
Local and Systemic Adverse Reactions to mRNA COVID-19 Vaccines Comparing Two Vaccine Types and Occurrence of Previous COVID-19 Infection

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 10 May 2021).
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers: A Living Rapid Review. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Coronavirus Disease 2019 (COVID-19) in the EU/EEA and the UK—Eighth Update. 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-rapid-risk-assessment-coronavirus-disease-2019-eighth-update-8-april-2020.pdf (accessed on 10 May 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Comirnaty, COVID-19 MRNA Vaccine Product Information; European Medicines Agency: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. COVID-19 Vaccine Moderna, COVID-19 MRNA Vaccine Product Information; European Medicines Agency: Amsterdam, The Netherlands, 2021. [Google Scholar]
- European Medicines Agency. EMA Recommends First COVID-19 for Authorisation in the EU. 2021. Available online: https://www.ema.europa.eu/en/news/ema-recommends-first-covid-19-vaccine-authorisation-eu (accessed on 10 May 2021).
- European Medicines Agency. EMA Recommends COVID-19 Vaccine Moderna for Authorisation in the EU. 2021. Available online: https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-moderna-authorisation-eu (accessed on 10 May 2021).
- Grupo de Trabajo Técnico de Vacunación COVID-19. Estrategia de Vacunación Frente a COVID-19 en España. 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/covid19/docs/COVID-19_EstrategiaVacunacion.pdf (accessed on 10 May 2021).
- McNeil, M.M.; DeStefano, F. Vaccine-associated hypersensitivity. J. Allergy Clin. Immunol. 2018, 141, 463–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. About Chronic Diseases|CDC. Available online: https://www.cdc.gov/chronicdisease/about/index.htm (accessed on 18 November 2021).
- Centers for Disease Control and Prevention. Reactions and Adverse Events of the Pfizer-BioNTech COVID-19 Vaccine. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html (accessed on 17 May 2021).
- Centers for Disease Control and Prevention. Local Reactions, Systemic Reactions, Adverse Events, and Serious Adverse Events: Moderna COVID-19 Vaccine. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/reactogenicity.html (accessed on 17 May 2021).
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Schoenmaker, L.; Witzigmann, D.; Kulkarni, J.A.; Verbeke, R.; Kersten, G.F.A.; Jiskoot, W.; Crommelin, D.J. mRNA-lipid nanoparticle COVID-19 vaccines: Structure and stability. Int. J. Pharm. 2021, 601, 120586. [Google Scholar] [CrossRef] [PubMed]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Gajula, V.; Madathala, R.R.; Chennaiahgari, N.; Malayala, S.V. Non-life-threatening adverse effects with COVID-19 mRNA-1273 vaccine: A randomized, cross-sectional study on healthcare workers with detailed self-reported symptoms. J. Med. Virol. 2021, 93, 4420–4429. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Lee, Y.W.; Lim, S.Y.; Lee, J.H.; Lim, J.S.; Lee, S.; Park, S.; Kim, S.K.; Lim, Y.J.; Kim, E.O.; et al. Adverse Reactions Following the First Dose of ChAdOx1 nCoV-19 Vaccine and BNT162b2 Vaccine for Healthcare Workers in South Korea. J. Korean Med. Sci. 2021, 36, e115. [Google Scholar] [CrossRef] [PubMed]
- Tré-Hardy, M.; Cupaiolo, R.; Papleux, E.; Wilmet, A.; Horeanga, A.; Antoine-Moussiaux, T.; Della Vecchia, A.; Beukinga, I.; Vekemans, M.; Blairon, L. Reactogenicity, safety and antibody response, after one and two doses of mRNA-1273 in seronegative and seropositive healthcare workers. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Simon, V. Robust spike antibody responses and increased reactogenicity in seropositive individuals after a 1 single dose of SARS-CoV-2 mRNA vaccine 23. medRxiv 2021. [Google Scholar] [CrossRef]
- Raw, R.K.; Kelly, C.A.; Rees, J.; Wroe, C.; Chadwick, D.R. Previous COVID-19 infection, but not Long-COVID, is associated with increased adverse events following BNT162b2/Pfizer vaccination. J. Infect. 2021, 83, 381–412. [Google Scholar] [CrossRef] [PubMed]
- Mathioudakis, A.G.; Ghrew, M.; Ustianowski, A.; Ahmad, S.; Borrow, R.; Papavasileiou, L.P.; Petrakis, D.; Bakerly, N.D. Self-reported real-world safety and reactogenicity of COVID-19 vaccines: A vaccine recipient survey. Life 2021, 11, 249. [Google Scholar] [CrossRef] [PubMed]
- Debes, A.K.; Xiao, S.; Colantuoni, E.; Egbert, E.R.; Caturegli, P.; Gadala, A.; Milstone, A.M. Association of Vaccine Type and Prior SARS-CoV-2 Infection with Symptoms and Antibody Measurements following Vaccination among Health Care Workers. JAMA Intern. Med. 2021, 181, 1660–1662. [Google Scholar] [CrossRef] [PubMed]
- Soriano, V.; de Mendoza, C.; Gómez-Gallego, F.; Corral, O.; Barreiro, P. Third Wave of COVID-19 in Madrid, Spain. Int. J. Infect. Dis. 2021, 107, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A., Jr.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA Vaccines to Prevent COVID-19 Disease and Reported Allergic Reactions: Current Evidence and Suggested Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 1423–1437. [Google Scholar] [CrossRef] [PubMed]
- Stone, C.A.; Rukasin, C.R.F.; Beachkofsky, T.M.; Phillips, E.J. Immune-mediated adverse reactions to vaccines. Br. J. Clin. Pharmacol. 2019, 85, 2694–2706. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. About COVID-19 Vaccines. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/about-vaccines/index.html (accessed on 17 May 2021).
- Centers for Disease Control and Prevention. Vaccine Adverse Event Reporting System (VAERS) Publications. 2021. Available online: https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vaers/publications.html (accessed on 8 September 2021).
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for COVID-19 vaccines: A rapid systematic review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n = 2929 | % (95% CI) | ||
|---|---|---|---|
| Gender | |||
| Women | 2338 | 79.8% (78.4%, 81.3%) | |
| Men | 589 | 20.1% (18.7%, 21.6%) | |
| Non-binary | 2 | 0.1% (0%, 0.16%) | |
| Age (in years) | |||
| Median (IQR) | 34 | 33, 35 | |
| Age group | |||
| 18–55 | 2251 | 76.9% (75.3%, 78.4%) | |
| >55 | 678 | 23.1% (21.6%, 24.7%) | |
| Workers category | |||
| Medical doctor | 586 | 20.0% (18.6%, 21.5%) | |
| Registered nurse | 1386 | 47.3% (45.5%, 49.1%) | |
| Other, with patient contact | 461 | 15.7% (14.4%, 17.1%) | |
| Other, without patient contact | 496 | 16.9% (15.6%, 18.3%) | |
| History of allergies | |||
| Yes | 130 | 4.4% (3.69%, 5.18%) | |
| No | 2799 | 95.6% (94.8%, 96.3%) | |
| History of chronic illness | |||
| Yes | 408 | 13.9% (12.7%, 15.2%) | |
| No | 2521 | 86.1% (84.8%, 87.3%) | |
| History of COVID-19 infection | |||
| Yes | 817 | 27.9% (26.3%, 29.5%) | |
| No | 2110 | 72.1% (70.5%, 73.7%) | |
| Seriousness of COVID-19 infection | |||
| Asymptomatic | 131 | 16.0% (13.5%, 18.6%) | |
| Mild or moderate symptoms | 654 | 80.0% (77.3%, 82.8%) | |
| Hospitalization | 32 | 3.9% (2.59%, 5.25%) | |
| Vaccine type | |||
| BNT162b2 vaccine | 2373 | 81% (79.6%, 82.4%) | |
| mRNA-1273 vaccine | 506 | 17% (15.9%, 18.6%) | |
| Not reported | 50 | 1.7% (1.24%, 2.18%) | |
| Dose 1 | p-Value 1 | Dose 2 | p-Value 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| BNT162b2 | mRNA-1273 | BNT162b2 | mRNA-1273 | ||||||||
| n = 2373 | % (95% CI) | n = 506 | % (95% CI) | n = 2344 | % (95% CI) | n = 121 | % (95% CI) | ||||
| Occurrence of any adverse reaction | 963 | 40.6% (38.6%, 42.6%) | 303 | 59.9% (55.6%, 64.2%) | <0.001 | 1646 | 70.2% (68.4%, 72.1%) | 111 | 91.7% (86.8%, 96.6%) | <0.001 | |
| Duration of the reaction (days, median, IQR) | 3 | 2, 3 | 3 | 2, 4 | <0.001 | 2 | 2, 3 | 3 | 2, 4 | <0.001 | |
| Pain at injection site | 883 | 37.2% (35.3%, 39.2%) | 292 | 57.7% (53.4%, 62.0%) | <0.001 | 1376 | 58.7% (56.7%, 60.7%) | 99 | 81.8% (74.9%, 88.7%) | <0.001 | |
| Fatigue | 312 | 13.1% (11.8%, 14.5%) | 155 | 30.6% (26.6%, 34.6%) | <0.001 | 1141 | 48.7% (46.7%, 50.7%) | 86 | 71.1% (63.0%, 79.2%) | <0.001 | |
| Headache | 291 | 12.3% (10.9%, 13.6%) | 118 | 23.3% (19.6%, 27.0%) | <0.001 | 935 | 39.9% (37.9%, 41.9%) | 63 | 52.1% (43.2%, 61.0%) | 0.008 | |
| Malaise | 213 | 9.0% (7.83%, 10.1%) | 118 | 23.3% (19.6%, 27.0%) | <0.001 | 1008 | 43.0% (41.0%, 45.0%) | 83 | 68.6% (60.3%, 76.9%) | <0.001 | |
| Swelling or redness at injection site | 192 | 8.1% (6.99%, 9.19%) | 120 | 23.7% (20.0%, 27.4%) | <0.001 | 314 | 13.4% (12.0%, 14.8%) | 55 | 45.5% (36.6%, 54.3%) | <0.001 | |
| Muscle or joint pain | 154 | 6.5% (5.50%, 7.48%) | 86 | 17.0% (13.7%, 20.3%) | <0.001 | 713 | 30.4% (28.6%, 32.3%) | 53 | 43.8% (35.0%, 52.6%) | 0.002 | |
| Chills | 125 | 5.3% (4.37%, 6.17%) | 83 | 16.4% (13.2%, 19.6%) | <0.001 | 744 | 31.7% (29.9%, 33.6%) | 80 | 66.1% (57.7%, 74.5%) | <0.001 | |
| Fever (≥37.5 °C) | 82 | 3.5% (2.72%, 4.19%) | 66 | 13.0% (10.1%, 16.0%) | <0.001 | 623 | 26.6% (24.8%, 28.4%) | 80 | 66.1% (57.7%, 74.5%) | <0.001 | |
| Nausea or vomiting | 48 | 2.0% (1.46%, 2.59%) | 41 | 8.1% (5.73%, 10.5%) | <0.001 | 275 | 11.7% (10.4%, 13.0%) | 22 | 18.2% (11.3%, 25.1%) | 0.034 | |
| Insomnia | 50 | 2.1% (1.53%, 2.68%) | 13 | 2.6% (1.19%, 3.95%) | 0.500 | 209 | 8.9% (7.76%, 10.1%) | 17 | 14.0% (7.86%, 20.2%) | 0.056 | |
| Adenopathy | 40 | 1.7% (1.17%, 2.20%) | 19 | 3.8% (2.10%, 5.41%) | 0.003 | 141 | 6.0% (5.05%, 6.98%) | 12 | 9.9% (4.59%, 15.2%) | 0.083 | |
| Hives or rash | 24 | 1.0% (0.61%, 1.41%) | 19 | 3.8% (2.10%, 5.41%) | <0.001 | 44 | 1.9% (1.33%, 2.43%) | 6 | 5.0% (1.09%, 8.83%) | 0.033 | |
| Need for medical leave | 37 | 1.6% (1.06%, 2.06%) | 34 | 6.7% (4.54%, 8.90%) | <0.001 | 252 | 10.8% (9.50%, 12.0%) | 31 | 25.6% (17.8%, 33.4%) | <0.001 | |
| Need for medical attention | 27 | 1.1% (0.71%, 1.56%) | 14 | 2.8% (1.34%, 4.20%) | 0.120 | 76 | 3.2% (2.53%, 3.96%) | 12 | 9.9% (4.59%, 15.2%) | 0.010 | |
| Potential life-threatening reaction | 0 | 0.0% (0%, 0%) | 0 | 0.0% (0%, 0%) | >0.999 | 1 | 0.0% (0%, 0.13%) | 0 | 0.0% (0%, 0%) | >0.999 | |
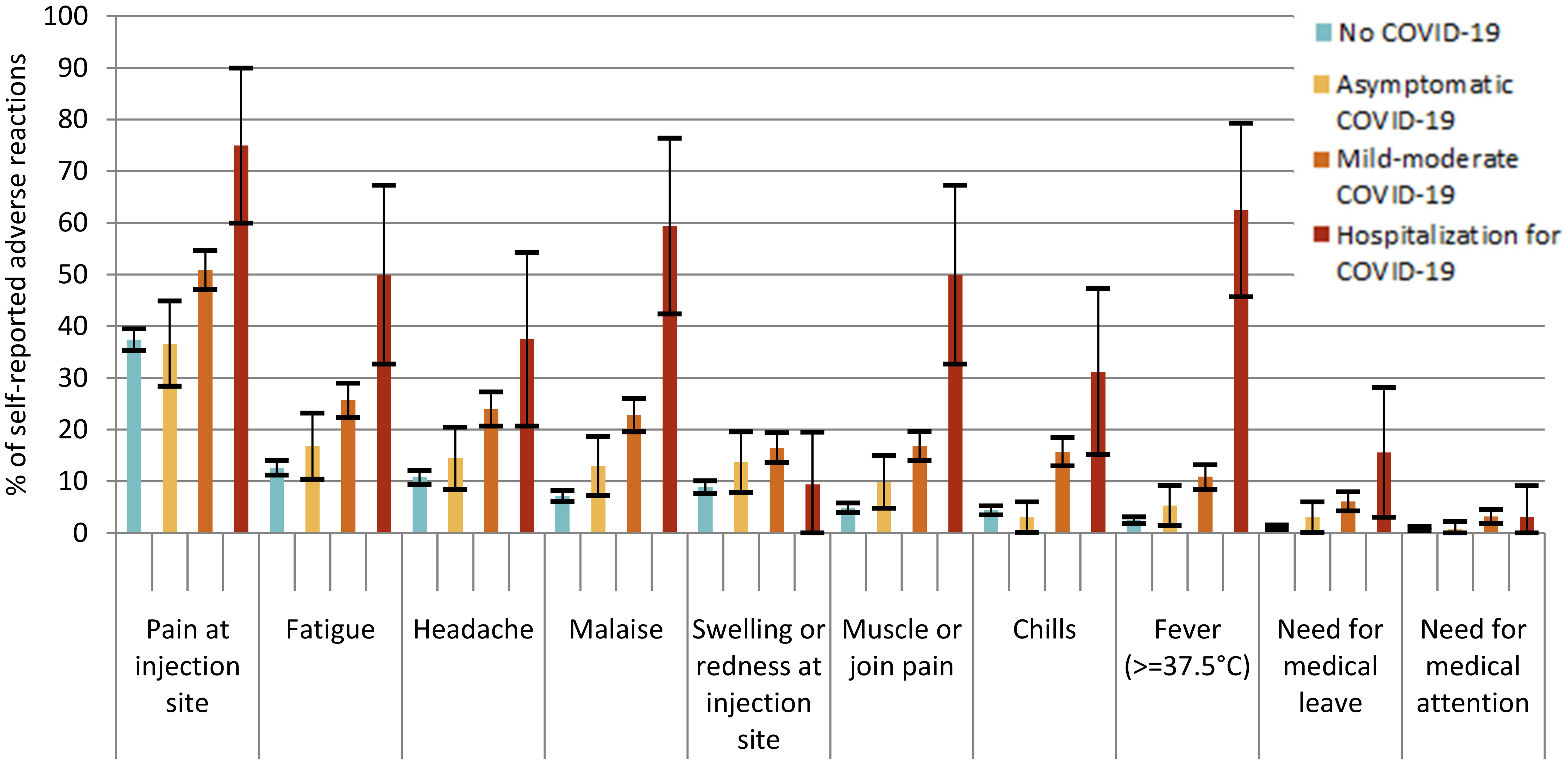
| No History of COVID-19 | Asymptomatic COVID-19 | Mild-Moderate COVID-19 | Hospitalization for COVID-19 | p-Value 1 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = 2110 | % (95% CI) | n = 131 | % (95% CI) | n = 654 | % (95% CI) | n = 32 | % (95% CI) | |||
| Vaccine dose 1 | ||||||||||
| Any adverse reaction | 852 | 40.4% (38.3%, 42.5%) | 53 | 40.5% (32.1%, 48.9%) | 354 | 54.1% (50.3%, 57.9%) | 26 | 81.3% (67.7%, 94.8%) | <0.001 | |
| Local adverse reaction | 807 | 38.2% (36.2%, 40.3%) | 48 | 36.6% (28.4%, 44.9%) | 337 | 51.5% (47.7%, 55.4%) | 24 | 75.0% (60.0%, 90.0%) | <0.001 | |
| Systemic adverse reaction | 462 | 21.9% (20.1%, 23.7%) | 32 | 24.4% (17.1%, 31.8%) | 261 | 39.9% (36.2%, 43.7%) | 25 | 78.1% (63.8%, 92.4%) | <0.001 | |
| Need for medical leave | 23 | 1.1% (0.65%, 1.53%) | 4 | 3.1% (0.11%, 6.00%) | 40 | 6.1% (4.28%, 7.95%) | 5 | 15.6% (3.04%, 28.2%) | <0.001 | |
| Need for medical attention | 18 | 0.9% (0.46%, 1.25%) | 1 | 0.8% (0%, 2.25%) | 21 | 3.2% (1.86%, 4.56%) | 1 | 3.1% (0%, 9.15%) | <0.001 | |
| Potential life-threatening reaction | 0 | 0% (0%, 0%) | 0 | 0% (0%, 0%) | 0 | 0% (0%, 0%) | 0 | 0% (0%, 0%) | >0.9 | |
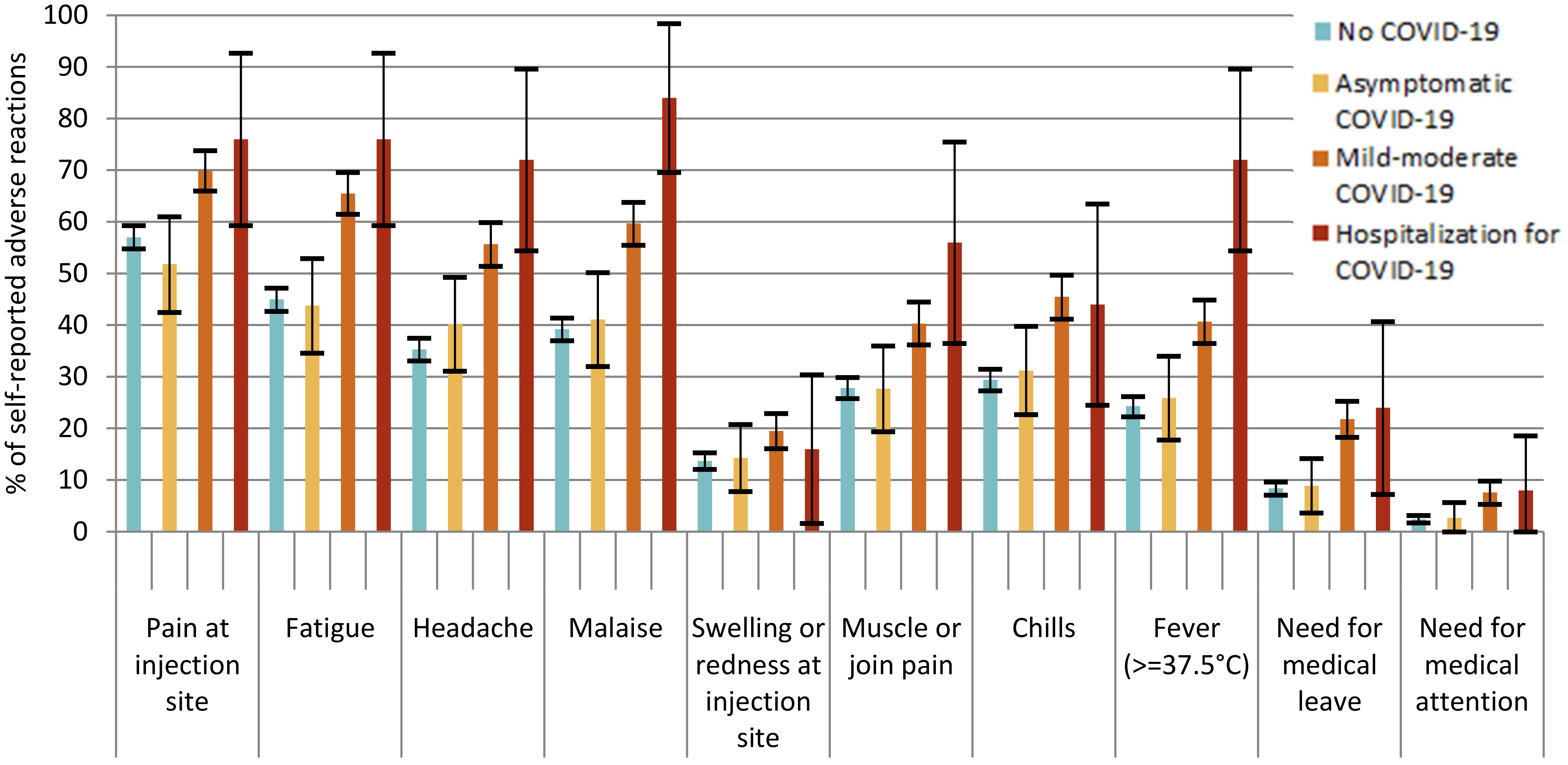
| Vaccine dose 2 | n = 1837 | % (95% CI) | n = 112 | % (95% CI) | n = 528 | % (95% CI) | n = 25 | % (95% CI) | ||
| Any adverse reaction | 1233 | 67.1% (65.0%, 69.3%) | 70 | 62.5% (53.5%, 71.5%) | 452 | 85.6% (82.6%, 88.6%) | 24 | 96.0% (88.3%, 100%) | <0.001 | |
| Local adverse reaction | 1062 | 57.8% (55.6%, 60.1%) | 58 | 51.8% (42.5%, 61.0%) | 376 | 71.2% (67.4%, 75.1%) | 19 | 76.0% (59.3%, 92.7%) | <0.001 | |
| Systemic adverse reaction | 1127 | 6.4% (59.1%, 63.6%) | 65 | 58.0% (48.9%, 67.2%) | 437 | 82.8% (79.5%, 86.0%) | 24 | 96.0% (88.3%, 100%) | <0.001 | |
| Need for medical leave | 154 | 8.4% (7.12%, 9.65%) | 10 | 8.9% (3.65%, 14.2%) | 115 | 21.8% (18.3%, 25.3%) | 6 | 24.0% (7.26%, 40.7%) | <0.001 | |
| Need for medical attention | 45 | 2.4% (1.74%, 3.16%) | 3 | 2.7% (0%, 5.67%) | 40 | 7.6% (5.32%, 9.83%) | 2 | 8.0% (0%, 18.6%) | <0.001 | |
| Potential life-threatening reaction | 0 | 0% (0%, 0%) | 0 | 0% (0%, 0%) | 1 | 0.2% (0%, 0.56%) | 0 | 0% (0%, 0%) | 0.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parés-Badell, O.; Martínez-Gómez, X.; Pinós, L.; Borras-Bermejo, B.; Uriona, S.; Otero-Romero, S.; Rodrigo-Pendás, J.Á.; Cossio-Gil, Y.; Agustí, A.; Aguilera, C.; et al. Local and Systemic Adverse Reactions to mRNA COVID-19 Vaccines Comparing Two Vaccine Types and Occurrence of Previous COVID-19 Infection. Vaccines 2021, 9, 1463. https://doi.org/10.3390/vaccines9121463
Parés-Badell O, Martínez-Gómez X, Pinós L, Borras-Bermejo B, Uriona S, Otero-Romero S, Rodrigo-Pendás JÁ, Cossio-Gil Y, Agustí A, Aguilera C, et al. Local and Systemic Adverse Reactions to mRNA COVID-19 Vaccines Comparing Two Vaccine Types and Occurrence of Previous COVID-19 Infection. Vaccines. 2021; 9(12):1463. https://doi.org/10.3390/vaccines9121463
Chicago/Turabian StyleParés-Badell, Oleguer, Xavier Martínez-Gómez, Laia Pinós, Blanca Borras-Bermejo, Sonia Uriona, Susana Otero-Romero, José Ángel Rodrigo-Pendás, Yolima Cossio-Gil, Antònia Agustí, Cristina Aguilera, and et al. 2021. "Local and Systemic Adverse Reactions to mRNA COVID-19 Vaccines Comparing Two Vaccine Types and Occurrence of Previous COVID-19 Infection" Vaccines 9, no. 12: 1463. https://doi.org/10.3390/vaccines9121463