

Expanded Polytetrafluoroethylene Membranes for Vascular Stent Coating: Manufacturing, Biomedical and Surgical Applications, Innovations and Case Reports

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. e-PTFE Membrane Preparation
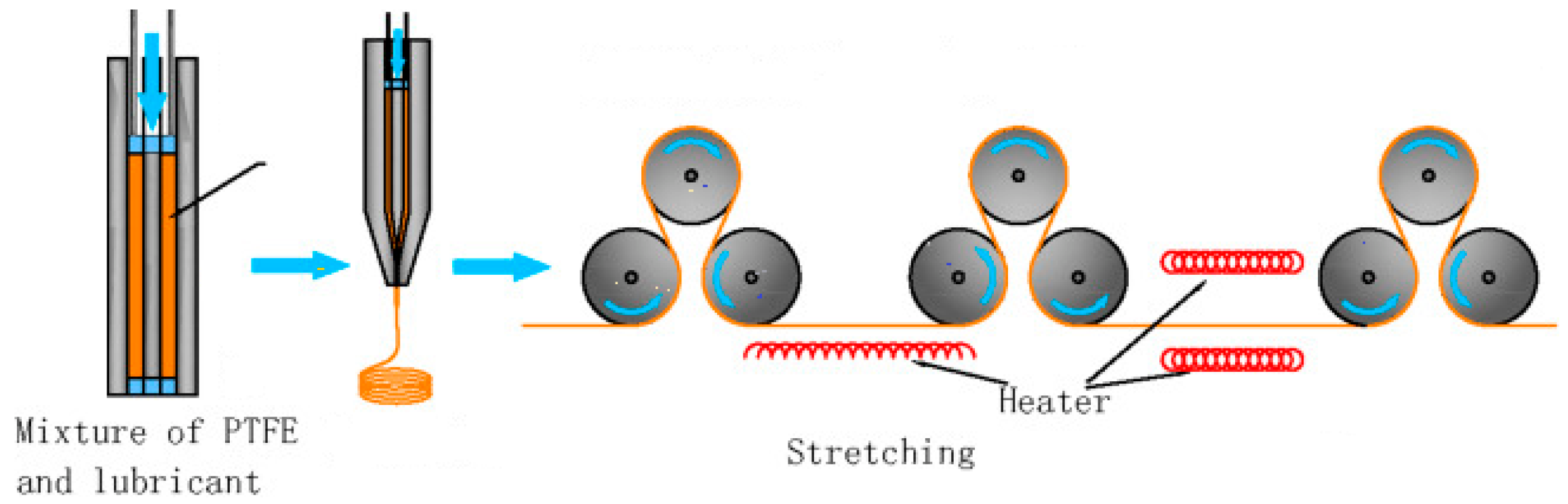
2.1. Stretching and Pore-Forming Process
2.2. Sintering Process
2.3. Wrapping Process
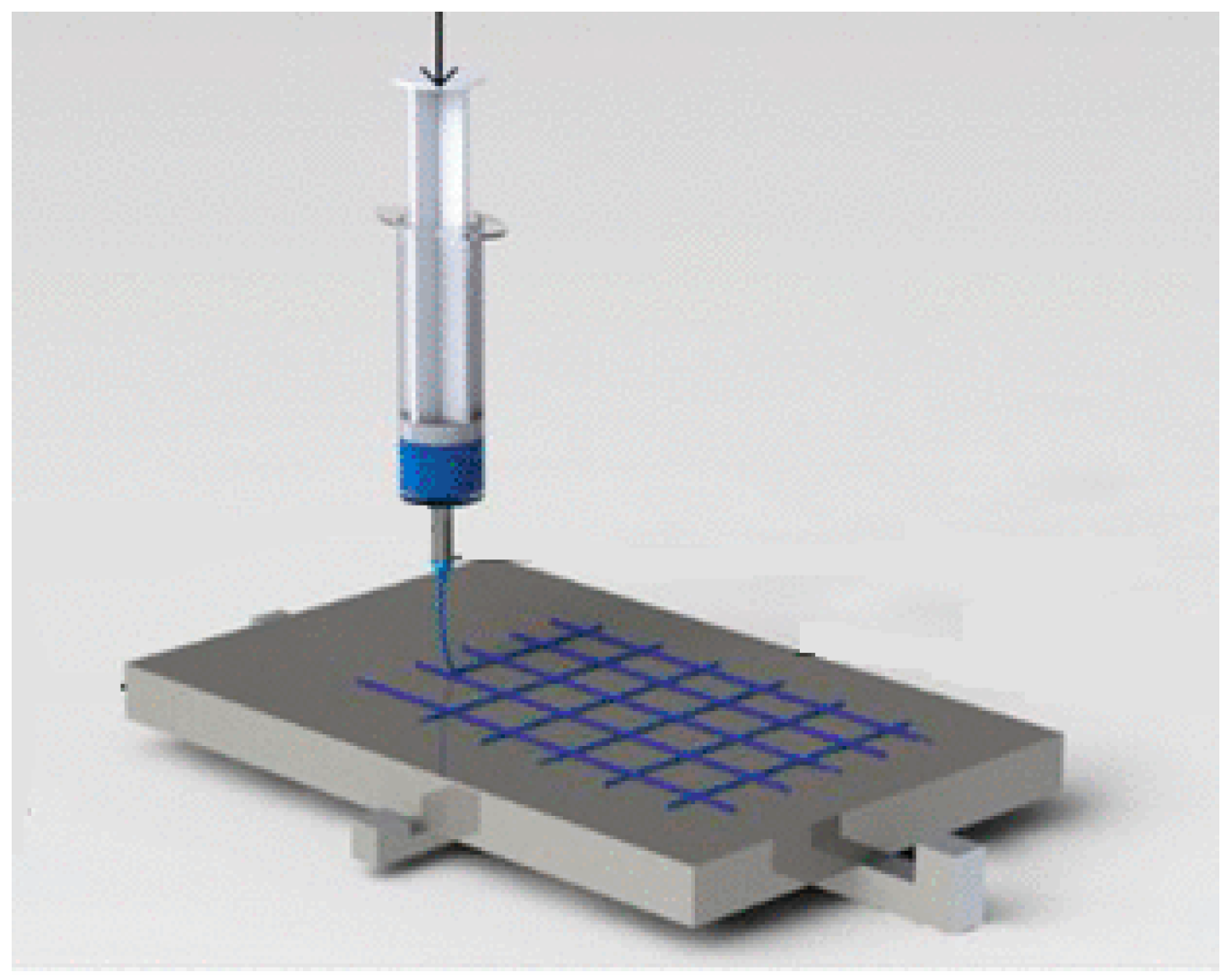
2.4. Near-Field Electrospinning Process
2.5. Electrospinning Process
3. e-PTFE Membrane Used in the Design of Covered Stents
4. The Advantages and Disadvantages of e-PTFE Membranes as Stent Coatings
5. Clinical Applications of Covered Stents
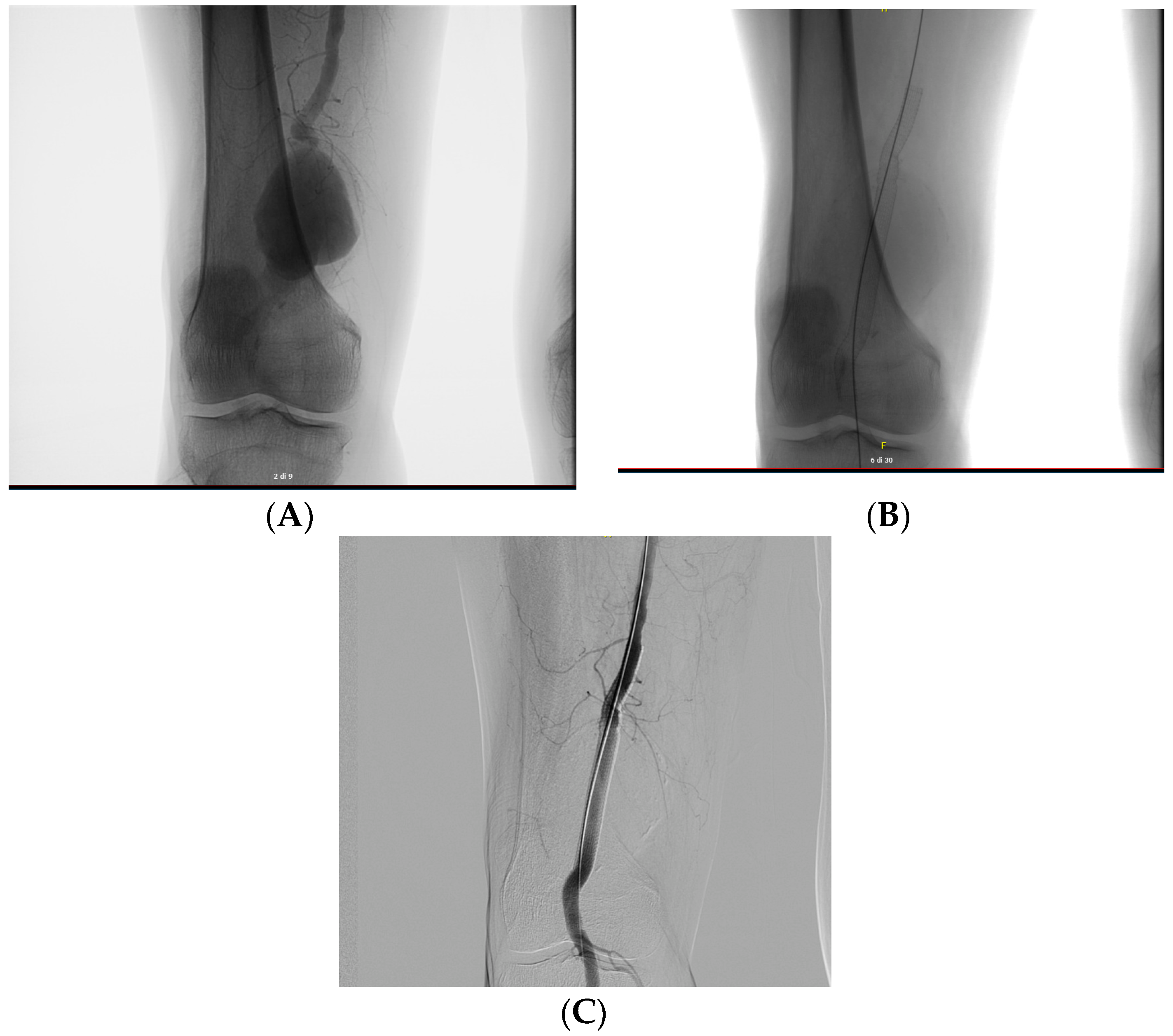
5.1. Popliteal Aneurysms
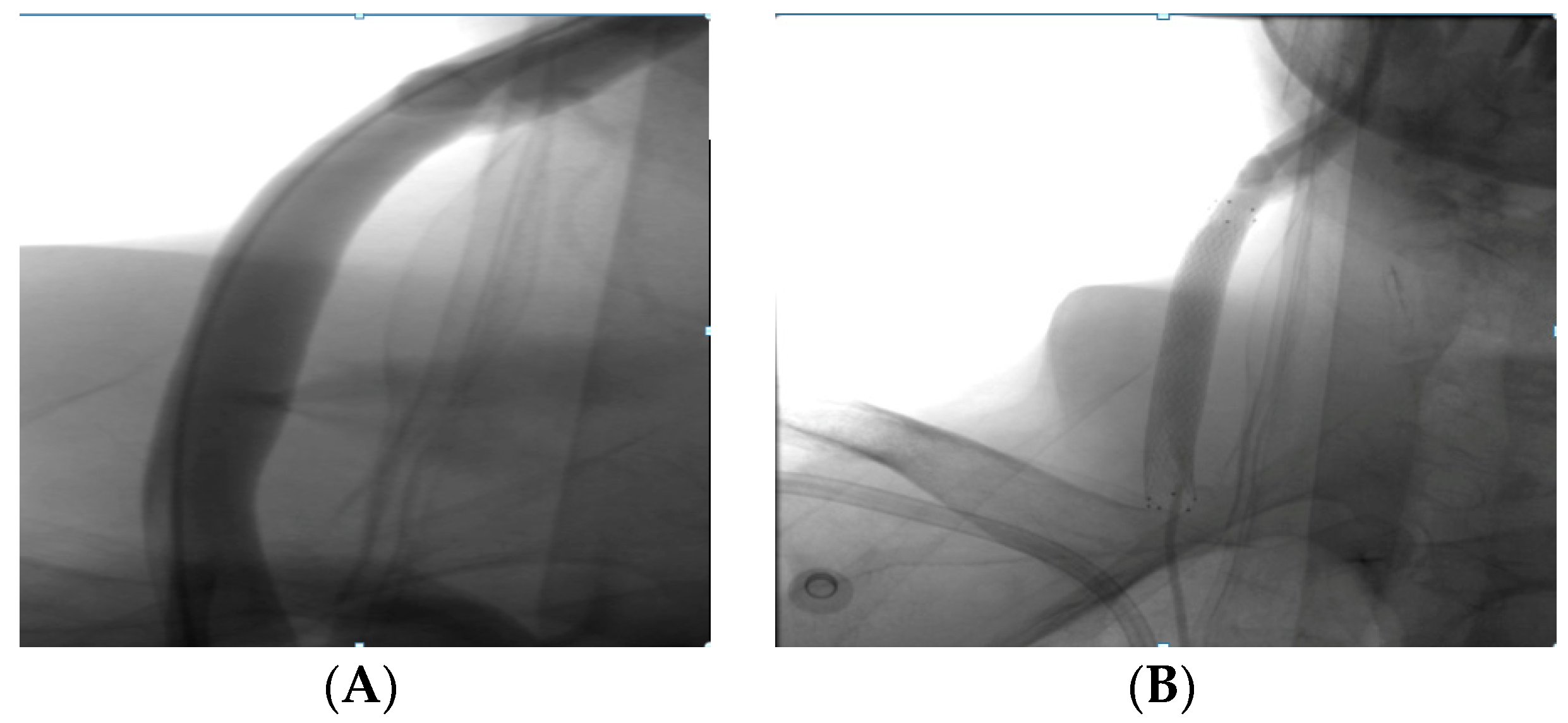
5.2. Covered Stent in Iatrogenic Perforations
5.3. Use of Covered Stent in e-PTFE in Leriche Syndrome Treatment
6. New Generation Stent Graft
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Case Report: Popliteal Aneurysm

Appendix A.2. Case Report: Bilateral Popliteal Aneurysm
Appendix A.3. Case Report: Iatrogen Perforation

Appendix A.4. Case Report: Leriche Syndrome

References
- Roina, Y.; Auber, F.; Hocquet, D.; Herlem, G. ePTFE functionalization for medical applications. Mater. Today Chem. 2021, 20, 100412. [Google Scholar] [CrossRef]
- Aronson, J.K. (Ed.) Polytetrafluoroethylene. In Meyler’s Side Effects of Drugs, 16th ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 872–873. [Google Scholar]
- Huang, H.; Yao, Q.; Zhang, X.; Wang, H. Microporous expanded polytetrafluoroethylene layer functionalized hydrophilic groups for excellent mechanical durability and superior performance in proton exchange membrane fuel cell. J. Power Sources 2022, 526, 231130. [Google Scholar] [CrossRef]
- Weaver, J.D.; Ku, D.N. A study on the effects of covered stents on tissue prolapse. J. Biomech. Eng. 2012, 134, 024505. [Google Scholar] [CrossRef] [PubMed]
- Farhatnia, Y.; Tan, A.; Motiwala, A.; Cousins, B.G.; Seifalian, A.M. Evolution of covered stents in the contemporary era: Clinical application, materials and manufacturing strategies using nanotechnology. Biotechnol. Adv. 2013, 31, 524. [Google Scholar] [CrossRef]
- Soldatos, N.K.; Stylianou, P.; Angelov, N.; Koidou, P.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017, 48, 131. [Google Scholar]
- Alauddin, M.S.; Ayman, N.; Hayei, A.; Sabarudin, M.A.; Haliza, N.; Baharin, M. Barrier Membrane in Regenerative Therapy: A Narrative Review. Membranes 2022, 12, 444. [Google Scholar] [CrossRef]
- Shiohara, A.; Prieto-Simon, B.; Voelcker, N.H. Porous polymeric membranes: Fabrication techniques and biomedical applications. J. Mater. Chem. B 2021, 9, 2129–2154. [Google Scholar] [CrossRef]
- Jain, R.; Shetty, S.; Yadav, K.S. Unfolding the electrospinning potential of biopolymers for preparation of nanofibers. J. Drug Deliv. Sci. Technol. 2020, 57, 101604. [Google Scholar] [CrossRef]
- Sun, M.; Han, K.; Hu, R.; Liu, D.; Fu, W.; Liu, W. Advances in micro/nanoporous membranes for biomedical engineering. Adv. Healthc. Mater. 2021, 10, 2001545. [Google Scholar] [CrossRef]
- Bottino, A.; Capannelli, G.; Comite, A.; Costaetal, C. Novel polytetrafluoroethylene tubular membranes for membrane distillation. Distill. Water Treat. 2015, 53, 6. [Google Scholar] [CrossRef]
- Guney, A.; Kara, F.; Ozgen, O.; Aksoy, E.A.; Hasirci, V.; Hasirci, N. Surface modification of polymeric biomaterials. Biomater. Surface Sci. 2013, 4, 89–158. [Google Scholar]
- Weinbaum, J.S.; Haskett, D.G.; Mandelkern, T.F.; Vorp, D.A. Advances in cell seeding of tissue engineered vascular grafts. In Tissue-Engineered Vascular Grafts; Walpoth, B., Bergmeister, H., Bowlin, G., Kong, D., Rotmans, J., Zilla, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; pp. 295–319. [Google Scholar]
- Zhang, L.L.; Ham, S.W.; Weaver, F.A.; Rowe, V.L.; Ziegler, K.R.; Magee, G.A.; Sukgu, M. Performance of Gore Viabahn VBX Compared with Atrium iCast as Bridging Stents During Fenestrated Endovascular Aortic Repairs. J. Vasc. Surg. 2019, 69, e215–e216. [Google Scholar] [CrossRef] [Green Version]
- Patel, N.J.; Agasthi, P.; Mhatre, A.U.; Heuser, R.R. Out of the Mind of Edward B. Diethrich: The Development of the PolytetrafluoroethyleneCovered Coronary Stent. J. Endovasc. Ther. 2020, 27, 157–159. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Qiu, C.; Li, D.; Zhang, H. Treatment of posttraumatic infrapopliteal pseudoaneurysm with a physician modified covered stent. Vasc. Investig. Ther. 2021, 4, 95. [Google Scholar]
- Patel, D.V. The Value of the GORE® VIABAHN® Endoprosthesis. Supplement to endovascular. 2019. [Google Scholar]
- Tenorio, E.R.; Oderich, G.S.; Kölbel, T.; Dias, N.V.; Sonesson, B.; Karelis, A.; A Farber, M.; Parodi, F.E.; Timaran, C.H.; Scott, C.K.; et al. Multicenter global early feasibility study to evaluate total endovascular arch repair using three-vessel inner branch stent-grafts for aneurysms and dissections. J. Vasc. Surg. 2021, 74, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, P.; Mahmoody, K.; Erne, P. Covered stents: A Review. Int. J. Cardiol. 2008, 130, 28. [Google Scholar] [CrossRef]
- Fenga, S.; Zhonga, Z.; Wanga, Y.; Xinga, W.; Drioli, E. Progress and perspectives in PTFE membrane: Preparation, modification, and applications. J. Membr. Sci. 2018, 549, 332–349. [Google Scholar] [CrossRef]
- Tan, X.M.; Rodrigue, D. A Review on Porous Polymeric Membrane Preparation. Part II: Production Techniques with Polyethylene, Polydimethylsiloxane, Polypropylene, Polyimide, and Polytetrafluoroethylene. Polymers 2019, 11, 1310. [Google Scholar] [CrossRef] [Green Version]
- Otto, C.; Handge, U.A.; Georgopanos, P.; Aschenbrenner, O.; Kerwitz, J.; Abetz, C.; Metze, A.L.; Abetz, V. Porous UHMWPE membranes and composites filled with carbon nanotubes: Permeability, mechanical, and electrical properties. Macromol. Mater. Eng. 2017, 302, 1600405. [Google Scholar] [CrossRef]
- Remanan, S.; Sharma, M.; Bose, S.; Das, N.C. Recent advances in preparation of porous polymeric membranes by unique techniques and mitigation of fouling through surface modification. ChemistrySelect 2018, 609–633. [Google Scholar] [CrossRef]
- Van Rooyen, L.J.; Bissett, H.; Khoathane, M.C.; Karger-Kocsis, J. Preparation of PTFE/graphene nanocomposites by compression moulding and free sintering: A guideline. J. Appl. Polym. Sci. 2016, 133, 43369. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-Y.; Ge, Q.; Yang, L.-L.; Shi, X.-J.; Li, J.-J.; Yang, D.-Q.; Sacher, E. Durable superhydrophobic PTFE films through the introduction of micro-and nanostructured pores. Appl. Surf. Sci. 2015, 339, 151–157. [Google Scholar] [CrossRef]
- Li, K.; Zhang, Y.; Xu, L.; Zeng, F.; Hou, D.; Wang, J. Optimizing stretching conditions in fabrication of PTFE hollow fber membrane for performance improvement in membrane distillation. J. Membr. Sci. 2018, 550, 126–135. [Google Scholar] [CrossRef]
- Wang, F.; Li, J.; Zhu, H.; Zhang, H.; Tang, H.; Chen, J.; Guo, Y. Effect of the highly asymmetric structure on the membrane characteristics and microfiltration performance of PTFE wrapped hollow fiber membrane. J. Water Proc. Eng. 2015, 7, 36–45. [Google Scholar] [CrossRef]
- He, X.-X.; Zheng, J.; Yu, G.-F.; You, M.-H.; Yu, M.; Ning, X.; Long, Y.-Z. Near-feld electrospinning: Progress and applications. J. Phys. Chem. C 2017, 121, 8663–8678. [Google Scholar] [CrossRef]
- Nazemi, M.M.; Khodabandeh, A.; Hadjizadeh, A. Near-Field Electrospinning: Crucial Parameters, Challenges, and Applications. ACS Appl. Bio Mater. 2022, 5, 394. [Google Scholar] [CrossRef]
- King, W.E.; Bowlin, G.L. Near-Field Electrospinning and Melt Electrowriting of Biomedical Polymers—Progress and Limitations. Polymers 2021, 13, 1097. [Google Scholar] [CrossRef]
- Kang, W.; Li, F.; Zhao, Y.; Qiao, C.; Ju, J.; Cheng, B. Fabrication of porous Fe2O3/PTFE nanofiber membranes and their application as a catalyst for dye degradation. RSC Adv. 2016, 6, 32646. [Google Scholar] [CrossRef]
- Dong, Z.-Q.; Ma, X.-h.; Xu, Z.-L.; You, W.-T.; Li, F. Superhydrophobic PVDF–PTFE electrospun nanofibrous membranes for desalination by vacuum membrane distillation. Desalination 2014, 347, 175. [Google Scholar] [CrossRef]
- Feng, Y.; Xiong, T.; Jiang, S.; Liu, S.; Hou, H. Mechanical properties and chemical resistance of electrospunpolyterafluoroethylenefibres. RSC Adv. 2016, 6, 24250. [Google Scholar] [CrossRef]
- Liu, G.; Gao, C.; Li, X.; Guo, C.; Chen, Y.; Lv, J. Preparation and properties of porous polytetrafluoroethylenehollow fiber membrane through mechanical operations. J. Appl. Polym. Sci. 2015, 132, 1. [Google Scholar] [CrossRef]
- Ghorbani, M.; Griessenauer, C.J.; Shojaei, H.; Wipplinger, C.; Hejazian, E. Endovascular reconstruction of iatrogenic internal carotid artery injury following endonasal surgery: A systematic review. Neurosurg. Rev. 2020, 44, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- McKavanagh, P.; Zawadowski, G.; Ahmed, N.; Kutryk, M. Expert Review of Cardiovascular The evolution of coronary stents. Therapy 2018, 16, 219–228. [Google Scholar]
- Stefanini, G.; Byrne, R.A.; Windecker, S.; Kastrati, A. State of the art: Coronary artery stents—Past, present and future. EuroIntervention 2017, 13, 706. [Google Scholar] [CrossRef]
- Sakamoto, A.; Torii, S.; Jinnouchi, H.; Virmani, R.; Finn, A.V. Histopathologic and physiologic effect of overlapping vs single coronary stents: Impact of stent evolution. Expert Rev. Med. Devices 2018, 9, 1–18. [Google Scholar] [CrossRef]
- Weekes, A.; Bartnikowski, N.; Pinto, N.; Jenkins, J.; Meinert, C.; Klein, T.J. Biofabrication of small diameter tissue-engineered vascular grafts. Acta Biomater. 2022, 138, 92–111. [Google Scholar] [CrossRef]
- Uthamaraj, S.; Tefft, B.J.; Jana, S.; Hlinomaz, O.; Kalra, M.; Lerman, A.; Dragomir-Daescu, D.; Sandhu, G.S.J. Fabrication of small caliber stent-grafts using electrospinning and balloon expandable bare metal stents. Vis. Exp. 2016, 116, e54731. [Google Scholar]
- Dalton, P.D.; Vaquette, C.; Farrugia, B.L.; Dargaville, T.R.; Brown, T.D.; Hutmacher, D.W. Electrospinning and additive manufacturing: Converging technologies. Biomater. Sci. 2013, 1, 171. [Google Scholar] [CrossRef]
- Cronenwett, J.L.; Johnston, K.W. Rutherford’s Vascular Surgery; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Li, C.; Guo, C.; Fitzpatrick, V.; Ibrahim, A.; Zwierstra, M.J.; Hanna, P.; Lechtig, A.; Nazarian, A.; Lin, S.J.; Kaplan, D.L. Design of biodegradable, implantable devices towards clinical translation. Nat. Rev. Mater. 2020, 5, 61. [Google Scholar] [CrossRef]
- Gao, F.; Hu, Y.; Li, G.; Liu, S.; Quan, L.; Yang, Z.; Wei, Y.; Pan, C. Layer-by-layer deposition of bioactive layers on magnesium alloy stent materials to improve corrosion resistance and biocompatibility. Bioact. Mater. 2020, 5, 611. [Google Scholar] [CrossRef]
- Labarrere, C.A.; Dabiri, A.E. Thrombogenic and Inflammatory Reactions to Biomaterials in Medical Devices. Front. Bioeng. Biotechnol. 2020, 8, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.S.; Kayumov, M.; Emechebe, G.A.; Kim, D.W.; Cho, H.J.; Jeong, Y.J.; Lee, D.W.; Park, J.K.; Park, C.H.; Kim, C.S.; et al. A Comparative Study of an Anti-Thrombotic Small-Diameter Vascular Graft with Commercially Available e-PTFE Graft in a Porcine Carotid Model. Tissue Eng. Regen. Med. 2022, 19, 537–551. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.; Chakraborty, R.; Banik, O.; Banoth, E.; Kumar, P. Surface Engineering of a Bioartificial Membrane for Its Application in Bioengineering Devices. ACS Omega 2023, 8, 3606–3629. [Google Scholar] [CrossRef]
- Sun, W.; Liu, W.; Wu, Z.; Chen, H. Chemical surface modification of polymeric biomaterials for biomedical applications. Macromol. Rapid Commun. 2020, 41, 1900430. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Mandal, B.B. Tissue-engineered vascular grafts: Emerging trends and technologies. Adv. Funct. Mater. 2021. [Google Scholar] [CrossRef]
- Jin, Y.J.; Kang, S.; Park, P.; Choi, D.; Kim, D.W.; Jung, D.; Koh, J.; Jeon, J.; Lee, M.; Ham, J.; et al. Anti-inflammatory and antibacterial effects of covalently attached biomembrane-mimic polymer grafts on gore-teximplants. ACS Appl. Mater. Interfaces 2017, 9, 5–30. [Google Scholar] [CrossRef]
- Lopez-Saucedo, F.; Flores-Rojas, G.; Magarinos, B.; Concheiro, A.; Alvarez, C.; Bucio, E. Radiation grafting of poly (methyl methacrylate) and poly(vinylimidazole) onto polytetrafluoroethylene films and silver immobilization for antimicrobial performance. Appl. Surf. Sci. 2019, 473, 951–959. [Google Scholar] [CrossRef]
- Al Meslmani, B.; Mahmoud, G.; Bakowsky, U. Development of expanded polytetrafluoroethylene cardiovascular graft platform based on immobilization of poly lactic-co-glycolic acid nanoparticles using a wet chemical modification technique. Int. J. Pharm. 2017, 529, 238–244. [Google Scholar] [CrossRef]
- Herten, M.; Idelevich, E.A.; Sielker, S.; Becker, K.; Scherzinger, A.S.; Osada, N.; Torsello, G.B.; Bisdas, T. Vascular graft impregnation with antibiotics: The influence of high concentrations of rifampin, vancomycin, daptomycin, and bacteriophage endolysin HY-133 on viability of vascular cells. Med. Sci. Monit. Basic Res. 2017, 23, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Geelhoed, W.; van der Bogt, K.; Rothuizen, T.; Damanik, F.; Hamming, J.; Mota, C.; van Agen, M.; de Boer, H.; Restrepo, M.T.; Hinz, B.; et al. A novel method for engineering autologous nonthrombogenic in situ tissue-engineered blood vessels for arteriovenous grafting. Biomaterials 2020, 229, 119577. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Liu, C.; Feng, F.; Wang, D.; Mo, H.; Si, L.; Wei, G.; Shen, J. Polyurethane/polyurethane nanoparticle-modified expanded poly(tetrafluoroethylene) vascular patches promote endothelialization. J. Biomed. Mater. Res. A 2018, 106, 2131–2140. [Google Scholar] [CrossRef] [PubMed]
- Táborská, J.; Riedelová, Z.; Brynda, E.; Májek, P.; Riedel, T. Endothelialization of an ePTFE vessel prosthesis modified with an antithrombogenic fibrin/heparin coating enriched with bound growth factors. RSC Adv. 2021, 11, 5903–5913. [Google Scholar]
- Tzchori, I.; Falah, M.; Shteynberg, D.; Ashkenazi, D.L.; Loberman, Z.; Perry, L.; Flugelman, M.Y. Improved patency of ePTFE grafts as a hemodialysis access site by seeding autologous endothelial cells expressing fibulin-5 and VEGF. Mol. Ther. 2018, 26, 1660–1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, B.; Ishihara, K. Formation of stable polydopamine layer on polytetrafluoroethylene substrate by hybrid process involved plasma treatment and spontaneous chemical reactions. Mater. Today Commun. 2020, 22, 100774. [Google Scholar] [CrossRef]
- Wulff, B.; Stahlhoff, S.; Vonthein, R.; Schmidt, A.; Sigler, M.; Torsello, G.B.; Herten, M. Biomimetic heparan sulfate-like coated ePTFE grafts reduce in-graft neointimal hyperplasia in ovine carotids. Ann. Vasc. Surg. 2017, 40, 274–284. [Google Scholar] [CrossRef] [Green Version]
- Aoki, J.; Tanabe, K. Mechanisms of drug eluting stent restenosis. Cardiovasc. Interv. Ther. 2021, 36, 23–29. [Google Scholar] [CrossRef]
- Gouëffic, Y.; Sauguet, A.; Desgranges, P.; Feugier, P.; Rosset, E.; Ducasse, E.; Kaladji, A.; Salomon du Mont, L.; Pernès, J.M.; Commeau, P.; et al. A Polymer-Free Paclitaxel-Eluting Stent Versus a Bare-Metal Stent for De Novo Femoropopliteal Lesions: The BATTLE Trial. J. Am. Coll. Cardiol. Intv. 2020, 447–457. [Google Scholar] [CrossRef]
- Kuramitsu, S. Drug-eluting stent thrombosis: Current and future perspectives. Cardiovasc. Interv. Ther. 2021, 36, 158–168. [Google Scholar] [CrossRef]
- Gohbara, M.; Sugano, T.; Ishikawa, T.; Tamura, K.; Kimura, K. A case of a coronary covered stent for repeated restenosis at the anastomosis site between saphenous vein graft and graft prosthesis. J. Cardiol. Cases 2021, 25, 110–114. [Google Scholar] [CrossRef]
- Wang, Y.; Li, G.; Yang, L.; Luo, R.; Guo, G. Development of Innovative Biomaterials and Devices for the Treatment of Cardiovascular Disease. Adv. Mater. 2022, 34, 2201971. [Google Scholar] [CrossRef]
- Radu, E.R.; Voicu, S.I.; Thakur, V.K. Polymeric Membranes for Biomedical Applications. Polymers 2023, 15, 619. [Google Scholar] [CrossRef] [PubMed]
- Smelt, H.; Cheng, W.; Tyler, S.; Virmani, R.J. TCT-125 Ultrahigh Molecular Weight Polyethylene Membrane for Use in Vascular Stent Graft Applications—Preliminary Evidence from an Ovine Peripheral Implantation Model. Am. Coll. Cardiol. 2017, 70, B56. [Google Scholar] [CrossRef]
- Farber, A.; Angle, N.; Avgerinos, E.; Dubois, L.; Eslami, M.; Geragh, P.; Haurani, M.; Jim, J.; Ketteler, E.; Pulli, R.; et al. The Society for Vascular Surgery clinical practice guidelines on popliteal artery aneurysms. J. Vasc. Surg. 2022, 75, 109S–120S. [Google Scholar] [CrossRef] [PubMed]
- Beuschel, B.; Nayfeh, T.; Kunbaz, A.; Haddad, A.; Alzuab, M.; Vindhyal, S.; Farber, A.; Murad, H. A systematic review and meta-analysis of treatment and natural history of popliteal artery aneurysms. J. Vasc. Surg. 2022, 75, 121S–125S.e14. [Google Scholar] [CrossRef]
- Jergovic, I.; Cheesman, M.A.; Siika, A.; Khashram, M.; Paris, S.M.; Roy, J.; Hultgren, R. Natural history, growth rates, and treatment of popliteal artery aneurysms. J. Vasc. Surg. 2022, 75, 205–212. [Google Scholar] [CrossRef]
- Kim, T.I.; Sumpio, B.E. Management of Asymptomatic Popliteal Artery Aneurysms. Int. J. Angiol. 2019, 28, 5–10. [Google Scholar] [CrossRef]
- Prozorov, S.A. Endovascular Treatment of Patients with Popliteal Artery Aneurysms (a Literature Review) Russian Sklifosovsky. J. Emerg. Med. Care 2019, 8, 437–442. [Google Scholar]
- Hellwig, K.; Hoffmann, L.; Rother, U.; Meyer, A.; Lang, W.; Schmid, A. Eligibility of Endovascular Repair for Popliteal Artery Aneurysms According the Instructions for Use, Germany. Ann. Vasc. Surg. 2020, 67, 370–375. [Google Scholar] [CrossRef]
- Oga, Y.; Kubo, Y.; Kemmochi, R.; Ujihira, K.; Masuda, Z.; Matsumoto, M. Three cases implanted with VIABAHN for popliteal artery hemorrhage post-total knee arthroplasty. Ann. Vasc. Surg. Brief Rep. Innov. 2022, 2, 100098. [Google Scholar] [CrossRef]
- Edward, J.; Jenkins, E.J. Management of a large ruptured popliteal artery aneurysm involving combined deployment of a covered stent graft and evacuation of popliteal fossa hematoma. J. Vasc. Surg. Cases Innov. Tech. 2020, 6, 27–30. [Google Scholar]
- Jaber, C.; Moulahi, N.; BenMrad, I.; Bousnina, M.; Damak, A.; Azabou, N.; Zairi, M.; Jemel, A.; Kaoue, K. Endovascular management of a ruptured popliteal artery aneurysm in a patient with Behçet’s disease. Ann. Vasc. Surg. Brief Rep. Innov. 2022, 2, 100097. [Google Scholar] [CrossRef]
- de Donato, G.; Pasqui, E.; Galzerano, G.; Anzaldi, M.G.; Cappelli, A.; Palasciano, G. The Combination of Vacuum-Assisted Thromboaspiration and Covered Stent Graft for Acute Limb Ischemia due to Thromboembolic Complications of Popliteal Aneurysm. Ann. Vasc. Surg. 2022, 89, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.L. Managing Iatrogenic Injury and Arteriovenous Fistulae Covered or bare-metal stents may be useful options for treating perforation and arteriovenous fistulae complicating below-the-knee arterial interventions. Endovasc. Today 2008. [Google Scholar]
- Harms, J.C.; Rangarajan, S.; Young, C.J.; Barker-Finkel, J.; Allon, M. Outcomes of arteriovenous fistulas and grafts with or without intervention before successful use. J. Vasc. Surg. 2016, 64, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, R.; Israrahmed, A.; Yadav, R.; Singh, S.; Behra, M.; Khuswaha, R.; Prasad, N.; Lal, H. Endovascular embolization in problematic hemodialysis arteriovenous fistulas: A nonsurgical technique. Indian J. Nephrol. 2021, 31, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Nojima, T.; Motomiya, Y. Graft inclusion technique: A new flow reduction procedure for high flow arteriovenous fistulae. Ann. Vasc. Dis. 2018, 11, 202. [Google Scholar] [CrossRef] [Green Version]
- Dukkipati, R.; Benjo, A.M.; Jimenez, A.; Lukitsch, I.; Echefu, G.C.; Kumbala, D.R. Iatrogenic Fistula in Hemodialysis Patients: An Alternative Approach to Thrombectomy of Arteriovenous Graft (AVG) Thrombosis. Hindawi Case Rep. Vasc. Med. 2022, 2022, 1–6. [Google Scholar] [CrossRef]
- Cuong, L.T.; Bang, H.T.; Tan, N.D. Endovascular treatment for a femoral arteriovenous fistula after removal of a hemodialysis catheter. Int. J. Med. Health Res. 2019, 11, 1–6. [Google Scholar] [CrossRef]
- Healy, D.A.; Kimura, S.; Power, D.; Elhaj, A.; Abdeldaim, Y.; Cross, K.S. A systematic review and meta-analysis of thrombotic events following endovenous thermal ablation of the great saphenous vein. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 410–424. [Google Scholar] [CrossRef] [Green Version]
- Tohmasi, S.; Kabutey, N.; Chen, S.L.; Sheehan, B.; Duong, W.Q.; Kuo, I.J.; Fujitani, R.M.; Kopchok, G.E.; Donayre, C.E. Iatrogenic Arteriovenous Fistula Formation after Endovenous Laser Treatment Resulting in High-output Cardiac Failure: A Case Report and Review of the Literature. Ann. Vasc. Surg. 2021, 72, 666.e13–666.e21. [Google Scholar] [CrossRef]
- Wee, I.J.Y.; Yap, H.Y.; Tang, T.Y.; Chong, T.T. A systematic review, meta-analysis, and meta-regression of the efficacy and safety of endovascular arteriovenous fistula creation. J. Vasc. Surg. 2020, 71, 309–317. [Google Scholar]
- Branco, B.C.; Boutrous, M.L.; DuBose, J.J.; Leake, S.S.; Charlton-Ouw, K.; Rhee, P. Outcome comparison between open and endovascular management of axillosubclavian arterial injuries. J. Vasc Surg. 2016, 63, 702–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, R.K.; Shingu, Y.; Fusegawa, M.; Ishigaki, T.; Wakasa, S. Iatrogenic Arteriovenous Fistula of Subclavian Artery to Vertebral Vein with Perimedullary Vein Reflux. Ann. Vasc. Dis. 2022, 15, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Aljobeh, A.; Josephson, T.; Bortolotti, C.; Cloft, H.; Lanzino, G. Vertebral Arteriovenous Fistula: A Review Article. World Neurosurg. 2019, 122, e1388–e1397. [Google Scholar] [CrossRef]
- Brown, K.; Muco, G.L. Leriche Syndrome. In Study Guide from StatPearls Publishing, Treasure Island (FL); StatPearls: Orlando, FL, USA, 2019. [Google Scholar]
- Liang, H.L.; Li, M.F.; Hsiao, C.C.; Wu, C.J.; Wu, T.H. Endovascular management of aorto-iliac occlusive disease (Leriche syndrome). J. Formos. Med. Assoc. 2021, 120, 1485–1492. [Google Scholar] [CrossRef]
- Kretschmann, T.; Usai, M.V.; Taneva, G.T.; Pitoulias, G.A.; Torsello, G.; Donas, K.P. The role of open and endovascular treatment of patients with chronic, aortoiliac Leriche syndrome. Vascular 2020, 28, 68–73. [Google Scholar] [CrossRef]
- Mallory, A.; Giannopoulos, S.; Lee, P.; Kokkinidis, D.G.; Armstrong, E.J. Covered Stents for Endovascular Treatment of Aortoiliac Occlusive Disease: A Systematic Review and Meta-Analysis. Vasc. Endovasc. Surg. 2021, 55, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Fujihara, M.; Takahara, M.; Yamaoka, T.; Iida, O.; Kojima, T.; Tobita, K.; Nakama, T.; Kyuragi, R.; Ichihashi, S.; Soga, Y. Clinical outcomes of endovascular procedure using VIABAHN®, VBX covered stent in complex aortoiliac artery disease: Result from AVOCADO study. Catheter. Cardiovasc. Interv. 2021, 98, 928–937. [Google Scholar] [CrossRef]
- Giusca, S.; Schmidt, A.; Korosoglou, G. Pave-and-crack’ technique for the recanalization of severely calcified occlusive aorto-ilio-femoral disease in type-III Leriche syndrome: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab059. [Google Scholar] [CrossRef]
- Bracale, U.M.; Giribono, A.M.; Spinelli, D.; Del Guercio, L.; Pipitò, N.; Ferrara, D.; Barillà, D.; Barbarisi, D.; Derone, G.; Benedetto, F. Long-term Results of Endovascular Treatment of TASC C and D Aortoiliac Occlusive Disease with Expanded Polytetrafluoroethylene Stent Graft. Ann. Vasc. Surg. 2019, 56, 254–260. [Google Scholar] [CrossRef]
- El Samadoni, A.; Eldmarany, H.A.; El Aini, K. Primary Covered Stent for Management of infrarenal aortic and Aortoiliac Occlusive Disease. Pilot Study J. Surg. 2017, 18, 103. [Google Scholar]
- Vahabli, E.; Mann, J.; Heidari, B.S.; Lawrence-Brown, M.; Norman, P.; Jansen, S.; De-Juan-Pardo, E.; Doyle, B. The Technological Advancement to Engineer Next-Generation Stent-Grafts: Design, Material, and Fabrication Techniques. Adv. Healthc. Mater. 2022, 11, 2200271. [Google Scholar] [CrossRef] [PubMed]
- Levi, D.S.; Kusnezov, N.; Carman, G.P. Smart materials applications for pediatric cardiovascular devices. Pediatr. Res. 2008, 63, 552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budun, S.; ̧Sgören, E.I.; Erdem, R.; Yüksek, M. Morphological and mechanical analysis of electrospun shape memory polymer fibers. Appl. Surf. Sci. 2016, 380, 294. [Google Scholar] [CrossRef]
- Zhao, W.; Liu, L.; Zhang, F.; Leng, J.; Liu, Y. Shape memory polymers and their composites in biomedical applications. Mater. Sci. Eng. 2019, 97, 8. [Google Scholar] [CrossRef]
- Small, W.; Wilson, T.S.; Buckley, P.R.; Benett, W.J.; Loge, J.M.; Hartman, J.; Maitland, D.J. Prototype Fabrication and Preliminary in Vitro Testing of a Shape Memory Endovascular Thrombectomy Device. IEEE Trans. Biomed. Eng. 2007, 54, 1657. [Google Scholar] [CrossRef]
- Maitland, J.; Small, W.; Ortega, J.M.; Buckley, P.R.; Rodriguez, J.; Hartman, J.; Wilson, T.S. Prototype laser-activated shape memory polymer foam device for embolic treatment of aneurysms. J. Biomed. Opt. 2007, 12, 030504. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yu, R.; Guo, B. Shape-Memory and Self-Healing Polymers Based on Dynamic Covalent Bonds and Dynamic Noncovalent Interactions: Synthesis, Mechanism, and Application. ACS Appl. Bio Mater. 2021, 4, 5926. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Zhang, Q.; Yao, Y.; Liu, L.; Liu, Y.; Leng, J. Direct-write fabrication of 4D active shape-changing structures based on a shape memory polymer and its nanocomposite. ACS Appl. Mater. Interfaces 2017, 9, 876. [Google Scholar] [CrossRef]
- He, W.; Zhou, D.; Gu, H.; Qu, R.; Cui, C.; Zhou, Y.; Wang, Y.; Zhang, X.; Wang, Q.; Wang, T.; et al. A Biocompatible 4D Printing Shape Memory Polymer as Emerging Strategy for Fabrication of Deployable Medical Devices. Macromol. Rapid Commun. 2022, 44, 2200553. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassano, R.; Perri, P.; Esposito, A.; Intrieri, F.; Sole, R.; Curcio, F.; Trombino, S. Expanded Polytetrafluoroethylene Membranes for Vascular Stent Coating: Manufacturing, Biomedical and Surgical Applications, Innovations and Case Reports. Membranes 2023, 13, 240. https://doi.org/10.3390/membranes13020240
Cassano R, Perri P, Esposito A, Intrieri F, Sole R, Curcio F, Trombino S. Expanded Polytetrafluoroethylene Membranes for Vascular Stent Coating: Manufacturing, Biomedical and Surgical Applications, Innovations and Case Reports. Membranes. 2023; 13(2):240. https://doi.org/10.3390/membranes13020240
Chicago/Turabian StyleCassano, Roberta, Paolo Perri, Antonio Esposito, Francesco Intrieri, Roberta Sole, Federica Curcio, and Sonia Trombino. 2023. "Expanded Polytetrafluoroethylene Membranes for Vascular Stent Coating: Manufacturing, Biomedical and Surgical Applications, Innovations and Case Reports" Membranes 13, no. 2: 240. https://doi.org/10.3390/membranes13020240