

Allylamines, Benzylamines, and Fungal Cell Permeability: A Review of Mechanistic Effects and Usefulness against Fungal Pathogens

Abstract
:1. Introduction to Drugs with Activity on Fungal Membranes—Summary/History of Allylamines and Benzylamines
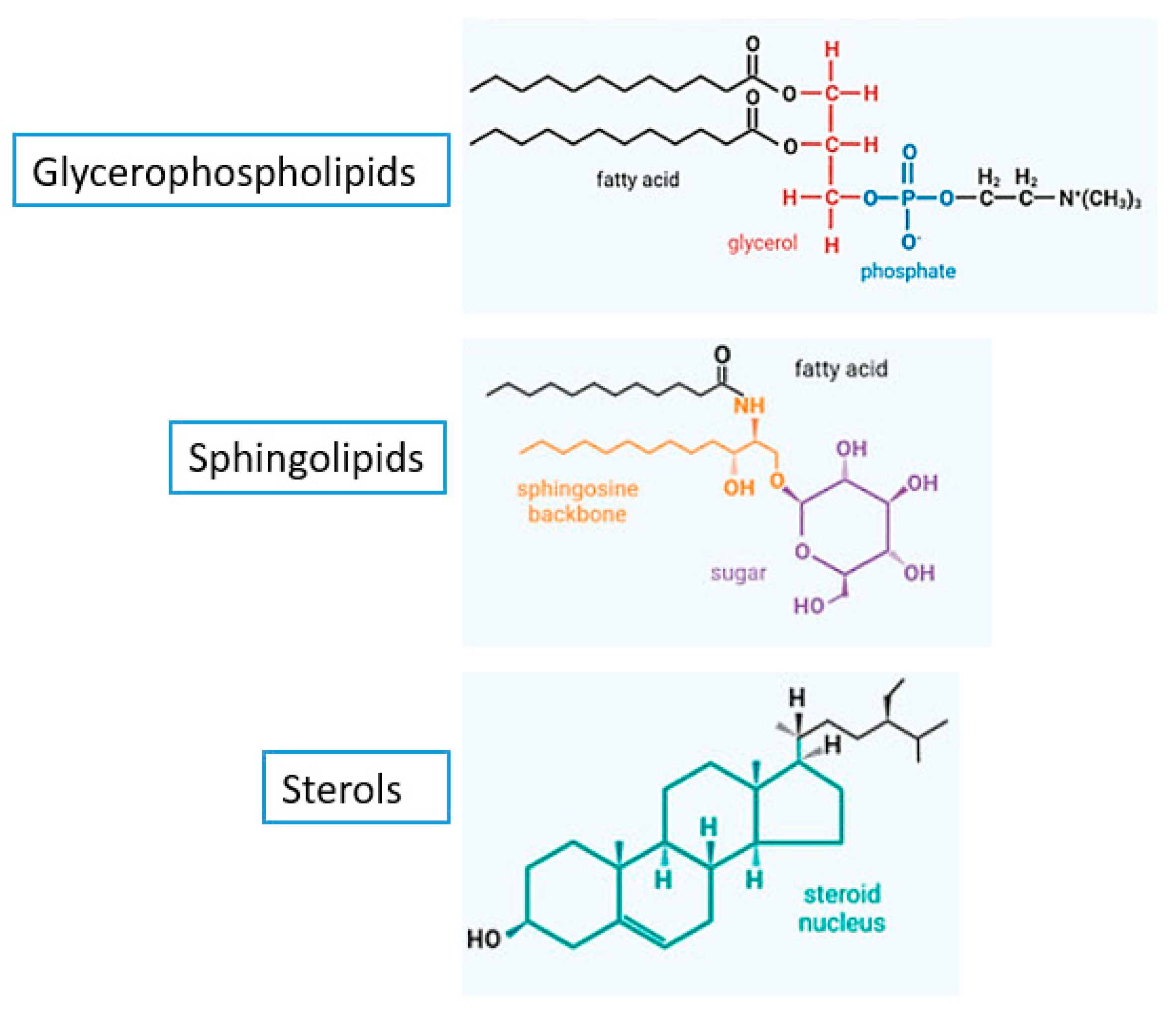
2. The Structure and Lipids of the Fungal Membrane
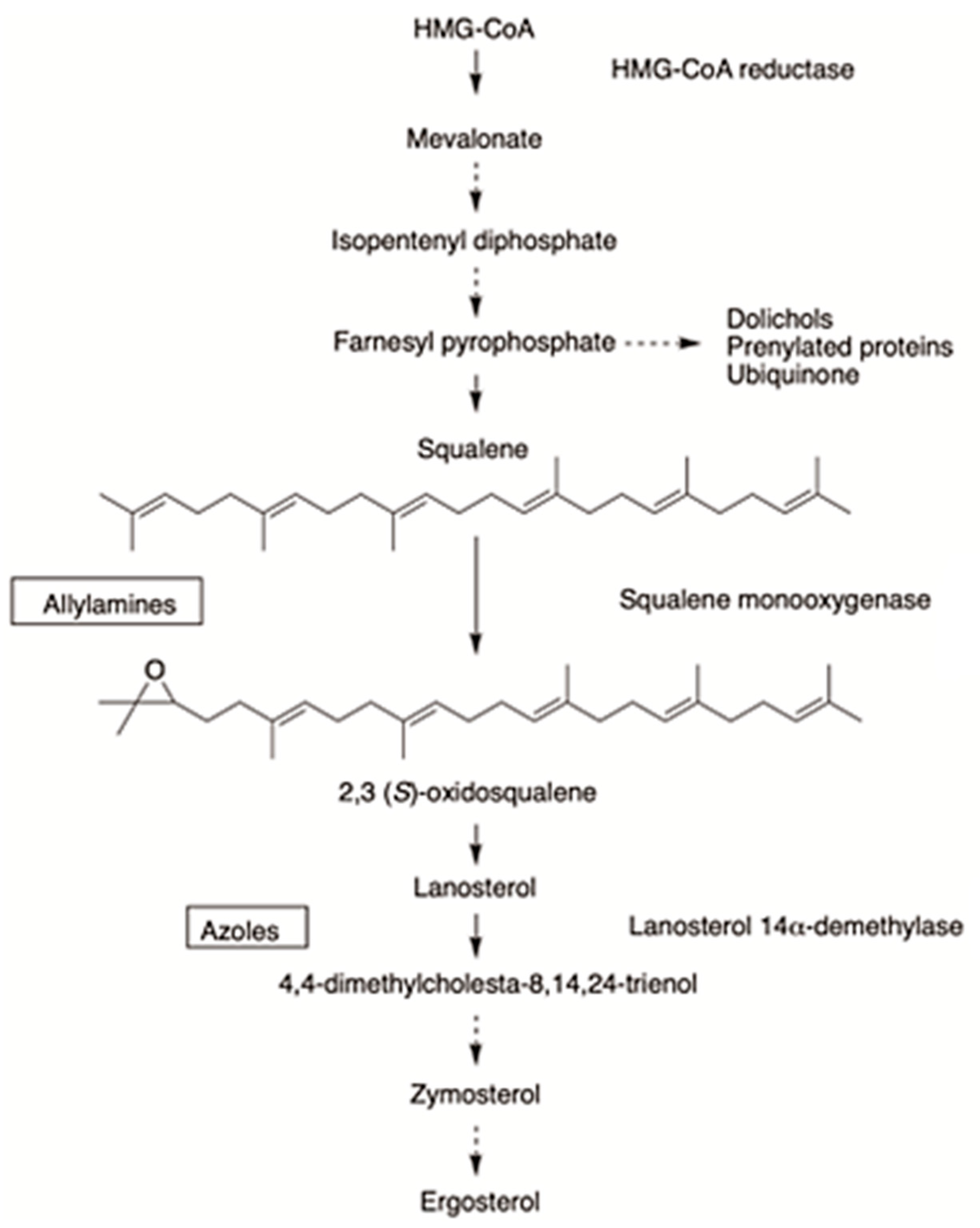
3. Mechanism of Action of Allylamines and Benzylamines
4. Dosage Forms and Pharmaceutical Formulations of Allylamines and Benzylamines
4.1. Overview of Conventional Dosage Forms of Allylamines and Benzylamines
4.2. Novel Drug Delivery Systems of Allylamines and Benzylamines
4.2.1. Microemulsions
4.2.2. Niosomes
4.2.3. Nanoemulsions
4.2.4. Dendrimers
4.2.5. Lipidic Nanoparticles
4.3. Penetration-Enhancing Strategies: Electroporation
5. Clinical Importance of Allylamines and Benzylamines
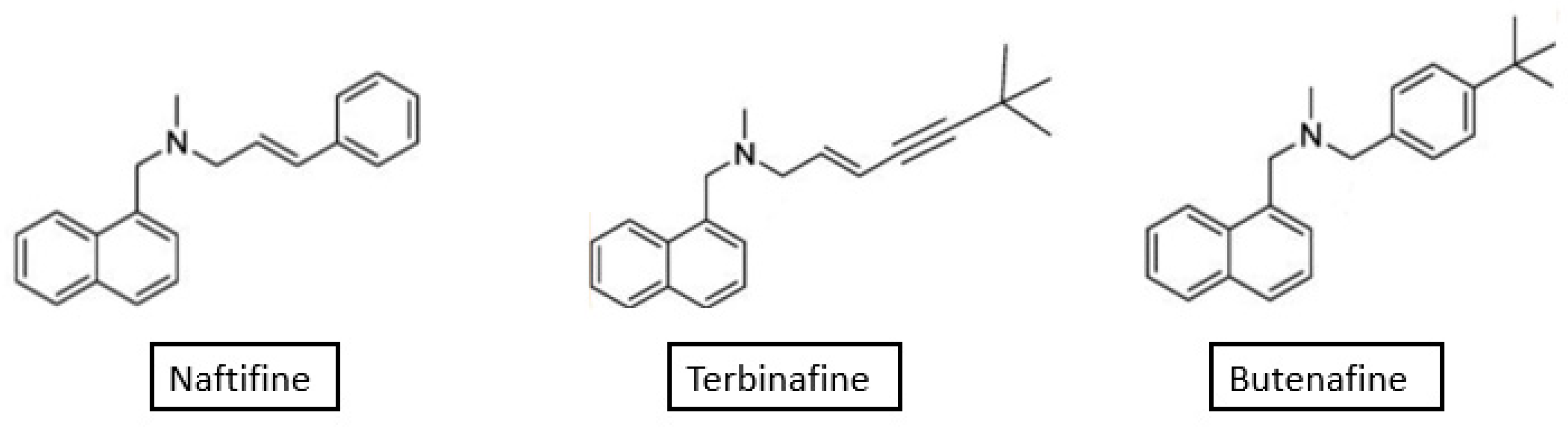
5.1. Naftifine
5.2. Terbinafine
5.3. Butenafine
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Firacative, C. Invasive Fungal Disease in Humans: Are We Aware of the Real Impact? Mem. Inst. Oswaldo Cruz 2020, 115, e200430. [Google Scholar] [CrossRef] [PubMed]
- Hasim, S.; Coleman, J.J. Targeting the Fungal Cell Wall: Current Therapies and Implications for Development of Alternative Antifungal Agents. Future Med. Chem. 2019, 11, 869–883. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases—Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Rayens, E.; Norris, K.A. Prevalence and Healthcare Burden of Fungal Infections in the United States, 2018. Open Forum Infect. Dis. 2022, 9, ofab593. [Google Scholar] [CrossRef] [PubMed]
- Gaffi—Global Action For Fungal Infections. Available online: https://gaffi.org/ (accessed on 4 July 2022).
- Garcia-Rubio, R.; de Oliveira, H.C.; Rivera, J.; Trevijano-Contador, N. The Fungal Cell Wall: Candida, Cryptococcus, and Aspergillus Species. Front. Microbiol. 2020, 10, 2993. [Google Scholar] [CrossRef] [PubMed]
- Bouz, G.; Doležal, M. Advances in Antifungal Drug Development: An Up-to-Date Mini Review. Pharmaceuticals 2021, 14, 1312. [Google Scholar] [CrossRef]
- Yang, C.; Hamel, C.; Vujanovic, V.; Gan, Y. Fungicide: Modes of Action and Possible Impact on Nontarget Microorganisms. ISRN Ecol. 2011, 2011, 130289. [Google Scholar] [CrossRef] [Green Version]
- Marek, C.L.; Timmons, S.R. 9-Antimicrobials in Pediatric Dentistry. In Pediatric Dentistry, 6th ed.; Nowak, A.J., Christensen, J.R., Mabry, T.R., Townsend, J.A., Wells, M.H., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 128–141.e1. ISBN 978-0-323-60826-8. [Google Scholar]
- Ghannoum, M.A.; Rice, L.B. Antifungal Agents: Mode of Action, Mechanisms of Resistance, and Correlation of These Mechanisms with Bacterial Resistance. Clin. Microbiol. Rev. 1999, 12, 501–517. [Google Scholar] [CrossRef] [Green Version]
- Spampinato, C.; Leonardi, D. Candida Infections, Causes, Targets, and Resistance Mechanisms: Traditional and Alternative Antifungal Agents. BioMed Res. Int. 2013, 2013, 204237. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, M.W.; Kontoyiannis, D.P.; Cornely, O.A.; Perfect, J.R.; Walsh, T.J. Novel Agents and Drug Targets to Meet the Challenges of Resistant Fungi. J. Infect. Dis. 2017, 216, S474–S483. [Google Scholar] [CrossRef]
- Mühlbacher, J.M. Naftifine: A Topical Allylamine Antifungal Agent. Clin. Dermatol. 1991, 9, 479–485. [Google Scholar] [CrossRef]
- Ryder, N.S.; Mieth, H. Allylamine Antifungal Drugs. Curr. Top. Med. Mycol. 1992, 4, 158–188. [Google Scholar] [PubMed]
- Terbinafine. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Nahm, W.K.; Orengo, I.; Rosen, T. The Antifungal Agent Butenafine Manifests Anti-Inflammatory Activity in Vivo. J. Am. Acad. Dermatol. 1999, 41, 203–206. [Google Scholar] [CrossRef]
- API | Butenafine. Available online: https://www.cdek.liu.edu/api/109827/ (accessed on 13 July 2022).
- PubChem Butenafine. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/2484 (accessed on 13 July 2022).
- Kodedová, M.; Valachovič, M.; Csáky, Z.; Sychrová, H. Variations in Yeast Plasma-Membrane Lipid Composition Affect Killing Activity of Three Families of Insect Antifungal Peptides. Cell. Microbiol. 2019, 21, e13093. [Google Scholar] [CrossRef]
- de Kroon, A.I.P.M.; Rijken, P.J.; De Smet, C.H. Checks and Balances in Membrane Phospholipid Class and Acyl Chain Homeostasis, the Yeast Perspective. Prog. Lipid Res. 2013, 52, 374–394. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Zhou, C.; Fan, J.; Shanklin, J.; Xu, C. Mechanisms and Functions of Membrane Lipid Remodeling in Plants. Plant J. 2021, 107, 37–53. [Google Scholar] [CrossRef]
- Sant, D.G.; Tupe, S.G.; Ramana, C.V.; Deshpande, M.V. Fungal Cell Membrane-Promising Drug Target for Antifungal Therapy. J. Appl. Microbiol. 2016, 121, 1498–1510. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, H.; Zhang, C.; Wu, T.; Ma, Z.; Chen, Y. Phospholipid Homeostasis Plays an Important Role in Fungal Development, Fungicide Resistance and Virulence in Fusarium Graminearum. Phytopathol. Res. 2019, 1, 16. [Google Scholar] [CrossRef] [Green Version]
- de Azevedo-Martins, A.C.; Ocaña, K.; de Souza, W.; de Vasconcelos, A.T.R.; Teixeira, M.M.G.; Camargo, E.P.; Alves, J.M.P.; Motta, M.C.M. The Importance of Glycerophospholipid Production to the Mutualist Symbiosis of Trypanosomatids. Pathogens 2021, 11, 41. [Google Scholar] [CrossRef]
- Malinsky, J.; Tanner, W.; Opekarova, M. Transmembrane Voltage: Potential to Induce Lateral Microdomains. Biochim. Biophys. Acta 2016, 1861, 806–811. [Google Scholar] [CrossRef]
- Klug, L.; Daum, G. Yeast Lipid Metabolism at a Glance. FEMS Yeast Res. 2014, 14, 369–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Rest, M.E.; Kamminga, A.H.; Nakano, A.; Anraku, Y.; Poolman, B.; Konings, W.N. The Plasma Membrane of Saccharomyces Cerevisiae: Structure, Function, and Biogenesis. Microbiol. Rev. 1995, 59, 304–322. [Google Scholar] [CrossRef] [PubMed]
- Rautenbach, M.; Troskie, A.M.; Vosloo, J.A. Antifungal Peptides: To Be or Not to Be Membrane Active. Biochimie 2016, 130, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Macabuhay, A.; Arsova, B.; Walker, R.; Johnson, A.; Watt, M.; Roessner, U. Modulators or Facilitators? Roles of Lipids in Plant Root-Microbe Interactions. Trends Plant Sci. 2022, 27, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.C.; Marquês, J.T.; Bento-Oliveira, A.; de Almeida, R.F.M. Sphingolipid-Enriched Domains in Fungi. FEBS Lett. 2020, 594, 3698–3718. [Google Scholar] [CrossRef] [PubMed]
- Young, S.A.; Mina, J.G.; Denny, P.W.; Smith, T.K. Sphingolipid and Ceramide Homeostasis: Potential Therapeutic Targets. Biochem. Res. Int. 2012, 2012, 248135. [Google Scholar] [CrossRef] [Green Version]
- Gault, C.; Obeid, L.; Hannun, Y. An Overview of Sphingolipid Metabolism: From Synthesis to Breakdown. Adv. Exp. Med. Biol. 2010, 688, 1–23. [Google Scholar]
- Martin, S.W.; Konopka, J.B. Lipid Raft Polarization Contributes to Hyphal Growth in Candida Albicans. Eukaryot. Cell 2004, 3, 675–684. [Google Scholar] [CrossRef] [Green Version]
- PAK Kinases Ste20 and Pak1 Govern Cell Polarity at Different Stages of Mating in Cryptococcus neoformans—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC519142/ (accessed on 16 July 2022).
- Singh, A.; Del Poeta, M. Lipid Signalling in Pathogenic Fungi. Cell. Microbiol. 2011, 13, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Mota Fernandes, C.; Del Poeta, M. Fungal Sphingolipids: Role in the Regulation of Virulence and Potential as Targets for Future Antifungal Therapies. Expert Rev. Anti Infect. Ther. 2020, 18, 1083–1092. [Google Scholar] [CrossRef]
- Joffrion, T.M.; Cushion, M.T. Sterol Biosynthesis and Sterol Uptake in the Fungal Pathogen Pneumocystis Carinii. FEMS Microbiol. Lett. 2010, 311, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Uemura, S.; Shishido, F.; Tani, M.; Mochizuki, T.; Abe, F.; Inokuchi, J. Loss of Hydroxyl Groups from the Ceramide Moiety Can Modify the Lateral Diffusion of Membrane Proteins in S. Cerevisiae. J. Lipid Res. 2014, 55, 1343–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Tong, J.; Lee, C.W.; Ha, S.; Eom, S.H.; Im, Y.J. Structural Mechanism of Ergosterol Regulation by Fungal Sterol Transcription Factor Upc2. Nat. Commun. 2015, 6, 6129. [Google Scholar] [CrossRef] [Green Version]
- Jordá, T.; Puig, S. Regulation of Ergosterol Biosynthesis in Saccharomyces cerevisiae. Genes 2020, 11, 795. [Google Scholar] [CrossRef] [PubMed]
- Man, S.M.; Karki, R.; Kanneganti, T.-D. Molecular Mechanisms and Functions of Pyroptosis, Inflammatory Caspases and Inflammasomes in Infectious Diseases. Immunol. Rev. 2017, 277, 61–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, M.L. The Multifunctional Fungal Ergosterol. mBio 2018, 9, e01755-18. [Google Scholar] [CrossRef] [Green Version]
- Gerhold, J.M.; Cansiz-Arda, Ş.; Lõhmus, M.; Engberg, O.; Reyes, A.; van Rennes, H.; Sanz, A.; Holt, I.J.; Cooper, H.M.; Spelbrink, J.N. Human Mitochondrial DNA-Protein Complexes Attach to a Cholesterol-Rich Membrane Structure. Sci. Rep. 2015, 5, 15292. [Google Scholar] [CrossRef] [Green Version]
- Alcazar-Fuoli, L.; Mellado, E. Ergosterol Biosynthesis in Aspergillus fumigatus: Its Relevance as an Antifungal Target and Role in Antifungal Drug Resistance. Front. Microbiol. 2013, 3, 439. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; He, B.; Ma, L.; Sun, Y.; Niu, Y.; Zeng, B. Recent Advances in Ergosterol Biosynthesis and Regulation Mechanisms in Saccharomyces cerevisiae. Indian J. Microbiol. 2017, 57, 270–277. [Google Scholar] [CrossRef]
- Aguilera, F.; Peinado, R.A.; Millán, C.; Ortega, J.M.; Mauricio, J.C. Relationship between Ethanol Tolerance, H+ -ATPase Activity and the Lipid Composition of the Plasma Membrane in Different Wine Yeast Strains. Int. J. Food Microbiol. 2006, 110, 34–42. [Google Scholar] [CrossRef]
- Vik, Å.; Rine, J. Upc2p and Ecm22p, Dual Regulators of Sterol Biosynthesis in Saccharomyces cerevisiae. Mol. Cell. Biol. 2001, 21, 6395–6405. [Google Scholar] [CrossRef] [PubMed]
- Dhingra, S.; Cramer, R.A. Regulation of Sterol Biosynthesis in the Human Fungal Pathogen Aspergillus fumigatus: Opportunities for Therapeutic Development. Front. Microbiol. 2017, 8, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristan, K.; Rižner, T.L. Steroid-Transforming Enzymes in Fungi. J. Steroid Biochem. Mol. Biol. 2012, 129, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Douglas, L.M.; Konopka, J.B. Plasma Membrane Organization Promotes Virulence of the Human Fungal Pathogen Candida albicans. J. Microbiol. Seoul Korea 2016, 54, 178–191. [Google Scholar] [CrossRef] [Green Version]
- Mazu, T.K.; Bricker, B.A.; Flores-Rozas, H.; Ablordeppey, S.Y. The Mechanistic Targets of Antifungal Agents: An Overview. Mini Rev. Med. Chem. 2016, 16, 555–578. [Google Scholar] [CrossRef]
- Petranyi, G.; Ryder, N.S.; Stütz, A. Allylamine Derivatives: New Class of Synthetic Antifungal Agents Inhibiting Fungal Squalene Epoxidase. Science 1984, 224, 1239–1241. [Google Scholar] [CrossRef]
- Birnbaum, J.E. Pharmacology of the Allylamines. J. Am. Acad. Dermatol. 1990, 23, 782–785. [Google Scholar] [CrossRef]
- Kathiravan, M.K.; Salake, A.B.; Chothe, A.S.; Dudhe, P.B.; Watode, R.P.; Mukta, M.S.; Gadhwe, S. The Biology and Chemistry of Antifungal Agents: A Review. Bioorg. Med. Chem. 2012, 20, 5678–5698. [Google Scholar] [CrossRef]
- Mascotti, M.L.; Juri Ayub, M.; Furnham, N.; Thornton, J.M.; Laskowski, R.A. Chopping and Changing: The Evolution of the Flavin-Dependent Monooxygenases. J. Mol. Biol. 2016, 428, 3131–3146. [Google Scholar] [CrossRef] [Green Version]
- Haria, M.; Bryson, H.M. Amorolfine. A Review of Its Pharmacological Properties and Therapeutic Potential in the Treatment of Onychomycosis and Other Superficial Fungal Infections. Drugs 1995, 49, 103–120. [Google Scholar] [CrossRef]
- Vardanyan, R.; Hruby, V. Chapter 33—Antifungal Drugs. In Synthesis of Best-Seller Drugs; Vardanyan, R., Hruby, V., Eds.; Academic Press: Boston, MA, USA, 2016; pp. 677–686. ISBN 978-0-12-411492-0. [Google Scholar]
- Ryder, N.S. Mechanism of Action and Biochemical Selectivity of Allylamine Antimycotic Agents. Ann. N. Y. Acad. Sci. 1988, 544, 208–220. [Google Scholar] [CrossRef] [PubMed]
- Lanyi, J.K.; Plachy, W.Z.; Kates, M. Lipid Interactions in Membranes of Extremely Halophilic Bacteria. II. Modification of the Bilayer Structure by Squalene. Biochemistry 1974, 13, 4914–4920. [Google Scholar] [CrossRef] [PubMed]
- Ngo, H.X.; Garneau-Tsodikova, S.; Green, K.D. A Complex Game of Hide and Seek: The Search for New Antifungals. MedChemComm 2016, 7, 1285–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scorzoni, L.; de Paula, E.; Silva, A.C.A.; Marcos, C.M.; Assato, P.A.; de Melo, W.C.M.A.; de Oliveira, H.C.; Costa-Orlandi, C.B.; Mendes-Giannini, M.J.S.; Fusco-Almeida, A.M. Antifungal Therapy: New Advances in the Understanding and Treatment of Mycosis. Front. Microbiol. 2017, 8, 36. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Barbhuniya, J.N.; Biswas, I.; Bhattacharya, S.; Kundu, P.K. Studies on Comparison of the Efficacy of Terbinafine 1% Cream and Butenafine 1% Cream for the Treatment of Tinea cruris. Indian Dermatol. Online J. 2010, 1, 8–9. [Google Scholar] [CrossRef]
- Iwatani, W.; Arika, T.; Yamaguchi, H. Two Mechanisms of Butenafine Action in Candida albicans. Antimicrob. Agents Chemother. 1993, 37, 785–788. [Google Scholar] [CrossRef] [Green Version]
- Sagatova, A.A. Strategies to Better Target Fungal Squalene Monooxygenase. J. Fungi 2021, 7, 49. [Google Scholar] [CrossRef]
- Gupta, M.; Sharma, V.; Chauhan, N.S. Chapter 11—Promising Novel Nanopharmaceuticals for Improving Topical Antifungal Drug Delivery. In Nano- and Microscale Drug Delivery Systems; Grumezescu, A.M., Ed.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 197–228. ISBN 978-0-323-52727-9. [Google Scholar]
- Sahni, K.; Singh, S.; Dogra, S. Newer Topical Treatments in Skin and Nail Dermatophyte Infections. Indian Dermatol. Online J. 2018, 9, 149–158. [Google Scholar] [CrossRef]
- Jaiswal, A.; Sharma, R.P.; Garg, A.P. An open randomized comparative study to test the efficacy and safety of oral terbinafine pulse as a monotherapy and in combination with topical ciclopirox olamine 8% or topical amorolfine hydrochloride 5% in the treatment of onychomycosis. Indian J. Dermatol. Venereol. Leprol. 2007, 73, 393–396. [Google Scholar] [CrossRef]
- Food and Drug Administration (FDA). Review and Evaluation of Pharmacology/Toxicology Data O Fbutenafine, NDA 21-307 (000)/09-29-2000. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2001/21-307_Lotrimin_pharmr.pdf. (accessed on 24 June 2019).
- Garg, A.; Sharma, G.S.; Goyal, A.K.; Ghosh, G.; Si, S.C.; Rath, G. Recent Advances in Topical Carriers of Anti-Fungal Agents. Heliyon 2020, 6, e04663. [Google Scholar] [CrossRef]
- Lam, P.L.; Lee, K.K.H.; Wong, R.S.M.; Cheng, G.Y.M.; Bian, Z.X.; Chui, C.H.; Gambari, R. Recent Advances on Topical Antimicrobials for Skin and Soft Tissue Infections and Their Safety Concerns. Crit. Rev. Microbiol. 2018, 44, 40–78. [Google Scholar] [CrossRef] [PubMed]
- Güngör, S.; Erdal, M.S.; Aksu, B. New Formulation Strategies in Topical Antifungal Therapy. J. Cosmet. Dermatol. Sci. Appl. 2013, 3, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Robert, M.E.M.; Kalia, Y.N. New Developments in Topical Antifungal Therapy. Am. J. Drug Deliv. 2006, 4, 231–247. [Google Scholar] [CrossRef]
- Gupta, M.; Agrawal, U.; Vyas, S.P. Nanocarrier-Based Topical Drug Delivery for the Treatment of Skin Diseases. Expert Opin. Drug Deliv. 2012, 9, 783–804. [Google Scholar] [CrossRef]
- Kumar, L.; Verma, S.; Bhardwaj, A.; Vaidya, S.; Vaidya, B. Eradication of Superficial Fungal Infections by Conventional and Novel Approaches: A Comprehensive Review. Artif. Cells Nanomed. Biotechnol. 2014, 42, 32–46. [Google Scholar] [CrossRef]
- Heuschkel, S.; Goebel, A.; Neubert, R.H.H. Microemulsions—Modern Colloidal Carrier for Dermal and Transdermal Drug Delivery. J. Pharm. Sci. 2008, 97, 603–631. [Google Scholar] [CrossRef]
- Erdal, M.S.; Gungor, S.; Ozsoy, Y. Microemulsions of Naftifine Hydrochloride: Characterization of Impact on Stratum Corneum Permeability with ATR-FTIR Spectroscopy. Eur. J. Pharm. Sci. 2011, 44, 159–160. [Google Scholar]
- Zhao, X.-Y.; Cao, Q.; Zheng, L.-Q.; Zhang, G.-Y. Rheological Properties and Microstructures of Gelatin-Containing Microemulsion-Based Organogels. Colloids Surf. Physicochem. Eng. Asp. 2006, 281, 67–73. [Google Scholar] [CrossRef]
- Morrow, D.I.J.; McCarron, P.A.; Woolfson, A.D.; Donnelly, R.F. Innovative Strategies for Enhancing Topical and Transdermal Drug Delivery. Open Drug Deliv. J. 2007, 1, 36–59. [Google Scholar] [CrossRef]
- Junginger, H.E.; Hofland, H.; Bouwstra, J.A. Liposomes and Niosomes : Interactions with Human Skin. Cosmet. Toilet. 1991, 106, 45–50. [Google Scholar]
- Choi, M.J.; Maibach, H.I. Liposomes and Niosomes as Topical Drug Delivery Systems. Skin Pharmacol. Physiol. 2005, 18, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Williams, A. Transdermal and Topical Drug Delivery from Theory to Clinical Practice; Pharmaceutical Press: London, UK, 2003. [Google Scholar]
- Barakat, H.S.; Darwish, I.A.; El-Khordagui, L.K.; Khalafallah, N.M. Development of Naftifine Hydrochloride Alcohol-Free Niosome Gel. Drug Dev. Ind. Pharm. 2009, 35, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Sathali, A.A.H.; Rajalakshmi, G. Evaluation of Transdermal Targeted Niosomal Drug Delivery of Terbinafine Hydrochloride. Int. J. PharmTech Res. 2010, 2, 2081–2089. [Google Scholar]
- Rai, V.K.; Mishra, N.; Yadav, K.S.; Yadav, N.P. Nanoemulsion as Pharmaceutical Carrier for Dermal and Transdermal Drug Delivery: Formulation Development, Stability Issues, Basic Considerations and Applications. J. Control. Release Off. J. Control. Release Soc. 2018, 270, 203–225. [Google Scholar] [CrossRef]
- Karri, V.V.S.R.; Raman, S.; Kuppusamy, G.; Mulukutla, S.; Ramaswamy, S.; Malayandi, R. Terbinafine Hydrochloride Loaded Nanoemulsion Based Gel for Topical Application. J. Pharm. Investig. 2014, 45, 79–89. [Google Scholar] [CrossRef]
- Khairnar, G.A.; Chavan-Patil, A.B.; Palve, P.R.; Bhise, S.B.; Mourya, V.K.; Kulkarni, C.G. Dendrimers: Potential Tool for Enhancement of Antifungal Activity. Int. J. PharmTech Res. 2010, 2, 736–739. [Google Scholar]
- Jain, S.; Patel, N.; Shah, M.K.; Khatri, P.; Vora, N. Recent Advances in Lipid-Based Vesicles and Particulate Carriers for Topical and Transdermal Application. J. Pharm. Sci. 2017, 106, 423–445. [Google Scholar] [CrossRef]
- Müller, R.H.; Radtke, M.; Wissing, S.A. Solid Lipid Nanoparticles (SLN) and Nanostructured Lipid Carriers (NLC) in Cosmetic and Dermatological Preparations. Adv. Drug Deliv. Rev. 2002, 54, S131–S155. [Google Scholar] [CrossRef]
- Garcês, A.; Amaral, M.H.; Sousa Lobo, J.M.; Silva, A.C. Formulations Based on Solid Lipid Nanoparticles (SLN) and Nanostructured Lipid Carriers (NLC) for Cutaneous Use: A Review. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2018, 112, 159–167. [Google Scholar] [CrossRef]
- Joshi, M.; Patravale, V. Nanostructured Lipid Carrier (NLC) Based Gel of Celecoxib. Int. J. Pharm. 2008, 346, 124–132. [Google Scholar] [CrossRef]
- Wiedersberg, S.; Leopold, C.S.; Guy, R.H. Bioavailability and Bioequivalence of Topical Glucocorticoids. Eur. J. Pharm. Biopharm. Off. J. Arb. Pharm. Verfahr. EV 2008, 68, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Vaghasiya, H.; Kumar, A.; Sawant, K. Development of Solid Lipid Nanoparticles Based Controlled Release System for Topical Delivery of Terbinafine Hydrochloride. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2013, 49, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Liu, D.-Z.; Liu, J.-J.; Chang, T.-W.; Ho, H.-O.; Sheu, M.-T. Development of Terbinafine Solid Lipid Nanoparticles as a Topical Delivery System. Int. J. Nanomed. 2012, 7, 4409–4418. [Google Scholar] [CrossRef] [Green Version]
- Gaba, B.; Fazil, M.; Khan, S.A.; Ali, A.; Baboota, S.; Ali, J. Nanostructured Lipid Carrier System for Topical Delivery of Terbinafine Hydrochloride. Bull. Fac. Pharm. Cairo Univ. 2015, 53, 147–159. [Google Scholar] [CrossRef] [Green Version]
- Novickij, V.; Švedienė, J.; Paškevičius, A.; Markovskaja, S.; Girkontaitė, I.; Zinkevičienė, A.; Lastauskienė, E.; Novickij, J. Pulsed Electric Field-Assisted Sensitization of Multidrug-Resistant Candida Albicans to Antifungal Drugs. Future Microbiol. 2018, 13, 535–546. [Google Scholar] [CrossRef]
- Rotta, I.; Ziegelmann, P.K.; Otuki, M.F.; Riveros, B.S.; Bernardo, N.L.M.C.; Correr, C.J. Efficacy of Topical Antifungals in the Treatment of Dermatophytosis: A Mixed-Treatment Comparison Meta-Analysis Involving 14 Treatments. JAMA Dermatol. 2013, 149, 341–349. [Google Scholar] [CrossRef]
- Rotta, I.; Sanchez, A.; Gonçalves, P.R.; Otuki, M.F.; Correr, C.J. Efficacy and Safety of Topical Antifungals in the Treatment of Dermatomycosis: A Systematic Review. Br. J. Dermatol. 2012, 166, 927–933. [Google Scholar] [CrossRef]
- Del Rosso, J.Q.; Kircik, L.H. Optimizing Topical Antifungal Therapy for Superficial Cutaneous Fungal Infections: Focus on Topical Naftifine for Cutaneous Dermatophytosis. J. Drugs Dermatol. 2013, 12, s165–s171. [Google Scholar]
- Stein Gold, L.F.; Parish, L.C.; Vlahovic, T.; Plaum, S.; Kircik, L.; Fleischer, A.B.; Verma, A.; Olayinka, B.; Hardas, B. Efficacy and Safety of Naftifine HCl Gel 2% in the Treatment of Interdigital and Moccasin Type Tinea Pedis: Pooled Results from Two Multicenter, Randomized, Double-Blind, Vehicle-Controlled Trials. J. Drugs Dermatol. 2013, 12, 911–918. [Google Scholar]
- Monk, J.P.; Brogden, R.N. Naftifine. A Review of Its Antimicrobial Activity and Therapeutic Use in Superficial Dermatomycoses. Drugs 1991, 42, 659–672. [Google Scholar] [CrossRef]
- Gupta, A.K.; Ryder, J.E.; Cooper, E.A. Naftifine: A Review. J. Cutan. Med. Surg. 2008, 12, 51–58. [Google Scholar] [CrossRef]
- Ryder, N.S.; Seidl, G.; Troke, P.F. Effect of the Antimycotic Drug Naftifine on Growth of and Sterol Biosynthesis in Candida albicans. Antimicrob. Agents Chemother. 1984, 25, 483–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venugopal, P.V.; Venugopal, T.V. Antimycotic Susceptibility Testing of Mould-Fungi with Allylamines by Disk Diffusion. Indian J. Med. Sci. 1995, 49, 109–113. [Google Scholar] [PubMed]
- Moț, A.C.; Pârvu, M.; Pârvu, A.E.; Roşca-Casian, O.; Dina, N.E.; Leopold, N.; Silaghi-Dumitrescu, R.; Mircea, C. Reversible Naftifine-Induced Carotenoid Depigmentation in Rhodotorula mucilaginosa (A. Jörg.) F.C. Harrison Causing Onychomycosis. Sci. Rep. 2017, 7, 11125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, M.H.; Bridges, T.; Avakian, E.; Plaum, S.; Pappert, E.J.; Fleischer, A.B.; Hardas, B. An Open-Label Study of Naftifine Hydrochloride 1% Gel in the Treatment of Tinea Versicolor. Skinmed 2011, 9, 283–286. [Google Scholar]
- Gold, M.H.; Bridges, T.; Avakian, E.V.; Plaum, S.; Fleischer, A.B.; Hardas, B. An Open-Label Pilot Study of Naftifine 1% Gel in the Treatment of Seborrheic Dermatitis of the Scalp. J. Drugs Dermatol. 2012, 11, 514–518. [Google Scholar]
- Sun, J.; Zhang, Y.; Su, J.; Dai, T.; Chen, J.; Zhang, L.; Wang, H.; Liu, W.; Huang, M.; Chen, Z. Naftifine Enhances Photodynamic Therapy against Staphylococcus Aureus by Inhibiting Staphyloxanthin Expression. Dyes Pigments 2020, 179, 108392. [Google Scholar] [CrossRef]
- Chen, F.; Di, H.; Wang, Y.; Cao, Q.; Xu, B.; Zhang, X.; Yang, N.; Liu, G.; Yang, C.-G.; Xu, Y.; et al. Small-Molecule Targeting of a Diapophytoene Desaturase Inhibits, S. Aureus Virulence. Nat. Chem. Biol. 2016, 12, 174–179. [Google Scholar] [CrossRef]
- Evans, E.G.; James, I.G.; Seaman, R.A.; Richardson, M.D. Does Naftifine Have Anti-Inflammatory Properties? A Double-Blind Comparative Study with 1% Clotrimazole/1% Hydrocortisone in Clinically Diagnosed Fungal Infection of the Skin. Br. J. Dermatol. 1993, 129, 437–442. [Google Scholar] [CrossRef]
- Gold, M.; Dhawan, S.; Verma, A.; Kuligowski, M.; Dobrowski, D. Efficacy and Safety of Naftifine HCl Cream 2% in the Treatment of Pediatric Subjects With Tinea Corporis. J. Drugs Dermatol. JDD 2016, 15, 743–748. [Google Scholar]
- Corazza, M.; Lauriola, M.M.; Virgili, A. Allergic Contact Dermatitis to Naftifine. Contact Dermat. 2005, 53, 302–303. [Google Scholar] [CrossRef] [PubMed]
- Routt, E.T.; Jim, S.C.; Zeichner, J.A.; Kircik, L.H. What Is New in Fungal Pharmacotherapeutics? J. Drugs Dermatol. 2014, 13, 391–395; quiz 396. [Google Scholar]
- Leung, A.K.C.; Lam, J.M.; Leong, K.F.; Hon, K.L.; Barankin, B.; Leung, A.A.M.; Wong, A.H.C. Onychomycosis: An Updated Review. Recent Pat. Inflamm. Allergy Drug Discov. 2020, 14, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Hawks, M.K.; Rupert, J.P.; Svarverud, J.E. Terbinafine for Onychomycosis. Am. Fam. Physician 2018, 98. [Google Scholar]
- Leung, A.K.C.; Hon, K.L.; Leong, K.F.; Barankin, B.; Lam, J.M. Tinea Capitis: An Updated Review. Recent Pat. Inflamm. Allergy Drug Discov. 2020, 14, 58–68. [Google Scholar] [CrossRef]
- Kreijkamp-Kaspers, S.; Hawke, K.; Guo, L.; Kerin, G.; Bell-Syer, S.E.; Magin, P.; Bell-Syer, S.V.; van Driel, M.L. Oral Antifungal Medication for Toenail Onychomycosis. Cochrane Database Syst. Rev. 2017, 7, CD010031. [Google Scholar] [CrossRef]
- Gupta, A.K.; Daigle, D.; Foley, K.A. Network Meta-Analysis of Onychomycosis Treatments. Skin Appendage Disord. 2015, 1, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, P.; Singal, A.; Pandhi, D.; Das, S. Comparative Efficacy of Continuous and Pulse Dose Terbinafine Regimes in Toenail Dermatophytosis: A Randomized Double-Blind Trial. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Paquet, M.; Simpson, F.; Tavakkol, A. Terbinafine in the Treatment of Dermatophyte Toenail Onychomycosis: A Meta-Analysis of Efficacy for Continuous and Intermittent Regimens. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 267–272. [Google Scholar] [CrossRef]
- Schäfer-Korting, M.; Schoellmann, C.; Korting, H.C. Fungicidal Activity plus Reservoir Effect Allow Short Treatment Courses with Terbinafine in Tinea Pedis. Skin Pharmacol. Physiol. 2008, 21, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Leung, A.K.; Lam, J.M.; Leong, K.F.; Hon, K.L. Tinea Corporis: An Updated Review. Drugs Context 2020, 9, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Ely, J.W.; Rosenfeld, S.; Seabury Stone, M. Diagnosis and Management of Tinea Infections. Am. Fam. Physician 2014, 90, 702–710. [Google Scholar] [PubMed]
- Ward, H.; Parkes, N.; Smith, C.; Kluzek, S.; Pearson, R. Consensus for the Treatment of Tinea Pedis: A Systematic Review of Randomised Controlled Trials. J. Fungi 2022, 8, 351. [Google Scholar] [CrossRef] [PubMed]
- El-Gohary, M.; van Zuuren, E.J.; Fedorowicz, Z.; Burgess, H.; Doney, L.; Stuart, B.; Moore, M.; Little, P. Topical Antifungal Treatments for Tinea Cruris and Tinea Corporis. Cochrane Database Syst. Rev. 2014, 172, CD009992. [Google Scholar] [CrossRef]
- de Chauvin, M.F.; Viguié-Vallanet, C.; Kienzler, J.-L.; Larnier, C. Novel, Single-Dose, Topical Treatment of Tinea Pedis Using Terbinafine: Results of a Dose-Finding Clinical Trial. Mycoses 2008, 51, 1–6. [Google Scholar] [CrossRef]
- Li, R.Y.; Wang, A.P.; Xu, J.H.; Xi, L.Y.; Fu, M.H.; Zhu, M.; Xu, M.L.; Li, X.Q.; Lai, W.; Liu, W.D.; et al. Efficacy and Safety of 1 % Terbinafine Film-Forming Solution in Chinese Patients with Tinea Pedis: A Randomized, Double-Blind, Placebo-Controlled, Multicenter, Parallel-Group Study. Clin. Drug Investig. 2014, 34, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Balfour, J.A.; Faulds, D. Terbinafine. A Review of Its Pharmacodynamic and Pharmacokinetic Properties, and Therapeutic Potential in Superficial Mycoses. Drugs 1992, 43, 259–284. [Google Scholar] [CrossRef]
- Ryder, N.S.; Wagner, S.; Leitner, I. In Vitro Activities of Terbinafine against Cutaneous Isolates of Candida albicans and Other Pathogenic Yeasts. Antimicrob. Agents Chemother. 1998, 42, 1057–1061. [Google Scholar] [CrossRef] [Green Version]
- Hossain, A.S.M.M.A.; Sil, B.C.; Iliopoulos, F.; Lever, R.; Hadgraft, J.; Lane, M.E. Preparation, Characterisation, and Topical Delivery of Terbinafine. Pharmaceutics 2019, 11, 548. [Google Scholar] [CrossRef] [Green Version]
- Hay, R.J. Therapeutic Potential of Terbinafine in Subcutaneous and Systemic Mycoses. Br. J. Dermatol. 1999, 141, 36–40. [Google Scholar] [CrossRef]
- Pérez, A. Terbinafine: Broad New Spectrum of Indications in Several Subcutaneous and Systemic and Parasitic Diseases. Mycoses 1999, 42, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.P.Z.; Sutton, D.A.; García, D.; Gené, J.; Thomson, P.; Wiederhold, N.; Guarro, J. Species Diversity of Aspergillus Section Versicolores in Clinical Samples and Antifungal Susceptibility. Fungal Biol. 2016, 120, 1458–1467. [Google Scholar] [CrossRef] [PubMed]
- de Ávila Antunes, T.; de Oliveira Nobre, M.; de Faria, R.O.; Meinerz, A.R.M.; Martins, A.A.; Cleff, M.B.; Fernandes, C.G.; Meireles, e.M.C.A. Experimental cutaneous sporotrichosis: In vivo evaluation of itraconazole and terbinafine. Rev. Soc. Bras. Med. Trop. 2009, 42, 706–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francesconi, G.; Valle, A.C.; Passos, S.; Reis, R.; Galhardo, M.C. Terbinafine (250 Mg/Day): An Effective and Safe Treatment of Cutaneous Sporotrichosis. J. Eur. Acad. Dermatol. Venereol. JEADV 2009, 23, 1273–1276. [Google Scholar] [CrossRef] [PubMed]
- Graminha, M.A.S.; Rocha, E.M.F.; Prade, R.A.; Martinez-Rossi, N.M. Terbinafine Resistance Mediated by Salicylate 1-Monooxygenase in Aspergillus nidulans. Antimicrob. Agents Chemother. 2004, 48, 3530–3535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranawaka, R.R. Treatment of Chromoblastomycosis with a Combination of Debulking Surgery, Intralesional Amphotericin B, and Oral Terbinafine. Int. J. Dermatol. 2021, 60, 1040–1041. [Google Scholar] [CrossRef] [PubMed]
- Mejías Manzano, M.L.Á.; Giráldez Gallego, Á.; Ontanilla Clavijo, G.; Sousa Martín, J.M. Terbinafine-induced hepatotoxicity. Gastroenterol. Hepatol. 2019, 42, 394–395. [Google Scholar] [CrossRef]
- Ricardo, J.W.; Lipner, S.R. Safety of current therapies for onychomycosis. Expert Opin. Drug Saf. 2020, 19, 1395–1408. [Google Scholar] [CrossRef]
- Andersson, N.W.; Thomsen, S.F.; Andersen, J.T. Evaluation of Association Between Oral and Topical Terbinafine Use in Pregnancy and Risk of Major Malformations and Spontaneous Abortion. JAMA Dermatol. 2020, 156, 375–383. [Google Scholar] [CrossRef]
- Shen, J.J.; Arendrup, M.C.; Verma, S.; Saunte, D.M.L. The Emerging Terbinafine-Resistant Trichophyton Epidemic: What Is the Role of Antifungal Susceptibility Testing? Dermatol. Basel Switz. 2022, 238, 60–79. [Google Scholar] [CrossRef]
- Mukherjee, P.K.; Leidich, S.D.; Isham, N.; Leitner, I.; Ryder, N.S.; Ghannoum, M.A. Clinical Trichophyton Rubrum Strain Exhibiting Primary Resistance to Terbinafine. Antimicrob. Agents Chemother. 2003, 47, 82–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begum, J.; Das, P. Antifungal Resistance in Dermatophytosis: A Global Health Concern: Antifungal Resistance in Dermatophytes. Lett. Anim. Biol. 2022, 2, 41–45. [Google Scholar]
- Favre, B.; Ghannoum, M.A.; Ryder, N.S. Biochemical Characterization of Terbinafine-Resistant Trichophyton Rubrum Isolates. Med. Mycol. 2004, 42, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Rudramurthy, S.M.; Shankarnarayan, S.A.; Dogra, S.; Shaw, D.; Mushtaq, K.; Paul, R.A.; Narang, T.; Chakrabarti, A. Mutation in the Squalene Epoxidase Gene of Trichophyton Interdigitale and Trichophyton Rubrum Associated with Allylamine Resistance. Antimicrob. Agents Chemother. 2018, 62, e02522-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurana, A.; Masih, A.; Chowdhary, A.; Sardana, K.; Borker, S.; Gupta, A.; Gautam, R.K.; Sharma, P.K.; Jain, D. Correlation of In Vitro Susceptibility Based on MICs and Squalene Epoxidase Mutations with Clinical Response to Terbinafine in Patients with Tinea Corporis/Cruris. Antimicrob. Agents Chemother. 2018, 62, e01038-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Masih, A.; Monroy-Nieto, J.; Singh, P.K.; Bowers, J.; Travis, J.; Khurana, A.; Engelthaler, D.M.; Meis, J.F.; Chowdhary, A. A Unique Multidrug-Resistant Clonal Trichophyton Population Distinct from Trichophyton Mentagrophytes/Trichophyton Interdigitale Complex Causing an Ongoing Alarming Dermatophytosis Outbreak in India: Genomic Insights and Resistance Profile. Fungal Genet. Biol. 2019, 133, 103266. [Google Scholar] [CrossRef]
- Singh, A.; Masih, A.; Khurana, A.; Singh, P.K.; Gupta, M.; Hagen, F.; Meis, J.F.; Chowdhary, A. High Terbinafine Resistance in Trichophyton Interdigitale Isolates in Delhi, India Harbouring Mutations in the Squalene Epoxidase Gene. Mycoses 2018, 61, 477–484. [Google Scholar] [CrossRef]
- Moreno-Sabater, A.; Normand, A.-C.; Bidaud, A.-L.; Cremer, G.; Foulet, F.; Brun, S.; Bonnal, C.; Aït-Ammar, N.; Jabet, A.; Ayachi, A.; et al. Terbinafine Resistance in Dermatophytes: A French Multicenter Prospective Study. J. Fungi 2022, 8, 220. [Google Scholar] [CrossRef]
- Yamada, T.; Maeda, M.; Alshahni, M.M.; Tanaka, R.; Yaguchi, T.; Bontems, O.; Salamin, K.; Fratti, M.; Monod, M. Terbinafine Resistance of Trichophyton Clinical Isolates Caused by Specific Point Mutations in the Squalene Epoxidase Gene. Antimicrob. Agents Chemother. 2017, 61, e00115-17. [Google Scholar] [CrossRef] [Green Version]
- Hiruma, J.; Noguchi, H.; Hase, M.; Tokuhisa, Y.; Shimizu, T.; Ogawa, T.; Hiruma, M.; Harada, K.; Kano, R. Epidemiological Study of Terbinafine-Resistant Dermatophytes Isolated from Japanese Patients. J. Dermatol. 2021, 48, 564–567. [Google Scholar] [CrossRef]
- Sacheli, R.; Hayette, M.-P. Antifungal Resistance in Dermatophytes: Genetic Considerations, Clinical Presentations and Alternative Therapies. J. Fungi 2021, 7, 983. [Google Scholar] [CrossRef] [PubMed]
- Singal, A. Butenafine and Superficial Mycoses: Current Status. Expert Opin. Drug Metab. Toxicol. 2008, 4, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Saple, D.G.; Amar, A.K.; Ravichandran, G.; Korde, K.M.; Desai, A. Efficacy and Safety of Butenafine in Superficial Dermatophytoses (Tinea Pedis, Tinea Cruris, Tinea Corporis). J. Indian Med. Assoc. 2001, 99, 274–275. [Google Scholar] [PubMed]
- Singal, A.; Pandhi, D.; Agrawal, S.; Das, S. Comparative Efficacy of Topical 1% Butenafine and 1% Clotrimazole in Tinea Cruris and Tinea Corporis: A Randomized, Double-Blind Trial. J. Dermatol. Treat. 2005, 16, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K. Butenafine: An Update of Its Use in Superficial Mycoses. Skin Ther. Lett. 2002, 7, 1–2, 5. [Google Scholar]
- Mingeot-Leclercq, M.P.; Gallet, X.; Flore, C.; Van Bambeke, F.; Peuvot, J.; Brasseur, R. Experimental and Conformational Analyses of Interactions between Butenafine and Lipids. Antimicrob. Agents Chemother. 2001, 45, 3347–3354. [Google Scholar] [CrossRef] [Green Version]
- Syed, T.A.; Maibach, H.I. Butenafine Hydrochloride: For the Treatment of Interdigital Tinea Pedis. Expert Opin. Pharmacother. 2000, 1, 467–473. [Google Scholar] [CrossRef]
- Maeda, T.; Takase, M.; Ishibashi, A.; Yamamoto, T.; Sasaki, K.; Arika, T.; Yokoo, M.; Amemiya, K. Synthesis and antifungal activity of butenafine hydrochloride (KP-363), a new benzylamine antifungal agent. Yakugaku Zasshi 1991, 111, 126–137. [Google Scholar] [CrossRef] [Green Version]
- Arika, T.; Yokoo, M.; Hase, T.; Maeda, T.; Amemiya, K.; Yamaguchi, H. Effects of Butenafine Hydrochloride, a New Benzylamine Derivative, on Experimental Dermatophytosis in Guinea Pigs. Antimicrob. Agents Chemother. 1990, 34, 2250–2253. [Google Scholar] [CrossRef] [Green Version]
- Porras, A.M.G.; Terra, B.S.; Braga, T.C.; Magalhães, T.F.F.; Martins, C.V.B.; da Silva, D.L.; Baltazar, L.M.; Gouveia, L.F.; de Freitas, G.J.C.; Santos, D.A.; et al. Butenafine and Analogues: An Expeditious Synthesis and Cytotoxicity and Antifungal Activities. J. Adv. Res. 2018, 14, 81–91. [Google Scholar] [CrossRef]
- Bezerra-Souza, A.; Fernandez-Garcia, R.; Rodrigues, G.F.; Bolas-Fernandez, F.; Dalastra Laurenti, M.; Passero, L.F.; Lalatsa, A.; Serrano, D.R. Repurposing Butenafine as An Oral Nanomedicine for Visceral Leishmaniasis. Pharmaceutics 2019, 11, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Guerrero, E.; Quintanilla-Cedillo, M.R.; Ruiz-Esmenjaud, J.; Arenas, R. Leishmaniasis: A Review. F1000Research 2017, 6, 750. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.W.; McLeod, R.; Rice, D.W.; Ginger, M.; Chance, M.L.; Goad, L.J. Fatty Acid and Sterol Metabolism: Potential Antimicrobial Targets in Apicomplexan and Trypanosomatid Parasitic Protozoa. Mol. Biochem. Parasitol. 2003, 126, 129–142. [Google Scholar] [CrossRef]
- Bezerra-Souza, A.; Yamamoto, E.S.; Laurenti, M.D.; Ribeiro, S.P.; Passero, L.F.D. The Antifungal Compound Butenafine Eliminates Promastigote and Amastigote Forms of Leishmania (Leishmania) Amazonensis and Leishmania (Viannia) Braziliensis. Parasitol. Int. 2016, 65, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Bezerra-Souza, A.; Jesus, J.A.; Laurenti, M.D.; Lalatsa, A.; Serrano, D.R.; Passero, L.F.D. Nanoemulsified Butenafine for Enhanced Performance against Experimental Cutaneous Leishmaniasis. J. Immunol. Res. 2021, 2021, 8828750. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Mays, R.R.; Foley, K.A. 42—Topical Antifungal Agents. In Comprehensive Dermatologic Drug Therapy, 4th ed.; Wolverton, S.E., Ed.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 480–492.e5. ISBN 978-0-323-61211-1. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Antifungal Agent | Dosage Forms | Reference |
|---|---|---|
| Allylamines | ||
| Naftifine | Cream (1–2%), gel (1–2%) | [65,66] |
| Terbinafine | Tablet (250 mg), solution (1%), cream (1%), spray (1%), gel (1%) | [65,67,68] |
| Benzylamines | ||
| Butenafine | Cream (1%) | [65,66] |
| Drug Delivery System | Characteristics | Advantages | Studied on | Reference | |
|---|---|---|---|---|---|
| Microemulsions | Clear, isotropic, thermodynamically stable dispersions Droplet diameter between 10–100 nm | Simple, lower cost, enhanced cutaneous delivery and retention Applicable for a wide range of hydrophilic and lipophilic drugs | Naftifine hydrochloride Butenafine hydrochloride | [65,75,76,77] | |
| Niosomes | Liposomes prepared with nonionic surfactants | In comparison to liposomes: lower cost, increased skin permeation, higher chemical stability, increased product’s shelf life Suitable for a wide range of drugs | Naftifine hydrochloride Terbinafine hydrochloride | [69,78,82,83] | |
| Nanoemulsions | Colloidal dispersions Droplets’ size of less than 1 µm (typically between 20–200 nm) | Transparent, high stability, increased interfacial area, enhanced drugs’ skin penetration, improved drugs’ solubility and bioavailability | Terbinafine hydrochloride | [65,84,85] | |
| Dendrimers | Polymers between 10 and 100 nm in diameter | Widely used for drug delivery and imaging applications | Terbinafine | [65,86] | |
| Lipidic Nanoparticles | Solid lipid NPs (SLNs) | First generation of lipid-based nanoparticles (NPs) Colloidal lipid carriers Particle size between 50 to 1000 nm | High biocompatibility and biodegradability, drug stability against chemical degradation, flexible and controlled release, enhanced skin penetration and retention, increased therapeutic efficacy, reduced toxicity, ease of scale-up and manufacturing Capable of incorporating hydrophilic and lipophilic drugs | Terbinafine hydrochloride | [65,73,87,88,89,92,93] |
| Nanostructured lipid carriers (NLCs) | Second generation of NPs | Overcome SLNs’ drawbacks: limited drug loading, gelation risk, drug leakage during storage | Terbinafine | [65,73,90,94] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hammoudi Halat, D.; Younes, S.; Mourad, N.; Rahal, M. Allylamines, Benzylamines, and Fungal Cell Permeability: A Review of Mechanistic Effects and Usefulness against Fungal Pathogens. Membranes 2022, 12, 1171. https://doi.org/10.3390/membranes12121171
Hammoudi Halat D, Younes S, Mourad N, Rahal M. Allylamines, Benzylamines, and Fungal Cell Permeability: A Review of Mechanistic Effects and Usefulness against Fungal Pathogens. Membranes. 2022; 12(12):1171. https://doi.org/10.3390/membranes12121171
Chicago/Turabian StyleHammoudi Halat, Dalal, Samar Younes, Nisreen Mourad, and Mohamad Rahal. 2022. "Allylamines, Benzylamines, and Fungal Cell Permeability: A Review of Mechanistic Effects and Usefulness against Fungal Pathogens" Membranes 12, no. 12: 1171. https://doi.org/10.3390/membranes12121171