
Chronic Inflammatory Demyelinating Polyneuropathy after ChAdOx1 nCoV-19 Vaccination

Abstract
:1. Introduction
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, B.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Oxford COVID Vaccine Trial Group. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Pavord, S.; Scully, M.; Hunt, B.J.; Lester, W.; Bagot, C.; Craven, B.; Rampotas, A.; Ambler, G.; Makris, M. Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis. N. Engl. J. Med. 2021, 385, 1680–1689. [Google Scholar] [CrossRef] [PubMed]
- Lunn, M.P.; Cornblath, D.R.; Jacobs, B.C.; Querol, L.; van Doorn, P.A.; Hughes, R.A.; Willison, H.J. COVID-19 vaccine and Guillain-Barré syndrome: Let’s not leap to associations. Brain 2021, 144, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Esposito, S. Vaccine-preventable diseases, vaccines and Guillain-Barre’ syndrome. Vaccine 2019, 37, 5544–5550. [Google Scholar] [CrossRef] [PubMed]
- Shui, I.M.; Rett, M.D.; Weintraub, E.; Marcy, M.; Amato, A.A.; Sheikh, S.I.; Ho, D.; Lee, G.M.; Yih, W.K. Vaccine Safety Datalink Research Team. Guillain-Barré syndrome incidence in a large United States cohort (2000–2009). Neuroepidemiology 2012, 39, 109–115. [Google Scholar] [CrossRef]
- Wakerley, B.R.; Uncini, A.; Yuki, N. GBS Classification Group; GBS Classification Group. Guillain-Barré and Miller Fisher syndromes--new diagnostic classification. Nat. Rev. Neurol. 2014, 10, 537–544. [Google Scholar] [CrossRef]
- Ruts, L.; Drenthen, J.; Jacobs, B.C.; Van Doorn, P.A. Dutch GBS Study Group. Distinguishing acute-onset CIDP from fluctuating Guillain-Barre syndrome: A prospective study. Neurology 2010, 74, 1680–1686. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.M.; Ramsamy, S.; Tarr, A.W.; Tighe, P.J.; Irving, W.L.; Tanasescu, R.; Evans, J.R. Guillain-Barré Syndrome Variant Occurring after SARS-CoV-2 Vaccination. Ann. Neurol. 2021, 90, 315–318. [Google Scholar] [CrossRef]
- Maramattom, B.V.; Krishnan, P.; Paul, R.; Padmanabhan, S.; Cherukudal Vishnu Nampoothiri, S.; Syed, A.A.; Mangat, H.S. Guillain-Barré Syndrome following ChAdOx1-S/nCoV-19 Vaccine. Ann. Neurol. 2021, 90, 312–314. [Google Scholar] [CrossRef]
- Bonifacio, G.B.; Patel, D.; Cook, S.; Purcaru, E.; Couzins, M.; Domjan, J.; Ryan, S.; Alareed, A.; Tuohy, O.; Slaght, S.; et al. Bilateral facial weakness with paraesthesia variant of Guillain-Barré syndrome following Vaxzevria COVID-19 vaccine. J. Neurol. Neurosurg. Psychiatry 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- McKean, N.; Chircop, C. Guillain-Barré syndrome after COVID-19 vaccination. BMJ Case Rep. 2021, 14, e244125. [Google Scholar] [CrossRef] [PubMed]
- Nasuelli, N.A.; De Marchi, F.; Cecchin, M.; De Paoli, I.; Onorato, S.; Pettinaroli, R.; Savoini, G.; Godi, L. A case of acute demyelinating polyradiculoneuropathy with bilateral facial palsy after ChAdOx1 nCoV-19 vaccine. Neurol. Sci. 2021, 17, 4747–4749. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, P.Y.K.; van Doorn, P.A.; Hadden, R.D.M.; Avau, B.; Vankrunkelsven, P.; Allen, J.A.; Attarian, S.; Blomkwist-Markens, P.H.; Cornblath, D.R.; Eftimov, F.; et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint Task Force-Second revision. Eur. J. Neurol. 2021. [Google Scholar] [CrossRef]
- Pegat, A.; Vogrig, A.; Khouri, C.; Masmoudi, K.; Vial, T.; Bernard, E. Adenovirus COVID-19 vaccines and Guillain-Barré syndrome with facial paralysis. Ann. Neurol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Oo, W.M.; Giri, P.; de Souza, A. AstraZeneca COVID-19 vaccine and Guillain- Barré Syndrome in Tasmania: A causal link? J. Neuroimmunol. 2021, 360, 577719. [Google Scholar] [CrossRef]
- Mathew, T.; Hareesh, P.; Souza, D.D.; Avati, A.; Sarma, G.R.K.; Nadig, R.; Therambil, M.; Parry, G.J. Bell’s palsy and guillain-barré syndrome may be 2 ends of the same spectrum. Muscle Nerve. 2019, 59, E48–E49. [Google Scholar] [CrossRef]
- Leonhard, S.E.; Mandarakas, M.R.; Gondim, F.A.A.; Bateman, K.; Ferreira, M.L.; Cornblath, D.R.; van Doorn, P.A.; Dourado, M.E.; Hughes, R.A.C.; Islam, B.; et al. Diagnosis and management of Guillain-Barré syndrome in ten steps. Nat. Rev. Neurol. 2019, 15, 671–683. [Google Scholar] [CrossRef]
- Pascual-Goñi, E.; Martín-Aguilar, L.; Querol, L. Autoantibodies in chronic inflammatory demyelinating polyradiculoneuropathy. Curr. Opin. Neurol. 2019, 32, 651–657. [Google Scholar] [CrossRef]
- Doneddu, P.E.; Bianchi, E.; Cocito, D.; Manganelli, F.; Fazio, R.; Filosto, M.; Mazzeo, G.; Cosentino, A.; Cortese, S.; Jann, A.M.; et al. Italian CIDP Database Study Group. Risk factors for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP): Antecedent events, lifestyle and dietary habits. Data from the Italian CIDP Database. Eur. J. Neurol. 2020, 27, 136–143. [Google Scholar] [CrossRef]
- Gable, K.L.; Afshari, Z.; Sufit, R.L.; Allen, J.A. Distal acquired demyelinating symmetric neuropathy after vaccination. J. Clin. Neuromuscul. Dis. 2013, 14, 117–122. [Google Scholar] [CrossRef]
- Fantini, J.; Di Scala, C.; Chahinian, H.; Yahi, N. Structural and molecular modelling studies reveal a new mechanism of action of chloroquine and hydroxychloroquine against SARS-CoV-2 infection. Int. J. Antimicrob. Agents 2020, 55, 105960. [Google Scholar] [CrossRef] [PubMed]
- Juliao Caamaño, D.S.; Alonso Beato, R. Facial diplegia, a possible atypical variant of Guillain-Barré Syndrome as a rare neurological complication of SARS-CoV-2. J. Clin. Neurosci. 2020, 77, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Palaiodimou, L.; Stefanou, M.I.; Katsanos, A.H.; Fragkou, P.C.; Papadopoulou, M.; Moschovos, C.; Michopoulos, L.; Kokotis, P.; Bakirtzis, C.; Naska, A.; et al. Prevalence, clinical characteristics and outcomes of Guillain-Barré syndrome spectrum associated with COVID-19: A systematic review and meta-analysis. Eur. J. Neurol. 2021, 28, 3517–3529. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age/Sex (Authors) | Symptoms/Signs | Respiratory Failure | Days from First Dose of Vaccine | CSF Findings | EMG Findings | MRI | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| 54/M [8] | Ascending distal limbs dysesthesias; bifacial paresis | None | 16 | P: 163 mg/dL; C: 19/mL | Day 16: Facial NCS showed severely reduced compound muscle action potential amplitude responses and normal terminal latencies bilaterally; sensory and motor NCS: normal | Enhancement of facial nerves | Prednisolone 60 mg/day × 5 days | Stabilized |
| 20/M [8] | Headache, LL dysesthesias, and bifacial paresis | None | 26 | P: 123 mg/dL; C: 14/mL | Day 13: Facial NCS showed borderline normal amplitude responses and normal terminal latencies bilaterally; sensory and motor NCS: normal | Normal non-contrast brain MRI | Prednisolone 60 mg/day × 5 days | Stabilized |
| 57/M [8] | Lumbar back pain, dysarthria and bifacial paresis; lower limb dysesthesias; proximal limb weakness on exam | None | 21 | P: 247 mg/dL; C: 8/mL | Day 13: Facial NCS, not performed; sensory and motor NCS: normal | Normal non-contrast brain MRI | IVIg | Stabilized |
| 55/M [8] | LL paresthesias; bifacial paresis | None | 29 | P: 89 mg/dL; C: <5/mL | NA | Enhancement of facial nerves | None | Subjective improvement of numbness |
| 43/F [9] | Bifacial paresis, areflexic quadriparesis, upper back pain | Yes | 10 | P: 72.2 mg/dL C: 5/mL | Demyelinating neuropathy | NA | IVIg IMV | Recovered |
| 67/F [9] | Bifacial paresis, right abducense palsy, bulbar palsy, Distal sensory impairment in the legs, areflexia, limb weakness | Yes | 14 | P: 345 mg/dL C: 3/mL | Axonal motor-sensory neuropathy | Normal brain and spine MRI | IVIg IMV PLEX | Still hospitalized |
| 53/F [9] | Bilateral LL numbness, weakness, right-sided facial, tongue numbness, and back pain, right trigeminal V2-V3 sensory impairment, areflexia | Yes | 12 | P: 120 mg/dL C: 3/mL | Demyelinating neuropathy | Normal brain and spine MRI | IVIg IMV | Still hospitalized |
| 68/F [9] | Facial diplegia, bulbar palsy, bilateral facial numbness, bilateral distal lower and UL numbness, and bilaterally trigeminal sensory loss, areflexia | Yes | 14 | P: 75 mg/dL C: 4/mL | Demyelinating neuropathy | Normal brain and spine MRI | IVIg IMV | Still hospitalized |
| 70/M [9] | Facial diplegia, bulbar palsy. Bilateral distal UL and LL numbness, areflexia | Yes | 11 | P: NA C: NA | Demyelinating neuropathy | NA | IVIg IMV | Still hospitalized |
| 69/F [9] | Facial diplegia, bulbar palsy, complete ophthalmoplegia, UL and LL distal numbness, UL and LL weakness, areflexia | Yes | 12 | P: NA C: NA | Demyelinating neuropathy | NA | IVIg PLEX | Still hospitalized |
| 69/F [9] | Facial diplegia, bulbar palsy, bilateral UL and LL numbness, areflexia | None | 13 | P: 83 mg/dL C: 2/mL | Demyelinating neuropathy | NA | IVIg IMV | Still hospitalized |
| 66/M [10] | Bilateral facial weakness with numbness of the tongue and mouth, interscapular back and LL pain, paresthesia of both hands and feet Normal tone, power and reflexes in both UL and LL, except absent right ankle jerk. Reduced light touch and pinprick sensation symmetrically in LL to the knee and vibration to the ankles. Gait was ataxic | None | 7 | P: 1.99 g/L C: 2/mL | Sensory NCS: UL and LL: reduced SNAP amplitude Motor NCS: UL and LL: Prolonged DMLs, and F-wave latencies Slow CV Dispersed CMAPs and CB. Facial NCS: Prolonged DMLs | MRI pre and post GAD contrast: normal except for bilateral smooth contrast enhancement along whole facial nerve | IVIg | Facial weakness resolved Pain and paresthesia improving. Intact reflexes including right ankle jerk |
| 43/M [10] | Severe bilateral facial weakness, Myalgia, paresthesia of both hands and feet, severe neck pain, urinary retention, dysphagia, altered taste and paresthesia of tongue Normal limb tone, with full power except mild weakness in right hip flexion. Reflexes initially present but then subsequently lost. Flexor plantar responses. Patchy, asymmetrical glove and stocking reduction in pinprick sensation and a sensory ataxia | None | 11 | P: 2.81 g/L C: 23/mL | Sensory NCS: UL: absent SNAPs LL: normal Motor NCS: UL and LL: Prolonged DMLs, and F-wave latencies Slow CV Dispersed CMAPs and CB Facial NCS: Absent. Facial EMG: Few fibrillations, no volitional motor units | MRI pre and post GAD contrast: normal except for bilateral smooth contrast enhancement along whole facial nerve | IVIg | 20% improvement in facial weakness. Ataxic gait and pain static. Areflexia persists. No longer in urinary retention |
| 51/M [10] | 3-week history of severe LL cramping pain. Numbness in feet and hands, spreading proximally to the ankles. Progressive right facial weakness became severe and bilateral after 5 days. Tone, power, and reflexes in limbs were normal. Impaired sensation in all modalities in UL and LL with a sensory ataxia | None | 7 | P: 5.14 g/L C: 1/mL | Sensory NCS: UL: reduced SNAP amplitudes LL: normal Motor NCS: UL and LL: Dispersed CMAPs Tibial F wave latencies prolonged Facial NCS: Normal except blink reflexes absent Facial EMG: Very reduced volitional motor units | MRI pre and post GAD contrast: normal except for bilateral smooth contrast enhancement along whole facial nerve | None | 95% improvement in facial weakness. Ataxic gait 80% better. 25% improvement in pain and paresthesia |
| 71/F [10] | Lower back and abdominal pain. Altered taste and sequential facial weakness within 24 h. Mild proximal LL weakness. Slight weakness in hip flexion bilaterally. Absent knee and left ankle reflexes with normal sensory examination | None | 12 | P: 0.96 g/L C: 1/mL | Sensory NCS: UL and LL: reduced/absent SNAP amplitudes and velocities Motor NCS: UL and LL: Prolonged DMLs Dispersed CMAPs Facial NCS: Not tested Facial EMG: Not tested | Normal MRI. NO post contrast study. Normal CT performed | None | Residual mild facial weakness, proximal leg weakness and mild paresthesia. Reflexes regained |
| 53/M [10] | Lower back discomfort and radicular pain. Facial, perioral and LL paresthesia progressing to severe simultaneous bilateral facial weakness. Depressed UL reflexes. Normal LL reflexes. Mild distal LL sensory loss to vibration and pinprick | None | 8 | P: 1.22 g/L C: 0/mL | Sensory NCS: Not tested Motor NCS: Not tested Facial NCS: Not tested Facial EMG: Not tested | Normal MRI. NO post contrast study. Normal CT performed | None | 95% resolution of facial weakness, pain and paresthesia |
| 48/M [11] | Severe back pain. Bilateral facial weakness | None | 10 | P: (1264 mg/L C: 8 × 10 × 6 /L lymphocytes | Severe, multifocal sensorimotor demyelinating polyneuropathy, with reduced compound motor action potentials, reflecting likely hypoexcitability | Normal CT and MRI of the brain | IVIgs Oral Prednisolone | Rapid improvement following the treatment |
| 59/M [12] | Four limb distal paresthesia and postural instability. Bilateral facial palsy (House–Brackmann grade V). Gait ataxia, global areflexia, and distal paresthesia both at the LL and UL; Normal pallesthesia. Segmental strength diffusely preserved (MRC: 5/5). No spine sensory level. No vegetative, or sphincter involvement | None | 10 | P: 140 mg/dL C: normal white blood cell count | Motor polyradiculoneuropathy with temporal dispersion of the tibial nerve cMAP bilaterally, with F reflex absent in all districts. No sensory involvement, particularly no temporal dispersion of the sural nerve SNAP bilaterally | Unremarkable brain and cervical MRI with gadolinium | IVIg | Slowly improved |
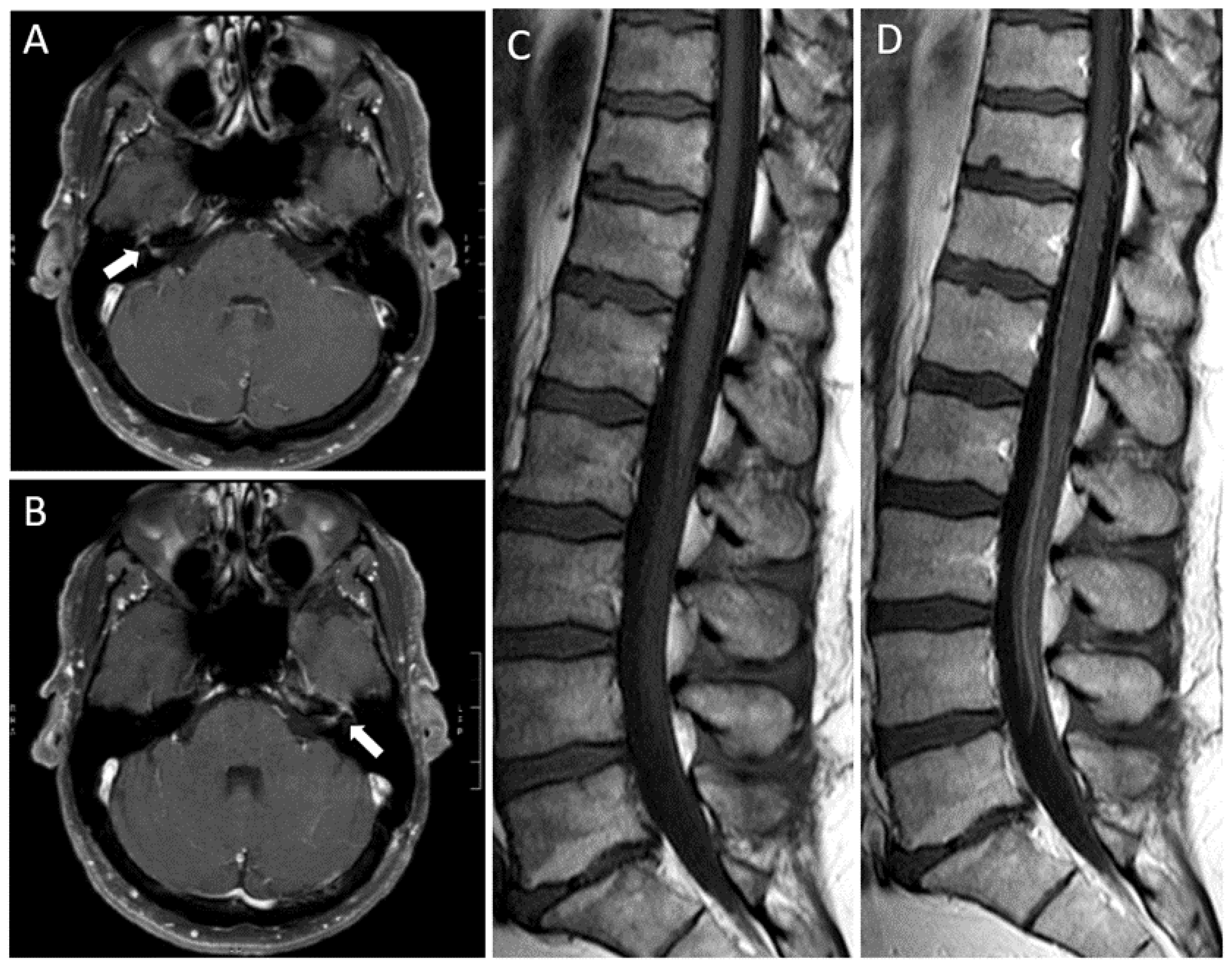
| 49/M (Present case report) | Headache, bifacial paresis and paresthesias; lower limbs areflexia, lumbar back pain | None | 16 | P: 110 mg/dL C: <5/mL | First admission: Blink reflex: absence of all potentials (R1i, R2i, R2c) with right-sided stimulation and normal findings after left supraorbital stimulation. NCS: absence of demyelinating/axonal neuropathy at upper and lower extremities Second admission: Blink reflex: delay of R1i, R2i after stimulation of left side and R2c delay with right supraorbital stimulation. Absence of R1i and R2i after right stimulation and absence of R2c with left-sided stimulation. NCS: demyelinating sensorimotor polyneuropathy at upper and lower extremities | Enhancement of facial nerves and cauda equina | IVIg | Progressed to CIDP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagella, C.F.; Corda, D.G.; Zara, P.; Elia, A.E.; Ruiu, E.; Sechi, E.; Solla, P. Chronic Inflammatory Demyelinating Polyneuropathy after ChAdOx1 nCoV-19 Vaccination. Vaccines 2021, 9, 1502. https://doi.org/10.3390/vaccines9121502
Bagella CF, Corda DG, Zara P, Elia AE, Ruiu E, Sechi E, Solla P. Chronic Inflammatory Demyelinating Polyneuropathy after ChAdOx1 nCoV-19 Vaccination. Vaccines. 2021; 9(12):1502. https://doi.org/10.3390/vaccines9121502
Chicago/Turabian StyleBagella, Caterina Francesca, Davide G. Corda, Pietro Zara, Antonio Emanuele Elia, Elisa Ruiu, Elia Sechi, and Paolo Solla. 2021. "Chronic Inflammatory Demyelinating Polyneuropathy after ChAdOx1 nCoV-19 Vaccination" Vaccines 9, no. 12: 1502. https://doi.org/10.3390/vaccines9121502