
Expression of Vascular Endothelial Growth Factor-C in the Trabecular Meshwork of Patients with Neovascular Glaucoma and Primary Open-Angle Glaucoma


Abstract: Purpose
1. Introduction
2. Materials and Methods
2.1. Human Surgical Sample
2.2. Immunofluorescence Microscopy
2.3. Enzyme-Linked Immunosorbent Assays (ELISA)
2.4. Cell Lines
2.5. Oxidative Stress Experiments
2.6. Hypoxic Condition
2.7. Hyperglycemic Stimulation
2.8. Western Blot Analysis
2.9. Evaluation of Apoptosis on TM Cells under Oxidative Stress
2.10. Statistical Analysis
3. Results
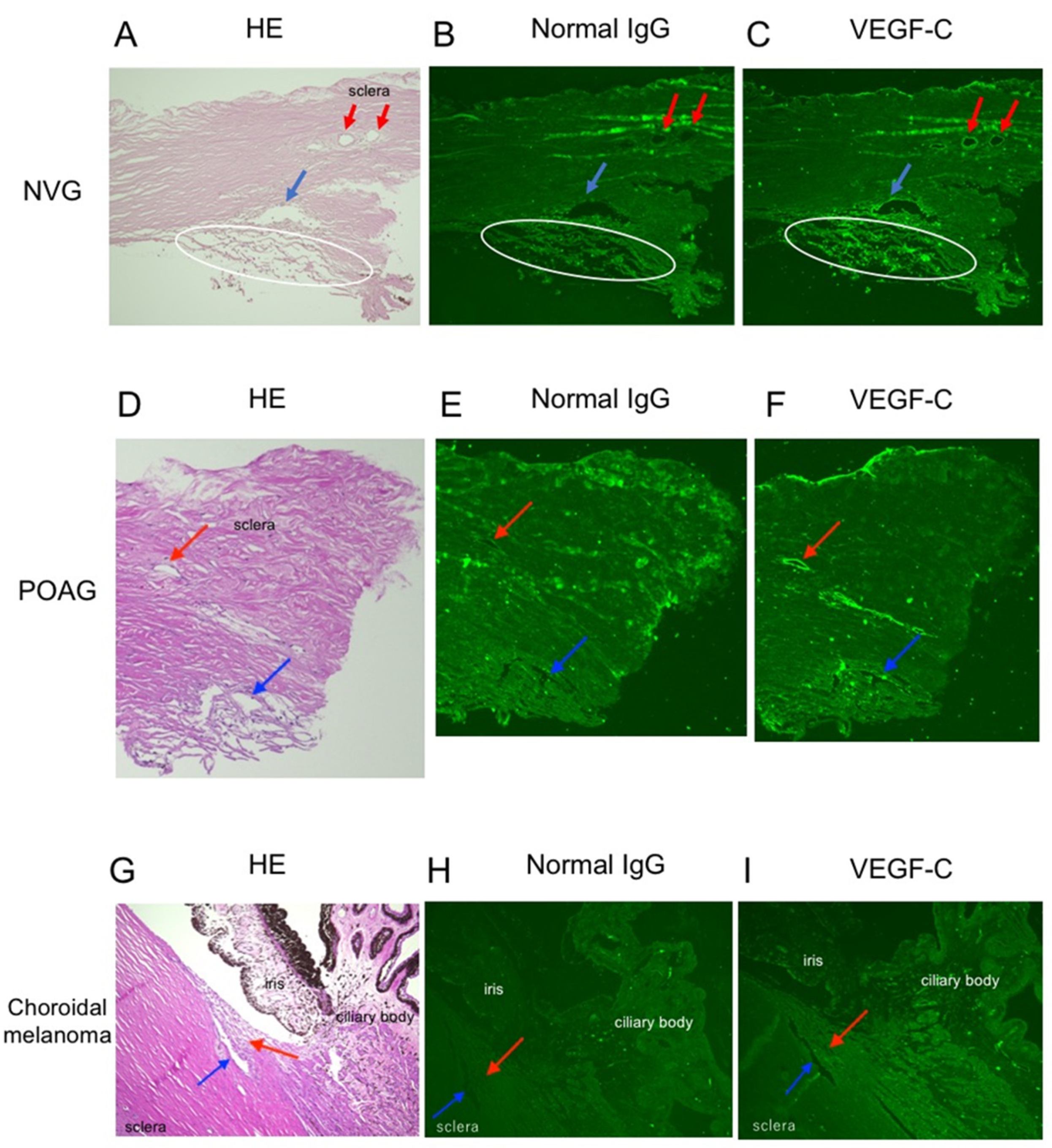
3.1. Immunoreactivity for VEGF-C in Various Angle Tissues with/without Glaucoma
3.2. VEGF-C Concentrations in the Aqueous Humor of Patients with/without Glaucoma
3.3. VEGF-C Concentrations in TM Cells Followed by Various Stimuli
3.4. VEGFR3 Protein Expression in TM Cells
3.5. Apoptosis on TM Cells under Oxidative Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Hann, C.R.; Fautsch, M.P. Recent developments in understanding the role of aqueous humor outflow in normal and primary open angle glaucoma. Curr. Ophthalmol. Rep. 2015, 3, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Mantravadi, A.V.; Vadhar, N. Glaucoma. Prim. Care 2015, 42, 437–449. [Google Scholar] [CrossRef]
- Shazly, T.A.; Latina, M.A. Neovascular glaucoma: Etiology, diagnosis and prognosis. Semin. Ophthalmol. 2009, 24, 113–121. [Google Scholar] [CrossRef]
- Havens, S.J.; Gulati, V. Neovascular glaucoma. Dev. Ophthalmol. 2016, 55, 196–204. [Google Scholar]
- Barac, I.R.; Pop, M.D.; Gheorghe, A.I.; Taban, C. Neovascular secondary glaucoma, etiology and pathogenesis. Rom. J. Ophthalmol. 2015, 59, 24–28. [Google Scholar] [PubMed]
- Tripathi, R.C.; Li, J.; Tripathi, B.J.; Chalam, K.V.; Adamis, A.P. Increased level of vascular endothelial growth factor in aqueous humor of patients with neovascular glaucoma. Ophthalmology 1998, 105, 232–237. [Google Scholar] [CrossRef]
- Simha, A.; Aziz, K.; Braganza, A.; Abraham, L.; Samuel, P.; Lindsley, K.B. Anti-vascular endothelial growth factor for neovascular glaucoma. Cochrane Database Syst. Rev. 2020, 2, CD007920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Liang, Y.; Zhou, P.; Wu, H.; Hou, X.; Ren, Z.; Li, X.; Zhao, M. Anti-VEGF treatment is the key strategy for neovascular glaucoma management in the short term. BMC Ophthalmol. 2016, 16, 150. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, R.N.; Khaw, P.T. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietze, J.; Blair, K.; Havens, S.J. Glaucoma; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Mandriota, S.J.; Jussila, L.; Jeltsch, M.; Compagni, A.; Baetens, D.; Prevo, R.; Banerji, S.; Huarte, J.; Montesano, R.; Jackson, D.G.; et al. Vascular endothelial growth factor-C-mediated lymphangiogenesis promotes tumour metastasis. EMBO J. 2001, 20, 672–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karpanen, T.; Egeblad, M.; Karkkainen, M.J.; Kubo, H.; Yla-Herttuala, S.; Jaattela, M.; Alitalo, K. Vascular endothelial growth factor C promotes tumor lymphangiogenesis and intralymphatic tumor growth. Cancer Res. 2001, 61, 1786–1790. [Google Scholar] [PubMed]
- Skobe, M.; Hawighorst, T.; Jackson, D.G.; Prevo, R.; Janes, L.; Velasco, P.; Riccardi, L.; Alitalo, K.; Claffey, K.; Detmar, M. Induction of tumor lymphangiogenesis by VEGF-C promotes breast cancer metastasis. Nat. Med. 2001, 7, 192–198. [Google Scholar] [CrossRef]
- Kovacs, K.; Marra, K.V.; Yu, G.; Wagley, S.; Ma, J.; Teague, G.C.; Nandakumar, N.; Lashkari, K.; Arroyo, J.G. Angiogenic and inflammatory vitreous biomarkers associated with increasing levels of retinal ischemia. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6523–6530. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Ge, J.; Tombran-Tink, J. Mitochondrial defects and dysfunction in calcium regulation in glaucomatous trabecular meshwork cells. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4912–4922. [Google Scholar] [CrossRef]
- McDonnell, F.; Dismuke, W.M.; Overby, D.R.; Stamer, W.D. Pharmacological regulation of outflow resistance distal to Schlemm’s canal. Am. J. Physiol. Cell Physiol. 2018, 315, C44–C51. [Google Scholar] [CrossRef]
- Carreon, T.; van der Merwe, E.; Fellman, R.L.; Johnstone, M.; Bhattacharya, S.K. Aqueous outflow—A continuum from trabecular meshwork to episcleral veins. Prog. Retin. Eye Res. 2017, 57, 108–133. [Google Scholar] [CrossRef]
- Aspelund, A.; Tammela, T.; Antila, S.; Nurmi, H.; Leppanen, V.M.; Zarkada, G.; Stanczuk, L.; Francois, M.; Makinen, T.; Saharinen, P.; et al. The Schlemm’s canal is a VEGF-C/VEGFR-3-responsive lymphatic-like vessel. J. Clin.Investig. 2014, 124, 3975–3986. [Google Scholar] [CrossRef]
- Greco, A.; Rizzo, M.I.; De Virgilio, A.; Gallo, A.; Fusconi, M.; de Vincentiis, M. Emerging Concepts in Glaucoma and Review of the Literature. Am. J. Med. 2016, 129, 1000.e7–1000.e13. [Google Scholar] [CrossRef]
- Wang, J.F.; Zhang, X.; Groopman, J.E. Activation of vascular endothelial growth factor receptor-3 and its downstream signaling promote cell survival under oxidative stress. J. Biol. Chem. 2004, 279, 27088–27097. [Google Scholar] [CrossRef] [Green Version]
- Morfoisse, F.; Kuchnio, A.; Frainay, C.; Gomez-Brouchet, A.; Delisle, M.B.; Marzi, S.; Helfer, A.C.; Hantelys, F.; Pujol, F.; Guillermet-Guibert, J.; et al. Hypoxia induces VEGF-C expression in metastatic tumor cells via a HIF-1alpha-independent translation-mediated mechanism. Cell Rep. 2014, 6, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Simiantonaki, N.; Jayasinghe, C.; Michel-Schmidt, R.; Peters, K.; Hermanns, M.I.; Kirkpatrick, C.J. Hypoxia-induced epithelial VEGF-C/VEGFR-3 upregulation in carcinoma cell lines. Int. J. Oncol. 2008, 32, 585–592. [Google Scholar] [CrossRef]
- Davies, P.D.; Duncan, G.; Pynsent, P.B.; Arber, D.L.; Lucas, V.A. Aqueous humour glucose concentration in cataract patients and its effect on the lens. Exp. Eye Res. 1984, 39, 605–609. [Google Scholar] [CrossRef]
- Sato, T.; Roy, S. Effect of high glucose on fibronectin expression and cell proliferation in trabecular meshwork cells. Investig. Ophthalmol. Vis. Sci. 2002, 43, 170–175. [Google Scholar]
- Varney, M.L.; Singh, R.K. VEGF-C-VEGFR3/Flt4 axis regulates mammary tumor growth and metastasis in an autocrine manner. Am. J. Cancer Res. 2015, 5, 616–628. [Google Scholar]
- Garces, C.A.; Kurenova, E.V.; Golubovskaya, V.M.; Cance, W.G. Vascular endothelial growth factor receptor-3 and focal adhesion kinase bind and suppress apoptosis in breast cancer cells. Cancer Res. 2006, 66, 1446–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baleriola, J.; Garcia-Feijoo, J.; Martinez-de-la-Casa, J.M.; Fernandez-Cruz, A.; de la Rosa, E.J.; Fernandez-Durango, R. Apoptosis in the trabecular meshwork of glaucomatous patients. Mol. Vis. 2008, 14, 1513–1516. [Google Scholar]
- Kumar, B.; Chile, S.A.; Ray, K.B.; Reddy, G.E.; Addepalli, M.K.; Kumar, A.S.; Ramana, V.; Rajagopal, V. VEGF-C differentially regulates VEGF-A expression in ocular and cancer cells; promotes angiogenesis via RhoA mediated pathway. Angiogenesis 2011, 14, 371–380. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NVG | POAG | CAT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No. | Gender | Age (Years) | Primary Disease | No. | Gender | Age (Years) | No. | Gender | Age (Years) |
| 1 | M | 52 | PDR | 1 | M | 60 | 1 | M | 70 |
| 2 | F | 66 | RR | 2 | M | 64 | 2 | M | 81 |
| 3 | M | 66 | RR | 3 | F | 57 | 3 | F | 80 |
| 4 | M | 65 | PDR | 4 | M | 50 | 4 | F | 62 |
| 5 | M | 72 | OIS | 5 | F | 75 | 5 | F | 72 |
| 6 | M | 74 | CRVO | 6 | F | 50 | 6 | F | 78 |
| 7 | M | 61 | CRVO | 7 | F | 64 | |||
| 8 | M | 74 | RR | 8 | F | 65 | |||
| 9 | M | 61 | PDR | 9 | M | 76 | |||
| 10 | M | 52 | PDR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hase, K.; Kase, S.; Kanda, A.; Shinmei, Y.; Noda, K.; Ishida, S. Expression of Vascular Endothelial Growth Factor-C in the Trabecular Meshwork of Patients with Neovascular Glaucoma and Primary Open-Angle Glaucoma. J. Clin. Med. 2021, 10, 2977. https://doi.org/10.3390/jcm10132977
Hase K, Kase S, Kanda A, Shinmei Y, Noda K, Ishida S. Expression of Vascular Endothelial Growth Factor-C in the Trabecular Meshwork of Patients with Neovascular Glaucoma and Primary Open-Angle Glaucoma. Journal of Clinical Medicine. 2021; 10(13):2977. https://doi.org/10.3390/jcm10132977
Chicago/Turabian StyleHase, Keitaro, Satoru Kase, Atsuhiro Kanda, Yasuhiro Shinmei, Kousuke Noda, and Susumu Ishida. 2021. "Expression of Vascular Endothelial Growth Factor-C in the Trabecular Meshwork of Patients with Neovascular Glaucoma and Primary Open-Angle Glaucoma" Journal of Clinical Medicine 10, no. 13: 2977. https://doi.org/10.3390/jcm10132977