12 (3.4%) | 12 (3.7%) | 0 (0%) | |
| N | 0 | 248 (69.3%) | 225 (69.7%) | 232 (74.1%) |
| 1 | 72 (20.1%) | 64 (19.8%) | 57 (18.2%) | |
| 2 | 17 (4.7%) | 15 (4.6%) | 16 (5.1%) | |
| 3 | 21 (5.9%) | 19 (5.9%) | 8 (2.6%) | |
| M | 0 | 348 (97.2%) | 313 (96.9%) | 312 (99.7%) |
| 1 | 10 (2.8%) | 10 (3.1%) | 1 (0.3%) | |
| ER | + | 283 (79.1%) | 255 (78.9%) | 256 (81.8%) |
| - | 75 (20.9%) | 68 (21.1%) | 57 (18.2%) | |
| PR | + | 261 (72.9%) | 236 (73.1%) | 237 (75.7%) |
| - | 97 (27.1%) | 87 (26.9%) | 76 (24.3%) | |
| HER2 | + | 52 (14.5%) | 47 (14.6%) | 41 (13.1%) |
| - | 283 (79.1%) | 256 (79.3%) | 252 (80.5%) | |
| Unknown | 23 (6.4%) | 20 (6.2%) | 20 (6.4%) | |
| Nuclear grade | 1 | 185 (51.7%) | 168 (52.0%) | 161 (51.4%) |
| 2 | 68 (19.0%) | 66 (20.4%) | 58 (18.5%) | |
| 3 | 97 (27.1%) | 82 (25.4%) | 84 (26.8%) | |
| Unknown | 8 (2.2%) | 7 (2.2%) | 10 (3.2%) |
| Clinical Prognostic Stage | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | IA | IB | IIA | IIB | IIIA | IIIB | IIIC | IV | Total | ||
| Anatomical stage | 0 | 36 * | 36 | ||||||||
| IA | 135 * | 10 | 145 | ||||||||
| IB | 4 | 4 | |||||||||
| IIA | 2 | 44 | 7 * | 8 | 1 | 62 | |||||
| IIB | 1 | 2 | 16 | 6 * | 4 | 29 | |||||
| IIIA | 6 | 3 * | 5 | 2 | 16 | ||||||
| IIIB | 5 * | 3 | 8 | ||||||||
| IIIC | 9 | 4 * | 13 | ||||||||
| IV | 10 * | 10 | |||||||||
| Total | 36 | 142 | 56 | 29 | 14 | 3 | 24 | 9 | 10 | 323 | |
| Pathological Prognostic Stage | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | IA | IB | IIA | IIB | IIIA | IIIB | IIIC | IV | Total | ||
| Anatomical stage | 0 | 36 * | 36 | ||||||||
| IA | 144 * | 8 | 152 | ||||||||
| IB | 4 | 4 | |||||||||
| IIA | 48 | 7 | 11 * | 1 | 67 | ||||||
| IIB | 7 | 8 | 3 | 6 * | 4 | 28 | |||||
| IIIA | 5 | 5 | 3 * | 4 | 17 | ||||||
| IIIB | |||||||||||
| IIIC | 4 | 4 | 8 | ||||||||
| IV | 1 * | 1 | |||||||||
| Total | 36 | 203 | 28 | 14 | 12 | 11 | 4 | 4 | 1 | 313 | |
| Clinical Prognostic Stage (n = 323) | Pathological Prognostic Stage (n = 313) | |
|---|---|---|
| 0 | 2.2 ± 1.4 (36) | 2.2 ± 1.4 (36) |
| IA | 2.6 ± 2.1 (142) | 2.8 ± 2.2 (203) |
| IB | 4.2 ± 3.5 (36) | 5.4 ±3.6 (28) |
| IIA | 5.2 ± 2.8 (29) | 6.3 ± 3.1 (14) |
| IIB | 7.7 ± 6.7 (14) | 9.2 ± 7.5 (12) |
| IIIA | 7.9 ± 6.0 (3) | 5.4 ± 3.9 (11) |
| IIIB | 5.8 ± 4.2 (24) | 3.0 ± 0.5 (4) |
| IIIC | 9.4 ± 6.0 (9) | 11.7 ± 7.8 (4) |
| IV | 7.3 ± 2.6 (10) | 5.3 (1) |
| III + IV * | 7.0 ± 4.5 (46) * | 6.2 ± 5.2 (20) * |
| - | - | Clinical Prognostic Stage | |||
|---|---|---|---|---|---|
| - | - | 0 | I | II | III + IV |
| Pathological prognostic stage | 0 | 1.000 | <0.001 * | <0.001 * | |
| I | 0.459 | <0.001 * | <0.001 * | ||
| II | <0.001 * | <0.001 * | 1.000 | ||
| III + IV | <0.001 * | 0.004 * | 1.000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, M.; Fujioka, T.; Kubota, K.; Katsuta, L.; Yashima, Y.; Nomura, K.; Yamaga, E.; Tsuchiya, J.; Hosoya, T.; Oda, G.; et al. Relationship between Prognostic Stage in Breast Cancer and Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography. J. Clin. Med. 2021, 10, 3173. https://doi.org/10.3390/jcm10143173
Mori M, Fujioka T, Kubota K, Katsuta L, Yashima Y, Nomura K, Yamaga E, Tsuchiya J, Hosoya T, Oda G, et al. Relationship between Prognostic Stage in Breast Cancer and Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography. Journal of Clinical Medicine. 2021; 10(14):3173. https://doi.org/10.3390/jcm10143173
Chicago/Turabian StyleMori, Mio, Tomoyuki Fujioka, Kazunori Kubota, Leona Katsuta, Yuka Yashima, Kyoko Nomura, Emi Yamaga, Junichi Tsuchiya, Tokuko Hosoya, Goshi Oda, and et al. 2021. "Relationship between Prognostic Stage in Breast Cancer and Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography" Journal of Clinical Medicine 10, no. 14: 3173. https://doi.org/10.3390/jcm10143173