
Effect of Posterior Pelvic Tilt Taping on Pelvic Inclination, Muscle Strength, and Gait Ability in Stroke Patients: A Randomized Controlled Study


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
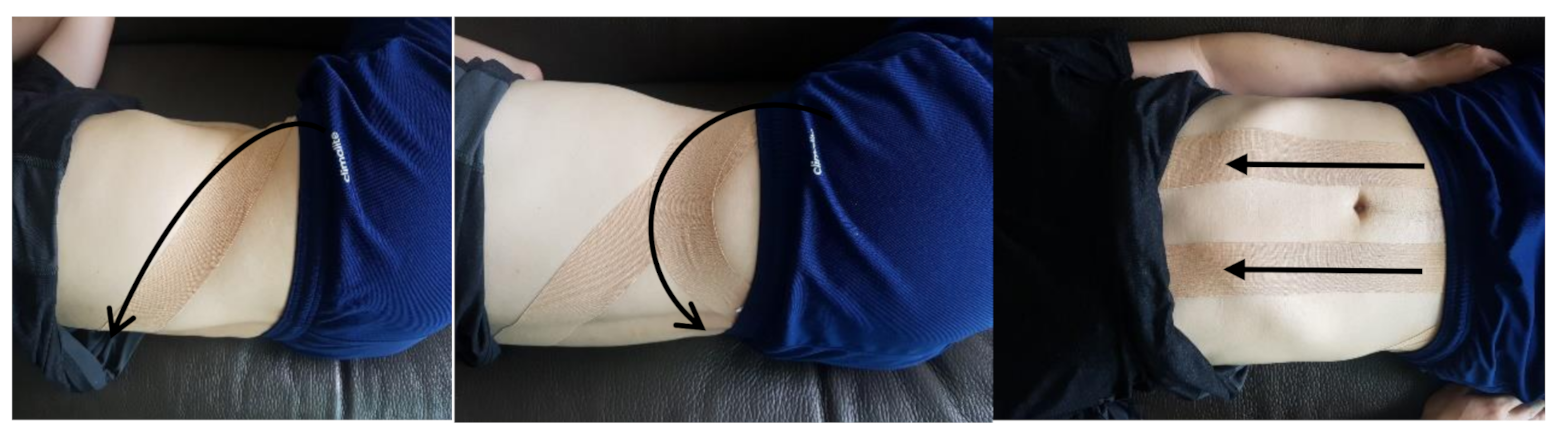
2.2. Intervention
2.3. Outcome Measurements
2.4. Data Analysis
3. Results
3.1. General Characteristics of Participants
3.2. Changes in Pelvic Inclination
3.3. Changes in Muscle Strength
3.4. Changes in Gait Speed
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dubey, L.; Karthikbabu, S.; Mohan, D. Effects of Pelvic Stability Training on Movement Control, Hip Muscles Strength, Walking Speed and Daily Activities after Stroke: A Randomized Controlled Trial. Ann. Neurosci. 2018, 25, 80–89. [Google Scholar] [CrossRef]
- Verheyden, G.; Vereeck, L.; Truijen, S.; Troch, M.; Herregodts, I.; Lafosse, C.; Nieuwboer, A.; De Weerdt, W. Trunk performance after stroke and the relationship with balance, gait and functional ability. Clin. Rehabil. 2006, 20, 451–458. [Google Scholar] [CrossRef]
- Staszkiewicz, R.; Chwala, W.; Forczek, W.; Laska, J. Three-dimensional analysis of the pelvic and hip mobility during gait on a treadmill and on the ground. Acta. Bioeng. Biomech. 2012, 14, 83–89. [Google Scholar]
- Chen, C.L.; Chen, H.C.; Tang, S.F.T.; Wu, C.Y.; Cheng, P.T.; Hong, W.H. Gait performance with compensatory adaptations in stroke patients with different degrees of motor recovery. Am. J. Phys. Med. Rehabil. 2003, 82, 925–935. [Google Scholar] [CrossRef]
- Dickstein, R.; Abulaffio, N. Postural sway of the affected and nonaffected pelvis and leg in stance of hemiparetic patients. Arch. Phys. Med. Rehabil. 2000, 81, 364–367. [Google Scholar] [CrossRef]
- Titianova, E.B.; Tarkka, I.M. Asymmetry in walking performance and postural sway in patients with chronic unilateral cerebral infarction. J. Rehabil. Res. Dev. 1995, 32, 236–244. [Google Scholar]
- Lomaglio, M.J.; Eng, J.J. Muscle strength and weight-bearing symmetry relate to sit-to-stand performance in individuals with stroke. Gait. Posture 2005, 22, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Tyson, S.F. Trunk kinematics in hemiplegic gait and the effect of walking aids. Clin. Rehabil. 1999, 13, 295–300. [Google Scholar] [CrossRef]
- Karthikbabu, S.; Chakrapani, M.; Ganesan, S.; Ellajosyula, R. Relationship between Pelvic Alignment and Weight-bearing Asymmetry in Community-dwelling Chronic Stroke Survivors. J. Neurosci. Rural Pract. 2016, 7, S37–S40. [Google Scholar] [CrossRef]
- Verheyden, G.; Ruesen, C.; Gorissen, M.; Brumby, V.; Moran, R.; Burnett, M.; Ashburn, A. Postural alignment is altered in people with chronic stroke and related to motor and functional performance. J. Neurol. Phys. Ther. 2014, 38, 239–245. [Google Scholar] [CrossRef]
- Briem, K.; Eythörsdöttir, H.; Magnúsdóttir, R.G.; Pálmarsson, R.; Rúnarsdöttir, T.; Sveinsson, T. Effects of kinesio tape compared with nonelastic sports tape and the untapped ankle during a sudden inversion perturbation in male athletes. J. Orthop. Sports Phys. Ther. 2011, 41, 328–335. [Google Scholar] [CrossRef] [Green Version]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic Applications of the Kinesio Taping Method, 2nd ed.; Kinesio Taping Association: Tokyo, Japan, 2003; pp. 19–39. [Google Scholar]
- Lee, H.; Lim, H. Effects of Double-Taped Kinesio Taping on Pain and Functional Performance due to Muscle Fatigue in Young Males: A Randomized Controlled Trial. Int. J. Environ. Res. Public. Health 2020, 17, 2364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoloni, M.; Bernetti, A.; Fratocchi, G.; Mangone, M.; Parrinello, L.; Cooper, M.D.P.; Sesto, L.; Di Sante, L.; Santilli, V. Kinesio taping applied to lumbar muscles influences clinical and electromyographic characteristics in chronic low back pain patients. Eur. J. Phys. Rehabil. Med. 2011, 47, 237–244. [Google Scholar] [PubMed]
- Lee, J.H.; Yoo, W.G.; Gak, H.B. The immediate effect of anterior pelvic tilt taping on pelvic inclination. J. Phys. Ther. Sci. 2011, 23, 201–203. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Yoo, W.G. The mechanical effect of anterior pelvic tilt taping on slump sitting by seated workers. Ind. Health 2011, 49, 403–409. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Yoo, W.G. Application of posterior pelvic tilt taping for the treatment of chronic low back pain with sacroiliac joint dysfunction and increased sacral horizontal angle. Phys. Ther. Sport 2012, 13, 279–285. [Google Scholar] [CrossRef]
- Bozorgmehr, A.; Takamjani, E.I.; Akbari, M.; Salehi, R.; Mohsenifar, H.; Rasouli, O. Effect of Posterior Pelvic Tilt Taping on Abdominal Muscle Thickness and Lumbar Lordosis in Individuals With Chronic Low Back Pain and Hyperlordosis: A Single-Group, Repeated-Measures Trial. J. Chiropr. Med. 2020, 19, 213–221. [Google Scholar] [CrossRef]
- Lee, J.H.; Yoo, W.G.; Kim, M.H.; Oh, J.S.; Lee, K.S.; Han, J.T. Effect of posterior pelvic tilt taping in women with sacroiliac joint pain during active straight leg raising who habitually wore high-heeled shoes: A preliminary study. J. Manip. Physiol. Ther. 2014, 37, 260–268. [Google Scholar] [CrossRef]
- Mehta, M.; Joshua, A.M.; Karthikbabu, S.; Misri, Z.; Unnikrishnan, B.; Mithra, P.; Nayak, A. Effect of Taping of Thoracic and Abdominal Muscles on Pelvic Alignment and Forward Reach Distance Among Stroke Subjects: A Randomized Controlled Trial. Ann. Neurosci. 2019, 26, 10–16. [Google Scholar] [CrossRef]
- Ting, W.Y. The Immediate Effect of Posterior Pelvic Tilt Taping on Gait Function and Balance in Chronic Stroke Patients. Master’s Thesis, Daegu University, Daegu, Korea, 2017. [Google Scholar]
- Kim, M.K.; Kim, S.G.; Shin, Y.J.; Choi, E.H.; Choe, Y.W. The relationship between anterior pelvic tilt and gait, balance in patient with chronic stroke. J. Phys. Ther. Sci. 2018, 30, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Hagins, M.; Brown, M.; Cook, C.; Gstalder, K.; Kam, M.; Kominer, G.; Strimbeck, K. Intratester and intertester reliability of the palpation meter (PALM) in measuring pelvic position. J. Manual. Manip. Ther. 1998, 6, 130–136. [Google Scholar] [CrossRef]
- Levine, D.; Whittle, M.W. The effects of pelvic movement on lumbar lordosis in the standing position. J. Orthop. Sports Phys. Ther. 1996, 24, 130–135. [Google Scholar] [CrossRef]
- Gnat, R.; Saulicz, E.; Bia1y, M.; K1aptocz, P. Does pelvic asymmetry always mean pathology? Analysis of mechanical factors leading to the asymmetry. J. Hum. Kinet. 2009, 21, 23–35. [Google Scholar] [CrossRef]
- Bohannon, R.W. Test-retest reliability of hand-held dynamometry during a single session of strength assessment. Phys. Ther. 1986, 66, 206–209. [Google Scholar] [CrossRef]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar]
- Shim, J.Y.; Lee, H.R.; Lee, D.C. The use of elastic adhesive tape to promote lymphatic flow in the rabbit hind leg. Yonsei Med. J. 2003, 44, 1045–1052. [Google Scholar] [CrossRef]
- Chang, H.Y.; Chou, K.Y.; Lin, J.J.; Lin, C.F.; Wang, C.H. Immediate effect of forearm Kinesio taping on maximal grip strength and force sense in healthy collegiate athletes. Phys. Ther. Sport 2010, 11, 122–127. [Google Scholar] [CrossRef]
- Lee, D. The Pelvic Girdle: An Integration of Clinical Expertise and Research, 3rd ed.; Churchill Livingstone: London, UK, 2004. [Google Scholar]
- Yu, S.H.; Park, S.D. The effects of core stability strength exercise on muscle activity and trunk impairment scale in stroke patients. J. Exerc. Rehabil. 2013, 9, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Patterson, K.K.; Parafianowicz, I.; Danells, C.J.; Closson, V.; Verrier, M.C.; Staines, W.R.; Black, S.E.; McIlroy, W.E. Gait asymmetry in community-ambulating stroke survivors. Arch. Phys. Med. Rehabil. 2008, 89, 304–310. [Google Scholar] [CrossRef]
- Moore, S.; Schurr, K.; Wales, A.; Moseley, A.; Herbert, R. Observation and analysis of hemiplegic gait: Swing phase. Aust. J. Physiother. 1993, 39, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Cruz, T.H.; Lewek, M.D.; Dhaher, Y.Y. Biomechanical impairments and gait adaptations post-stroke: Multi-factorial associations. J. Biomech. 2009, 42, 1673–1677. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | PPTT Group (n = 20) | Control Group (n = 20) | p |
|---|---|---|---|
| Sex (male/female) | 14/6 | 15/5 | 0.723 b |
| Affected side(right/left) | 12/8 | 11/9 | 0.749 b |
| Age (years) | 55.8 ± 8.5 a | 54.4 ± 9.9 | 0.361 c |
| Height (cm) | 165.9 ± 9.1 | 166.5 ± 9.9 | 0.856 c |
| Weight (kg) | 62.4 ± 8.7 | 63.9 ± 8.4 | 0.758 c |
| Stroke duration (months) | 8.0 ± 1.9 | 7.1 ± 2.6 | 0.315 c |
| Disease (diabetes/hypercholesterolemia/hypertension/≥ 2) | 1/1/12/6 | 1/2/10/7 | |
| Work (engineer/white-collar jobs/etc.) | 5/10/5 | 6/8/6 | |
| Sport activities (none/running/golf/tennis) | 14/3/3/2 | 12/4/3/1 |
| PPTT Group | Control Group | Difference | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Difference | Pre-Test | Post-Test | |||
| Pelvic inclination (°) | 18.2 ± 3.6 | 14.2 ± 2.8 * | −4.0 ± 2.8 | 16.9 ± 2.8 | 15.5 ± 2.8 * | −1.4 ± 1.2 | <0.001 |
| PPTT Group | Control Group | Difference | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Difference | Pre-Test | Post-Test | |||
| Muscle strength (kg) | 9.9 ± 2.4 | 14.6 ± 3.0 * | 4.7 ± 2.3 | 10.7 ± 1.7 | 12.6 ± 1.6 * | 1.8 ± 1.7 | <0.001 |
| PPTT Group | Control Group | Difference | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Difference | Pre-Test | Post-Test | |||
| 10MWT (sec) | 26.0 ± 5.1 | 21.1 ± 4.1 * | −4.9 ± 1.6 | 24.6 ± 4.6 | 22.3 ± 4.0 * | −2.3 ± 2.8 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
In, T.-s.; Jung, J.-h.; Kim, M.; Jung, K.-s.; Cho, H.-y. Effect of Posterior Pelvic Tilt Taping on Pelvic Inclination, Muscle Strength, and Gait Ability in Stroke Patients: A Randomized Controlled Study. J. Clin. Med. 2021, 10, 2381. https://doi.org/10.3390/jcm10112381
In T-s, Jung J-h, Kim M, Jung K-s, Cho H-y. Effect of Posterior Pelvic Tilt Taping on Pelvic Inclination, Muscle Strength, and Gait Ability in Stroke Patients: A Randomized Controlled Study. Journal of Clinical Medicine. 2021; 10(11):2381. https://doi.org/10.3390/jcm10112381
Chicago/Turabian StyleIn, Tae-sung, Jin-hwa Jung, May Kim, Kyoung-sim Jung, and Hwi-young Cho. 2021. "Effect of Posterior Pelvic Tilt Taping on Pelvic Inclination, Muscle Strength, and Gait Ability in Stroke Patients: A Randomized Controlled Study" Journal of Clinical Medicine 10, no. 11: 2381. https://doi.org/10.3390/jcm10112381