
Effects of Whole-Body Vibration and Balance Training on Female Athletes with Chronic Ankle Instability


Abstract
:1. Introduction
2. Methods
2.1. Study Procedures
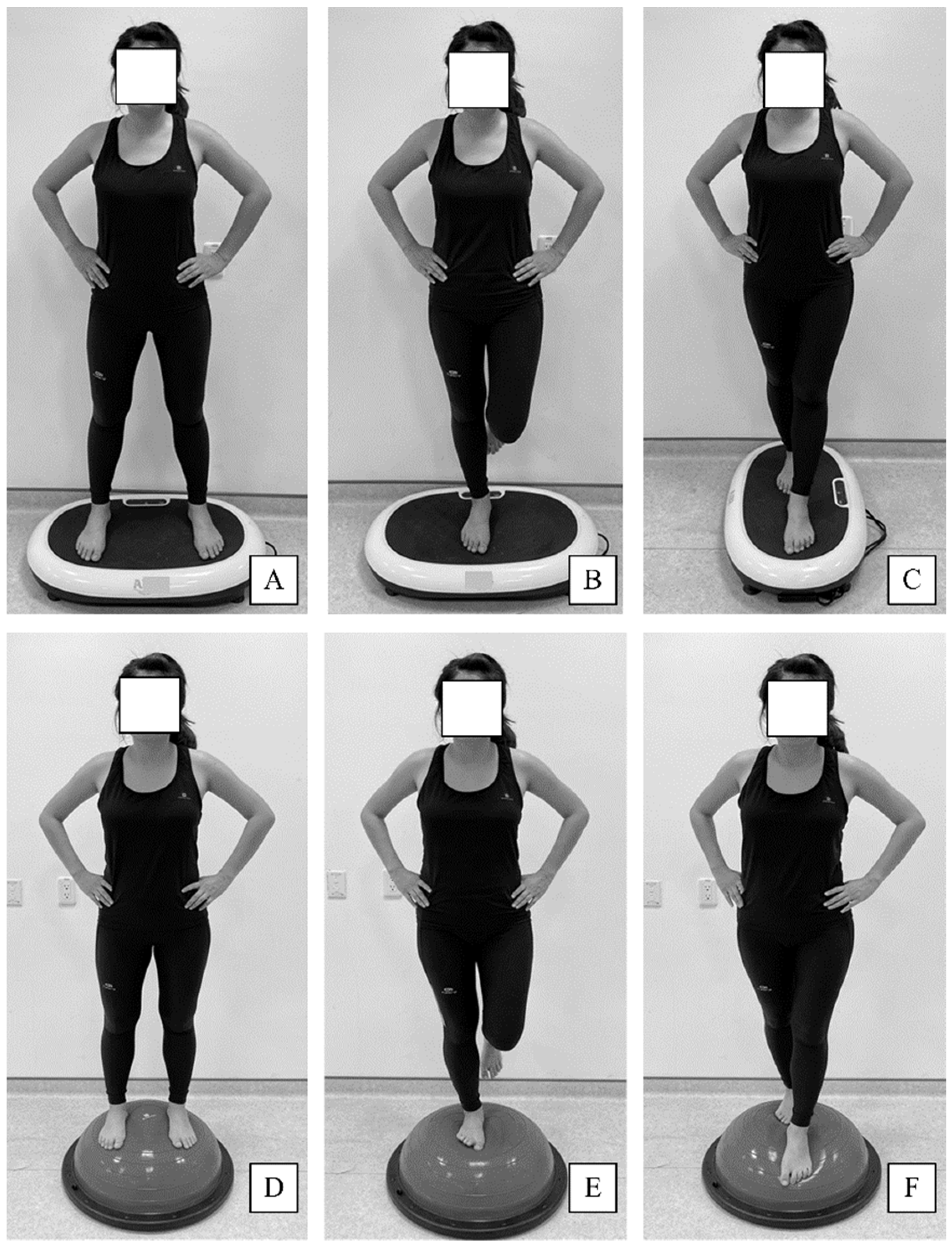
2.2. Exercise Training Program
2.3. Assessments
2.3.1. Star Excursion Balance Test
2.3.2. Joint Position Sense Test
2.3.3. Isokinetic Strength Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| WBV | whole-body vibration |
| CAI | chronic ankle instability |
| SEBT | Star Excursion Balance Test |
| CON | concentric contraction |
| ECC | eccentric contraction |
References
- Sierra-Guzmán, R.; Jiménez, F.; Abián-Vicén, J. Predictors of chronic ankle instability: Analysis of peroneal reaction time, dynamic balance and isokinetic strength. Clin. Biomech. 2018, 54, 28–33. [Google Scholar] [CrossRef]
- Eechaute, C.; Vaes, P.; Duquet, W. The dynamic postural control is impaired in patients with chronic ankle instability: Reliability and validity of the multiple hop test. Clin. J. Sport Med. 2009, 19, 107–114. [Google Scholar] [CrossRef]
- Delahunt, E.; Coughlan, G.F.; Caulfield, B.; Nightingale, E.J.; Lin, C.W.; Hiller, C.E. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med. Sci. Sports Exerc. 2010, 42, 2106–2121. [Google Scholar] [CrossRef]
- Schiftan, G.S.; Ross, L.A.; Hahne, A.J. The effectiveness of proprioceptive training in preventing ankle sprains in sporting populations: A systematic review and meta-analysis. J. Sci. Med. Sport. 2015, 18, 238–244. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, R.; Willems, T.; Vanrenterghem, J.; Roosen, P. Influence of balance surface on ankle stabilizing muscle activity in subjects with chronic ankle instability. J. Rehabil. Med. 2015, 47, 632–638. [Google Scholar] [CrossRef] [Green Version]
- Levin, O.; Vanwanseele, B.; Thijsen, J.R.; Helsen, W.F.; Staes, F.F.; Duysens, J. Proactive and reactive neuromuscular control in subjects with chronic ankle instability: Evidence from a pilot study on landing. Gait Posture 2015, 41, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Cloak, R.; Nevill, A.; Day, S.; Wyon, M. Six-week combined vibration and wobble board training on balance and stability in footballers with functional ankle instability. Clin. J. Sport Med. 2013, 23, 384–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardinale, M.; Bosco, C. The use of vibration as an exercise intervention. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.D.; Woledge, R.C.; Martin, F.C.; Newham, D.J. Effects of whole body vibration on motor unit recruitment and threshold. J. Appl. Physiol. 2012, 112, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Peters, M. Footedness: Asymmetries in foot preference and skill and neuropsychological assessment of foot movement. Psychol. Bull. 1988, 103, 179–192. [Google Scholar] [CrossRef] [PubMed]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldemeyer, L.E.; Brown, S.M.; Mulcahey, M.K. Neuromuscular training for the prevention of ankle sprains in female athletes: A systematic review. Phys. Sportsmed. 2020, 48, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Ristolainen, L.; Heinonen, A.; Waller, B.; Kujala, U.M.; Kettunen, J.A. Gender differences in sport injury risk and types of inju-ries: A retrospective twelve-month study on cross-country skiers, swimmers, long-distance runners and soccer players. J. Sports Sci. Med. 2009, 8, 443–451. [Google Scholar] [PubMed]
- Hosea, T.M.; Carey, C.C.; Harrer, M.F. The gender issue: Epidemiology of ankle injuries in athletes who participate in basketball. Clin. Orthop. Relat. Res. 2000, 372, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Brumitt, J.; Mattocks, A.; Loew, J.; Lentz, P. Preseason functional performance test measures are associated with injury in female college volleyball players. J. Sport Rehabil. 2020, 29, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.M.; Caulfield, B.; Docherty, C.L.; Fong, D.T.; Fourchet, F.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J. Athl. Train. 2014, 49, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sefton, J.M.; Yarar, C.; Hicks-Little, C.A.; Berry, J.W.; Cordova, M.L. Six weeks of balance training improves sensorimotor function in individuals with chronic ankle instability. J. Orthop. Sports Phys. Ther. 2011, 41, 81–89. [Google Scholar] [CrossRef]
- Hertel, J.; Miller, S.; Denegar, C. Intratester and intertester reliability during the Star Excursion Balance Tests. J. Sport Rehab. 2000, 9, 104–116. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J.; Braham, R.A.; Hale, S.A.; Olmsted-Kramer, L.C. Simplifying the star excursion balance test: Analyses of subjects with and without chronic ankle instability. J. Orthop. Sports Phys. Ther. 2006, 36, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Sekir, U.; Yildiz, Y.; Hazneci, B.; Ors, F.; Saka, T.; Aydin, T. Reliability of a functional test battery evaluating functionality, proprioception, and strength in recreational athletes with functional ankle instability. Eur. J. Phys. Rehabil. Med. 2008, 44, 407–415. [Google Scholar]
- Brown, C.; Ross, S.; Mynark, R.; Guskiewics, K. Assessing functional ankle instability with joint position sense, time to stabilization, and electromyography. J. Sport Rehabil. 2004, 13, 122–134. [Google Scholar] [CrossRef]
- Tankevicius, G.; Lankaite, D.; Krisciunas, A. Test-retest reliability of biodex system 4 pro for isometric ankle-eversion and -inversion measurement. J. Sport Rehabil. 2013, 22, 212–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fish, M.; Milligan, J.; Killey, J. Is it possible to establish reference values for ankle muscle isokinetic strength? A meta-analytical study. Isokinet. Exerc. Sci. 2014, 22, 85–97. [Google Scholar] [CrossRef] [Green Version]
- Kaminski, T.W.; Buckley, B.D.; Powers, M.E.; Hubbard, T.J.; Ortiz, C. Effect of strength and proprioception training on eversion to inversion strength ratios in subjects with unilateral functional ankle instability. Br. J. Sports Med. 2003, 37, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Willems, T.M.; Witvrouw, E.; Delbaere, K.; Philippaerts, R.; De Bourdeaudhuij, I.; De Clercq, D. Intrinsic risk factors for inversion ankle sprains in females—A prospective study. Scand. J. Med. Sci. Sports 2005, 15, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Renström, P.A.; Alosa, D.M.; Baumhauer, J.F.; Vacek, P.M. Ankle ligament injury risk factors: A prospective study of college athletes. J. Orthop. Res. 2001, 19, 213–220. [Google Scholar] [CrossRef]
- Quatman, C.E.; Ford, K.R.; Myer, G.D.; Paterno, M.V.; Hewett, T.E. The effects of gender and pubertal status on generalized joint laxity in young athletes. J. Sci. Med. Sport 2008, 11, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Frank, R.M.; Romeo, A.A.; Bush-Joseph, C.A.; Bach, B.R., Jr. Injuries to the female athlete in 2017: Part II: Upper and lower-extremity injuries. JBJS Rev. 2017, 5, e5. [Google Scholar] [CrossRef]
- Pierobon, A.; Raguzzi, I.; Soliño, S.; Salzberg, S.; Vuoto, T.; Gilgado, D.; Perez Calvo, E. Minimal detectable change and reliability of the star excursion balance test in patients with lateral ankle sprain. Physiother. Res. Int. 2020, 25, 1850. [Google Scholar] [CrossRef]
- Halabchi, F.; Hassabi, M. Acute ankle sprain in athletes: Clinical aspects and algorithmic approach. World J. Orthop. 2020, 11, 534–558. [Google Scholar] [CrossRef] [PubMed]
- D’Hooghe, P.; Cruz, F.; Alkhelaifi, K. Return to play after a lateral ligament ankle sprain. Curr. Rev. Musculoskelet. Med. 2020, 13, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.G.; Koschnitzky, M.M. Ankle muscle activation when using the Both Sides Utilized (BOSU) balance trainer. J. Strength Cond. Res. 2010, 24, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Strøm, M.; Thorborg, K.; Bandholm, T.; Tang, L.; Zebis, M.; Nielsen, K.; Bencke, J. Ankle joint control during single-legged balance using common balance training devices–implications for rehabilitation strategies. Int. J. Sports Phys. Ther. 2016, 11, 388–399. [Google Scholar] [PubMed]
- Rendos, N.K.; Jun, H.P.; Pickett, N.M.; Lew Feirman, K.; Harriell, K.; Lee, S.Y.; Signorile, J.F. Acute effects of whole body vibration on balance in persons with and without chronic ankle instability. Res. Sports Med. 2017, 25, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Guzmán, R.; Jiménez-Diaz, F.; Ramírez, C.; Esteban, P.; Abián-Vicén, J. Whole-body-vibration training and balance in recreational athletes with chronic ankle instability. J. Athl. Train. 2018, 53, 355–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, X.; Ma, T.; Li, Q.; Song, Y.; Hua, Y. Chronic ankle instability is associated with proprioception deficits: A systematic review with meta-analysis. J. Sport Health Sci. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Sousa, A.S.P.; Leite, J.; Costa, B.; Santos, R. Bilateral proprioceptive evaluation in individuals with unilateral chronic ankle instability. J. Athl. Train. 2017, 52, 360–367. [Google Scholar] [CrossRef]
- Lönn, J.; Crenshaw, A.G.; Djupsjöbacka, M.; Pedersen, J.; Johansson, H. Position sense testing: Influence of starting position and type of displacement. Arch. Phys. Med. Rehabil. 2000, 81, 592–597. [Google Scholar] [CrossRef]
- Otzel, D.M.; Hass, C.J.; Wikstrom, E.A.; Bishop, M.D.; Borsa, P.A.; Tillman, M.D. Motoneuron function does not change following whole-body vibration in individuals with chronic ankle instability. J. Sport Rehabil. 2019, 28, 614–622. [Google Scholar] [CrossRef]
- Baumbach, S.F.; Fasser, M.; Polzer, H.; Sieb, M.; Regauer, M.; Mutschler, W.; Schieker, M.; Blauth, M. Study protocol: The effect of whole body vibration on acute unilateral unstable lateral ankle sprain—A biphasic randomized controlled trial. BMC Musculoskelet. Disord. 2013, 14, 22. [Google Scholar] [CrossRef] [Green Version]
- Rittweger, J.; Just, K.; Kautzsch, K.; Reeg, P.; Felsenberg, D. Treatment of chronic lower back pain with lumbar extension and whole-body vibration exercise: A randomized controlled trial. Spine 2002, 27, 1829–1834. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, G.B.; Pinerola, J.J.; Caturano, R.W. Invertor vs. evertor peak torque and power deficiencies associated with lateral ankle ligament injury. J. Orthop. Sports Phys. Ther. 1997, 26, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J. Functional snatomy, pathomechanics, and pathophysiology of lateral ankle instability. J. Athl. Train. 2002, 37, 364–375. [Google Scholar] [PubMed]
- Ko, K.R.; Lee, H.; Lee, W.Y.; Sung, K.S. Ankle strength is not strongly associated with postural stability in patients awaiting surgery for chronic lateral ankle instability. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 326–333. [Google Scholar] [CrossRef]
- Munn, J.; Beard, D.J.; Refshauge, K.M.; Lee, R.Y. Eccentric muscle strength in functional ankle instability. Med. Sci. Sports Exerc. 2003, 35, 245–250. [Google Scholar] [CrossRef]
- Willems, T.; Witvrouw, E.; Verstuyft, J.; Vaes, P.; De Clercq, D. Proprioception and muscle strength in subjects with a history of ankle sprains and chronic instability. J. Athl. Train. 2002, 37, 487–493. [Google Scholar]
- Bosien, W.R.; Staples, S.; Russell, S.W. Residual disability following acute ankle sprains. J. Bone Jt. Surg. Am. 1955, 37, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Brent, I.S.; Carrie, L.D.; Janet, S.; Joanne, K.; John, S. Ankle strength and force sense after a progressive, 6-week strength training programme in people with functional ankle instability. J. Athl. Train. 2012, 47, 282–288. [Google Scholar]
- Yildiz, Y.; Aydin, T.; Sekir, U.; Hazneci, B.; Komurcu, M.; Kalyon, T.A. Peak and end range eccentric evertor/concentric invertor muscle strength ratios in chronically unstable ankles: Comparison with healthy individuals. J. Sports Sci. Med. 2003, 2, 70–76. [Google Scholar]
- Mohd Salim, N.S.; Umar, M.A.; Shaharudin, S. Effects of the standard physiotherapy programme on pain and isokinetic ankle strength in individuals with grade I ankle sprain. J. Taibah. Univ. Med. Sci. 2018, 13, 576–581. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group A (n = 21) | Group B (n = 21) | Group C (n = 21) | p | |
|---|---|---|---|---|
| Age (y) | 20.31 ± 1.28 | 20.43 ± 1.25 | 21.23 ± 1.47 | 0.08 |
| Height (cm) | 168.34 ± 5.78 | 166.8 ± 6.84 | 169.53 ± 4.78 | 0.32 |
| Weight (kg) | 61.01 ± 22.39 | 58.83 ± 13.14 | 58.67 ± 16.54 | 0.89 |
| Dominant leg (Lt/Rt) | 5/16 | 4/17 | 5/16 | 0.91 |
| Composite score of CAIT | 19.21 ± 1.89 | 19.14 ± 2.01 | 19.25 ± 1.91 | 0.89 |
| Assessed Variables | Group | Time | Time × Group | ||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |
| Composite of star excursion balance test | 5.30 | 0.03 | 0.54 | 67.78 | 0.001 | 0.87 | 17.84 | 0.001 | 0.79 |
| Active repositioning | |||||||||
| 15° of ankle inversion | 3.35 | 0.08 | 0.42 | 12.37 | 0.006 | 0.55 | 0.48 | 0.63 | 0.09 |
| 0° in ankle neutral position | 6.59 | 0.01 | 0.59 | 12.26 | 0.006 | 0.54 | 1.58 | 0.25 | 0.26 |
| 10° of ankle eversion | 0.51 | 0.61 | 0.10 | 8.27 | 0.01 | 0.45 | 1.60 | 0.25 | 0,27 |
| Passive repositioning | |||||||||
| 15° of ankle inversion | 1.27 | 0.32 | 0.22 | 1.15 | 0.32 | 0.10 | 0.34 | 0.71 | 0.07 |
| 0° in ankle neutral position | 0.16 | 0.84 | 0.03 | 0.67 | 0.42 | 0.06 | 0.18 | 0.83 | 0.03 |
| 10° of ankle eversion | 0.56 | 0.58 | 0.11 | 0.70 | 0.41 | 0.06 | 0.87 | 0.44 | 0.16 |
| Ankle inversion | |||||||||
| 30°/s COM (N-m/kg) | 3.01 | 0.10 | 0.40 | 0.04 | 0.82 | 0.01 | 4.49 | 0.04 | 0.50 |
| 30°/s ECC (N-m/kg) | 14.02 | 0.002 | 0.75 | 5.56 | 0.04 | 0.35 | 0.71 | 0.51 | 0.13 |
| 120°/s COM (N-m/kg) | 1.42 | 0.28 | 0.24 | 2.44 | 0.14 | 0.19 | 0.97 | 0.41 | 0.17 |
| 120°/s ECC (N-m/kg) | 1.83 | 021 | 029 | 001 | 056 | 001 | 022 | 045 | 0.04 |
| Ankle eversion | |||||||||
| 30°/s COM (N-m/kg) | 1.53 | 0.26 | 0.25 | 2.76 | 0.12 | 0.21 | 0.53 | 0.60 | 0.10 |
| 30°/s ECC (N-m/kg) | 0.16 | 0.85 | 0.03 | 0.49 | 0.48 | 0.04 | 0.22 | 0.80 | 0.04 |
| 120°/s COM (N-m/kg) | 2.73 | 0.11 | 0.37 | 4.12 | 0.07 | 0.45 | 4.07 | 0.06 | 0.47 |
| 120°/s ECC (N-m/kg) | 0.34 | 0.71 | 0.07 | 4.72 | 0.06 | 0.32 | 3.22 | 0.09 | 0.41 |
| Group A | Group B | |||||
|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | |
| Composite of star excursion balance test | 2.52 | −8.29–13.34 | 0.58 | −2.92 | −6.68–0.84 | 0.10 |
| Active repositioning | ||||||
| 15° of ankle inversion | −0.05 | −0.19–−0.09 | 0.03 | 0.01 | −0.08–0.12 | 0.71 |
| 0° in ankle neutral position | 0.30 | 0.04–0.56 | 0.02 | −0.02 | −0.13–−0.001 | 0.04 |
| 10° of ankle eversion | −0.05 | −0.25–0.15 | 0.55 | 0.02 | −0.04–0.10 | 0.38 |
| Passive repositioning | ||||||
| 15° of ankle inversion | −0.15 | −0.32–0.01 | 0.05 | −0.02 | −0.09–0.03 | 0.34 |
| 0° in ankle neutral position | −0.02 | −0.15–0.11 | 0.69 | 0.02 | −0.03–0.07 | 0.36 |
| 10° of ankle eversion | 0.05 | −0.09–0.21 | 0.41 | −0.009 | −0.07–0.05 | 0.73 |
| Ankle inversion | ||||||
| 30°/s COM (N-m/kg) | −0.07 | −0.15–−0.01 | 0.04 | −0.01 | −0.03–0.008 | 0.17 |
| 30°/s ECC (N-m/kg) | 0.04 | −0.14–0.23 | 0.56 | −0.005 | −0.05–0.04 | 0.80 |
| 120°/s COM (N-m/kg) | −0.03 | −0.11–0.04 | 0.31 | −0.006 | −0.03–0.02 | 0.64 |
| 120°/s ECC (N-m/kg) | 0.03 | −0.09–0.16 | 0.53 | 0.002 | −0.02–0.03 | 0.88 |
| Ankle eversion | ||||||
| 30°/s COM (N-m/kg) | −0.02 | −0.09–0.04 | 0.36 | −0.02 | −0.04–0.005 | 0.09 |
| 30°/s ECC (N-m/kg) | 0.02 | −0.07–0.12 | 0.60 | −0.01 | −0.04–0.02 | 0.48 |
| 120°/s COM (N-m/kg) | 0.06 | −0.06–0.18 | 0.26 | −0.005 | −0.03–0.02 | 0.69 |
| 120°/s ECC (N-m/kg) | −0.07 | −0.25–0.10 | 0.34 | −0.01 | −0.04–0.008 | 0.13 |
| Group A | Group B | Group C | ||||
|---|---|---|---|---|---|---|
| Pre- | Post- | Pre- | Post- | Pre- | Post- | |
| Anterior | 80.63 ± 9.78 | 88.27 ± 10.83 | 76.16 ± 7.56 | 91.30 ± 4.94 + | 78.31 ± 12.40 | 81.45 ± 6.48 |
| Anterolateral | 72.35 ± 8.26 | 79.61 ± 15.14 | 71.74 ± 7.73 | 82.71 ± 8.54 + | 75.65 ± 5.36 | 72.93 ± 2.88 |
| Anteromedial | 87.01 ± 15.30 | 93.69 ± 9.58 * | 85.18 ± 6.14 | 98.25 ± 7.07 + | 87.99 ± 11.85 | 80.63 ± 11.20 |
| Posteromedial | 81.27 ± 13.50 | 91.08 ± 13.51 | 85.59 ± 10.64 | 98.59 ± 11.04 + | 85.20 ± 9.91 | 84.71 ± 11.86 |
| Posterior | 71.62 ± 13.16 | 85.42 ± 16.69 | 70.49 ± 13.95 | 97.33 ± 12.54 + | 73.53 ± 10.34 | 79.50 ± 7.21 |
| Posterolateral | 68.10 ± 10.76 | 80.14 ± 12.39 * | 63.37 ± 13.12 | 91.65 ± 13.01 + | 68.17 ± 13.02 | 69.68 ± 6.47 |
| Medial | 87.27 ± 16.96 | 93.62 ± 8.91 | 84.64 ± 6.90 | 97.73 ± 4.82 + | 86.84 ± 8.54 | 91.15 ± 5.10 |
| Lateral | 64.73 ± 13.36 | 70.33 ± 13.39 * | 65.85 ± 13.26 | 85.58 ± 16.49 + | 67.41 ± 8.20 | 59.69 ± 3.06 |
| Composite | 76.62 ± 9.80 | 85.27 ± 11.76 | 75.38 ± 5.83 | 92.89 ± 7.80 + | 77.89 ± 4.60 | 77.47 ± 5.07 |
| Group A | Group B | Group C | ||||
|---|---|---|---|---|---|---|
| Pre- | Post- | Pre- | Post- | Pre- | Post- | |
| Active repositioning | ||||||
| 15° of ankle inversion | 7.78 ± 5.60 | 4.67 ± 2.49 * | 7.32 ± 3.67 | 5.14 ± 1.84 + | 8.33 ± 1.40 | 6.73 ± 1.66 |
| 0° in ankle neutral position | 6.94 ± 3.83 | 4.55 ± 2.87 * | 9.52 ± 2.71 | 6.55 ± 1.40 + | 9.06 ± 2.94 | 9.25 ± 1.02 |
| 10° of ankle eversion | 7.22 ± 4.94 | 4.35 ± 2.24 * | 7.65 ± 3.31 | 4.55 ± 2.16 + | 7.00 ± 4.10 | 6.84 ± 2.92 |
| Passive repositioning | ||||||
| 15° of ankle inversion | 6.17 ± 4.72 | 5.55 ± 3.45 | 6.45 ± 3.56 | 4.23 ± 1.07 | 7.67 ± 4.43 | 4.79 ± 2.51 |
| 0° in ankle neutral position | 6.78 ± 3.32 | 5.21 ± 3.47 | 5.40 ± 3.03 | 5.16 ± 3.86 | 5.86 ± 4.31 | 5.16 ± 3.12 |
| 10° of ankle eversion | 6.41 ± 3.42 | 4.50 ± 2.74 | 6.75 ± 2.69 | 6.25 ± 3.62 | 6.45 ± 4.36 | 6.70 ± 3.78 |
| Group A | Group B | Group C | ||||
|---|---|---|---|---|---|---|
| Pre- | Post- | Pre- | Post- | Pre- | Post- | |
| Ankle inversion | ||||||
| 30°/s COM (N-m/kg) | 28.47 ± 9.79 | 32.27 ± 9.25 * | 27.52 ± 9.26 | 29.91 ± 6.80 + | 26.89 ± 11.14 | 21.90 ± 7.35 |
| 30°/s ECC (N-m/kg) | 30.23 ± 6.53 | 33.15 ± 9.75 * | 29.73 ± 5.61 | 32.45 ± 6.17 + | 23.06 ± 9.06 | 23.31 ± 7.13 |
| 120°/s COM (N-m/kg) | 26.81 ± 7.14 | 32.00 ± 10.89 | 23.11 ± 11.33 | 26.44 ± 7.35 | 24.45 ± 12.83 | 24.35 ± 10.40 |
| 120°/s ECC (N-m/kg) | 29.61 ± 11.18 | 31.75 ± 9.42 | 26.05 ± 8.83 | 23.96 ± 8.17 | 26.63 ± 11.22 | 27.27 ± 10.77 |
| Ankle eversion | ||||||
| 30°/s COM (N-m/kg) | 22.87 ± 5.36 | 26.74 ± 6.79 | 20.40 ± 8.85 | 21.39 ± 8.61 | 20.12 ± 4.00 | 21.61 ± 8.83 |
| 30°/s ECC (N-m/kg) | 28.18 ± 6.09 | 30.83 ± 7.15 | 28.20 ± 8.24 | 29.73 ± 7.24 | 28.59 ± 7.99 | 27.74 ± 8.80 |
| 120°/s COM (N-m/kg) | 24.84 ± 8.86 | 29.22 ± 8.18 | 21.00 ± 12.16 | 32.08 ± 3.48 | 21.08 ± 4.30 | 22.39 ± 4.91 |
| 120°/s ECC (N-m/kg) | 29.65 ± 7.10 | 32.90 ± 8.28 | 26.72 ± 10.23 | 35.64 ± 5.74 | 29.87 ± 8.91 | 28.35 ± 7.10 |
| Angular velocity (30°/s) | ||||||
| COMeverton/COMinverton | 0.85 ± 0.25 | 0.90 ± 0.36 | 0.76 ± 0.23 | 0.81 ± 0.45 | 0.84 ± 0.31 | 0.90 ± 0.43 |
| ECCeverton/ECCinverton | 0.97 ± 0.29 | 1.02 ± 0.43 | 0.96 ± 0.25 | 0.98 ± 0.35 | 0.95 ± 0.32 | 0.98 ± 0.48 |
| ECCeverton/COMinverton | 1.05 ± 0.30 | 1.07 ± 0.46 | 1.21 ± 0.47 | 1.06 ± 0.44 | 1.09 ± 0.64 | 1.23 ± 0.52 |
| Angular velocity (120°/s) | ||||||
| COMeverton/COMinverton | 1.05 ± 0.46 | 1.05 ± 0.52 | 1.08 ± 0.49 | 1.01 ± 0.34 | 1.27 ± 0.29 | 1.04 ± 0.38 |
| ECCeverton/ECCinverton | 1.20 ± 0.72 | 1.13 ± 0.51 | 1.14 ± 0.55 | 1.21 ± 0.46 | 1.16 ± 0.33 | 1.11 ± 0.46 |
| ECCevertor/COMinvertor | 1.18 ± 0.43 | 1.15 ± 0.49 | 1.31 ± 0.67 | 1.22 ± 0.38 | 1.25 ± 0.39 | 1.20 ± 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, W.-D.; Chen, S.; Tsou, Y.-A. Effects of Whole-Body Vibration and Balance Training on Female Athletes with Chronic Ankle Instability. J. Clin. Med. 2021, 10, 2380. https://doi.org/10.3390/jcm10112380
Chang W-D, Chen S, Tsou Y-A. Effects of Whole-Body Vibration and Balance Training on Female Athletes with Chronic Ankle Instability. Journal of Clinical Medicine. 2021; 10(11):2380. https://doi.org/10.3390/jcm10112380
Chicago/Turabian StyleChang, Wen-Dien, Shuya Chen, and Yung-An Tsou. 2021. "Effects of Whole-Body Vibration and Balance Training on Female Athletes with Chronic Ankle Instability" Journal of Clinical Medicine 10, no. 11: 2380. https://doi.org/10.3390/jcm10112380