
Impact of CRRT in Patients with PARDS Treated with VV-ECMO

Abstract
:1. Introduction
1.1. Fluid Balance in PARDS
1.2. Fluid Overload in ECMO
1.3. AKI in VV-ECMO
1.4. Indications for CRRT in VV-ECMO
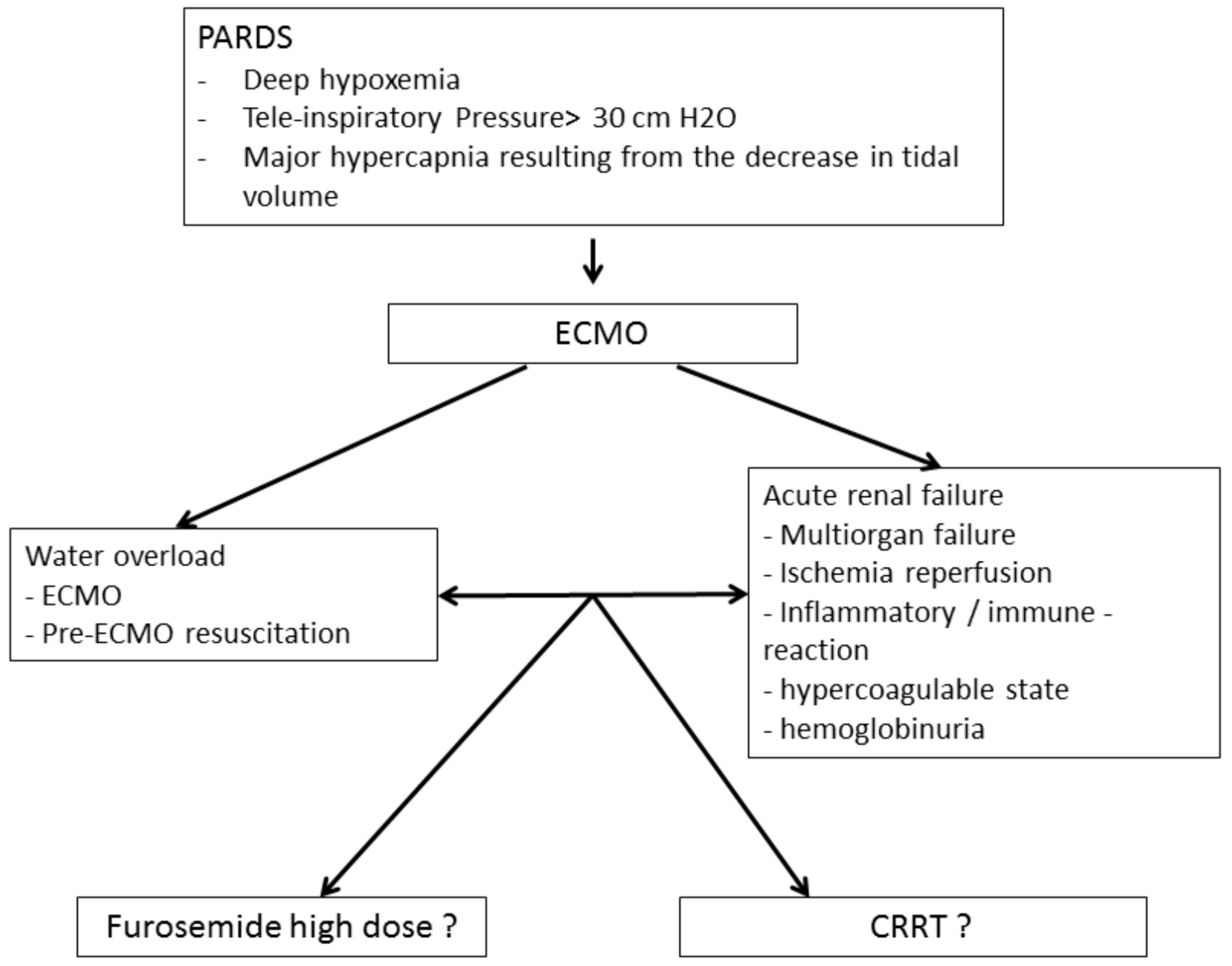
1.5. Illustrative Case
1.6. Rationale and Purpose of the Study
2. Methods
2.1. Data Collection
2.2. Definition of Severity of Illness Scores
2.3. Definition of AKI
2.4. ECMO and CRRT Technique
2.5. Endpoints
2.6. Statistical Analysis
3. Results
4. Discussion
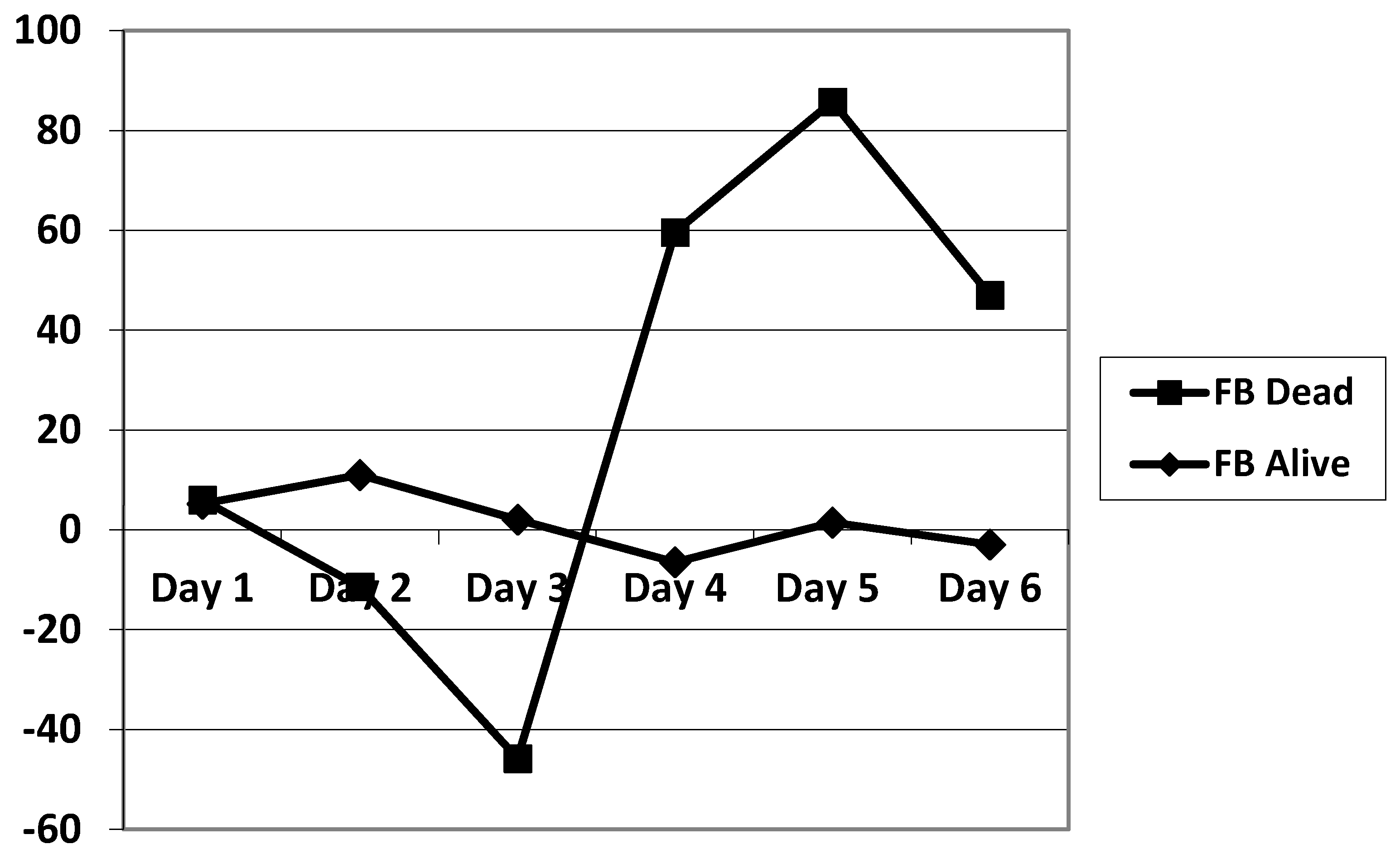
4.1. Mortality
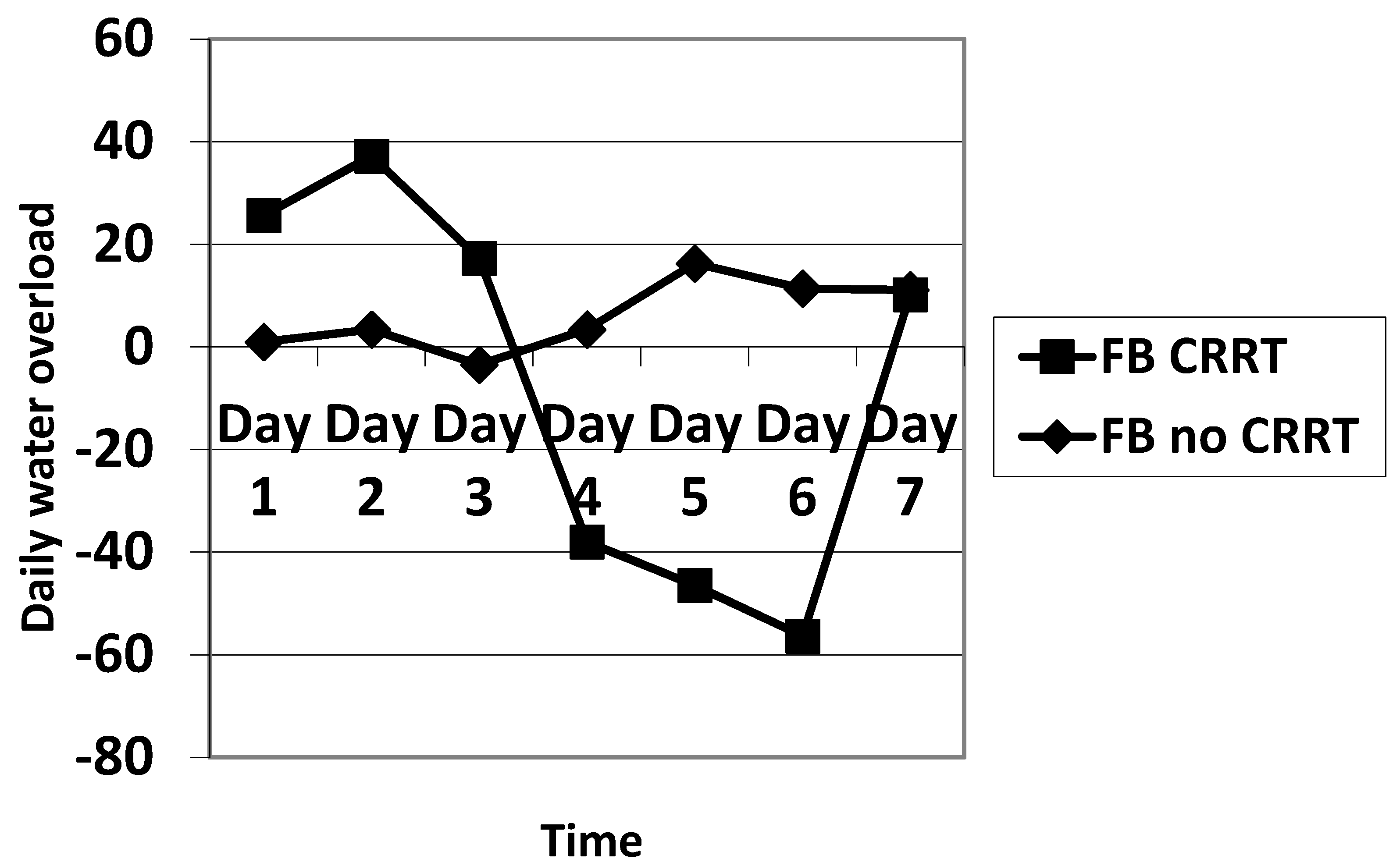
4.2. Fluid Balance and Renal Function
4.3. Consumption of Blood Products
4.4. Impact on Outcomes
4.5. Hemodynamic Instability
4.6. Pediatric Specificities of Creatinine Measurements in AKI
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zimmerman, J.J.; Akhtar, S.R.; Caldwell, E.; Rubenfeld, G.D. Incidence and outcomes of pediatric acute lung injury. Pediatrics 2009, 124, 87–95. [Google Scholar] [CrossRef]
- Khemani, R.G.; Smith, L.; Lopez-Fernandez, Y.M.; Kwok, J.; Morzov, R.; Klein, M.J.; Yehya, N.; Willson, D.; Kneyber, M.C.J.; Lillie, J.; et al. Paediatric acute respiratory distress syndrome incidence and epidemiology (PARDIE): An international, observational study. Lancet Respir. Med. 2019, 7, 115–128. [Google Scholar] [CrossRef]
- Cheifetz, I.M. Pediatric ARDS. Respir. Care 2017, 62, 718–731. [Google Scholar] [CrossRef]
- He, P.; Zhang, S.; Hu, B.; Wu, W. Retrospective study on the effects of the prognosis of patients treated with extracorporeal membrane oxygenation combined with continuous renal replacement therapy. Ann. Transl. Med. 2018, 6, 455. [Google Scholar] [CrossRef]
- Flori, H.R.; Church, G.; Liu, K.D.; Gildengorin, G.; Matthay, M.A. Positive fluid balance is associated with higher mortality and prolonged mechanical ventilation in pediatric patients with acute lung injury. Crit. Care Res. Pract. 2011, 2011, 854142. [Google Scholar] [CrossRef]
- Valentine, S.L.; Sapru, A.; Higgerson, R.A.; Spinella, P.C.; Flori, H.R.; Graham, D.A.; Brett, M.; Convery, M.; Christie, L.M.; Karamessinis, L.; et al. Fluid balance in critically ill children with acute lung injury. Crit. Care Med. 2012, 40, 2883–2889. [Google Scholar] [CrossRef] [Green Version]
- Anderson, H.L., 3rd; Coran, A.G.; Drongowski, R.A.; Ha, H.J.; Bartlett, R.H. Extracellular fluid and total body water changes in neonates undergoing extracorporeal membrane oxygenation. J. Pediatr. Surg. 1992, 27, 1003–1007, discussion 1007-1008. [Google Scholar] [CrossRef] [Green Version]
- Gbadegesin, R.; Zhao, S.; Charpie, J.; Brophy, P.D.; Smoyer, W.E.; Lin, J.J. Significance of hemolysis on extracorporeal life support after cardiac surgery in children. Pediatr. Nephrol. 2009, 24, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Selewski, D.T.; Cornell, T.T.; Lombel, R.M.; Blatt, N.B.; Han, Y.Y.; Mottes, T.; Kommareddi, M.; Kershaw, D.B.; Shanley, T.P.; Heung, M. Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med. 2011, 37, 1166–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, S.M.; Zappitelli, M.; Alexander, S.R.; Chua, A.N.; Brophy, P.D.; Bunchman, T.E.; Hackbarth, R.; Somers, M.J.; Baum, M.; Symons, J.M.; et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: The prospective pediatric continuous renal replacement therapy registry. Am. J. Kidney Dis. 2010, 55, 316–325. [Google Scholar] [CrossRef]
- Schmidt, M.; Bailey, M.; Kelly, J.; Hodgson, C.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; Bellomo, R.; Pilcher, D. Impact of fluid balance on outcome of adult patients treated with extracorporeal membrane oxygenation. Intensive Care Med. 2014, 40, 1256–1266. [Google Scholar] [CrossRef] [PubMed]
- Extracorporeal Life Support Organizatio. ELSO Guidelines for Cardiopulmonary Extracorporeal Life Support Version 1.4. Available online: https://www.elso.org/Portals/0/ELSO%20Guidelines%20General%20All%20ECLS%20Version%201_4.pdf (accessed on 7 March 2021).
- Askenazi, D.J.; Selewski, D.T.; Paden, M.L.; Cooper, D.S.; Bridges, B.C.; Zappitelli, M.; Fleming, G.M. Renal replacement therapy in critically ill patients receiving extracorporeal membrane oxygenation. Clin. J. Am. Soc. Nephrol. 2012, 7, 1328–1336. [Google Scholar] [CrossRef] [Green Version]
- Kurundkar, A.R.; Killingsworth, C.R.; McIlwain, R.B.; Timpa, J.G.; Hartman, Y.E.; He, D.; Karnatak, R.K.; Neel, M.L.; Clancy, J.P.; Anantharamaiah, G.M.; et al. Extracorporeal membrane oxygenation causes loss of intestinal epithelial barrier in the newborn piglet. Pediatr. Res. 2010, 68, 128–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mildner, R.J.; Taub, N.; Vyas, J.R.; Killer, H.M.; Firmin, R.K.; Field, D.J.; Kotecha, S. Cytokine imbalance in infants receiving extracorporeal membrane oxygenation for respiratory failure. Biol. Neonate 2005, 88, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Urlesberger, B.; Zobel, G.; Zenz, W.; Kuttnig-Haim, M.; Maurer, U.; Reiterer, F.; Riccabona, M.; Dacar, D.; Gallisti, S.; Leschnik, B.; et al. Activation of the clotting system during extracorporeal membrane oxygenation in term newborn infants. J. Pediatr. 1996, 129, 264–268. [Google Scholar] [CrossRef]
- Reed, R.C.; Rutledge, J.C. Laboratory and clinical predictors of thrombosis and hemorrhage in 29 pediatric extracorporeal membrane oxygenation nonsurvivors. Pediatr. Dev. Pathol. 2010, 13, 385–392. [Google Scholar] [CrossRef]
- Jacobs, R.; Honore, P.M.; Spapen, H.D. Intertwining extracorporeal membrane oxygenation and continuous renal replacement therapy: Sense or nonsense? Crit. Care 2015, 19, 145. [Google Scholar] [CrossRef] [Green Version]
- Betrus, C.; Remenapp, R.; Charpie, J.; Kudelka, T.; Brophy, P.; Smoyer, W.E.; Lin, J.J. Enhanced hemolysis in pediatric patients requiring extracorporeal membrane oxygenation and continuous renal replacement therapy. Ann. Thorac. Cardiovasc. Surg. 2007, 13, 378–383. [Google Scholar]
- Haneya, A.; Diez, C.; Philipp, A.; Bein, T.; Mueller, T.; Schmid, C.; Lubnow, M. Impact of Acute Kidney Injury on Outcome in Patients With Severe Acute Respiratory Failure Receiving Extracorporeal Membrane Oxygenation. Crit. Care Med. 2015, 43, 1898–1906. [Google Scholar] [CrossRef]
- Fleming, G.M.; Askenazi, D.J.; Bridges, B.C.; Cooper, D.S.; Paden, M.L.; Selewski, D.T.; Zappitelli, M. A multicenter international survey of renal supportive therapy during ECMO: The Kidney Intervention During Extracorporeal Membrane Oxygenation (KIDMO) group. ASAIO J. 2012, 58, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Antonucci, E.; Lamanna, I.; Fagnoul, D.; Vincent, J.L.; De Backer, D.; Silvio Taccone, F. The Impact of Renal Failure and Renal Replacement Therapy on Outcome During Extracorporeal Membrane Oxygenation Therapy. Artif. Organs 2016, 40, 746–754. [Google Scholar] [CrossRef]
- Bailly, D.K.; Reeder, R.W.; Zabrocki, L.A.; Hubbard, A.M.; Wilkes, J.; Bratton, S.L.; Thiagarajan, R.R.; Extracorporeal Life Support Organization Member, C. Development and Validation of a Score to Predict Mortality in Children Undergoing Extracorporeal Membrane Oxygenation for Respiratory Failure: Pediatric Pulmonary Rescue With Extracorporeal Membrane Oxygenation Prediction Score. Crit. Care Med. 2017, 45, e58–e66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- KDIGO Clinical Practice Guideline for Acute Kidney Injury. Available online: https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf (accessed on 7 March 2021).
- Hamrick, S.E.; Gremmels, D.B.; Keet, C.A.; Leonard, C.H.; Connell, J.K.; Hawgood, S.; Piecuch, R.E. Neurodevelopmental outcome of infants supported with extracorporeal membrane oxygenation after cardiac surgery. Pediatrics 2003, 111, e671–e675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolovos, N.S.; Bratton, S.L.; Moler, F.W.; Bove, E.L.; Ohye, R.G.; Bartlett, R.H.; Kulik, T.J. Outcome of pediatric patients treated with extracorporeal life support after cardiac surgery. Ann. Thorac. Surg. 2003, 76, 1435–1441, discussion 1441–1432. [Google Scholar] [CrossRef]
- Ricci, Z.; Morelli, S.; Favia, I.; Garisto, C.; Brancaccio, G.; Picardo, S. Neutrophil gelatinase-associated lipocalin levels during extracorporeal membrane oxygenation in critically ill children with congenital heart disease: Preliminary experience. Pediatr. Crit. Care Med. 2012, 13, e51–e54. [Google Scholar] [CrossRef]
- Wolf, M.J.; Chanani, N.K.; Heard, M.L.; Kanter, K.R.; Mahle, W.T. Early renal replacement therapy during pediatric cardiac extracorporeal support increases mortality. Ann. Thorac. Surg. 2013, 96, 917–922. [Google Scholar] [CrossRef]
- Aubron, C.; Cheng, A.C.; Pilcher, D.; Leong, T.; Magrin, G.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V. Factors associated with outcomes of patients on extracorporeal membrane oxygenation support: A 5-year cohort study. Crit. Care 2013, 17, R73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, S.; MacLaren, G.; Paul, E.; Best, D.; Delzoppo, C.; Butt, W. Hemofiltration is not associated with increased mortality in children receiving extracorporeal membrane oxygenation. Pediatr. Crit. Care Med. 2015, 16, 161–166. [Google Scholar] [CrossRef]
- Pottel, H.; Hoste, L.; Dubourg, L.; Ebert, N.; Schaeffner, E.; Eriksen, B.O.; Melsom, T.; Lamb, E.J.; Rule, A.D.; Turner, S.T.; et al. An estimated glomerular filtration rate equation for the full age spectrum. Nephrol. Dial. Transplant. 2016, 31, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legrand, M.; Dupuis, C.; Simon, C.; Gayat, E.; Mateo, J.; Lukaszewicz, A.C.; Payen, D. Association between systemic hemodynamics and septic acute kidney injury in critically ill patients: A retrospective observational study. Crit. Care 2013, 17, R278. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, S.; Santiago, M.J.; Gonzalez, R.; Urbano, J.; Lopez, J.; Solana, M.J.; Sanchez, A.; Del Castillo, J.; Lopez-Herce, J. Hemodynamic impact of the connection to continuous renal replacement therapy in critically ill children. Pediatr. Nephrol. 2019, 34, 163–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slessarev, M.; Salerno, F.; Ball, I.M.; McIntyre, C.W. Continuous renal replacement therapy is associated with acute cardiac stunning in critically ill patients. Hemodial. Int. 2019, 23, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Rydzewska-Rosolowska, A.; Gozdzikiewicz-Lapinska, J.; Borawski, J.; Koc-Zorawska, E.; Mysliwiec, M.; Naumnik, B. Unexpected and striking effect of heparin-free dialysis on cytokine release. Int. Urol. Nephrol. 2017, 49, 1447–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeney, V. Pro-Inflammatory Actions of Red Blood Cell-Derived DAMPs. In Experientia Supplementum; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; pp. 211–233. [Google Scholar] [CrossRef]
- Burnstock, G. Purinergic Signaling in the Cardiovascular System. Circ. Res. 2017, 120, 207–228. [Google Scholar] [CrossRef] [Green Version]
- Askenazi, D.J.; Ambalavanan, N.; Hamilton, K.; Cutter, G.; Laney, D.; Kaslow, R.; Georgeson, K.; Barnhart, D.C.; Dimmitt, R.A. Acute kidney injury and renal replacement therapy independently predict mortality in neonatal and pediatric noncardiac patients on extracorporeal membrane oxygenation. Pediatr. Crit. Care Med. 2011, 12, e1–e6. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 45) | No CRRT (n = 37) | CRRT (n = 8) | p-Value | |
|---|---|---|---|---|
| Age, months | 3.5 [0.0–18.2] | 1 [0.0–16.5] | 6.5 [0.7–46.2] | 0.3 |
| Weight, kg | 4.7 [3.6–9.8] | 4.7 [3.6–8.7] | 5.8 [3.5–16.2] | 0.63 |
| Male, n (%) | 23 (51) | 21 (56) | 5 (62.5) | 0.45 |
| Pneumonia, n (%) | 22 (48) | 21 (56) | 5 (62.5) | 0.9 |
| Sepsis, n (%) | 6 (13) | 5 (13) | 1 (12) | 0.98 |
| Inhalation, n (%) | 17 (37) | 15 (42) | 2 (25) | 0.69 |
| Scores | ||||
| PIM | 8.0 [1.3–15.8] | 8.0 [2.3–15.8] | 2.9 [0.7–28.7] | 0.25 |
| PRISM | 22.6 ± 13.1 | 22.6 ± 12.8 | 22.2 ± 15.7 | 0.71 |
| PRISM Predicted mortality (%) | 55.2 [18–88.9] | 59.6 [20–88.5] | 17.6 [4.1–98.4] | 0.69 |
| PELOD | 10 [6.0–12.5] | 9.5 [5.7–11.7] | 11 [10–18] | 0.15 |
| PELOD (non- renal) | 10 [6.0–12.5] | 9.5 [5.7–11.7] | 11 [10–18] | 0.23 |
| PELOD Predicted mortality (%) | 10.7 [1.4–19.2] | 8.5 [1.4–19.2] | 14.5 [3.9–27.5] | 0.24 |
| P-PREP | 6.0 [4.0–10] | 7 [4.5–10] | 5.5 [3.2–9.5] | 0.87 |
| P-PREP (non- renal) | 0.5 [−2–2.7] | 0.5 [−1.75–2.0] | 1 [−2–3.75] | 0.8 |
| LIS | 3.3 [3.0–3.7] | 3.3 [3–3.7] | 3.2 [2.6–3.6] | 0.7 |
| VIS max | 30 [7.7–60.5] | 21.6 [6.9–54.6] | 44.5 [29.2–94.5] | 0.042 |
| Creatinine max mg/dl | 0.7 ± 0.4 | 0.6 ± 0.3 | 1.1 ± 0.6 | 0.0032 |
| Clearance min, ml/min | 39 [25–63] | 46 [27–66] | 28 [21–31] | 0.11 |
| Fluid balance max, ml/kg | 139 [35–264] | 133 [20–264] | 155 [103–345] | 0.35 |
| Lactate max, mg/dl | 3.46 [2.0–6.0] | 3.34 [1.9–6.0] | 4.2 [2.5–6.8] | 0.24 |
| Pre-ECMO pH | 7.16 [7.09–7.30] | 7.17 [7.10–7.30] | 7.13 [7.06–7.39] | 0.62 |
| Treatment | ||||
| NA, mg/kg | 0.0 [0.02–0.28] | 0.0 [0.0–0.21] | 0.43 [0.0–1.0] | 0.0033 |
| Furosemide, mg/kg | 21.7 [4.9–56.2] | 20.3 [4.0–56.2] | 39.0 [7.2–92.6] | 0.33 |
| NO, n (%) | 33 (73) | 27 (72.9) | 6 (75) | 0.83 |
| Corticoids, n (%) | 12 (27) | 8 (21) | 4 (50) | 0.17 |
| Ig, n (%) | 5 (11) | 5 (13) | 0 (0) | 0.56 |
| NMBA, n (%) | 40 (88) | 33 (94) | 7 (87) | 0.98 |
| ECMO, duration, h | 126 [92–177] | 121 [90–175] | 159 [111–271] | 0.15 |
| ICU LOS, d | 15 [9.7–26.0] | 13.5 [9.7–20.2] | 24.0 [10.7–71.0] | 0.16 |
| ICU mortality, n (%) | 9 (20) | 7 (18) | 3 (37) | 0.71 |
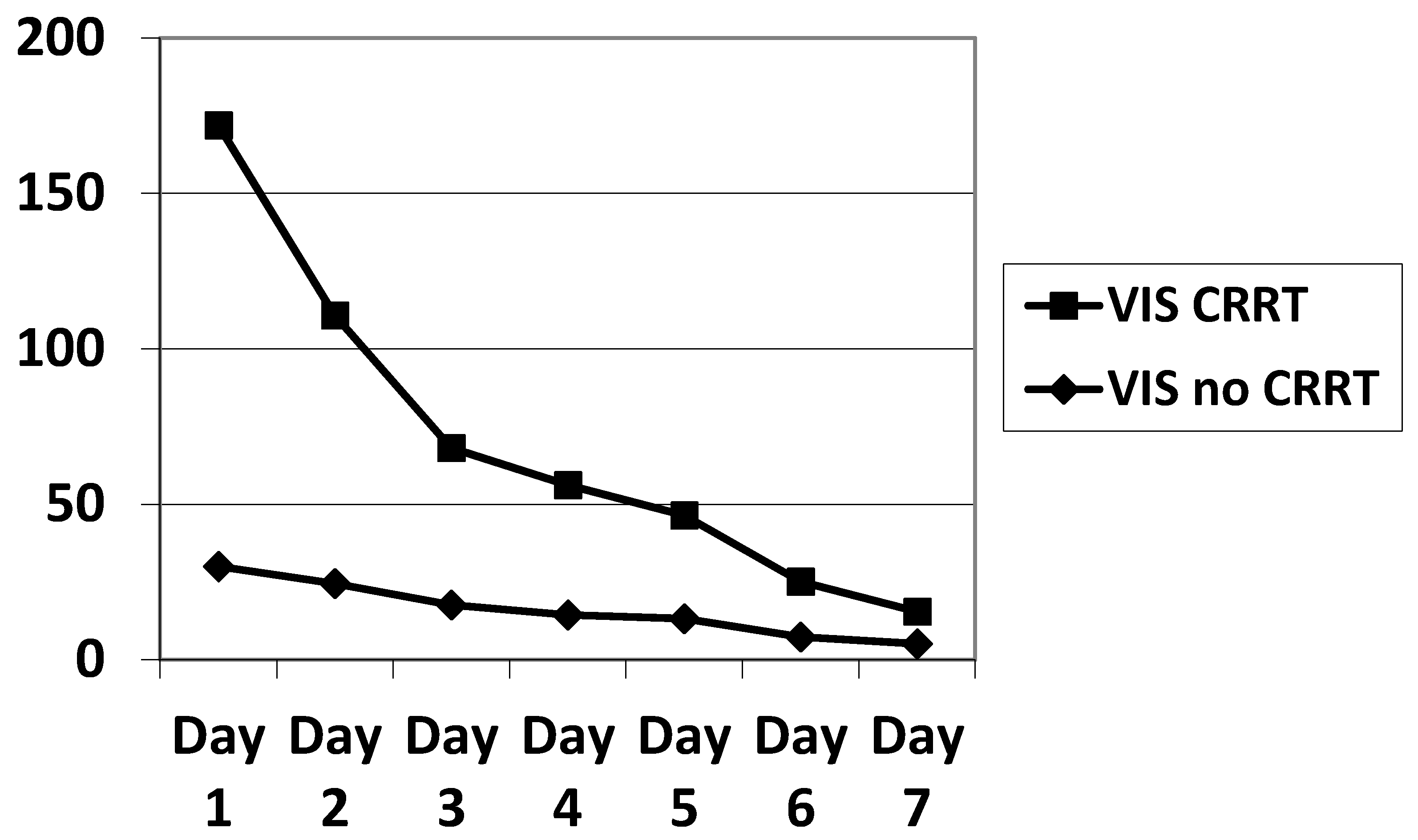
| VIS no CRRT | VIS CRRT | p | |
|---|---|---|---|
| Day 1 | 20 [0–117] | 65 [14–379] | 0.0003 |
| Day 2 | 10 [0–107] | 92.5 [7–167] | 0.0035 |
| Day 3 | 7.2 [0–93] | 37 [0–107] | 0.0231 |
| Day 4 | 10 [0–75] | 20 [3–104] | 0.0671 |
| Day 5 | 4 [0–87] | 15 [0–102] | 0.0898 |
| Day 6 | 0 [0–116] | 7.5 [0–63] | 0.0477 |
| Day 7 | 0 [0–76] | 5 [0–33] | 0.1284 |
| No CRRT | CRRT | p | |
|---|---|---|---|
| OSI | 11.1 [3.2–26.3] | 17.4 [7.8–24.3] | 0.0663 |
| Tidal Volume, mL/kg | 3.7 [1–14] | 4.9 [1.8–8.7] | 0.6706 |
| PEEP, cm H2O | 8.5 [2–16] | 9 [5–12] | 0.9551 |
| Plateau, cm H2O | 25.5 [15–40] | 30 [24–32] | 0.0721 |
| Driving pressure, cm H2O | 16 [4–30] | 17.5 [0–25] | 0.5742 |
| P/V, cm H2O/L | 6.75 [2–18] | 6 [3.4–13.3] | 0.9921 |
| Compliance mL/cm H2O | 1.12 [0.3–31.8] | 2.1 [0.2–4.5] | 0.7915 |
| Control (n = 16) | CRRT (n = 8) | p-Value | |
|---|---|---|---|
| Age, months | 0.0 [0.0–16.5] | 6.5 [0.7–46.2] | 0.21 |
| Weight, kg | 3.9 [3.4–10.0] | 5.8 [3.5–16.2] | 0.44 |
| Male, n (%) | 9 (56) | 5 (62.5) | 0.66 |
| Pneumonia, n (%) | 5 (31) | 5 (62.5) | 0.65 |
| Sepsis, n (%) | 3 (18) | 1 (12) | >0.99 |
| Inhalation, n (%) | 7 (43) | 2 (25) | 0.65 |
| Scores | |||
| PIM | 12.8 [3.8–32.4] | 2.9 [0.7–28.7] | 0.13 |
| PRISM | 27.0 ± 10.5 | 22.2 ± 15.7 | 0.4 |
| PRISM Predicted mortality (%) | 45.2 ± 33.7 | 36.4 ± 43.5 | 0.61 |
| PELOD | 10.5 [7.5–20.0] | 11 [10–18] | 0.15 |
| PELOD Predicted mortality (%) | 14.5 [4.7–19.2] | 14.5 [3.9–27.5] | 0.61 |
| P-PREP | 7.8 ± 2.9 | 5.7 ± 4.3 | 0.17 |
| P-PREP (non- renal) | 0.6 ± 2.8 | 0.75 ± 2.8 | 0.95 |
| LIS | 3.4 [3.0–3.9] | 3.2 [2.6–3.6] | 0.55 |
| VIS max | 16.3 [6.7–34.0] | 44.5 [29.2–94.5] | 0.01 |
| Creatinine max mg/dl | 0.8 ± 0.3 | 1.1 ± 0.6 | 0.17 |
| Clearance min, ml/min | 32 [18-64] | 28 [21–31] | 0.7 |
| Fluid balance max, ml/kg | 71 [12–258] | 155 [103–345] | 0.23 |
| Lactate max, mg/dl | 4.0 [2.7–6.0] | 4.2 [2.5–6.8] | 0.78 |
| Pre-ECMO pH | 7.18 ± 0.15 | 7.18 ± 0.19 | 0.79 |
| Treatment | |||
| NA, mg/kg | 0.0 [0.0–0.17] | 0.43 [0.0–1.0] | 0.005 |
| Furosemide, mg/kg | 26.5 [5.2–44.2] | 39.0 [7.2–92.6] | 0.37 |
| ECMO, duration, h | 105 [−302] | 159 [111–271] | 0.37 |
| ICU LOS, d | 15 [10.0–33.2] | 24.0 [10.7–71.0] | 0.42 |
| ICU mortality, n (%) | 4 (25) | 3 (37) | 0.64 |
| No CRRT | CRRT | p | |
|---|---|---|---|
| RBC, mL/kg | 39 [26–62] | 114 [76–174] | 0.0005 |
| RBC, mL/kg after CRRT | 35 [17–54] | 74 [45–160] | 0.015 |
| PLT, mL/kg | 20 [8–43] | 83 [68–152] | 0.0002 |
| PLT mL/kg after CRRT | 13 [0–36] | 55 [16–145] | 0.0014 |
| FFP, mL/kg | 0 [0–10] | 36 [6–53] | 0.0025 |
| FFP, mL/kg after CRRT | 0 [0–0.8] | 17 [0–35] | 0.0303 |
| All (n = 45) | Survivors (n = 35) | Non-Survivors (n = 10) | p-Value | |
|---|---|---|---|---|
| Age, months | 3.5 [0.0–18.2] | 2 [0.0–18.7] | 4.5 [0.7–46.2] | 0.56 |
| Weight, kg | 4.7 [3.6–9.8] | 4.2 [3.5–9.4] | 5.0 [3.9–10.8] | 0.38 |
| Male, n (%) | 26 (57) | 20 (57) | 6 (60) | 0.72 |
| Pneumonia, n (%) | 22 (50) | 16 (55) | 6 (60) | 0.48 |
| Sepsis, n (%) | 6 (13) | 2 (5) | 4 (40) | 0.01 |
| Inhalation, n (%) | 17 (37) | 17 (48) | 0 (0) | 0.007 |
| Scores | ||||
| PIM | 8.0 [1.3–15.8] | 10 [2.8–22.7] | 2.7 [0.8–7.6] | 0.01 |
| PRISM | 22.6 ± 13.1 | 23.9 ± 13.9 | 17.3 ± 8.4 | 0.18 |
| PRISM Predicted mortality (%) | 55.2 [18–88.9] | 58.0 [19–91.1] | 17.8 [6.9–75.3] | 0.16 |
| PELOD | 10 [6.0–12.5] | 9.5 [6.0–11.0] | 13 [8.7–20] | 0.06 |
| PELOD (non- renal) | 10 [6.0–12.5] | 9.5 [6.0–11.0] | 13 [8.7–20] | 0.06 |
| PELOD Predicted mortality (%) | 10.7 [1.4–19.2] | 8.5 [1.3–18.4] | 16.2 [10–32] | 0.06 |
| P-PREP | 6.0 [4.0–10] | 6 [2.0–8.0] | 10 [5.5–11] | 0.02 |
| P-PREP (non- renal) | 0.5 [−2–2.7] | −1 [−2.0–2.0] | 3 [2.0–4.0] | <0.0001 |
| LIS | 3.3 [3.0–3.7] | 3.3 [3.0–3.7] | 3.1 [2.3–3.7] | 0.32 |
| VIS max | 30 [7.7–60.5] | 30 [10–79] | 29 [5.0–57] | 0.62 |
| Creatinine max mg/dl | 0.7 ± 0.4 | 0.75 ± 0.36 | 0.76 ±0.65 | 0.52 |
| Clearance min, ml/min | 39 [25–63] | 39 [26–62] | 43 [21–71] | 0.91 |
| Fluid balance max, ml/kg | 139 [35–264] | 133 [28–244] | 139 [36–377] | 0.58 |
| Lactate max, mg/dl | 3.46 [2.0–6.0] | 4.0 [2.0–6.2] | 2.3 [1.6–3.1] | 0.03 |
| Pre-ECMO pH | 7.16 [7.09–7.30] | 7.16 [7.10–7.30] | 7.20 [7.07–7.28] | 0.62 |
| Treatment | ||||
| CVVH, n (%) | 8 (17) | 5 (11) | 3 (30) | 0.34 |
| NA, mg/kg | 0.02 [0.00–0.28] | 0.01 [0.0–0.21] | 0.22 [0.0–0.8] | 0.47 |
| Furosemide, mg/kg | 21.7 [4.9–56.2] | 21.2 [5.0–58.0] | 18.8 [1.8–57.46] | 0.64 |
| ECMO, duration, h | 126 [92–177] | 126 [99–177] | 107 [41–232] | 0.46 |
| ICU LOS, d | 15 [9.7–26.0] | 15 [9.2–27.5] | 16 [10.0–27.2] | 0.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redant, S.; Barbance, O.; Tolwani, A.; Beretta-Piccoli, X.; Massaut, J.; De Bels, D.; Taccone, F.S.; Honoré, P.M.; Biarent, D. Impact of CRRT in Patients with PARDS Treated with VV-ECMO. Membranes 2021, 11, 195. https://doi.org/10.3390/membranes11030195
Redant S, Barbance O, Tolwani A, Beretta-Piccoli X, Massaut J, De Bels D, Taccone FS, Honoré PM, Biarent D. Impact of CRRT in Patients with PARDS Treated with VV-ECMO. Membranes. 2021; 11(3):195. https://doi.org/10.3390/membranes11030195
Chicago/Turabian StyleRedant, Sébastien, Océane Barbance, Ashita Tolwani, Xavier Beretta-Piccoli, Jacques Massaut, David De Bels, Fabio S. Taccone, Patrick M. Honoré, and Dominique Biarent. 2021. "Impact of CRRT in Patients with PARDS Treated with VV-ECMO" Membranes 11, no. 3: 195. https://doi.org/10.3390/membranes11030195